Article Text

Abstract
Introduction The aim of our study is to explore the value of serum glycosylated hemoglobin A1c (HbA1c) in disease severity and clinical outcomes of acute pancreatitis (AP).
Research design and Methods Patients with AP were included from January 2013 to December 2020, retrospectively, dividing into normal serum HbA1c level (N-HbA1c) group and high serum HbA1c level (H-HbA1c) group according to the criteria HbA1c <6.5%. We compared patient characteristics, biochemical parameters, disease severity, and clinical outcomes of patients with AP in two groups. Besides, we evaluated the efficacy of serum HbA1c to predict organ failure (OF) in AP patients by receiver operating curve (ROC).
Results We included 441 patients with AP, including 247 patients in N-HbA1c group and 194 patients in H-HbA1c group. Serum HbA1c level was positively correlated with Atlanta classification, systemic inflammatory response syndrome, local complication, and OF (all p<0.05). Ranson, BISAP (bedside index of severity in acute pancreatitis), and CT severity index scores in patients with H-HbA1c were markedly higher than those in patients with N-HbA1c (all p<0.01). ROC showed that the best critical point for predicting the development of OF in AP with serum HbA1c is 7.05% (area under the ROC curve=0.79). Logistic regression analysis showed H-HbA1c was the independent risk factor for the development of OF in AP. Interestingly, in patients with presence history of diabetes and HbA1c <6.5%, the severity of AP was significantly lower than that in H-HbA1c group. Besides, there was no significant difference between with and without history of diabetes in N-HbA1c group.
Conclusions Generally known, diabetes is closely related to the development of AP, and strict control of blood glucose can improve the related complications. Thus, the level of glycemic control before the onset of AP (HbA1c as an indicator) is the key to poor prognosis of AP, rather than basic history of diabetes. Elevated serum HbA1c level can become the potential indicator for predicting the disease severity of AP.
- HbA1c
- digestion
Data availability statement
No data are available. Based on the principle of confidentiality of patient information, data cannot be disclosed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Generally known, previous diabetes history plays a key role in the progress of acute pancreatitis (AP), which can make patients susceptible to pancreatic structural changes and increase the risk of AP.
WHAT THIS STUDY ADDS
The level of glycemic control before the onset of AP (glycosylated hemoglobin A1c (HbA1c) as an indicator) is the key risk factor for the poor prognosis of AP, rather than the diagnosis of diabetes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our study demonstrated that elevated serum HbA1c level could become the potential indicator for predicting the disease severity of AP and might help to carry out stratification of patients with AP at an early stage in the future.
Introduction
Acute pancreatitis (AP) is one of the the most common acute gastrointestinal diseases, and its incidence rate is increasing year by year around the world. According to epidemiological data, the incidence rate of AP is on the rise year by year, but the mortality rate has declined.1 2 About 80% of patients with AP have mild disease courses and usually obtain recovery in the first week. However, the remainder progresses to moderate or severe cases with local or systemic complications and organ failure (OF), which ultimately leads to a significant increase in mortality.3 Especially mortality in AP patients with metabolic syndrome is noteworthy.4 Metabolic syndrome can increase the risk of cardiovascular diseases, including diabetes, dyslipidemia, and abdominal obesity.5 Szentesi et al6 showed that obesity, hyperlipidemia, and hypertension were the independent risk factors for the poor prognosis of AP. Many clinical studies have confirmed that patients with diabetes have an elevated risk of AP compared with patients without diabetes,7 and early hyperglycemia may predispose to systemic complications in AP.8 Nagy et al9 also found that peak blood glucose at admission and during hospitalization was independently associated with increased AP severity and mortality, and thus the control of blood glucose and the appropriate treatment of hyperglycemia are essential in the treatment of AP.
Hence, early identification of patients with AP with high mortality risk is the key to determine the treatment strategies for AP. The Atlanta classification revised in 2012 is considered the gold standard to evaluate the severity of AP. Nowadays, some clinical and biochemical scoring systems, including Ranson, bedside index of severity in acute pancreatitis (BISAP), CT severity index (CTSI), acute physiology and chronic health evaluation II (APACHE II) scores, and individual serum test (such as C reactive protein (CRP) and blood urea nitrogen (BUN)) are used to predict the occurrence of severe AP (SAP).10 Although these scoring systems have a certain predictive function on the severity of AP, they are cumbersome to operate and not convenient for clinical practice.11 Thus, there is an urgent need to develop a simple, sensitive, ideal marker to predict the disease severity of AP in the existing clinical setting.
Glycosylated hemoglobin A1c (HbA1c) is formed by the glycosylation of hemoglobin in the circulating red cell, which is a non-enzymatic condensate of glucose and hemoglobin.12 Glycosylated hemoglobin is divided into glycosylated hemoglobin A, glycosylated hemoglobin B, and glycosylated hemoglobin C. Among the various glycated hemoglobins, HbA1c is the predominant fraction.13 The level of serum HbA1c is a useful indicator for the retrospective assessment of glycemic status during the previous 2–3 months. Serum HbA1c level is closely related to inflammatory diseases, and elevated serum HbA1c level has been proven to strongly predict diabetic complications14 and cardiovascular morbidity.15 Selvin et al showed that every 1% increase in HbA1c was related to the 18% increase in the hazard of cardiovascular disease and 17% in stroke incidence.16 Furthermore, in patients with sepsis, serum HbA1c level is associated with the progression of persistent OF and with intensive care unit mortality.17
Diabetes can increase the prevalence of AP, which is one of the independent risk factors for the poor prognosis of AP. Generally known, strictly controlling glucose can improve the prognosis of related complications, such as diabetic nephropathy, macrovascular disease, and so on. We speculate whether patients with diabetes with controlling glucose before AP onset can improve the poor prognosis of AP. Thus, we conducted a retrospective study to determine the impact of controlling glucose on the severity and clinical outcomes of patients with AP by using HbA1c to assess the serum glucose control before AP onset.
Materials and methods
Patients
One thousand one hundred and ninety-six patients diagnosed with AP admitted to the Affiliated Hospital of Yangzhou University from January 2013 to December 2020 were included in our study. The diagnostic criteria of AP required two or more of the following criteria: persistent abdominal pain, elevated serum or plasma amylase and/or lipase levels (more than three times the upper limit of the normal), and characteristic results of AP in imaging studies.18 The exclusion criteria mainly included the following: (1) <18 years old, (2) during pregnancy, (3) history of cancer, (4) patients hospitalized repeatedly, and (5) patients without complete medical data and serum HbA1c values.
Data collection
After inclusion, demographic and clinical characteristics, including age, gender, weight, previous history, and personal history of patients with AP were collected. CTSI, Ranson, and BISAP scores were determined to evaluate the disease severity of AP. All patients were evaluated for blood routine and biochemical tests on admission. Leukocyte level and neutrophil and monocyte ratios were obtained from blood routine test. Serum levels of total bilirubin (TB), direct bilirubin (DB), albumin (ALB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), γ-glutamyl transferase (γ-GGT), lactate dehydrogenase (LDH), urea (UA), BUN, creatinine (Cr), glucose (GLU), triglyceride (TG), cholesterol (CHO), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) were obtained from blood biochemical test.
Serum HbA1c level was under the standard techniques by ion chromatography technique on the manufacturer’s instructions and its reference value was 0%–6.5%. According to the criteria HbA1c ≥6.5% after admission, patients were divided into two groups, including the normal serum HbA1c level group (N-HbA1c group) and high serum HbA1c level group (H-HbA1c group). The H-HbA1c group was further divided into 6.5%≤HbA1c<8%, 8%≤HbA1c<10%, and 10%≤HbA1c. The electronic medical records and laboratory results of included patients were checked by a professional doctor. The study conformed to the principles of the Declaration of Helsinki. Due to the retrospective characteristics of our study from January 2013 to December 2020, informed consent was waived and the ethics committee of the Affiliated hospital of Yangzhou University approved our study (No 2018-YKL11-27).
Assessment of the severity of AP
Based on the 2012 revised Atlanta classification, we divided the severity of AP into three groups: mild AP (MAP), moderately severe AP (MSAP), and SAP. MAP involved no OF and local/systemic complications. MSAP was accompanied by local/systemic complications and/or transient OF within 48 hours. SAP referred to patients with AP with single or multiple persistent OF and/or local or systemic complications over more than 48 hours. Local complications of AP included acute peripancreatic fluid collection, pancreatic pseudocyst, acute necrotizing collection, and walled-off necrosis.16 Finally, persistent OF was referred to as a modified Marshall score of ≥2 of the three organ systems (respiratory, cardiovascular, and renal), over a period of more than 48 hours.19
Diagnostic criteria for systemic inflammatory response syndrome (SIRS)
We defined the SIRS diagnostic standard on admission as two or more of the following four factors: (1) temperature >38°C or <36°C, (2) heart rate >90 beats/min, (3) respiratory rate >20 breaths/min (tachypnea) or arterial carbon dioxide pressure (PaCO2)<32 mm Hg (hyperventilation), and (4) leukocyte count >12×109/L or <4×109/L.
Statistical analysis
Data were analyzed with SPSS 19.0 (SPSS, Chicago, Illinois, USA). All continuous variables were represented as the mean±SD or median plus IQR. Categorical variables were presented as percentage. χ2 test and independent sample t-test were used to compare categorical variables and continuous variables, respectively. Comparisons between groups were made by using one-way analysis of variance. Pearson correlation analysis was used to assess the correlation between serum HbA1c level and laboratory test indicators. Receiver operator characteristic (ROC) curve analysis was used to assess serum HbA1c level for the prediction of severity of AP and to evaluate the sensitivity and specificity of HbA1c by GraphPad Prism 7.0 software. Gender, weight, smoking, drinking, diagnosed diabetes, non-alcoholic fatty liver disease (NAFLD), hypertriglyceridemia, previous AP, leukocyte count, ALT, AST, γ-GGT, LDH, TG, HDL, GLU, Cr, BUN, and H-HbA1c were set as independent variables for logistic regression analysis, and the OF was set as a dependent variable. We define bilateral p<0.05 as a statistically significant difference.
Results
General baseline situation
One thousand one hundred and ninety-six patients with AP from 2013 to 2020 were initially screened for the study, but 755 patients with AP were excluded and finally 441 cases were enrolled for analysis (online supplemental figure S1). Of all 441 patients with AP, the average age was 49.5 years old and 281 patients with AP (63.7%) were men. Of them, the N-HbA1c group had 247 (56%) patients, whereas the H-HbA1c group had 194 patients (44%).
Supplemental material

Associations between HbA1c level and different disease severity or clinical outcomes in patients with AP. The serum HbA1c level of different disease severity in patients with AP (A). The serum HbA1c level of AP patients with or without SIRS (B), LC (C) and OF (D) respectively. From N-HbA1c to 10% ≤ HbA1c patients, the proportion of different disease severity (E), SIRS (F), LC (G) and OF (H) in AP patients. AP, acute pancreatitis; HbA1c, glycosylated hemoglobin A1c; LC, local complication; MAP, mild AP; MSAP, moderately severe AP; OF, organ failure; SAP, severe AP; SIRS, systemic inflammatory response syndrome.
In terms of age, gender, smoking, hypertension, coronary heart disease, and previous AP, these baseline characteristics showed no significant differences between the two groups. The proportion of NAFLD and weight in H-HbA1c group were higher than those in N-HbA1c group (all p<0.05). Besides, whether in N-HbA1c group or H-HbA1c group, the most common AP etiology was hypertriglyceridemia (40.1% vs 59.8%), then biliary diseases (31.2% vs 13.9%), alcohol consumption (11.3% vs 13.9%), and other causes (17.4% vs 12.4%), as shown in table 1.
Comparison of baseline clinical characteristics for patients with groups
Biochemical parameter comparison between two groups
Table 2 showed the comparison of biochemical parameters between two groups. The serum leukocyte, UA, GLU, CHO, and TG (both p<0.05) levels in H-HbA1c group were significantly elevated compared with N-HbA1c group. Interestingly, patients with AP in the N-HbA1c group had higher levels of main liver function indexes, including AST and ALT (both p<0.05). Moreover, there was no significant difference in terms of neutrophil, monocyte, ALB, BUN, and Cr between the two groups.
Biochemistry characteristics of patients with groups
Serum HbA1c levels and the severity of AP
In figure 1, serum HbA1c level was remarkably associated with the AP severity scoring system. The level of serum HbA1c increased gradually from MAP to SAP (p<0.001). Moreover, serum HbA1c level had a significant increase in patients with OF, local complications, and SIRS (all p<0.01). In table 3, we found that the proportion of patients with MSAP and SAP was higher in H-HbA1c group. Meanwhile, clinical scoring systems (CTSI, Ranson score, and BISAP score) and major complications (including SIRS, local complications, and OF) were also more serious in the H-HbA1c group (all p<0.05). Interestingly enough, we found that in patients with presence history of diabetes and HbA1c <6.5%, the severity of AP was significantly lower than that in H-HbA1c group. Furthermore, in N-HbA1c group, there was no significant difference between with and without history of diabetes.
Comparison of the Atlanta classification, scores, and clinical outcomes with groups
According to the above results, the H-HbA1c group was further divided into 6.5%≤HbA1c<8%, 8%≤HbA1c<10%, and 10%≤HbA1c. As shown in figure 1E–H, from N-HbA1c group to the 10%≤HbA1c group, the MAP ratio decreased, while the SAP ratio increased (both p<0.001). At the same time, we found that the incidences of SIRS, local complications, and OF in the 10%≤HbA1c patients were significantly higher than those in the N-HbA1c patients, which were consistent with the above results (all p<0.05).
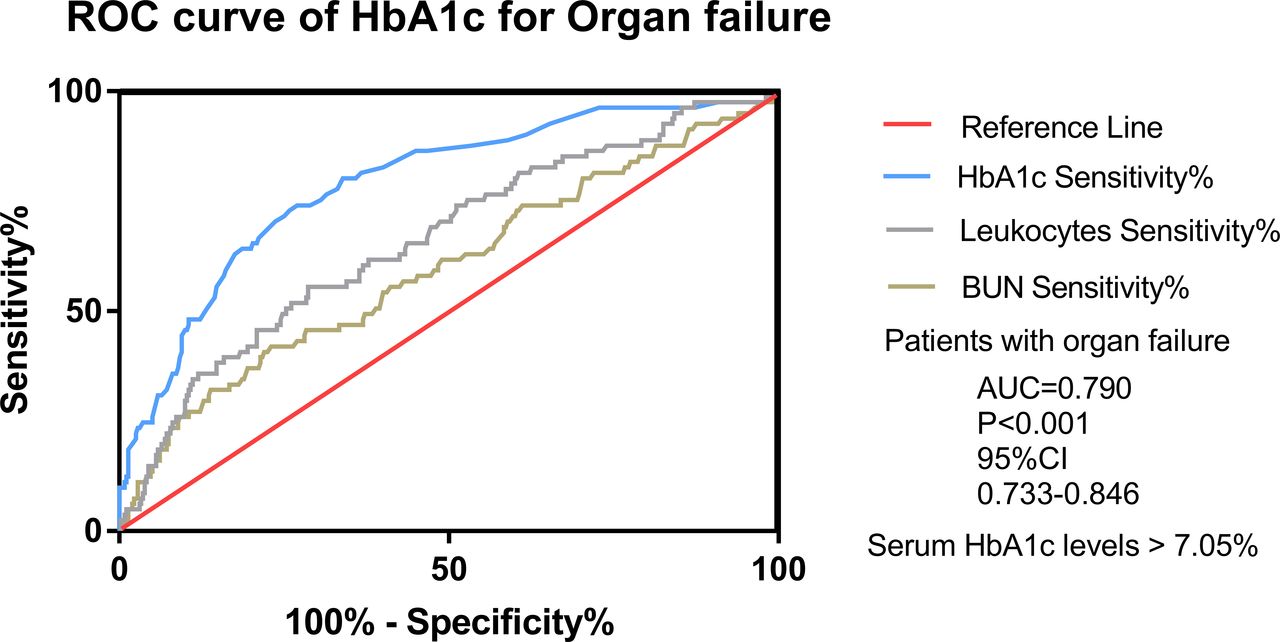
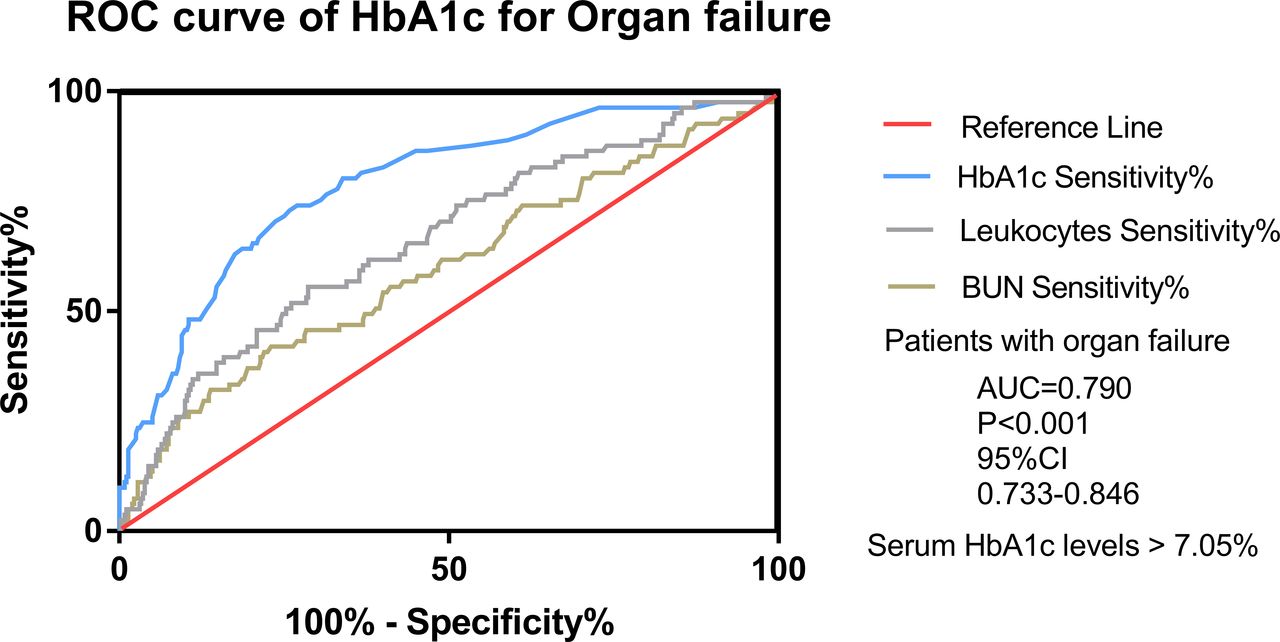
ROC curve analysis of HbA1c for predicting OF in AP
In figure 2, we found that the area under the ROC curve of HbA1c for OF in patients with AP was 0.79 and the optimal cut-off level was 7.05%, which provided 74.1% sensitivity and 73.1% specificity. Our study also found that the ability of HbA1c to predict OF in patients with AP was better than leukocytes and BUN.
{kind=link}
{kind=link}
HbA1c, leukocytes, and BUN for the prediction in organ failure of patients with AP: ROC analysis. AUC, area under the ROC curve; AP, acute pancreatitis; BUN, blood urea nitrogen; HbA1c, glycosylated hemoglobin A1c; ROC, receiver operating curve.
Besides, logistic regression analysis showed that advanced leukocytes, LDH, GLU, and H-HbA1c were independent risk factors for the development of OF in patients with AP (online supplemental table S1). Further adjusting for confounding factors, we found that HbA1c was indeed the independent risk factor for the development of OF in AP (online supplemental table S2).
Supplemental material
Correlation between serum HbA1c levels and clinical indicators
To better evaluate the predictive ability of serum HbA1c level on the severity and prognosis of AP, we conducted the correlation analysis between serum HbA1c and clinical markers. In online supplemental table S3, serum HbA1c level was positively correlated with serum levels of leukocytes (R=0.19, p<0.001), GLU (R=0.745, p<0.001), TG (R=0.26, p<0.001), and CHO (R=0.321, p<0.001). Whereas serum HbA1c level was negatively correlated with the serum levels of ALT (R=−0.157, p=0.001) and AST (R=−0.137, p=0.004). However, there was no significant correlation between serum HbA1c levle and the levels of serum HDL, LDL.
Testing for selection bias
To verify whether there was a selection bias in all patients with AP in our study, we compared patients with available serum HbA1c level (n=441) and patients with unavailable serum HbA1c level (n=755). Except for age, there was no significant difference in general baseline and clinical characteristics between two groups (online supplemental table S4). Patients with unavailable HbA1c level were older (52.3 vs 49.5 years, p=0.002). There was no significant difference between the two groups in disease severity and underlying disease.
Discussion
AP is the clinical emergency in which local inflammatory injury of pancreas progresses to complications or multiorgan involvement. The prognosis of AP is mainly based on the development of OF and local complications.20 Our results showed that the incidence of OF caused by AP is about 18.6%, which was in line with previous research results.21 Therefore, early identification of high risk of OF in patients with AP seems to be the key for early medical intervention. Although many scales have been performed to predict the clinical prognosis of AP, scales involves more tests, indices, and larger time span. Hence, it is of great urgency to develop a clinically applicable marker to forecast patients with SAP in the existing clinical setting.
Ramin et al22 showed that there was a close relationship between the severity of AP and the incidence of metabolic syndrome and its constituent factors, including obesity, hyperglycemia, and hypertriglyceridemia. Previous studies reported that patients with diabetes had a higher risk for AP,7 and hyperglycemia may predispose patients with AP to OF.8 Shenoy et al23 revealed that more than half of the patients with AP could observe transient hyperglycemia. In addition, Das et al24 showed that the incidence rate of diabetes was 15% 1 year after the onset of AP and 23% 5 years later. A recent meta-analysis also further confirmed that the incidence rate of diabetes within 5 years after the onset of AP was 23%, and the incidence rate after 5 years was 37%.25 Previously, our team found that diabetes could aggravate the severity of AP possibly via the activation of NOD-like receptor thermal protein domain associated protein 3 (NLRP3) inflammasome pathway.26 Previous studies have pointed out that pre-existing diabetes negatively influences the outcome of AP and increases the risk of renal failure, local complications, and mortality.27 However, our research focused on the blood glucose control before the onset of AP, rather than the impact of diabetes itself on AP. Blood glucose level was an important criterion for the RANSON score, which was used to assess the prognosis of AP.28 The gold standard for evaluating blood glucose level was HbA1c, and high serum HbA1c level was also related to the risk of complications in patients with diabetes.29 Controlling glucose may be more effective than diabetes in the prognosis of AP. Thus, the main focus of our study was the predictive ability of serum HbA1c in the early AP.
Our study fully confirmed the evaluation of HbA1c on the prognosis of AP. According to the overall severity, local complications, systemic complications, ROC curve, and multiple regression analysis, we found that the high level of HbA1c suggested the poor prognosis of AP. Based on this, we pay more attention to people who have a clear history of diabetes but have good blood glucose control. It was most amusing to discover that in patients with presence history of diabetes and HbA1c <6.5%, the severity of AP was significantly lower than that in H-HbA1c group. Furthermore, in N-HbA1c group, there was no significant difference between with and without history of diabetes. Therefore, the results clearly show that previous glycemic control, rather than diabetes history, has a more pronounced effect on the prognosis of AP. Paragomi et al30 also showed that pre-existing diabetes mellitus might not be a risk factor for severe AP, which was consistent with our results. Interestingly, we found that HbA1c is still the independent risk factor for OF in patients with AP in the population with different confounding factors. In addition, we also found that both HbA1c and serum glucose level after admission were risk factors for the poor prognosis of AP, which suggested that glucose metabolism played a significant role in the poor prognosis of AP.
Generally known, pancreatic diabetes, also known as type 3c diabetes mellitus (T3cDM), is a type of diabetes caused by pancreatic exocrine diseases.31 The etiology of T3cdm mainly includes AP, chronic pancreatitis, pancreatic cancer, cystic fibrosis, and so on.32 Recent studies have found that it is inevitable that the patients with AP complicated with pancreatic necrosis may have some form of impaired glucose metabolism. The study indicates that about 25% of patients with AP are diagnosed with diabetes within 5 years and that proportion may even be higher after 5 years.24 Thus, we detect serum HbA1c in the early AP, which is conducive to the differential diagnosis of pancreatic diabetes.
Diabetes could make patients in chronic inflammation for a long time, which would lead to the spread of inflammatory factor reactions in patients. Emanuela et al showed that serum CRP, tumor necrosis factor-α, interleukin (IL)-1β, and IL-6 levels in diabetes could cause pancreatic islets β-cell dysfunction and apoptosis, so suggested that inflammatory markers may be involved in islets β-cell damage and insulin resistance.33 Given that the level of serum HbA1c reflects a patient’s glycemic state during 2–3 months, high serum HbA1c level indicate the persistent hyperglycemic state.34 This causes the increase in the levels of inflammatory factors above, which may be a major reason for aggravating AP. Besides, chronic hyperglycemic state may damage the endothelial glycocalyx.35 Degradation of the endothelial glycocalyx alters endothelial barrier permeability and may cause damage to the microcirculation, which leads to OF.17 The endothelial glycocalyx damage may be more severe in patients with H-HbA1c levels than N-HbA1c level.17 SAP may damage the endothelial glycocalyx by releasing inflammatory markers, which leads to malfunction of the intestinal microcirculation and mucosal barrier.36 This means that patients with elevated serum HbA1c level who develop SAP may suffer from more severe endothelial glycocalyx destruction, because of chronic hyperglycemia on the endothelial glycocalyx. Moreover, we need further studies to determine whether the risk of OF can be reduced by improving microcirculation in patients with AP.
However, there are several potential limitations of our study. On the one hand, it was retrospective, and there are only 10 people in previous diagnosed diabetes and HbA1c <6.5% group, which is likely to have data bias. On the other hand, it is difficult for us to observe the dynamic change of this index in AP. Thus, the prospective, multicenter study is warranted to confirm the prediction of HbA1c on the disease severity and clinical outcome of AP.
Conclusion
All in all, our study demonstrated that elevated serum HbA1c level is an important predictor of disease severity and OF in patients with AP. HbA1c may help to carry out stratification of patients with AP at an early stage in the future.
Data availability statement
No data are available. Based on the principle of confidentiality of patient information, data cannot be disclosed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FH, X-lS and J-jP contributed equally.
Contributors FH, X-lS, and J-jP helped design the study and wrote the manuscript. X-pJ, L-hH, and G-tL helped design the study and oversaw all study operations. K-yW, Q-tZ, and C-cY had access to data and conducted data analysis. W-mX, Y-bD, X-pY, and W-qL reviewed findings and provided critical revisions to the manuscript. All authors revised the manuscript critically and approved the final version of the manuscript. G-tL is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This research was funded by National Natural Science Foundation of China (Nos 82070668 and 82004291); Cultivation Foundation of Yangzhou Municipal Key Laboratory (No YZ2021147); Shanghai Shuguang Program (No 20SG36); and International scientific and technological cooperation project (YZ2022207).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.