Article Text

Abstract
Objective To use admission inpatient glycated hemoglobin (HbA1c) testing to help investigate the prevalence of unrecognized diabetes, the cumulative prevalence of unrecognized and known diabetes, and the prevalence of poor glycemic control in both. Moreover, we aimed to determine the 6-month outcomes for these patients. Finally, we aimed to assess the independent association of diabetes with these outcomes.
Research, design, and methods Prospective observational cohort study conducted in a tertiary hospital in Melbourne, Australia.
Patients A cohort of 5082 inpatients ≥54 years admitted between July 2013 and January 2014 underwent HbA1c measurement. A previous diagnosis of diabetes was obtained from the hospital medical record. Patient follow-up was extended to 6 months.
Results The prevalence of diabetes (known and unrecognized) was 34%. In particular, we identified that unrecognized but HbA1c-confirmed diabetes in 271 (5%, 95% CI 4.7% to 6.0%) patients, previously known diabetes in 1452 (29%, 95% CI 27.3% to 29.8%) patients; no diabetes in 3359 (66%, 95% CI 64.8–67.4%) patients. Overall 17% (95% CI 15.3% to 18.9%) of patients with an HbA1c of >6.5% had an HbA1c ≥8.5%. After adjusting for age, gender, Charlson Index score, estimated glomerular filtration rate, and hemoglobin levels, with admission unit treated as a random effect, patients with previously known diabetes had lower 6-month mortality (OR 0.69, 95% CI 0.56 to 0.87, p=0.001). However, there were no significant differences in proportions of intensive care unit admission, mechanical ventilation or readmission within 6 months between the 3 groups.
Conclusions Approximately one-third of all inpatients ≥54 years of age admitted to hospital have diabetes of which about 1 in 6 was previously unrecognized. Moreover, poor glycemic control was common. Proportions of intensive care unit admission, mechanical ventilation, or readmission were similar between the groups. Finally, diabetes was independently associated with lower 6-month mortality.
- HbA1c
- Hospital Care
- Quality Improvement
- Testing
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Approximately one-third of all inpatients ≥54 years have diabetes with 5% of all inpatients ≥54 are previously unrecognized with diabetes.
Routine inpatient glycated hemoglobin testing to measure glycemic status utilizes a currently missed opportunity to identify patients with previously unrecognized diabetes and poor glycemic control.
We demonstrate a feasible method of conducting such an initiative, utilizing electronic health infrastructure to identify patients at greatest risk for prioritization for review.
Introduction
Diabetes mellitus poses a progressive challenge for health services worldwide. Recent Australian data suggest that the rate of diabetes in hospitalized patients rises markedly above the age of 54 years.1 Current estimates suggest that up to 11% of diabetes in hospitalized patients remain unrecognized.1 Thus, routine measurement of glycated hemoglobin (HbA1c) in hospitalized patients provides an opportunity to identify patients with unrecognized diabetes.
Given a higher prevalence of diabetes in the hospital setting, hospitalization represents a currently missed opportunity to identify patients with unrecognized diabetes as well as those with poor diabetes control. Identification of inpatients with diabetes is hampered by confounding factors such as stress hyperglycemia, use of glucocorticoid medications, and fasting requirements.2 The International Expert Committee recommends HbA1c as the preferred test for the diabetes detection with a diagnostic threshold of 6.5% (48 mmol/mol).3 Advantages of HbA1c testing compared with glucose testing include lower biological variability, less preanalytic instability, no requirement for fasting, and less effects from stress hyperglycemia.4
Several observational studies demonstrate increased mortality and morbidity associated with hyperglycemia.5 ,6 Adverse outcomes associated with hyperglycemia are reported in coronary care,7 stroke,8 and intensive care unit (ICU)6 settings with proposed mechanisms including susceptibility to sepsis,9 poor wound healing,10 and increased thrombosis.11 However, other studies report no increase in risk and yet others report lower mortality.12–14
Routine HbA1c measurement to aid inpatient clinical care is not current practice. We hypothesized that information technology tools such as Cerner Millennium clinical information system will aid the identification of patients with unrecognized diabetes and those with poor glycemic control. We also aimed to determine the clinical characteristics and outcomes of patients with known and unrecognized diabetes as well as those with poor glycemic control, defined as HbA1c ≥8.5% (69 mmol/mol), as part of the Diabetes Discovery Initiative at Austin Health.
Methods
All patients admitted to Austin Health, a tertiary teaching hospital, during the study period (17 July 2013 to 17 January 2014) were eligible for this prospective observational study. Owing to known high prevalence of inpatient diabetes, during the 6-month study period, all inpatients above age 54 years underwent HbA1c testing on admission coordinated via an automated order through Cerner Millennium® as part of routine clinical care. If the criteria, age ≥54 years, acute admission, no HbA1c recorded within 3 months (figure 1), were satisfied, an automatic request for HbA1c testing was generated. All HbA1c results were reported via Cerner and were accessible to patients’ treating physicians. As part of the Diabetes Discovery Initiative, all patients with HbA1c ≥8.5% (69 mmol/mol) were reviewed by endocrinology registrars to intensify diabetes treatment, screen for complications, and devise plans for further management as required. A paragraph describing the HbA1c result and its interpretation was automatically inserted into each discharge summary to patients’ local doctors. As part of the Diabetes Discovery Initiative, hospital medical and nursing staff were educated on the use of HbA1c in the identification and management of diabetes.

Criteria for automatic generation of glycated hemoglobin (HbA1c) request on Cerner.
EDTA whole blood was collected from each patient for analysis. HbA1c was measured by turbidimetric inhibition immunoassay on Cobas Integra 800 (Roche Diagnostics, Mannheim, Germany). The assay is standardized to The International Federation of Clinical Chemistry (IFCC) reference method with a between run coefficient of variation 2.5% for HbA1c 5.6% (30 mmol/mol) and 1.5% for HbA1c 9.7% (83 mmol/mol).
Prespecified demographic data, clinical characteristics (symptoms, medical history, medications, treatments administered), outcome of episode (length of stay, ICU admission, mechanical ventilation, mortality within 6 months, and readmission at 6 months), and biochemical laboratory values (HbA1c levels, hemoglobin (Hb), serum creatinine, estimated glomerular filtration rate (eGFR), and fasting lipid profile) were extracted from medical records and hospital databases. Approximately 20% of the records were reviewed by clinicians to verify accuracy of data extraction algorithms. For statistical accuracy, data from treating units with small numbers of inpatients were amalgamated. Patients with multiple admissions were assessed on data from the first admission.
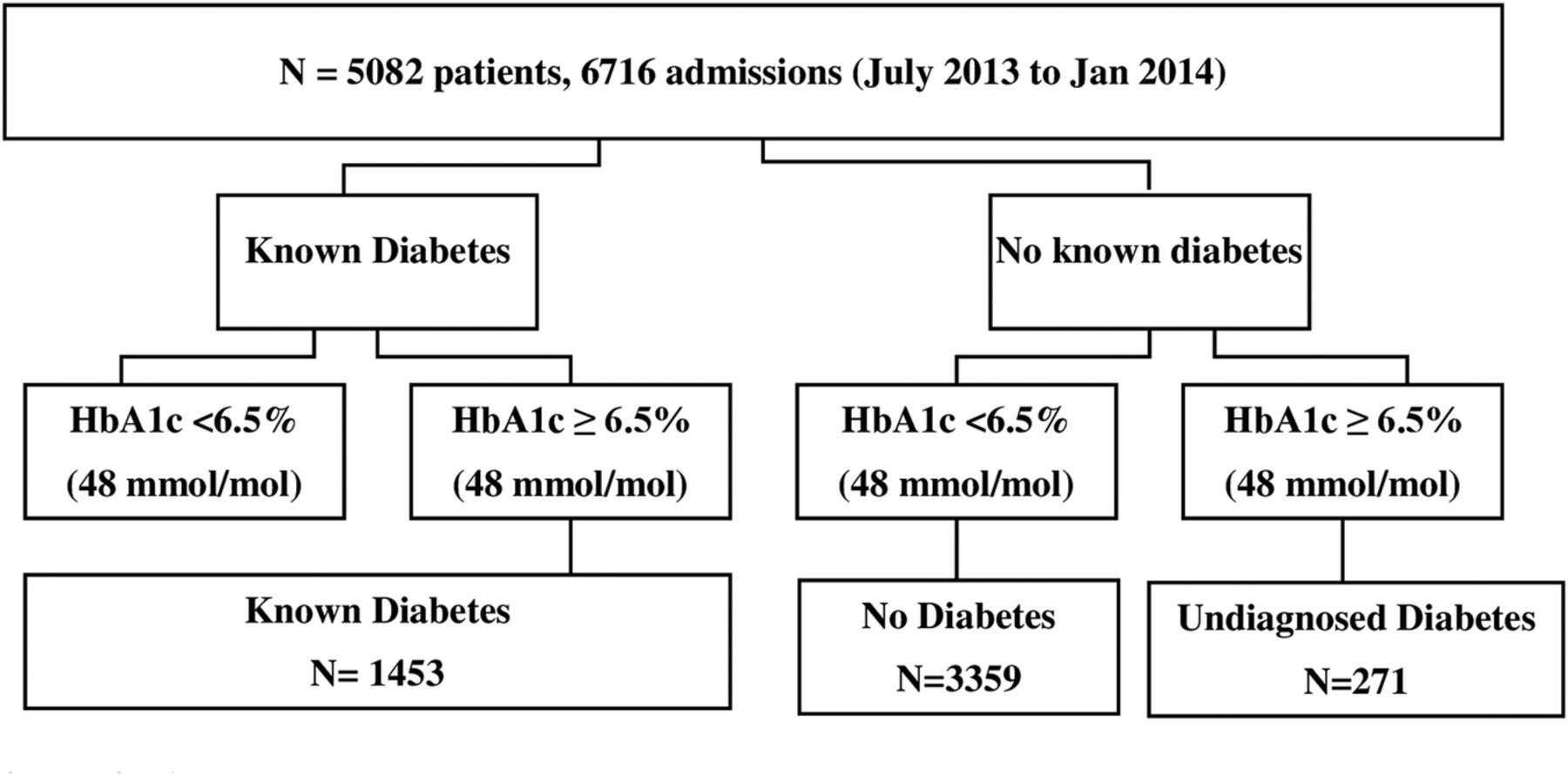
Patients were categorized into three groups according to medical record and HbA1c (figure 2). ‘No diabetes’ defined as no diabetes diagnosis in the medical record and HbA1c <6.5% (48 mmol/mol), ‘Known diabetes’ where a diabetes diagnosis has been documented in the medical record (International Classification of Disease 10-Australian modification codes E10-14), and ‘unrecognized diabetes’ where no known diabetes diagnosis has previously been made according to the medical record and HbA1c ≥6.5% (48 mmol/mol).
Study profile (HbA1c, glycated hemoglobin).
Information regarding comorbidities was obtained from each patient's medical record to calculate a Charlson Index score. This validated method of weighting the impact of chronic disease assigns each chronic condition a score of 1, 2, 3, or 6, depending on severity and impact on mortality.15 Charlson Index scores were determined from ICD 10 AM codes using the previously validated ICD 10 adaptation of the Charlson Index.16 As diabetes status was considered a separate variable, the Charlson score was calculated without inclusion of diabetes. Mortality was determined if patients had died during the admission or if the hospital had been notified of the death during the 6-month study period. Readmission within 6 months was defined as readmission to this hospital during the 6-month study period.
Patient groups were compared with respect to baseline characteristics, length of stay, ICU admission, mortality within 6 months, mechanical ventilation, and readmission at 6 months. Given that these indices were not normally distributed, these continuous explanatory variables were summarized as medians with IQRs and analyzed with the use of Wilcoxon tests or Kruskal-Wallis tests as appropriate. Categorical explanatory variables were reported as percentages and analyzed with χ2 tests or Fisher's exact test as appropriate. Because of the hierarchical nature of the data where individual patient outcomes are ‘nested’ within the treating units, association between diabetes status (yes/no) and outcomes adjusted for age, gender, Charlson score (excluding diabetes component), eGFR (Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI) eGFR17), and Hb levels were investigated using an appropriate random-effect regression model with treating unit treated as a random effect. Multivariable analyses were based on negative binomial regression for the length of stay calculations and on logistic regression for binary outcomes. All p values were calculated from two-tailed tests of statistical significance with a type 1 error rate of 5%. All analyses were performed with Stata software V.13.0 (StataCorp). We also conducted exploratory subgroup analysis of these outcomes in patients with diabetes (known and unrecognized) with/without chronic kidney disease (eGFR <45 and <60 mL/min/1.73 m2) and in patients with diabetes (known and unrecognized) with/without anemia (Hb <100 g/L).
Results
We studied 5082 patients (6716 admissions). The prevalence of diabetes (known and unrecognized) was 34%. In particular, we identified that unrecognized but HbA1c-confirmed diabetes in 271 (5.3%, 95% CI 4.7% to 6.0%) patients, previously known diabetes in 1452 (29%, 95% CI 27.3% to 29.8%) patients; no diabetes in 3359 (66%, 95% CI 64.8% to 67.4%) patients (figure 3).

{kind=link}
{kind=link}
{kind=link}
The prevalence of known, unrecognized and no diabetes in inpatients ≥54 years.
The baseline characteristics of patients with previously known diabetes, previously unrecognized diabetes, and without diabetes are presented in table 1. Patients with diabetes were more likely to be admitted to medical units and had a significantly lower eGFR.
Patient characteristics by diabetes status
Of the patients with diabetes, 17% had HbA1c ≥8.5% (69 mmol/mol). Median age of patients in this group was greater than those with diabetes and HbA1c <8.5% (69 mmol/qmol; 74 vs 70 years, p<0.01). There were no other significant differences between patients with diabetes with HbA1c ≥8.5% (69 mmol/mol) and patients with diabetes with HbA1c <8.5% (69 mmol/mol) with respect to the variables studied. Approximately one in six patients with diabetes demonstrated poor glycemic control with a HbA1c ≥8.5% (69 mmol/mol).
Patient outcomes
The unadjusted 6-month patient outcomes are presented in table 2. These unadjusted data highlight that patients with diabetes were more likely to be readmitted to hospital within 6 months of their index presentation.
Unadjusted patient outcomes by diabetes status
Association of diabetes with outcomes
The independent association of diabetes with key outcomes is presented in table 3.
Association of diabetes with outcome
After adjusting for age, gender, Charlson Index score, eGFR, and Hb levels, with admission unit treated as a random effect, patients with previously known diabetes had lower 6-month mortality (OR 0.69, 95% CI 0.56 to 0.87, p=0.001, table 3). There was no difference in mortality between patients with unrecognized diabetes and those with no diabetes. Furthermore, following adjustments for age, gender, Charlson Index score, eGFR, and Hb levels, there were no significant differences in proportions of ICU admission, mechanical ventilation, or readmission within 6 months between the three groups.
Discussion
The current study uses information technology systems to examine the prevalence of diabetes (known and unrecognized) in all inpatients above age 54 years, in real time. In this cohort of 5082 patients, aged 54 years and above, 5% had unrecognized diabetes and 29% had pre-existing diabetes. Furthermore, almost 6% of all inpatients aged ≥54 years had poor glycemic control with HbA1c ≥8.5% (69 mmol/mol). After adjusting for age, gender, Charlson Index score, eGFR, and Hb levels, with admission unit treated as a random effect, patients with previously known diabetes had lower 6-month mortality. However, there were no significant differences in proportions of ICU admission, mechanical ventilation, or readmission within 6 months between the three groups.
The use of fasting plasma glucose for diabetes diagnosis is limited given the high prevalence of stress hyperglycemia and frequent use of glucocorticoid medications in inpatients18; oral glucose tolerance test for inpatient diabetes screening is resource intensive and impractical.19 HbA1c testing is superior for the inpatient diagnosis of diabetes1; however, sensitivity may be lowered by significant renal impairment, anemia, blood transfusions, and hemoglobinopathies, while prolonged stress hyperglycemia may produce false-positive results.20 ,21 These conditions are unlikely to be in numbers large enough to affect overall screening.22 HbA1c has the advantage of aiding both diabetes diagnosis and management.
Following adjustments for age, gender, Charlson Index score, eGFR, and Hb levels, with admission unit treated as a random effect, patients with previously known diabetes had lower 6-month mortality. There was no difference in mortality between patients with unrecognized diabetes and those with no diabetes. There is variation in the literature regarding diabetes being an independent predictor of mortality in inpatients. Vincent et al12 found no significant difference in mortality in the intensive care setting between patients with a history of insulin-requiring diabetes mellitus. Diabetes was associated with increased mortality in patients with community-acquired pneumonia in one study23; however, there was no association between diabetes and increased mortality in patients with community-acquired bacteremia,13 severe sepsis,12 trauma, burns, and acute cardiac failure.24 However, in the aforementioned studies, the presence of diabetes was determined from clinical history. In the current study, HbA1c as well as clinical records was used to identify patients with diabetes. In patients with congestive cardiac failure, those HbA1c <6.4% (46 mmol/mol) had higher all-cause mortality compared with those with HbA1c ≥8.7% (72 mmol/mol).25 Other studies have found a U-shaped association between HbA1c and mortality, with the lowest HR at HbA1c 7.5% (58 mmol/mol).26 The observational nature of this study means that we are unable to infer causality regarding the differences observed between groups. As yet we have no explanation for this surprising finding.
Electronic medical records and clinical information systems are increasingly utilized to identify and manage patients at risk. Examples include chronic kidney disease27 and colon cancer28 ,29 screening; ‘sepsis sniffers’ are an automated tool for the early identification and treatment of inpatients with acute sepsis.30 To our knowledge, the current study is the first reported example of large-scale programme to identify and treat patients with unrecognized and poorly controlled diabetes in an acute inpatient setting. In this large study, we investigated the clinical utility of routine HbA1c measurements in hospital inpatients. We demonstrate the use of electronic systems for aiding clinical care and early biochemical identification of a chronic disease; specifically using a combination of HbA1c results and the hospital medical records, we have demonstrated a method for the identification of patients with previously unrecognized diabetes as well as those with poorly controlled diabetes. This utilizes a previously missed opportunity of engaging with patients who are in hospital for non-diabetes-related conditions. Previous studies suggest that many patients with unrecognized diabetes do not have general practitioners.1 Interestingly, general practitioner rates were similar in the group of patients with unrecognized diabetes compared with those with no diabetes. This highlights the role of determining the glycemic status of inpatients for identifying patients who may otherwise remain unrecognized (and untreated). The utility of early diagnosis of diabetes in preventing diabetes-related complications depends on communicating this information to patients’ local doctors. One of the benefits of using electronic medical record to identify these patients is that electronic discharge summary can be used to communicate relevant information to patients’ local doctors automatically.
The prevalence of unrecognized diabetes has previously been reported to be 11% in a study of 2360 patients in another state of Australia in 2011.1 The lower proportion of unrecognized diabetes in our study may reflect increased diabetes awareness or age, ethnic, and socioeconomic differences between the study populations. Unlike those published previously,8 ,31 following adjustments for age, gender, Charlson Index score, eGFR, and Hb levels, with admission unit treated as a random effect, we did not observe an increase in length of stay associated with diabetes. Furthermore, we used median length of stay as an outcome variable which more accurately represents the non-parametric nature of this variable.
Diabetes and comorbidity data were obtained from medical record coding which may underestimate true prevalence. However, manual audits of the 20% of the sample found similar results. As mortality was determined by composite of in hospital mortality as well as patients’ deaths notified to the hospital, it is possible that some deaths were unrecorded. The short follow-up period means that we were unable to demonstrate any benefits of identification of unrecognized diabetes diagnosis on long-term complications. Given the 6-month study period, the effect of seasonal variation was not analyzed. This study investigated patients aged ≥54 years, as previous data suggested that the prevalence of unrecognized diabetes would be significantly greater in older patients32; however, it would be interesting to see if these results would be affected by the inclusion of younger patients. The observational nature of this study means that we are unable to infer causality regarding the differences observed between groups.
Conclusions
Approximately one third of all inpatients ≥54 years have diabetes with 5% of all inpatients ≥54 are previously undiagnosed with diabetes. Routine inpatient HbA1c testing to measure glycaemic status utilises a currently missed opportunity to identify patients with newly diagnosed diabetes and poor glycaemic control. We demonstrate a feasible method of conducting such an initiative, utilising electronic health infrastructure to identify patients at greatest risk for prioritisation for review. The impact of early identification and treatment of poor glycaemic control on patient outcomes requires further study.
References
Footnotes
JDZ and EIE contributed equally.
Acknowledgements The authors are grateful to Peter Davey (Department of Administrative informatics, Austin Health) and Harvey Sutcliffe (Pathology IT Services, Austin Health) for assistance with data retrieval and information technology support.
Contributors NN was involved in literature review and synthesis, data acquisition, detailed data analysis, critical discussion, drafting and revision of the manuscript. HN was involved in critical discussion, data collection, detailed data analysis and assisted revision of the manuscript. LC conducted statistical analysis, analysis and input into the manuscript. AK was involved in critical discussion, drafting and revision of the manuscript. NP contributed to experimental design and data collection. GKH was involved in inception of decision support programmes in the Electronic Health Records projects, review of manuscript, coordinated project team, critical discussion, drafting and revision of the manuscript. EO-J, JW and JR contributed to experimental design, assistance with decision support programmes in the Electronic Health Records projects. VS contributed to experimental design. RB was involved in critical discussion, drafting and revision of the manuscript. QL was involved in critical discussion and data acquisition. NC contributed to experimental design and data collection. RR was involved in data acquisition and analysis. DJ and STB were involved in critical discussion, drafting and revision of the manuscript. JDZ was involved in project conception, analysis of the manuscript, supervision of the project. EIE was involved in project conception, experimental design, analysis of the manuscript, supervision of the project. All authors fulfilled the roles required for authorship including involvement in conception, design, acquisition, analysis and interpretation of data and drafting and revising article and final approval. EIE is the guarantor.
Competing interests None declared.
Ethics approval This study was approved as an audit by the Austin Health Human Research Ethics Committee (LNR/14/Austin/82).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.