Article Text

Abstract
Evidence is still emerging on the relationships of arterial stiffness with cardiac autonomic neuropathy (CAN) and peripheral neuropathy (PN). To our knowledge no systematic reviews or meta-analyses of these associations have been published. The purpose of our review was to assess the association of arterial stiffness with each type of neuropathy. Medline and Embase were systematically searched for observational studies of arterial stiffness and neuropathy.
The systematic review of 60 studies (25 for CAN and 37 for PN), 59 including people with diabetes, showed arterial stiffness overall was higher in people with neuropathy than people without neuropathy. Forty-three studies were included in the meta-analysis. For CAN (19 studies), arterial stiffness was increased in people with neuropathy compared with without, as measured by pulse wave velocity (PWV) (mean difference: 1.32 m/s, 95% CI 0.82 to 1.81, p<0.00001), pulse pressure (PP) (mean difference: 6.25 mmHg, 95% CI 4.51 to 7.99, p<0.00001) or augmentation index (mean difference: 5.52%, 95% CI 3.46 to 7.58, p<0.0001). For PN (26 studies), arterial stiffness was increased in people with neuropathy compared with those without, as measured by PWV (mean difference: 1.22 m/s, 95% CI 0.87 to 1.58, p<0.00001) or PP (mean difference: 4.59 mmHg, 95% CI 2.96 to 6.22, p<0.00001). Only two cohort studies were located so the temporality of the association between arterial stiffness and neuropathy remains unclear. Increased arterial stiffness is associated with CAN and PN.
PROSPERO registration number: CRD42019129563.
- meta-analysis
- compliance
- diabetic neuropathies
- epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There are an increasing number of studies in people with diabetes that investigate the association of arterial stiffness with cardiac autonomic neuropathy (CAN) and peripheral neuropathy (PN). The evidence, however, as far as we are aware, has not been assessed by way of systematic review and meta-analysis.
WHAT THIS STUDY ADDS
This review identifies, in people with diabetes, clear evidence of an association of arterial stiffness with CAN and PN and indicates that arterial stiffness could be associated with the development of each type of neuropathy. The review also reveals that further research is required to establish the temporality of the relationship.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Arterial stiffness, which is inexpensive and easily able to be assessed in clinical practice, is not usually evaluated in people with diabetes. Incorporation of this measure may help to identify people who are at increased risk of CAN and PN. The reduction of arterial stiffness may also form a new research avenue for therapeutics that prevent and treat each type of neuropathy. Further investigation, however, is first required to understand the temporality of the relationships of arterial stiffness with CAN and PN.
Neuropathy is a common complication of diabetes. The most usual type of neuropathy is distal symmetric peripheral polyneuropathy, also referred to as peripheral neuropathy (PN), defined in people with diabetes as the presence of symptoms or signs of peripheral damage to nerves (sensory or motor) after the exclusion of other causes.1 The incidence and prevalence of PN is uncertain but is estimated to occur in at least 20% of people who have had type 1 diabetes for at least 20 years2 3 and 50% of people who have had type 2 diabetes for at least 10 years.4 5 PN can lead to foot ulceration and is a major contributor to falls and fractures.1
Cardiac autonomic neuropathy (CAN), which results from damage to the autonomic nerve fibers to the heart, is also prevalent in populations who have had diabetes for many years. CAN was found in 30% of one cohort of people who had type 1 diabetes for at least 20 years3 6 and is present in 60% of people who had type 2 diabetes for 15 years.7 8 CAN is associated with significantly increased risk of cardiovascular mortality as well as progression of diabetic nephropathy and chronic kidney disease.1
CAN and PN are for the most part irreversible though treatments do exist to alleviate patient symptoms. Historically, diagnosis of neuropathy requires examination by skilled personnel and can involve specialized equipment.9 In its early stages, CAN is often asymptomatic and can only be detected by decreased heart rate variability (HRV).1
The identification of modifiable risk factors for neuropathy could assist in the diagnosis of neuropathy, as well as provide new research avenues for the prevention and treatment of the condition. An emerging modifiable risk factor is arterial stiffness, which is the loss of compliance in the more elastic arteries. This leads to reduced cushioning of the cardiac pulse when blood is ejected from the heart and enhanced systolic blood pressure (SBP). This in turn, results in an increase in pulsatile stress in the microcirculation, leading to tearing of endothelial and smooth muscle cells in the smaller arteries that supply blood to the peripheral and cardiac nerves.10
Arterial stiffness can be measured by waveform analysis. The most common measures are pulse wave velocity (PWV), with carotid-femoral PWV considered the “gold standard,” augmentation index (AIx), and the cruder measure of pulse pressure (PP). With advances in technology, devices that measure arterial stiffness with waveform analysis have become increasingly inexpensive, non-invasive, easy to use, and portable.11
An increasing number of studies have measured the relationship between arterial stiffness and neuropathy. To our knowledge, these studies have yet to be assessed by way of systematic review or meta-analysis. Accordingly, we conducted a systematic review and meta-analysis of observational studies that examined the association between arterial stiffness and neuropathy (limited to CAN or PN). We hypothesized that, compared with people who have lower arterial stiffness, people with higher arterial stiffness were more likely to have neuropathy or experience a progression in neuropathy.
Methods
Data sources and searches
We conducted our systematic review and meta-analyses in accordance with both the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines12 and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines.13 The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on August 27, 2019 (registration number CRD42019129563).
AB searched Medline and Embase up to June 13, 2022. The search strategy for Medline, which was adapted for Embase, is set out in online supplemental table 1. In addition, AB searched the reference lists of eligible articles and previous reviews for additional studies, and the gray literature using Google and Web of Science, as well as PROSPERO for any ongoing or recently completed systematic reviews. Studies reported in abstracts were included. There was no restriction on language with non-English articles translated using Google Translate. For cohort studies, there was no restriction on length of follow-up.
Supplemental material
Study selection
We included observational studies, namely, cross-sectional, case-control, or cohort studies. We excluded case series and case reports. There was no restriction on participants, including age, sex, blood pressure level, diabetes status, type, or duration.
Neuropathy studies were limited to those that investigated CAN or PN. We included studies where participants were classified as having neuropathy either through a recorded history of neuropathy, or the use of a validated screening instrument (with any adaptations) including for CAN, the Ewing battery of tests14 and for PN, the Michigan Neuropathy Screening Instrument (MNSI),15 and the Neuropathy Disability Score (NDS).16 We also included studies that employed one or more validated tests used to help diagnose neuropathy (such tests may also be incorporated into screening instruments), which included for CAN, measures of HRV, and for PN, included self-report, nerve conduction velocity (NCV), quantitative sensory testing (QST), vibration perception with a tuning fork, pinprick sensation using a monofilament, and ankle reflexes tested with a hammer.1 9
Studies were further limited to those that used waveform analysis, including PWV, AIx, and PP, to measure arterial stiffness. In relation to cross-sectional and case-control studies, we included studies where the exposure was arterial stiffness and the outcome was neuropathy and vice versa. In relation to cohort studies, we included studies where the exposure was arterial stiffness and the outcome was the development or progression of neuropathy.
Following the search, duplicates were removed. Titles and abstracts were screened by AB and JS who also undertook the final study selection, based on the inclusion criteria and the full-text articles. Rayyan software was used for both parts of the screening process.17 Any discrepancies were resolved by consensus and discussion with any disagreements between the authors resolved through discussion with RKRS.
Data extraction and quality assessment
Data were extracted by AB and checked by JS. Any calculations using the study data were conducted by AB. The quality of each included study was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS) for case-control and cohort studies.18 NOS was also adapted for cross-sectional studies. There were five criteria for cross-sectional studies, with a study able to obtain a maximum of six points; and eight criteria for case-control or cohort studies, with a study able to obtain a maximum of nine points. Studies were judged to be of high quality (≥3 for cross-sectional studies or ≥5 for case-control or cohort studies) or low quality (<3 for cross-sectional studies or <5 for case-control or cohort studies).
Data synthesis and analysis
For the systematic review, a qualitative summary was used to summarize and explain the characteristics and outcomes of the included studies. We further performed a meta-analysis if we identified at least two studies with results that could be combined into such an analysis. For the meta-analysis, studies were separated into CAN and PN. Case-control and cross-sectional studies were combined in the same meta-analyses. The vast majority of results suitable for meta-analysis (which may not be the only results presented) reported the number of people with and without neuropathy, likely due to the ease of categorization. Arterial stiffness was predominantly recorded as a continuous measure. To perform a meta-analysis in these studies, therefore, we also treated neuropathy as the exposure and arterial stiffness as the outcome. We extracted the number of people with and without neuropathy, as recorded by the study investigators, and the mean and SD of the different measures of arterial stiffness for each exposure group. The few studies that split participants into people with high and low arterial stiffness differed in their measures of arterial stiffness, as well as the cut-points applied to such measures, and hence were unable to be combined into a meta-analysis where arterial stiffness was the exposure and neuropathy was the outcome.
Weighted mean differences and 95% CIs were calculated for each continuous exposure. When the outcome measure was reported as mean and SEM, SDs were estimated using Review Manager V.5.4 software (https://training.cochrane.org/online-learning/core-software/revman). If the outcome measures were reported as the median and IQR, mean and SD values were estimated using formulas published by Luo et al19 and Wan et al.20 Where a study separated out an exposure or non-exposure group into two or more groups, such as when participants with neuropathy were grouped by severity of neuropathy (ie, participants may be grouped as having early stage neuropathy or manifest neuropathy based on the number of abnormal tests), where possible, we combined those groups into one exposure or non-exposure group. If a study, while using a measure of arterial stiffness, determined that measure at more than one site, such as carotid-femoral PWV and brachial-ankle PWV, the most central measure was used. Random-effects models were used in the meta-analyses to provide the most conservative estimates. We assessed heterogeneity with Cochran’s Q test and the I2 statistic, with an I2 >50% taken to indicate substantial heterogeneity.21
When we detected substantial heterogeneity, and there were at least 10 studies,21 we conducted subgroup analyses in relation to type of PWV (central or peripheral), age, diabetes duration and SBP as well as meta-regression, where each subgroup had at least four studies,22 in relation to other potential sources of heterogeneity including sex and study size. Sensitivity analyses were conducted by excluding the one low-quality study (as assessed using NOS), by excluding the two studies published only by way of abstract and by assessing whether the review conclusions would have been different if a fixed effect model had been used. Where there were at least 10 studies in a meta-analysis, we also generated funnel plots for the visual assessment of publication bias,23 and performed Egger’s test.24 All tests were two-tailed and a p value <0.05 was considered statistically significant. We undertook the meta-analysis using Review Manager V.5.4 software and R statistical software package V.4.0.5 (https://www.r-project.org/).
We used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to evaluate the overall certainty of the body of evidence for each outcome.25 GRADE has four levels: high, moderate, low, or very low, with observational studies initially classified as providing low quality of evidence.
Results
Study characteristics
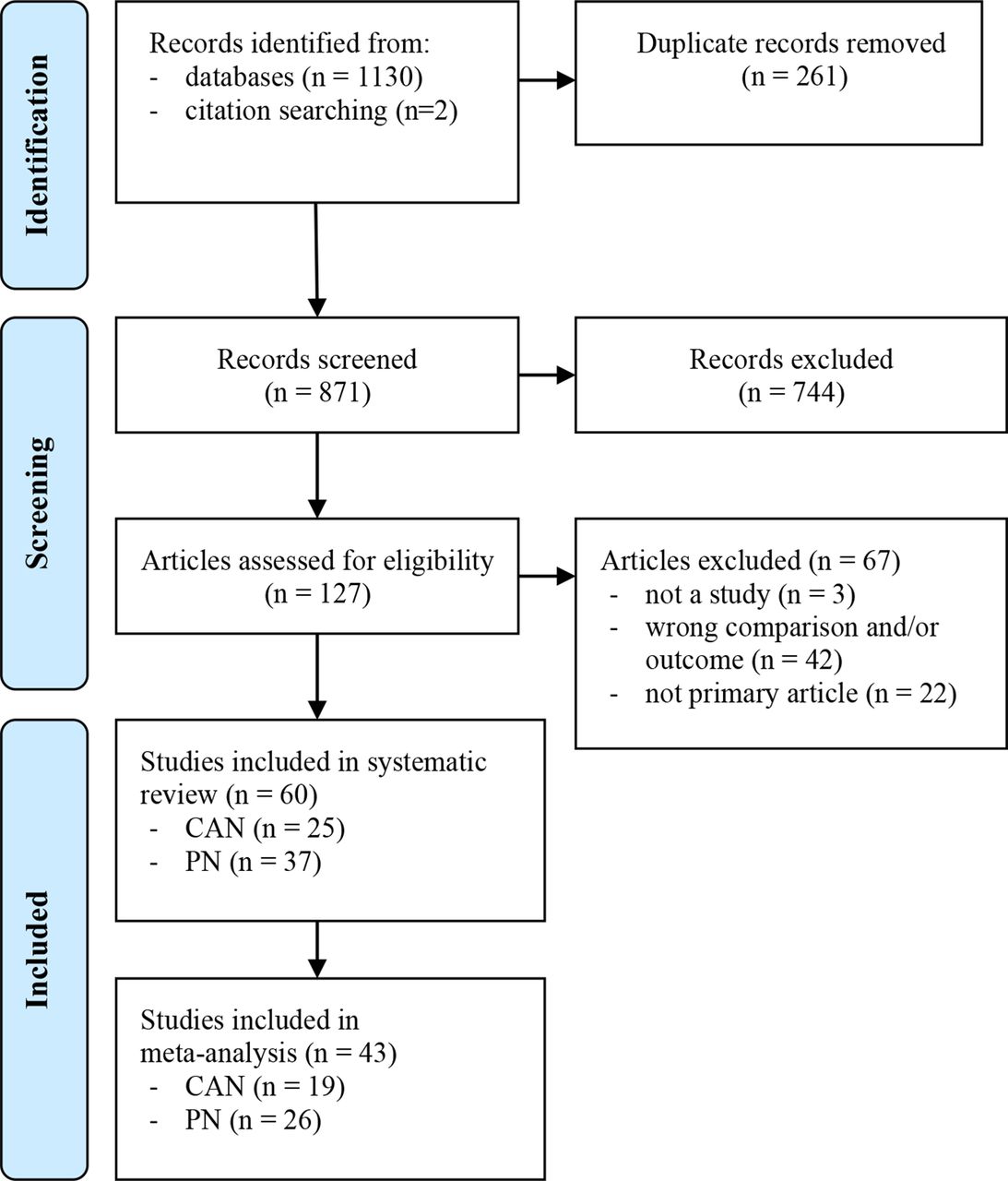
In total, 60 studies were included in the systematic review,26–85 with 43 of those studies including at least one arterial stiffness measurement suitable for meta-analysis.29–31 33–35 37–39 41 42 46 47 52 53 55 57 59–77 79–85 Although various studies adjusted for age, sex, diabetes duration, or SBP in data analysis, the values used in the meta-analyses were not adjusted for, other than those studies that only included participants of one sex.65 75 Aso et al29 and Yokoyama et al83 investigated both CAN and PN (figure 1). Characteristics of the studies included in the meta-analysis are summarized in table 1 in respect of those measures included in the meta-analysis. More detailed characteristics, as well as results, for all studies included in the systematic review are set out in online supplemental table 2 (CAN) and online supplemental table 3 (PN). Those articles that fit the inclusion criteria but were excluded, as they were not the primary article, are set out in online supplemental table 4.

Flowchart diagram for study selection of systematic review and meta-analysis (based on PRISMA guideline). CAN, cardiac autonomic neuropathy; PN, peripheral neuropathy.
Characteristics of observational studies included in meta-analysis on the association between arterial stiffness and neuropathy
For the purposes of investigating arterial stiffness and neuropathy, we classified 53 of the studies as cross-sectional,26 28–31 33–36 38–62 64–67 69 71 73–85 5 as case-control37 63 68 70 72 and 2 as cohort.27 32 For cross-sectional studies, all participants had diabetes, except Allison et al26 and Kuo et al,46 who included participants regardless of diabetes status, as well as Cho et al,35 who alongside participants with diabetes, also separately analyzed those with no history of disease known to cause PN. Amione-Guerra and Prasad28 did not state diabetes status. In case-control studies, we only analyzed participants with diabetes (to avoid confounding where cases had diabetes and neuropathy and controls were healthy). All participants in cohort studies had diabetes.
Of the 59 studies specifying inclusion of participants with diabetes, 38 were carried out in people with type 2 diabetes,27 29 30 32–34 36 39 41–43 45 48 49 51 54–56 59 60 62 64–67 70–72 75–77 79–85 11 in people with type 1 diabetes37 40 44 47 50 53 58 63 69 74 78 and 4 in people with either type 1 or type 2 diabetes31 38 57 73 with Fleischer et al38 and Moţăţăianu et al57 reporting separate results for type 1 and type 2 diabetes. Six studies did not specify diabetes type.26 35 46 52 61 68 Of the 49 studies that reported mean diabetes duration, 26 had a mean diabetes duration of at least 10 years29 31 33 34 36–38 40 41 44 48 50 53 54 56 58 59 62 63 67–69 74 76 78 82 and 22 had a mean diabetes duration of less than 10 years.27 30 32 39 42 43 47 49 55 60 64 65 70 71 73 75 79–81 83–85 Moţăţăianu et al57 reported mean diabetes duration of 16 years for type 1 diabetes and mean diabetes duration of 7 years for type 2 diabetes.
Nine studies reported mean SBP ≥140 mmHg,32 33 35 36 38 41 54 57 76 but for Fleischer et al38 and Moţăţăianu et al57 this was only in respect of participants with type 2 diabetes. Fourteen studies did not report mean SBP28 44–46 48 51 52 61 68 70–73 77 with the remainder of studies reporting mean SBP <140 mmHg. Five studies reported participants with a mean age of ≤30 years,40 44 47 50 71 34 studies reported participants with a mean age of between 31 and 59 years,30–32 34 37 39 42 43 45 49 52 53 55 57 58 60–66 68–70 72–74 78 81–85 and 18 studies reported participants with a mean age of ≥60 years.26 27 29 33 35 36 41 46 48 54 56 59 67 75–77 79 80 Fleischer et al38 reported participants with a mean age of 50 in the type 1 diabetes group and 64 in the type 2 diabetes group. Two studies did not report mean age.28 51 Refaie65 only included women. Morimoto et al56 and Tanaka et al75 only included men. Scarpello et al68 did not report sex. All other studies included men and women.
Arterial stiffness was measured by way of PWV in 32 studies,29 30 32–34 36 37 39 40 46 47 50–52 60–62 66 68 70–79 81–83 PP in 27 studies,30 31 33–35 38 39 41 42 53–55 57 59 60 63–65 67 69 75 76 80 82–85 AIx in 6 studies,34 47 66 69–71 AIx adjusted to a heart rate of 75 bpm in 4 studies,30 40 56 78 ankle-brachial index (ABI) in 5 studies,26–28 49 58 cardio ankle vascular index (CAVI) in 4 studies,43–45 82 pulsatility index in 1 study,74 stiffness index in 1 study,48 and the subendocardial viability ratio in 1 study.69
Association of CAN and arterial stiffness
There were 25 studies that investigated the association between CAN and arterial stiffness.29 31 33 36 38 40 44 47 50 53 55 57 58 60 63–66 69–71 78 79 83 85 Seventeen reported a positive association of CAN with at least one measure of arterial stiffness without adjusting for age, sex, diabetes duration, or SBP.29 31 36 38 47 50 53 55 58 60 66 69–71 78 79 83 Four other studies did not find a relationship.33 57 64 85 Of those studies that adjusted for age, sex, diabetes duration, or SBP, eight studies reported a positive association of CAN with at least one measure of arterial stiffness.29 40 44 50 65 66 69 79 Five studies did not find a relationship33 36 63 78 85 (table 1 and online supplemental table 2).
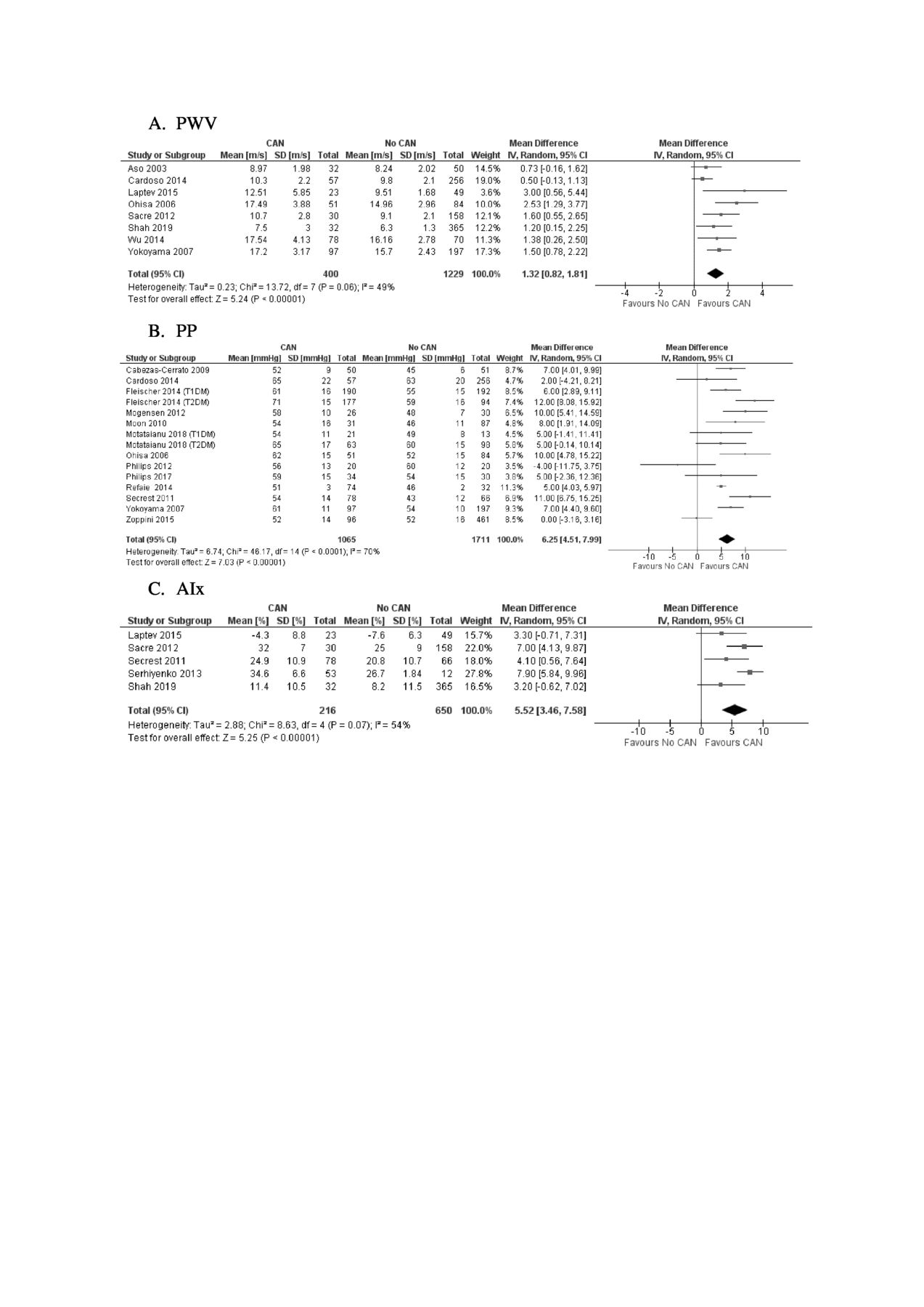
There were 19 studies with sufficient data to be included in the meta-analysis to estimate the association of CAN with arterial stiffness29 31 33 38 47 53 55 57 60 63–66 69–71 79 83 85 (figure 2). Eight studies measured arterial stiffness by way of PWV with a total number of 1629 participants: 400 with CAN and 1229 without CAN29 33 47 60 66 71 79 83 (figure 2A). Overall, PWV was higher in participants with CAN than those without CAN (mean difference: 1.32 m/s, 95% CI 0.82 to 1.81, p<0.00001).
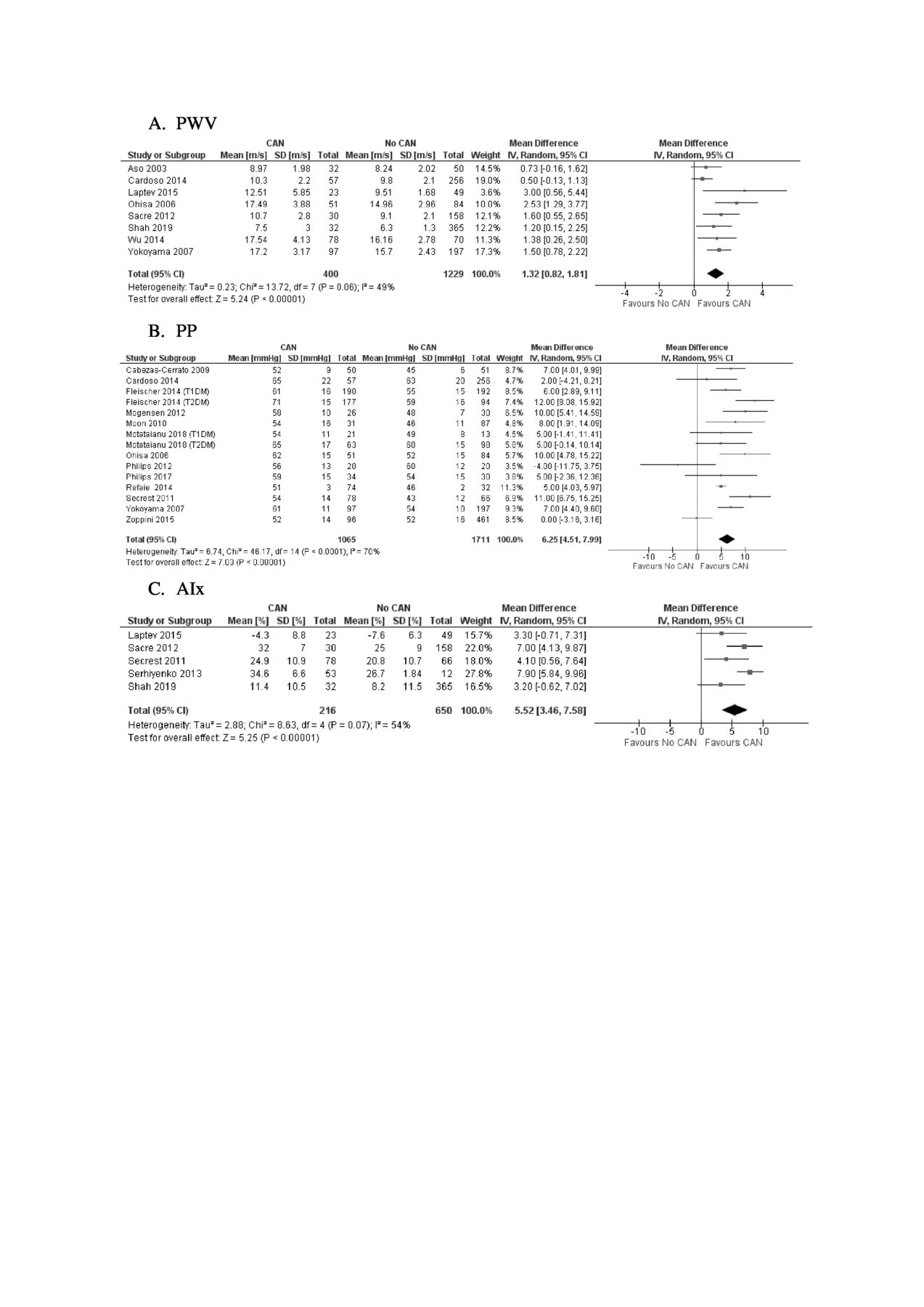
Forest plot of the association of cardiac autonomic neuropathy (CAN) with arterial stiffness. AIx, augmentation index; PP, pulse pressure (mmHg); PWV, pulse wave velocity (m/s); T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Thirteen studies measured arterial stiffness by way of PP, with Fleischer et al38 and Moţăţăianu et al57 reporting separate results for type 1 and type 2 diabetes.31 33 38 53 55 57 60 63–65 69 83 85 There was a total number of 2776 participants: 1065 with CAN and 1711 without CAN (figure 2B). PP was higher in participants with CAN than those without CAN (mean difference: 6.25 mmHg, 95% CI 4.51 to 7.99, p<0.0001).
Five studies measured arterial stiffness by way of AIx with a total number of 866 participants: 216 with CAN and 650 with no CAN47 66 69–71 (figure 2C). AIx was higher in participants with CAN than those with no CAN (mean difference: 5.52%, 95% CI 3.46 to 7.58, p<0.0001).
Association of PN with arterial stiffness
There were 37 studies that investigated the association between PN and arterial stiffness.26–30 32 34 35 37 39 41–43 45 46 48 49 51 52 54 56 59 61 62 67 68 72–77 80–84 Twenty-three studies reported a positive association of PN with at least one measure of arterial stiffness without adjusting for age, sex, diabetes duration, or SBP.27 29 30 32 34 37 39 41 46 48 51 54 59 62 67 68 72 76 77 81–84 Seven other studies did not find a relationship.35 42 52 61 73 74 80 Of those studies that controlled for age, sex, diabetes duration, or SBP, 11 reported a positive association of PN with at least one measure of arterial stiffness.26 28 29 32 43 45 46 62 75 76 82 Seven studies did not find a relationship30 39 49 56 67 77 81 (table 1 and online supplemental table 3).
There were 26 studies with sufficient data to be included in the meta-analysis to estimate the association of PN with arterial stiffness29 30 34 35 37 39 41 42 46 52 59 61 62 67 68 72–77 80–84 (figure 3). Eighteen studies measured arterial stiffness by way of PWV with a total number of 6137 participants: 1634 with PN and 4503 with no PN29 30 34 37 39 46 52 61 62 68 72–77 81 83 (figure 3A). Overall, arterial stiffness, as measured by PWV, was higher in participants with PN than those with no PN (mean difference: 1.22 m/s 95% CI 0.87 to 1.58, p<0.00001).

{kind=link}
{kind=link}
{kind=link}
Forest plot of association of peripheral neuropathy (PN) with arterial stiffness. Forest plot A is stratified by type of PWV. DM, diabetes mellitus; PP, pulse pressure (mmHg); PWV, pulse wave velocity (m/s).
Fourteen studies measured arterial stiffness by way of PP, with Cho et al35 reporting separate results for people with and without diabetes30 34 35 39 41 42 59 67 75 76 80 82–84 (figure 3B). There was a total number of 7909 participants: 2555 with PN and 5354 without PN. PP was higher in participants with PN than without PN (mean difference: 4.59 mmHg, 95% CI 2.96 to 6.22, p<0.00001).
The two longitudinal studies included found arterial stiffness was predictive of PN in people with type 2 diabetes. That is, Cardoso et al32 reported that increased aortic stiffness (carotid-femoral PWV≥10 m/s) was associated with new PN or a progression in PN over a median follow-up period of 6.2 years (incidence rate ratio: 2.04, 95% CI 1.28 to 3.23) and Alves-Cabratosa et al27 reported that increased aortic stiffness (1.3≤ABI<3) was associated with the development of PN over a median follow-up period of 6.0 years (HR=1.44, 95% CI 1.08 to 1.92; reference group: 1.1≤ABI< 1.3).
Subgroup and sensitivity analysis
There was substantial heterogeneity in relation to CAN when arterial stiffness was measured by way of PP (I2=70%, p<0.0001) and AIx (I2=54%, p=0.07) (figure 2B,C). For PP, heterogeneity may have arisen due to various factors with subgroup analysis suggesting age may have played a role (I2 for subgroup differences=87.7%, p=0.004) (online supplemental figure 1) and meta-regression indicating diabetes duration, diabetes type, sex, and study setting may have also have contributed to heterogeneity (online supplemental table 5).
For AIx, heterogeneity no longer appeared to be substantial when Serhiyenko et al,70 the only study in the analysis which was case-control was removed from the analysis (I2=17%, p<0.00001) (online supplemental figure 2).
There was substantial heterogeneity in relation to PN when arterial stiffness was measured by way of PWV (I2=75%, p<0.00001) and PP (I2=75%, p<0.00001) (figure 3). For PWV, heterogeneity was partially explained by whether PWV was measured centrally (mean difference: 0.88 m/s, 95% CI 0.41 to 1.35, p=0.0003) or peripherally (mean difference: 1.68, 95% CI 1.38 to 1.99, p<0.00001) (I2 for subgroup differences=87.2%, p=0.005) (figure 3A). No heterogeneity was indicated between studies using peripheral measures (I2=0%, p=0.90) with six39 46 73 75 81 83 out of the eight studies employing brachial-ankle PWV. Heterogeneity remained substantial for studies using central measures (I2=81%, p<0.00001) and there appeared to be more variation in the types of central measures used, although at least half of the studies29 34 62 74 76 relied on carotid-femoral PWV. Meta-regression indicated mean SBP, PWV type, and study size may have contributed to the differences in association (online supplemental table 6) but was unable to further explain potential sources of heterogeneity for PP (online supplemental table 7). In respect of both CAN and PN, studies often used differing tests to evaluate a participant’s neuropathy status. This may also have contributed toward heterogeneity but was unable to be investigated as studies could not be placed into sufficiently similar subgroups.
For both CAN and PN, we would not have changed our review conclusions based on sensitivity analyses where we used a fixed effect model, where we excluded Shi et al,72 the only study of low quality, or where we excluded Pek et al62 and Teoh et al,77 which were only reported by way of abstract.
Assessment of bias
As assessed by the NOS, all of the studies, other than Shi et al,72 were of high quality (online supplemental tables 8–10). This was predominantly due to participants with diabetes being assessed as being somewhat representative of people with neuropathy, the review’s wide parameters around the acceptability of measures used to assess arterial stiffness and CAN or PN, and studies controlling for confounders in data analysis. When we investigated meta-analyses of more than 10 studies, there was little evidence of publication bias from funnel plots, nor from Egger’s test (online supplemental figure 3).
Grade assessment
Following the GRADE approach, we are moderately confident the effect estimates for CAN and arterial stiffness measured by PWV, PP, and Alx, as well as the effect estimate for PN and PWV, are correct (ie, the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different). Our confidence that the effect estimate for PN and arterial stiffness measured by PP is correct is low, due to high inconsistency (ie, the true effect may be substantially different from the estimate of effect). Although all outcomes were initially rated as low quality, they were all upgraded to moderate, due to the large magnitude of effect for each outcome, with the association for PN and PP being downgraded due to unexplained heterogeneity (online supplemental table 11).
Discussion
As far as we know, this is the first systematic review and meta-analysis of the association between arterial stiffness and neuropathy. We have shown that arterial stiffness is increased in people with CAN and PN regardless of how arterial stiffness was measured (table 1, online supplemental tables 2 and 3, figures 2 and 3). All but one of the studies, as assessed by NOS, were of high quality (online supplemental tables 8–10) and there was little evidence of reporting bias including publication bias (online supplemental figure 3).
In our meta-analysis, we compensated for potential heterogeneity by using a random-effects model. For CAN, heterogeneity was not evident when arterial stiffness was measured by way of PWV. For PN, subgroup analysis and meta-regression showed a difference between central and peripheral measures of PWV. PWV can be measured at various arterial sites, with varying levels of elasticity and levels of pulsatility, with more peripheral sites resulting in higher PWV values than more central sites.86 Although subgroup analyses for PN showed no heterogeneity for studies that used peripheral measures, remaining heterogeneity for central measures may have reflected variation between studies in the choice of central arterial sites used to assess PWV. We were unable to ascertain any sources of heterogeneity for PP. It is possible, however, as PP can be measured centrally and peripherally, that the site of PP measurement could be a cause of heterogeneity in these studies (figures 2 and 3). As studies investigating CAN and PN often employed differing tests to identify neuropathy status, this may also have contributed to heterogeneity. This source of heterogeneity was unable to be investigated further.
Following our GRADE assessment, we are moderately confident that the effect estimate observed for CAN and arterial stiffness measured by PWV, PP, and AIx, and for PN and arterial stiffness measured by PWV, is correct. Our confidence that the effect estimate observed in studies of arterial stiffness measured by PP and PN was correct, however, is low. This suggests that PWV may be preferable to PP in assessing whether a person’s arterial stiffness is indicative of neuropathy, at least in respect of PN.
Our review suggests increased arterial stiffness may lead to the development of neuropathy, particularly in relation to PN. The direction of causation is supported by Alves-Cabratosa et al27 and Cardoso et al,32 the two cohort studies in the review, which both found an association between increased arterial stiffness at baseline and the future development or progression of PN. The direction is also biologically plausible as arterial stiffness can damage the small vessels that supply blood to the peripheral nerves and nerves surrounding the heart, as it impairs the aortic buffering function which prevents the transmission of harmful pulsatile pressure waves into the microcirculation.10 For CAN, it has been hypothesized that stiffening of the carotid arteries and the aorta may affect the function of stretch-sensitive baroreceptors, which, in turn, impacts on HRV.87
Conversely, neuropathy may increase arterial stiffness as it may lead to calcification of the tunica media of the arterial wall, which, in turn, impacts on vascular tone and vasomotion.36 88 The relationship may also be causal in either direction resulting in a vicious cycle where each condition sustains the other. It also cannot be ruled out that the association seen with arterial stiffness and neuropathy may be non-causal and due only to the sharing of a common pathway. For example, hyperglycemia may result in the formation of advanced glycation end products that result in the stiffening of elastic arteries,89 as well as neural inflammation which may ultimately lead to neuropathy.90
Furthermore, as the data in most of our studies came from patients with diabetes, our results are only generalizable to people with this condition. For people with diabetes, our results suggest that arterial stiffness could potentially be used to identify people at higher risk of neuropathy. This is practical as devices to measure arterial stiffness, including PWV, are increasingly accessible and easy to use. People identified as being at increased risk could then be referred for more accurate diagnostics and provided with preventative measures such as glucose control and lifestyle changes. The reduction of arterial stiffness may well also be a focal point for research investigating therapeutics for the prevention and treatment of neuropathy. This could include exploration of the effectiveness of existing medications which may improve arterial stiffness, such as angiotensin-converting enzyme (ACE) inhibitors and advanced glycation end product (AGE) cross-link breakers.91 Before arterial stiffness can be considered as a tool to combat neuropathy, however, steps first need to be taken to more firmly establish the temporality of the relationship of neuropathy and arterial stiffness, particularly in relation to CAN, where we were unable to locate any cohort studies.
In conclusion, the summary evidence from this review indicates that neuropathy is associated with increased arterial stiffness, particularly when measured by way of PWV. The identification of this modifiable risk factor could assist in the diagnosis of neuropathy and provide new research avenues for the treatment of the latter condition. Further longitudinal research is first required to determine the temporality of the association of arterial stiffness and neuropathy.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AB designed the study, registered the protocol, and searched databases. AB and JS performed the selection of studies with the assistance of RKRS. AB analyzed the data. JS checked the data analysis. AB wrote the manuscript. JS and RKRS critically evaluated the protocol, systematic review, and meta-analysis. All authors reviewed and approved the final manuscript. AB is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.