Article Text

Abstract
Objective The number of individuals diagnosed with type 2 diabetes mellitus is expected to rise disproportionately in Hispanic/Latino populations. We therefore aimed to assess the efficacy and safety of the dipeptidyl peptidase-4 inhibitor linagliptin specifically in Hispanic/Latino patients with type 2 diabetes mellitus.
Research design and methods Data from 745 patients who self-identified their ethnicity as Hispanic or Latino were pooled from six randomized, placebo-controlled phase 3 trials. Participants received linagliptin (5 mg/day) or placebo as monotherapy, or in combination with other oral antidiabetes drugs for 18 or 24 weeks.
Results The placebo-adjusted mean change (95% CI) in glycated hemoglobin from baseline (mean 8.2%) was –0.63% (–0.77 to –0.48; p<0.0001) at week 18, and –0.58% (–0.74 to –0.42; p<0.0001) at week 24. The placebo-adjusted mean change (95% CI) in fasting plasma glucose from baseline was −11.7 mg/dL (−19.3 to –4.0; p=0.0028) at week 18 and –14.1 mg/dL (–22.0 to –6.3; p=0.0004) at week 24. Hypoglycemia incidence was 17.4% with linagliptin and 21% with placebo. In patients not receiving concomitant sulfonylurea, the hypoglycemia incidence was 10.1% with linagliptin and 19.4% with placebo. The overall incidence of adverse events (AEs), drug-related AEs, and serious AEs with linagliptin was similar to placebo (AEs 67.6% vs 68.9%; drug-related AEs 15.1% vs 18.7%; serious AEs 3.6% vs 3.0%). The mean body weight remained unchanged in both groups.
Conclusions In Hispanic/Latino patients with inadequately controlled type 2 diabetes mellitus, linagliptin provided clinically meaningful improvements in glycemic control without weight gain or increased risk of hypoglycemia.
- A1C
- Hispanic
- Clinical Trial(s)
- Endocrinology Diabetes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The efficacy and safety of a DPP-4 inhibitor, linagliptin, was investigated specifically in Hispanic/Latino patients with type 2 diabetes mellitus.
-
Data were pooled from rigorously conducted randomized controlled trials; however, patients were not randomized specifically for this analysis, and therefore it remains possible that baseline differences between groups could have confounded the results.
-
This pooled analysis is also limited by the relatively short duration (maximum 24 weeks) of the original studies.
Introduction
Type 2 diabetes mellitus (T2DM) represents a large disease burden in Latin American countries and in Hispanic/Latino populations in the USA. In South and Central America, an estimated 8.2% of the adult population had diabetes in 2013. This number is expected to rise by close to 60% over the next 20 years,1 largely due to an obesity epidemic fueled by the lifestyle changes associated with the economic transitions occurring in this region. In the USA, the age-adjusted prevalence of diabetes in Hispanic/Latino adults (estimated at 12.1%) is currently even higher than in South and Central America, with individuals in this population 1.7 times more likely than non-Hispanic/Latino white adults to have been diagnosed with diabetes by a physician.2 Furthermore, this group has an increased risk of diabetes-related complications and mortality.3
The reasons underlying the increased burden of T2DM in Hispanic/Latino populations are complex and involve a combination of genetic, socioeconomic, and cultural factors. For example, in the USA, ethnic disparities are evident in the quality of T2DM care, with Hispanic/Latino patients more frequently diagnosed at a later disease stage and not adequately treated compared with non-Hispanic/Latino patients.4 Furthermore, for a variety of reasons, many Hispanic/Latino patients with T2DM are resistant to initiating insulin therapy or increasing insulin dosage as necessary to achieve glycemic control.5 Some data also suggest the presence of a genetic predisposition toward increased insulin resistance,6–10 which may be further exacerbated by a high prevalence of abdominal obesity in this group.
It is acknowledged that responses to pharmacological therapy may vary across different racial and ethnic groups. The evidence for the efficacy and safety of glucose-lowering agents in Hispanic/Latino populations is scarce and a need for randomized controlled clinical trials exists. Until these studies are initiated, pooled data from the large development programs of new glucose-lowering drugs will provide valuable insights. Linagliptin is an oral, selective dipeptidyl peptidase-4 (DPP-4) inhibitor indicated to improve glycemic control in adults with T2DM.11 Evidence from the linagliptin clinical trial program, as well as subgroup analyses of pooled data, demonstrates that linagliptin improves glycemic control across a range of patient groups.11 Most patients within the linagliptin trials self-reported their ethnicity as non-Hispanic/Latino; however, a large number of Hispanic/Latino patients were included across studies. Pooling of data from these trials was facilitated by comparable study designs and endpoints, and this pooled analysis was therefore undertaken to assess the safety and efficacy of linagliptin in self-identified Hispanic/Latino patients with T2DM from North and South America.
Methods
Patient population
In this retrospective analysis, data were pooled from six randomized, double-blind, placebo-controlled phase 3 trials of linagliptin given once daily as monotherapy or in addition to other glucose-lowering therapies. The pooled analysis included only those patients who self-identified ethnicity as Hispanic/Latino; patients also self-identified race. Two trials were of 18-week duration and four trials were of 24-week duration12–17 (table 1). Patients participated at centers in six North and South American countries: Argentina, Brazil, Canada, Mexico, Peru, and the USA. Eligible patients with T2DM were treated with linagliptin 5 mg once daily or placebo, as monotherapy in treatment-naïve and metformin-intolerant patients (NCT00740051),12 monotherapy in treatment-naïve or previously treated patients (NCT00798161),13 add-on to metformin (NCT00601250),14 add-on to sulfonylurea (NCT00819091),15 add-on to metformin and sulfonylurea (NCT00602472),16 or add-on to basal insulin with or without metformin and/or pioglitazone (NCT00954447; table 1). The difference in patient numbers in the linagliptin and placebo treatment arms is due to the randomizations reflected in table 1. The study design of the linagliptin phase 3 trials included in this retrospective analysis is shown in online supplementary figure S1 and results have been reported previously.12–17 All protocols were approved by relevant local independent ethical committees or Institutional Review Boards, and trials were conducted according to the Declaration of Helsinki and the International Conference on Harmonized Tripartite Guideline for Good Clinical Practice.
Randomized, double-blind, placebo-controlled phase 3 trials of linagliptin included in this pooled analysis
Study endpoints
The primary endpoint of the original studies was change in glycated hemoglobin (HbA1c) from baseline to week 18 or 24. Secondary endpoints were the change in HbA1c from baseline by week over time and the change in fasting plasma glucose (FPG) from baseline by week over time. A meal tolerance test (MTT) was performed in a subgroup of patients in one trial (NCT00601250), and the change in postprandial glucose (PPG) levels after 24 weeks of treatment was also considered a secondary endpoint. Before the MTT, blood was collected for determination of FPG. For the MTT, patients ingested two nutrition bars and 200 mL of diet Ensure Plus, after which, blood was drawn for the determination of 2 h PPG. Other safety-related endpoints were the change in body weight from baseline to week 18 or 24, and the changes from baseline in lipid parameters (including cholesterol, low-density lipoprotein, high-density lipoprotein, and plasma triglycerides), blood pressure, and heart rate. Except for changes in body weight and lipid parameters, the studies of 24-week duration included assessments at week 18. Safety was assessed in terms of the incidence and intensity of adverse events (AEs) up to 18 or 24 weeks. Hypoglycemic episodes that were regarded as AEs were classified by the investigator as asymptomatic, symptomatic, or severe hypoglycemia.
Statistical analyses
Efficacy analyses were performed on the full analysis set (FAS), which comprised all randomized patients who were treated with ≥1 dose of study drug and who had a baseline and ≥1 on-treatment HbA1c measurement. Missing data were imputed using a last observation carried forward approach, including linear interpolation for measurements missing between visits. The changes in mean HbA1c and FPG from baseline to week 18 or 24 were compared between the linagliptin and placebo groups in the pooled population using an analysis of covariance (ANCOVA) model that included continuous baseline HbA1c and fixed effects for treatment, study, and washout (where applicable, patients who were pretreated with non-permitted antidiabetes agents underwent a 4-week washout period, followed by a 2-week placebo run-in period). The model for FPG also included continuous baseline FPG. The OBSMARGIN option for the computation of least squares means coefficients (LSMEANS), which corresponds to the number of observations per treatment, was used in the models without interactions. Interactions of treatment-by-subgroup were included in the models for subgroup analyses, and therefore an equal weighting option was used for the computation of LSMEANS. Subgroup analysis was performed according to baseline HbA1c categories (<7%, ≥7% to <8%, ≥8% to <9% and ≥9%), duration of diabetes categories (≤1 year, >1 to ≤5 years and >5 years), age categories (≤50, 51 to <65, 65 to <75 and ≥75 years), body mass index (BMI) <30 and ≥30 kg/m2, sex, the presence or absence of metabolic syndrome (identified using the International Diabetes Federation definition), and the presence or absence of basal insulin treatment.
The change in 2 h PPG was analyzed for the MTT FAS set using an ANCOVA model that included fixed effects for treatment, washout, continuous baseline HbA1c, and continuous baseline PPG after 2 h as covariates. The MTT FAS set consisted of all patients in the FAS who had a valid MTT at baseline and at least one valid on-treatment MTT. An MTT was considered valid if it had a valid FPG and a valid 2 h PPG value. Safety analyses were performed on the treated set, which comprised all patients who were treated with ≥1 dose of study drug.
Results
Patient disposition and baseline characteristics
In total, 745 Hispanic/Latino patients with T2DM received either linagliptin 5 mg once daily (n=478) or placebo (n=267). The FAS comprised 467 and 264 patients treated with linagliptin and placebo, respectively. The MTT FAS set comprised 28 and 9 patients treated with linagliptin and placebo, respectively. As shown in table 2, patients were generally well matched between treatment arms. The overall population at baseline had a mean (SD) age of 57.2 (9.9) years, mean (SD) HbA1c of 8.24% (0.88), mean (SD) FPG of 159.5 (45.7) mg/dL, and mean (SD) BMI of 30.7 (4.9) kg/m2. Overall, 68.1% of patients receiving linagliptin, and 71.2% of patients receiving placebo, had been diagnosed with T2DM at least 5 years prior to study entry.
Baseline demographic and clinical characteristics for pooled patients
Efficacy
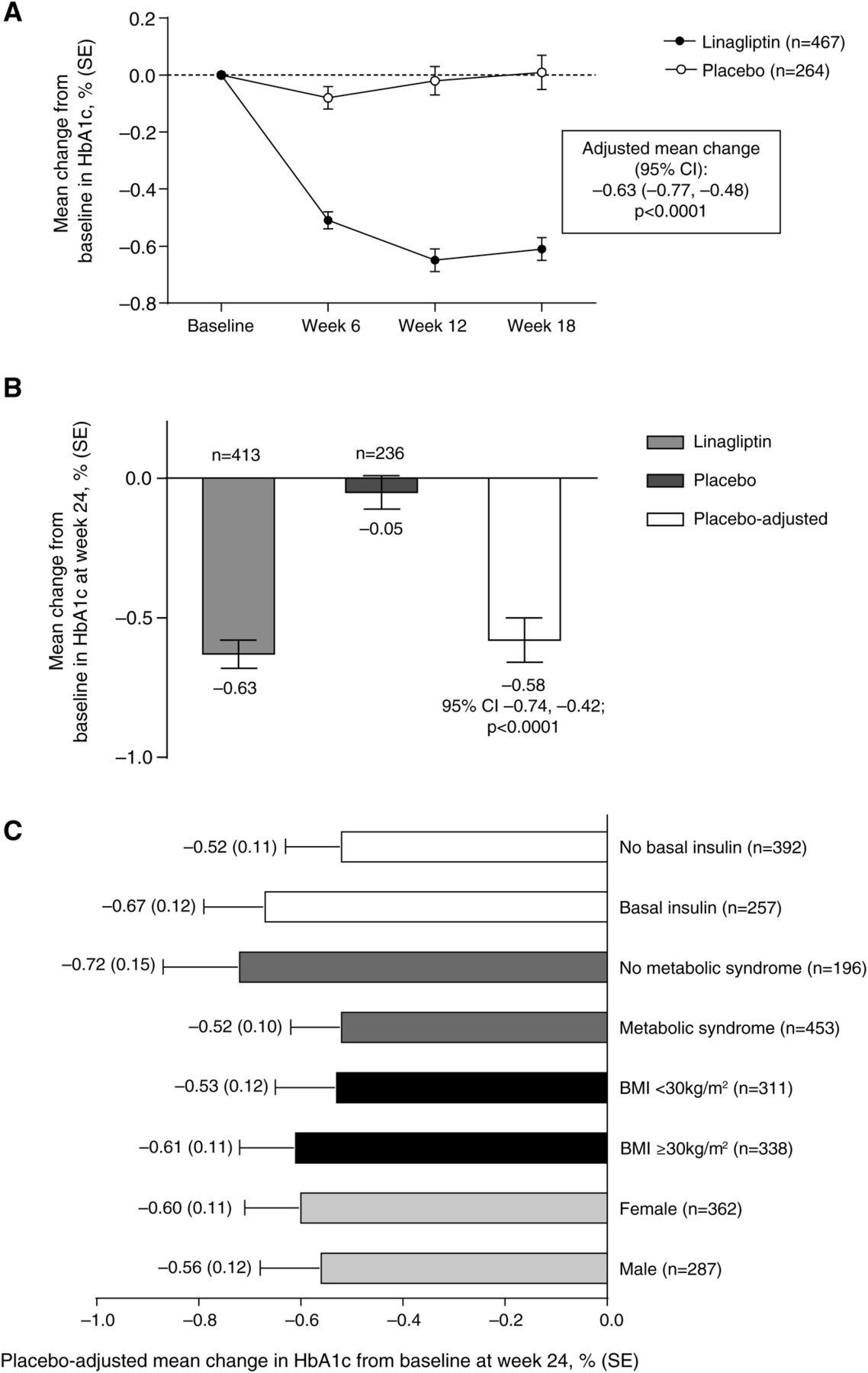
The adjusted mean change (SE) in HbA1c from baseline to week 18 (including data from all six trials) was –0.61% (0.04) in patients receiving linagliptin and 0.01% (0.06) in patients receiving placebo. The placebo-adjusted mean change in HbA1c from baseline to week 18 was –0.63% (95% CI −0.77 to −0.48; p<0.0001; figure 1A). At week 24, the adjusted mean change (SE) in HbA1c was –0.63% (0.05) and –0.05% (0.06) in patients receiving linagliptin and placebo, respectively (including data from four trials). The placebo-adjusted mean change in HbA1c from baseline to week 24 was –0.58% (95% CI −0.74 to −0.42; p<0.0001; figure 1B). Further analyses indicated that this efficacy response was similar across the investigated subgroups, meaning that there were no significant (p<0.05) quantitative subgroup-by-treatment interactions for any of the subgroups, except for age at week 18. The placebo-adjusted mean change in HbA1c from baseline for patients aged ≥75 years was –0.01 (95% CI −0.76 to 0.73) at week 18 and –0.04 (95% CI −0.84 to 0.77) at week 24. However, owing to the small number of patients aged ≥75 years (n=26), the results should be considered with caution. The observed interaction is not regarded as qualitative interaction. The results for a number of different subgroups are presented in figure 1C.
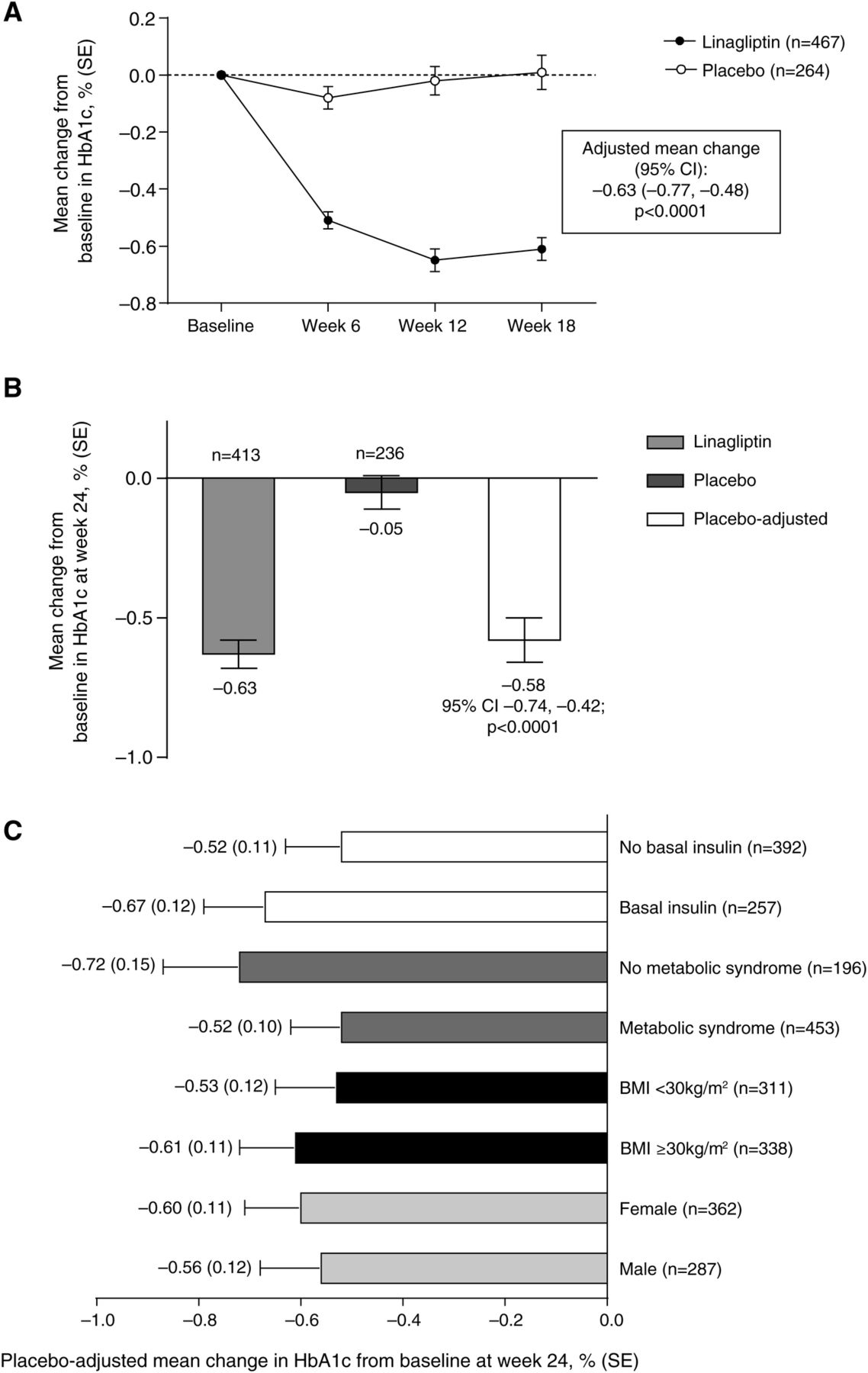
(A) Change from baseline in HbA1c over time (data based on six clinical trials, FAS LOCF). (B) Change from baseline in HbA1c at week 24 (data based on four clinical trials, FAS LOCF). (C) Placebo-adjusted mean change from baseline in HbA1c at week 24 in different subgroups (FAS LOCF). Numbers next to bars indicate placebo-adjusted mean change (SE) value. BMI, body mass index; FAS LOCF, full analysis set last observation carried forward; HbA1c, glycated hemoglobin.
Linagliptin treatment resulted in significant improvements in FPG and PPG compared with placebo. The adjusted mean change (SE) from baseline to week 18 in FPG was –5.5 (2.3) mg/dL and 6.1 (3.1) mg/dL in patients receiving linagliptin and placebo, respectively. The placebo-adjusted mean change in FPG from baseline to week 18 was –11.7 (95% CI −19.3 to −4.0; p=0.0028). The adjusted mean change (SE) from baseline to week 24 in FPG was –6.6 (2.3) mg/dL and 7.5 (3.1) mg/dL in patients receiving linagliptin and placebo, respectively. The placebo-adjusted mean change in FPG from baseline to week 24 was –14.1 mg/dL (95% CI −22.0 to −6.3; p=0.0004). The adjusted mean change (SE) from baseline to week 24 in 2 h PPG was –58.6 (10.9) mg/dL and 16.9 (19.5) mg/dL in patients receiving linagliptin and placebo, respectively. The placebo-adjusted mean change in 2 h PPG from baseline to week 24 was –75.5 mg/dL (95% CI −121.3 to −29.7; p=0.0020), although the limited number of patients available for this analysis should be noted (n=37).
Of the patients who were being treated with basal insulin at baseline (NCT00954447), 82.9% had a time since diagnosis >5 years. The mean (SD) total daily insulin dose (IU) at baseline was 41.50 (23.04) and 43.99 (22.24) for the subgroups of linagliptin and placebo patients receiving basal insulin, respectively. Among these patients, the placebo-adjusted mean change in HbA1c from baseline to week 24 was –0.67% (95% CI −0.90 to −0.44; p<0.0001).
Safety
Overall, AEs and drug-related AEs were experienced by similar proportions of patients in the linagliptin and placebo groups (table 3). Serious drug-related AEs occurred in just 0.4% of patients in each treatment arm. Two patients who received linagliptin experienced a serious AE that was considered to be related to the study drug (one case of bronchial hyperactivity and one case of pancreatitis). A single patient in the linagliptin arm died as a result of cardiorespiratory arrest. The patient, an ex-smoker, had been receiving medication for hypertension and dyslipidemia, and the cause of death was considered to be unrelated to the study drug.
Overall summary of AEs (treated set)
The incidence of investigator-defined hypoglycemia was 17.4% with linagliptin and 21% with placebo. In a subgroup analysis of patients who did not have any background sulfonylurea, the incidence of investigator-defined hypoglycemia in those receiving linagliptin was 10.1%, compared with 19.4% in those receiving placebo (figure 2). Furthermore, in the subgroup of patients receiving insulin, investigator-defined hypoglycemia was comparable in both treatment arms, with events occurring in 20.5% and 26.4% of patients receiving linagliptin and placebo, respectively.

{kind=link}
{kind=link}
Hypoglycemic events (treated set).
Linagliptin and placebo were weight-neutral, with an adjusted mean (SE) change from baseline of 0.26 (0.33) kg and 0.09 (0.49) kg at week 18 for linagliptin and placebo, respectively. The placebo-adjusted mean change in body weight from baseline to week 18 was 0.17 kg (95% CI −1.03 to 1.37; p=0.7782). At week 24, the adjusted mean (SE) change from baseline was 0.37 (0.15) kg for linagliptin and 0.21 (0.21) for placebo. The placebo-adjusted mean change in body weight from baseline to week 24 was 0.16 kg (95% CI −0.37 to 0.69; p=0.5454). Overall, there were no trends of clinical relevance revealed by vital signs and safety laboratory data (see online supplementary table S1). Mean baseline (SE) estimated glomerular filtration rate (eGFR) was 98.65 (1.34) mL/min/1.73 m2 for the linagliptin group, and 95.18 (1.84) mL/min/1.73 m2 for the placebo group. The mean change (SE) in eGFR from baseline at week 18 was –8.54 (2.33) mL/min/1.73 m2 for linagliptin (n=46), and –8.65 (3.09) mL/min/1.73 m2 for placebo (n=22). At week 24, the mean change (SE) in eGFR from baseline was –3.64 (0.92) mL/min/1.73 m2 for linagliptin (n=388), and –4.95 (1.12) mL/min/1.73 m2 for placebo (n=220).
Discussion
The prevalence of T2DM is increasing in Latin American countries,1 and is higher in US ethnic minority populations compared with White populations.2 According to the US Census Bureau, the Hispanic/Latino population is the largest minority group in the USA, representing about 17% of the total population, and is therefore the largest minority group with T2DM in terms of absolute numbers.2 Studies have highlighted ethnic disparities, including higher HbA1c levels, rates of obesity, and metabolic syndrome among Latin American and US Hispanic/Latino patients with diabetes, as well as inadequate access to care.3–10 ,18 ,19 This pooled analysis of data from six randomized, controlled phase 3 trials of up to 24 weeks in duration was performed to assess the glucose-lowering potential and safety of linagliptin in Latin American and US Hispanic/Latino patients with inadequately controlled T2DM. Treatment with oral linagliptin 5 mg once daily led to significant and clinically meaningful improvements in glycemic control as assessed by changes in HbA1c and FPG in a patient population with predominantly long-standing disease (>5 years’ duration), and against a broad background of other commonly used antidiabetes drugs, including insulin. The overall incidence of AEs was similar in patients receiving linagliptin and placebo, as were all other indices of safety including serious AEs, drug-related AEs, and discontinuations due to AEs. Furthermore, treatment with linagliptin was also weight-neutral.
The overall incidence of investigator-defined hypoglycemia was similar for linagliptin and placebo. A similar observation was made when patients with background insulin or without background sulfonylurea were analyzed separately. A low risk for hypoglycemia is clinically relevant, because such events have been associated with a reduction in quality of life in patients with diabetes and a fear of hypoglycemia is common in certain Hispanic/Latino groups.20 This may lead to compensatory behaviors such as decreasing oral antidiabetes medications or insulin doses, which ultimately result in worsening of glycemic control and an increased risk of complications. A fear of hypoglycemia may also contribute to a reluctance to begin insulin therapy, and such ‘psychological insulin resistance’ is particularly common in Hispanic/Latino populations.21 An oral antidiabetes drug with a limited risk of hypoglycemia would therefore enhance therapeutic options for Hispanic/Latino populations, and this study demonstrates the efficacy and safety of linagliptin in this group, as well as its low risk of hypoglycemia.
The efficacy of linagliptin has been demonstrated across ethnic groups, including in Japanese, Chinese, and Black/African American populations.22–24 Although the results of this pooled analysis add to the knowledge of the efficacy and safety profile of linagliptin in an important and previously understudied ethnic population, the findings are limited by the retrospective nature of the analysis. As with all pooled analyses, the patients in this study were not randomized specifically for this analysis, and therefore it remains possible that baseline differences between the groups could have confounded the results; however, baseline values for key efficacy criteria, such as HbA1c or FPG, were similar between the linagliptin and placebo groups. The analysis is also limited by the relatively short-term nature of the original studies, with a maximum duration of 6 months. For linagliptin, longer term (2 years) safety and efficacy data are available for the general T2DM population.25 ,26 A 2-year, head-to-head comparison of add-on linagliptin versus add-on sulfonylurea in patients with T2DM inadequately controlled on metformin showed that linagliptin was non-inferior in lowering HbA1c, but was associated with relative weight loss and significantly less hypoglycemia.26 Further evidence of the efficacy of this combination was provided by a 52-week study demonstrating that initial combination therapy with linagliptin and metformin was superior to metformin monotherapy for reducing HbA1c levels in patients with poor glycemic control, with the additional benefits of no weight gain and a low risk of hypoglycemia.27
Studies suggest that adherence to diabetes treatment is improved through the use of fixed-dose combination (FDC) formulations.28 FDCs are generally competitively priced compared with the same combinations as separate tablets,29 ,30 and therefore may be of particular value in US Hispanic/Latino populations and developing countries from the perspective of overall healthcare costs, as well as individual costs to the patient. In 2012, FDC tablets of linagliptin and metformin were approved for use in adults with T2DM.31 The provision of this drug combination, which has been shown to be efficacious and well tolerated with a low risk of hypoglycemia, in an FDC formulation, is likely to prove a valuable addition to the treatment options available to Hispanic/Latinos.
The cardiovascular safety of linagliptin has been demonstrated in a prespecified meta-analysis of the clinical trial program.32 Further evidence of the beneficial glycemic effects and tolerability of linagliptin are expected when data become available from the ongoing CAROLINA trial (Cardiovascular outcome study of linagliptin versus glimepiride in patients with type 2 diabetes; ClinicalTrials.gov: NCT01243424), an active comparator study investigating the long-term cardiovascular outcomes of linagliptin versus the commonly used sulfonylurea glimepiride.33 Of the 6000 patients included in CAROLINA, about 18% are of Hispanic/Latino ethnicity.33 This study will therefore provide useful insights for the management of T2DM in the Hispanic/Latino population.
The CARMELINA (Cardiovascular safety and renal microvascular outcome with linagliptin in patients with type 2 diabetes mellitus at high vascular risk; Clinical-Trials.gov: NCT01897532) trial recently enrolled its first patient, and is the first investigation of a DPP-4 inhibitor designed and powered to explore cardiovascular and renal microvascular outcomes in at-risk patients. The study, expected to complete in 2018, plans to enroll 8300 patients globally, including participants from Latin American countries. Its renal outcome component may provide particular insight into Hispanic/Latino patients, in whom the rate of end-stage renal disease (ESRD) is 1.5 times greater than that seen in the non-Hispanic/Latino population in the USA.34 ,35 This higher prevalence of ESRD, despite findings of similar prevalence of chronic kidney disease (CKD), indicates a more rapid progression of CKD after onset in Hispanic/Latino patients.35 Evidence suggests that albuminuria may be an important therapeutic target for preventing the progression of CKD.36 ,37 Notably, linagliptin administered in addition to a stable dose of renin–angiotensin–aldosterone system inhibition led to a significant reduction in albuminuria in patients with T2DM and renal dysfunction.38
The efficacy results observed in this pooled analysis of Hispanic/Latino patients are consistent with the findings of individual studies that consider the entire patient population, as well as studies that focus on special populations with T2DM, such as older adults and individuals with severe renal impairment.12–17 ,39 ,40 The lowering in HbA1c of approximately –0.6%, observed in the present analysis, suggests that clinically meaningful improvements in glycemic control can be achieved in Hispanic/Latino patients whether as monotherapy or against a background of common antidiabetes treatments, including insulin. In conclusion, these data demonstrate the glycemic efficacy of linagliptin in Hispanic/Latino patients with inadequately controlled T2DM. Together with the additional benefits of its weight neutrality, low risk of hypoglycemia, and convenient oral dosing (that does not require dose adjustment in patients with renal or hepatic impairment), this study supports the use of linagliptin as a treatment option for this highly burdened population.
Acknowledgments
Writing support was provided by Howard Christian and Ann Kerrigan of Envision Scientific Solutions, which was contracted and compensated by Boehringer Ingelheim Pharmaceuticals Inc (BIPI) for this service.
References
Footnotes
-
Contributors All authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE), were fully responsible for all content and editorial decisions, and were involved at all stages of manuscript development. MM, H-JW, and MvE designed the study. MM conducted the statistical analysis. All authors contributed to interpretation of the data and provided final approval for publication. JAD is the study guarantor.
-
Funding This work was supported by BIPI.
-
Competing interests JAD has received consulting/advisory fees from Boehringer Ingelheim. RL is a scientific advisor to Boehringer Ingelheim, and RBA has served on Boehringer Ingelheim advisory boards. RBA and RL have received speaker's bureau fees from Boehringer Ingelheim. MM, H-JW, and MvE are employees of Boehringer Ingelheim.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.