Article Text

Abstract
Introduction Diabetic foot ulceration (DFU) is a common and challenging complication of diabetes. Risk stratification can guide further management. We aim to evaluate the prognostic performance of bedside tests used for peripheral arterial disease (PAD) diagnosis to predict DFU healing.
Research design and methods Testing for Arterial Disease in Diabetes (TrEAD) was a prospective observational study comparing the diagnostic performance of commonly used tests for PAD diagnosis. We performed a secondary analysis assessing whether these could predict DFU healing. Follow-up was performed prospectively for 12 months. The primary outcome was sensitivity for predicting ulcer healing. Secondary endpoints were specificity, predictive values, and likelihood ratios for ulcer healing.
Results 123 of TrEAD participants with DFU were included. In 12 months, 52.8% of ulcers healed. The best negative diagnostic likelihood ratio (NDLR) was observed for the podiatry ankle duplex scan (PAD-scan) monophasic or biphasic with adverse features(NDLR 0.35, 95% CI 0.14–0.90). The highest positive likelihood ratios were observed for toe brachial pressure index of ≤0.2 (positive diagnostic likelihood ratio (PDLR) 7.67, 95% CI 0.91–64.84) and transcutaneous pressure of oxygen of ≤20 mm Hg (PDLR 2.68, 95% CI 0.54–13.25). Cox proportional hazards modeling demonstrated significantly greater probabilities of healing with triphasic waveforms (HR=2.54, 95% CI 1.23–5.3, p=0.012) and biphasic waveforms with non-adverse features (HR=13.67, 95% CI 4.78–39.1, p<0.001) on PAD-scan.
Conclusions No single test performed well enough to be used in isolation as a prognostic marker for the prediction of DFU healing.
Trial registration number NCT04058626.
- Diabetic Foot
- Peripheral Arterial Disease
- Point-of-Care Systems
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Diabetic foot ulceration (DFU) is a common and challenging complication of diabetes. Risk stratification can guide further management. The clinical utility of the prognostic performance of bedside tests in this patient cohort remains uncertain.
WHAT THIS STUDY ADDS
In this multicenter prospective cohort study, no single test performed well enough to be used in isolation as a prognostic marker for the prediction of DFU healing. The podiatry ankle duplex scan (PAD-scan) was the only test to independently predict ulcer healing at 12 months, but the clinical utility of this finding remains uncertain.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study demonstrates a role of PAD-scans in predicting ulcer healing. However, this test did not have an acceptable trade-off between sensitivity and specificity for the prediction of ulcer healing. As such, further research is required into the role of the PAD-scan in the prognostication of DFU.
Introduction
Diabetic foot ulceration (DFU) is a common, costly, and challenging complication of diabetes mellitus. It is estimated that up to one in four patients with diabetes mellitus develop DFU in their lifetime.1 Even if healing is achieved, DFUs recur in 40% of patients within 1 year.2 This has huge implications as DFUs are associated with a poor quality of life3 and very high rates of mortality and major amputation,4–7 to the extent that DFUs are the leading cause of non-traumatic lower limb amputation.8 9
Peripheral arterial disease (PAD) is a key risk factor in the development of DFU and is also associated with delayed healing, increased risk of infection and subsequent amputation.10 The accurate and timely diagnosis of PAD in patients with DFU is an important aspect of the diabetic foot assessment. However, it is also necessary to evaluate the degree to which PAD may affect the chances of wound healing. This process of risk stratification can inform decisions regarding revascularization, wound management, ulcer prevention strategies, and medical therapy for optimization of cardiovascular risk, potentially facilitating new referral pathways, improvement in clinical outcomes, and substantial healthcare cost savings.
The recent Testing for Arterial Disease in Diabetes (TrEAD) study compared the diagnostic performance of bedside tests for the diagnosis of PAD in diabetes.11 The results demonstrated that the visual waveform assessment is the most accurate11 and cost-effective12 diagnostic modality as compared with commonly used tests. However, the prognostic value of these tests in predicting wound healing remains unclear and has not been subject to a side-by-side comparison in the same group of patients.
This study aimed to determine the prognostic value of ankle brachial pressure index (ABPI), ankle pressure (AP), toe brachial pressure index (TBPI), toe pressure (TP), transcutaneous pressure of oxygen (TcPO2) and ankle visual waveform assessment using point-of-care vascular ultrasound (podiatry ankle duplex scan; PAD-scan) in predicting wound healing at 12 months of follow-up.
Methods
Study design and participants
TrEAD was a prospective observational study comparing the diagnostic performance of commonly used bedside tests for the diagnosis of PAD in people with diabetes as compared with a reference test of a full lower limb duplex ultrasound.11 13 The study was registered on ClinicalTrials.gov registry (NCT04058626). Patients aged 18 years or over with a known history of diabetes presenting to two teaching hospital multidisciplinary diabetic foot clinics in London (center A and center B) were eligible to participate. Of note, both centers are within the same vascular network; with center B as the vascular hub and center A as a spoke site. Standard of care did not vary between both centers otherwise. Patients were excluded if they could not provide informed consent, their PAD status was known on anatomical imaging or if they had undergone vascular intervention within the past year. All participants gave written informed consent to participate and be followed up at 12 months by review of their clinical records. For this analysis, we only included participants who suffered from active DFU at baseline (online supplemental figure S1).
Supplemental material

Likelihood ratio graph. The plotted dots on this graph correspond to the sensitivity and specificity of the respective index test at different thresholds, while the slope of the line connecting the dot to point (1,1) corresponds to the negative diagnostic likelihood ratio (NDLR) and the slope of the line passing through (0,0) corresponds to the positive diagnostic likelihood ratio (PDLR). ABPI, ankle brachial pressure index; PAD-scan, podiatry ankle duplex scan; TBPI, toe brachial pressure index; TcPO2, transcutaneous pressure of oxygen.
Procedures
Full details of study procedures have been described in previous publications.11 13 Briefly, all participants underwent usual clinical care including testing for neuropathy and grading of ulcer severity using the University of Texas Score (if DFU was present).14 15 All patients were treated according to standard of care within a multidisciplinary diabetic foot team, with regular wound care as determined by patient need. All patients received optimal medical therapy as judged by their primary clinician and were suitably offloaded, with appropriate antibiotics prescribed as necessary. Decisions for revascularization as well as the optimal method for revascularization were made following multidisciplinary team discussion.
In the TrEAD study, pulse palpation and six bedside tests (ABPI, TBPI, TcPO2, audible handheld Doppler, visual handheld Doppler and PAD-scan) were evaluated. All bedside tests were performed after a period of acclimatization and in a logical sequence to reduce the chance of influence carrying over from one test to another; tests involving qualitative waveform interpretation were performed first, followed by tests with a quantitative output. All tests were performed by one of two vascular scientists (aside from audible Doppler and pulse palpation which were performed by the clinical team as part of standard care).
For this analysis we have chosen to include PAD-scan as the only method of visual waveform assessment as it demonstrated superior diagnostic performance as compared with audible and visual handheld Doppler. PAD-scan is a focused duplex ultrasound scan of the distal anterior and posterior tibial arteries. It allows for direct visualization of the vessels (using B-mode imaging and color Doppler), followed by sampling of the visual Doppler waveform. Waveforms can be classified as normal (triphasic or biphasic with no adverse features) or abnormal (occlusion, monophasic or biphasic with adverse features); online supplemental figure S2. Adverse features (assessed qualitatively) are defined as slow systolic rise time, spectral broadening, infilling of the spectral window and long diastolic forward flow; online supplemental figure S3. PAD-scan was performed using a portable ultrasound machine (Mindray M7; Shenzhen, China) with a linear 6–14 Hz transducer. All waveforms were sampled from the center of each vessel using a Doppler angle of <60° and optimized for interpretation by adjusting sample volume, sample size, Doppler scale, Doppler gain and wall thump filter settings. Pictures of all PAD-scan waveforms were saved, and 40 of them were randomly selected for assessment by an external blinded vascular scientist to assess interobserver reliability.
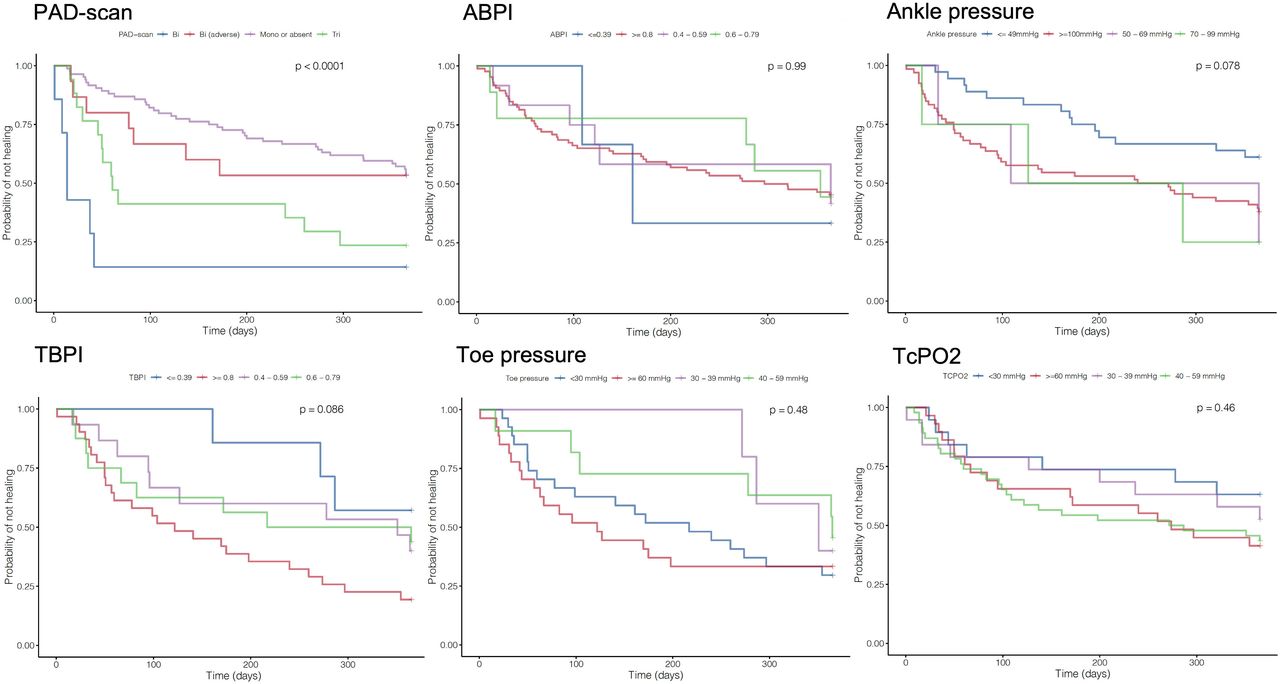
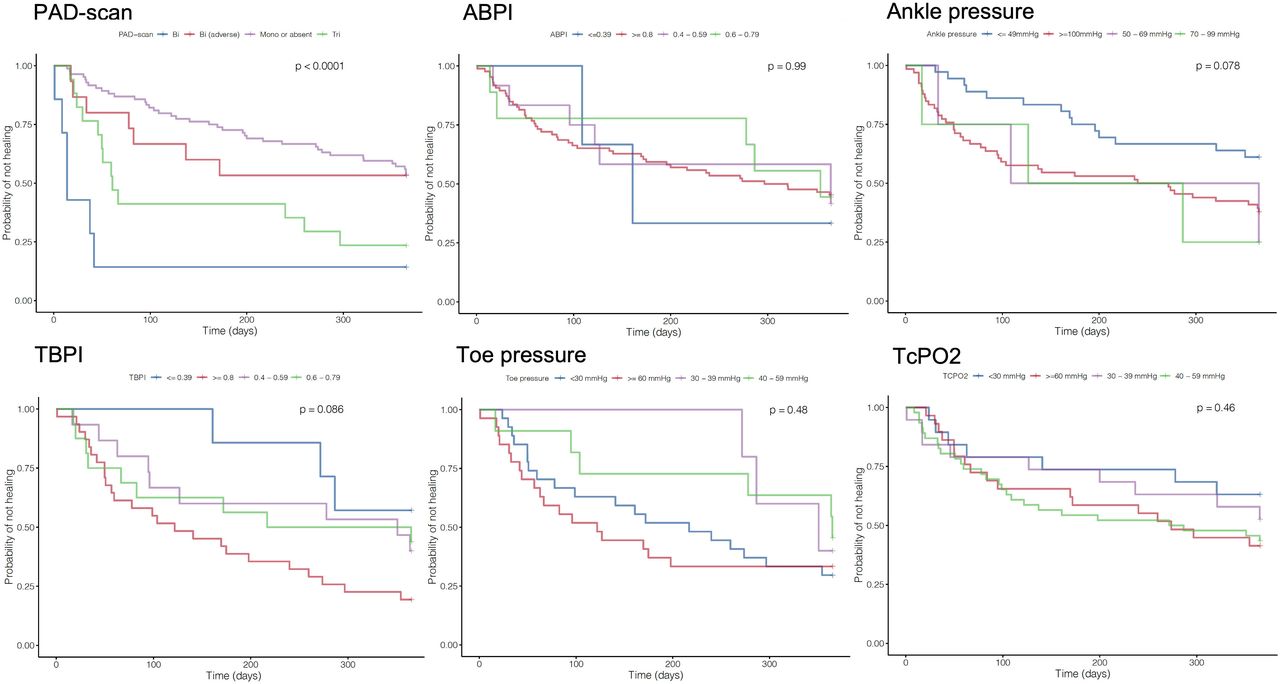
Kaplan-Meier curves for categorical index test results comparing ankle brachial pressure index (ABPI), ankle pressure (AP), toe brachial pressure index (TBPI), toe pressure (TP), transcutaneous pressure of oxygen (TcPO2) and ankle visual waveform assessment using point-of-care vascular ultrasound (podiatry ankle duplex scan; PAD-scan).
{kind=link}
{kind=link}
{kind=link}
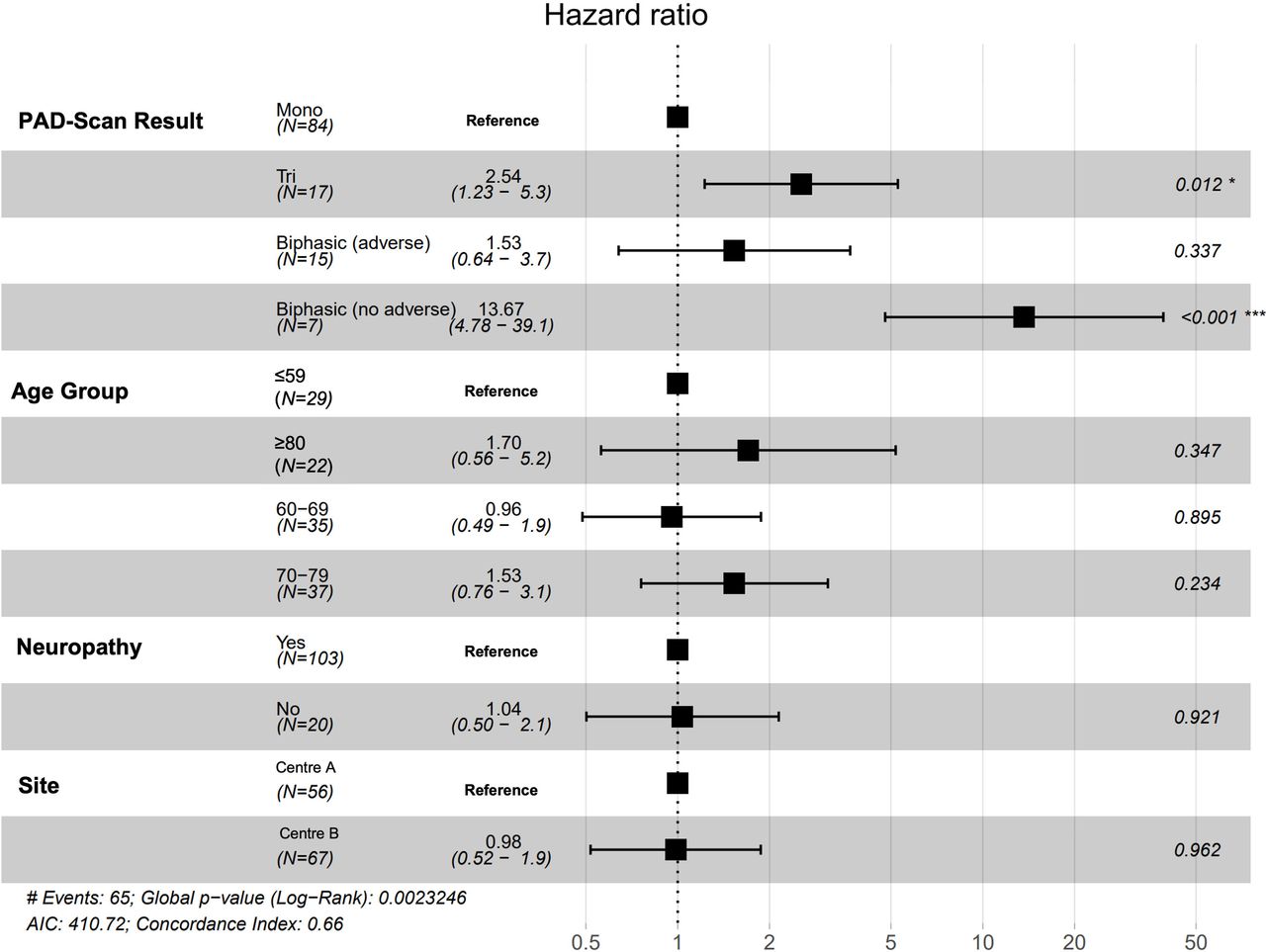
Forest plot output of Cox proportional hazards model for healing. Only ankle visual waveform assessment using point-of-care vascular ultrasound (podiatry ankle duplex scan; PAD-scan) was included as it was the only test to reach statistical significance. AIC denotes Akaike information criterion. * denotes significance with p< 0.05. *** denotes significance with p<0.001.
For this analysis we have also added two variations of existing tests (AP and TP) that were evaluated in the TrEAD study. These two tests are commonly referred to in the wider risk stratification literature and guidance.
ABPI and AP measurements were performed using a sphygmomanometer cuff placed at the ankle and a handheld Doppler device (Dopplex D900 audio-only Doppler, Huntleigh Healthcare, Cardiff) to measure dorsalis pedis and posterior tibial artery systolic pressure. Brachial artery pressures from both arms were taken and the highest reading used to calculate the ABPI.
TBPI and TP measurements were made using the Huntleigh Toe Pressure Kit (Huntleigh Healthcare) employing an infrared sensor placed on the hallux and both index fingers. The highest upper limb reading was used to calculate the TBPI.
TcPO2 measurements were taken from the dorsum of the foot using an automated machine equipped with Clark electrodes (Periflux System 5000; Perimed, Sweden). Dry skin was removed and the skin cleansed before fixing transducers using double-sided adhesive rings and contact liquid. The machine was calibrated prior to every patient assessment. Remembraning of electrodes was carried out on a weekly basis. Electrodes were kept on for 15 min prior to taking readings and measurements were performed away from bony prominences, wounds, superficial vessels, callused skin, edematous and inflamed areas.
Follow-up
Follow-up was performed prospectively for 12 months by regular quarterly review of electronic health records. This method of follow-up was possible as patients with DFU are reviewed regularly, and progress is documented on standardized electronic proformas by clinical care teams. This methodology also made it possible to continue follow-up despite overlap with the first wave of the COVID-19 pandemic.
The primary clinical outcome of interest was ulcer healing. Ulcer healing was defined as complete healing with full skin epithelialization (intact skin). Healing of a minor (below the level of the ankle) or major (above the level of the ankle) amputation wound was not considered as healing in this definition. We also collected data on the occurrence of minor and major amputations, revascularization, non-fatal major adverse cardiovascular events (stroke, myocardial infarction or heart failure requiring hospital admission) and all-cause mortality.
Endpoint
The primary endpoint was sensitivity for predicting healing status at 12 months following initial recruitment. Secondary endpoints of interest were specificity, predictive values and likelihood ratios. Likelihood ratios were interpreted based on their described effect on probability of disease.16 17
Statistical analysis
All statistical analyses were performed using R (V.3.3.1; R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org).
Intergroup statistical comparisons were performed using the χ2 test for categorical data and t-test for continuous data. All p values ≤0.05 were considered significant.
For tests that generate more than one output, that is, tests that involve assessment of more than one vessel (ie, waveform assessment, ABPI and AP), the worse result was used for analysis. For each test, a 2×2 contingency table consisting of true positive, false positive, true negative and false negative values, based on concordance between the index tests and the presence of an unhealed ulcer at 12 months of follow-up, was generated. Sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), positive diagnostic likelihood ratio (PDLR) and negative diagnostic likelihood ratio (NDLR) were calculated for different index test cut-off values using the R package DTComPair.18 19
Likelihood ratios measure a test’s ability to modify pretest probabilities. They indicate how many times more likely a test result is in a patient with the disease (ie, unhealed ulcer at 12 months of follow-up) compared with a person without the disease (ie, healed ulcer at 12 months of follow-up). The NDLR is the ratio between the proportion of the patients having the disease and presenting with a negative test result to the proportion of patients not having the disease and presenting with a negative test result; (1-Sensitivity)/Specificity. Likelihood ratios can be used to estimate the approximate change in probability of the disease. NDLR values less than 0.1 are strongly indicative for the absence of disease and indicate an estimated shift, in prior probability to posterior probability, of at least 45%. Negative likelihood ratio (NLR) values between 0.1 and 0.2 indicate an estimated shift of at least 30%, and values between 0.2 and 0.5 indicate an estimated shift of at least 15%.16 20 The PDLR is the ratio between the proportion of the patients having the disease and presenting with a positive test result to the proportion of patients not having the disease and presenting with a positive test result; Sensitivity/(1-Specificity). PDLR values greater than 1 increase the probability of disease.
Cut-off values used for TBPI, ABPI, TP, AP and TcPO2 were those recommended in current guidelines for risk stratification21–23 (online supplemental table S1). Uncertainty was quantified using 95% CIs.24 Missing data were excluded from analysis.
The Kaplan-Meier method and log-rank test were used to compare probability of not achieving healing between different categorical values for each test with the R packages survival25 and survminer.26 Tests with a statistically significant log-rank test were further evaluated in a Cox proportional hazards model to derive adjusted HRs for healing. Patient demographic variables that were different between the healed and unhealed groups (p values ≤0.1) were selected for inclusion in the Cox proportional hazards model.
Results
Demographics
Results are reported according to the Standards for Reporting of Diagnostic Accuracy Studies checklist (online supplemental table S2). Between 4 March 2019 and 18 October 2019, three hundred and five participants were consecutively enrolled into the TrEAD study across two centers. A total of 123 of these participants presented with active DFU and were therefore included in this follow-up study. Baseline characteristics, stratified by healing at 12 months following recruitment, for participants are included in table 1.
Patient cohort demographics demonstrating statistical significance in comparison of patient age, hospital site and trending toward significance for neuropathy
During the 12-month follow-up 52.8% (n=65) of ulcers healed. There were statistically significant differences in ulcer healing with age and site of care; a healed ulcer was more likely with younger patients (65.3±SD 11.9 vs 71.1±SD 12.5, p=0.01) and with treatment at center B (healed (center A=44.6% vs center B=55.4%, p=0.032). There was also a trend toward significance for neuropathy, with 91.4% of patients who did not heal presenting with neuropathy compared with 76.9% of patients who went on to heal (p=0.054).
Patients with unhealed ulcers had a higher incidence of minor amputation (18.2% vs 3.1%, p=0.015), major amputation (8.6% vs 0%, p=0.05) and mortality (32.8% vs 10.8%, p=0.006) during the 12-month follow-up period. There were no statistically significant differences in the incidence of revascularization (17.2% vs 13.8%, p=0.79) or non-fatal major cardiovascular events (10.3% vs 9.2%, p=1) between the unhealed and healed groups, respectively.
Missing or indeterminate data were observed in 13 (11%) patients for ABPI and AP (pain, n=5; ankle wounds, n=2; incompressible vessels, n=6), 53 (43%) patients for TBPI and TP (previous hallux amputation, n=12; hallux ulceration, n=33; hallux deformity, n=3; tremor, n=2; pain, n=3), and 7 (6%) patients for TcPO2 (technical, n=5; patient abandonment, n=2).
Prognostic performance of tests
Sensitivity, specificity, predictive values and likelihood ratios for different cut-off values of the tests under evaluation are presented in table 2. Tabulated results are available in online supplemental table S2. Overall, no single test demonstrated an acceptable trade-off between sensitivity and specificity; figure 1. The best sensitivities were achieved by TcPO2 (0.96, 95% CI 0.92–1.00), AP (0.94, 95% CI 0.87–1.00) and the PAD-scan (0.93, 95% CI 0.87–1.00). The best specificity was observed for ABPI (0.64, 95% CI 0.52–0.76). The best NLR was observed for PAD-scan (NDLR 0.35) with a threshold of biphasic waveform with adverse features. A negative PAD-scan result can be interpreted as resulting in a small (at least 15%) decrease in likelihood of an unhealed ulcer at 12 months. The highest positive likelihood ratios were observed for TBPI at threshold of ≤0.2 (PDLR 7.67) and TcPO2 at threshold of ≤20 mm Hg (PDLR 2.68). Positive TBPI and TcPO2 results can be interpreted as resulting in a moderate increase (at least 30%) and a small increase (at least 15%) in likelihood of an unhealed ulcer at 12 months, respectively.
Summary of prognostic performance comparing PAD-scan, ABPI, ankle pressure, TBPI, toe pressure and TcPO2
Survival analysis
We used the Kaplan-Meier method and log-rank test to compare the probability of not achieving healing based on categorical values for each test (figure 2). We observed that PAD-scan was the only test to achieve a statistically significant difference (p<0.001) between categorical test values. However, there was a trend toward statistical significance for AP (p=0.078) and TBPI (p=0.086).
Kaplan-Meier survival plots for the PAD-scan demonstrate that groups with normal waveforms (triphasic or biphasic without adverse features) diverge early from those with abnormal waveforms (biphasic with adverse features, monophasic or absent signal), indicating a higher probability of healing within the first 8 weeks. The two groups with abnormal waveforms, particularly those with monophasic signals, achieved healing slowly and were more likely to have a persistent ulcer at 12 months of follow-up.
PAD-scan was the only test to independently predict no healing at 12 months on log-rank test and was therefore included in a Cox proportional hazards model alongside the demographic variable’s hospital site, neuropathy and age in order to derive adjusted HRs for healing (figure 3). The results indicate that triphasic and biphasic waveforms (with no adverse features) increase the probability of healing over the 12-month follow-up period as compared with monophasic waveforms. The HR estimates here should be interpreted with caution given the small sample size and the asymmetry in group size; that is, many patients in the monophasic group and relatively few in other waveform groups.
Discussion
This study aimed to directly compare the prognostic performance of PAD diagnostic tests in the same group of participants. To our knowledge, this study provides the most extensive comparison to date. The major strength of this approach is that any difference in performance can be attributed to the intrinsic properties of the tests as opposed to differences in study methodology.11 27 Moreover, this is the first study to evaluate the prognostic performance of focused point-of-care duplex ultrasound testing (PAD-scan).
Our results indicate that none of the tests evaluated have an acceptable trade-off between sensitivity and specificity for the prediction of ulcer healing. This is consistent with the findings of a previous systematic review by the International Working Group on the Diabetic Foot (IWGDF).28 These findings are also aligned with the complex underlying etiology of DFU, with multiple important predictors of healing, not just PAD.10 ,29 ,30 The National Diabetic Foot Care Audit identified 15 independent variables that influence DFU healing including PAD as well as the size, number of ulcers, sex, duration of diabetes, and acute comorbidities.31 It is important to note that although PAD is the variable with the greatest influence on DFU healing,10 31 other factors must be considered in prognostication.
Our study showed that the PAD-scan was the only test to independently predict ulcer healing at 12 months. After adjusting for confounders, triphasic and biphasic waveforms (with no adverse features) were noted to significantly increase the probability of healing when compared with monophasic and biphasic waveforms with adverse features. To the best of our knowledge, this is the first study to demonstrate this relationship. Arterial spectral waveforms hold important hemodynamic information about the upstream and downstream status of the sampled circulation.11 We have previously demonstrated that assessment of arterial spectral waveform morphology has superior diagnostic performance compared with other tests.11 This study demonstrates a role of PAD-scans in predicting ulcer healing, thus illustrating a further possible utility for the PAD-scan in clinical practice. However, the asymmetry in group size (namely the disproportionately large number of patients with monophasic waveforms and relatively few patients in other waveform groups) mandates cautious interpretation of this finding. Furthermore, as mentioned earlier, this test did not have an acceptable trade-off between sensitivity and specificity for the prediction of ulcer healing. As such, the clinical utility of the PAD-scan to predict ulcer healing in patients with DFU remains uncertain.
Should further support for our findings emerge, we suggest the integration of visual waveform analysis into established DFU classification systems for grading of ischemia. For instance, the validated Wound, Ischemia, Foot Infection score classification system32 currently only grades ischemia according to either TcPO2, ABPI, or TP.14 32–34 We have found that PAD-scan is the only independent predictor of ulcer healing in our cohort. Future risk stratification systems could use PAD-scan results to allow for improved classification, providing further information to the clinician regarding prognostication of a complex disease process which is often oversimplified by current tools.
Furthermore, our results suggest that ABPI, AP, TBPI, TP and TcPO2 do not predict ulcer healing at 12-month follow-up in patients with DFU, although the possibility of a type 2 error in the context of our small sample size remains. Although there was a trend toward significance for TBPI, this did not reach statistical significance for healing prediction and we found that TBPI could not be performed in almost a quarter of patients, thereby limiting its utility in routine clinical practice. This parallels the findings of the original TrEAD study in which these tests performed poorly for the diagnosis of PAD.11 This is also consistent with the findings of a previous systematic review by the IWGDF.28 Furthermore, a high rate of missingness was reported for TBPI and TP (43%) which suggested a limited value for these tests in a high-risk population with history of amputation and active ulceration. However, some discrepancies between our findings and previous studies are noteworthy.
For example, concerning ABPI, our results contradict the findings by Ravidas et al who found that it was a valuable tool for predicting wound healing in patients with diabetic foot ulcers.35 This discrepancy may be attributed to the differences in patient characteristics. Patients in our study were older, ulcer healing times were longer, and the incidence of major and minor amputations was higher. Although baseline characteristics such as the presence of comorbidities and the presence or absence of neuropathy were not reported in their study, it is likely that our patient cohort represents a higher risk population.
In addition, a meta-analysis by Arsenault et al 36 showed that periwound TcPO2 values were independent predictors of failed wound healing. Recently, another group identified TcPO2 as the only test (when compared with ABPI, AP, TBPI and TP) that could independently predict ulcer healing at 24 weeks.37 One explanation is that these studies were not restricted to DFU. Another possible reason for such discrepancy is that TcPO2 measurements were taken from the dorsum of the foot in our study, compared with periwound TcPO2 in other studies. Currently, there is no consensus regarding the exact position of the TcPO2 electrode in clinical practice38 and, to our knowledge, there are no head-to-head comparisons to shed light onto this issue.
One aspect that merits further discussion is the difference in healing rate between both centers. This was unexpected given that both centers were teaching hospitals that provide the same standard of care. One possible explanation is that patients referred to center B (a tertiary vascular center) may have had extensive treatment in the community for their DFU prior to referral, reflecting a discrepancy in times from community referral to clinic appointments between secondary and tertiary centers in the National Health Service.
An important strength in this study is that recruited patients represented a high-risk DFU population. Our results are therefore highly relevant to clinical practice, especially to high-risk diabetic foot clinics. There was a high prevalence of PAD in this patient cohort—this is predictable given the high-risk DFU population and results should therefore be interpreted considering this.
Several limitations, however, merit further discussion. Notably, most tests were performed by two vascular scientists whose experience is not necessarily generalizable.11 Additionally, the high-risk population in this study rendered asymmetry in group size, with a disproportionately low proportion of patients falling in a low-risk category based on test results. This may have influenced our analyses and suggests cautious interpretation of our results. PPV and NPV may have been particularly distorted by the disproportionate prevalence of high-risk patients when compared with the general population.39 The issue is further compounded by the high rate of missing data, especially for TP and TBPI, which further underpowers the analysis. This is further highlighted by a particularly high overall mortality rate in our cohort compared with published literature.40 While the high mortality rate reflects a higher risk population with elevated cardiovascular risk, it may also be attributed to the first wave of the COVID-19 pandemic which coincided with our follow-up. Since many deaths occurred outside of the host institutions, we could not accurately identify the causes of death.
In addition, we acknowledge there was a high risk of overfitting, given the number of events versus covariates. Finally, although many adverse features and indices of waveforms have been identified,41 we have focused on a select few that were deemed easily and quickly extractable through visual inspection and were investigated previously in the TrEAD study.11 However, it remains unclear which features, or combination of features, are the most important for predicting healing.
In conclusion, we aimed to directly compare the prognostic performance of PAD diagnostic tests in the same group of participants. None of the tests evaluated have an acceptable trade-off between sensitivity and specificity for the prediction of ulcer healing. The PAD-scan was the only test to independently predict ulcer healing at 12 months; however, the clinical utility of this finding remains uncertain.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved on 21 December 2017 by London–City & East Research Ethics Committee (REC reference: 17/LO/1447). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Huntleigh Healthcare for providing toe pressure and digital Dopplex devices for the evaluation in this study. We extend our gratitude to the clinical teams and patients for their support and participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The initial TrEAD study received input and advice from a wide range of experts in their respective fields. PN was responsible for this project design and completed the study analysis. SS was responsible for data collection. HE and PN were responsible for initial interpretation, drafting and critical review of the manuscript. All other authors contributed to revisions and critical review of the manuscript. AHD is an NIHR senior investigator. HE accepts full responsibility for the work and/or the conduct of the study, has access to the data, and controlled the decision to publish
Funding The TrEAD study was funded by the Chelsea and Westminster Plus Charity (grant number: 051). PN is funded by a National Institute of Health Research (NIHR) Academic Clinical Lectureship. Infrastructure support for this research was provided by the NIHR Imperial Biomedical Research Centre (BRC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.