Article Text

Abstract
Objective We assessed the efficacy of routine glycated hemoglobin (HbA1c) testing to detect undiagnosed diabetes and prediabetes in an urban Australian public hospital emergency department (ED) located in an area of high diabetes prevalence.
Methods Over 6 weeks, all patients undergoing blood sampling in the ED had their random blood glucose measured. If ≥5.5 mmol/L (99 mg/dL), HbA1c was measured on the same sample. HbA1c levels ≥6.5% (48 mmol/mol) and 5.7–6.4% (39–46 mmol/mol) were diagnostic of diabetes and prediabetes, respectively. Hospital records were reviewed to identify patients with previously diagnosed diabetes.
Results Among 4580 presentations, 2652 had blood sampled of which 1267 samples had HbA1c measured. Of these, 487 (38.4%) had diabetes (either HbA1c≥6.5% or a prior diagnosis), and a further 347 (27.4%) had prediabetes. Among those with diabetes, 32.2% were previously undiagnosed.
Conclusions Routine HbA1c testing in the ED identifies a large number of people with undiagnosed diabetes and prediabetes, and provides an opportunity to improve their care.
- HbA1c
- Emergency Room
- Diagnosis
- Pre-Diabetes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
We demonstrate that glycated hemoglobin measurement undertaken in the setting of an emergency department is an effective and feasible means of finding cases of diabetes and prediabetes particularly in an area known to have a high prevalence of diabetes.
Approximately a third of patients tested were previously unaware that they had diabetes.
Earlier detection of prediabetes provides an opportunity to introduce measures that may prevent progression to diabetes.
Introduction
Diabetes has traditionally been diagnosed by the 75 g oral glucose tolerance test (75 g OGTT), but recent adoption of glycated hemoglobin (HbA1c) as a diagnostic tool for high-risk individuals has simplified the diagnostic process.1–3 Underdetection remains a major barrier to prevention of diabetes and associated complications. Targeted HbA1c testing of high-risk populations could enhance the detection of diabetes and prediabetes. The purpose of this study was to test this hypothesis in patients presenting to a hospital emergency department (ED).
Methods
The study was conducted over 6 weeks in the ED of Blacktown-Mt Druitt Hospital, located in the western suburbs of Sydney, Australia. This is an area of high diabetes prevalence.4 Opportunistic blood glucose measurements were undertaken in all non-pregnant individuals ≥16 years of age who had blood collected after presenting to the ED, irrespective of the presenting problem. HbA1c was automatically measured if the random glucose was ≥5.5 mmol/L (99 mg/dL). This cut-off level was chosen based on another Australian ED study5 and a substudy that we undertook (unpublished). In this substudy, HbA1c measurements were undertaken in 50 patients presenting through ED with random glucose levels <5.5 mmol/L (<99 mg/dL). Only three individuals were noted to have HbA1c levels ≥6.5% and the glucose cut-off of ≥5.5 mmol/L (99 mg/dL) was deemed reasonable.
In patients who re-presented within the study period, HbA1c testing was undertaken only on the first presentation. As per American Diabetes Association recommendations, diabetes was diagnosed if HbA1c≥6.5% (48 mmol/mol) and prediabetes was diagnosed if HbA1c was between 5.7% and 6.4% (39–46 mmol/mol).1 HbA1c was measured using a turbidimetric inhibition immunoassay on a Siemens Dimension Vista 1500 platform. Coefficient of variation was 2.9% and 2.4%, at a HbA1c level of 5.7% and 10.1%, respectively. Demographic data, previous diagnosis of diabetes, and coding information were obtained from the hospital's database. This study was discussed with and approved by the Human Research Ethics Committee of the Western Sydney Local Health District.
Results
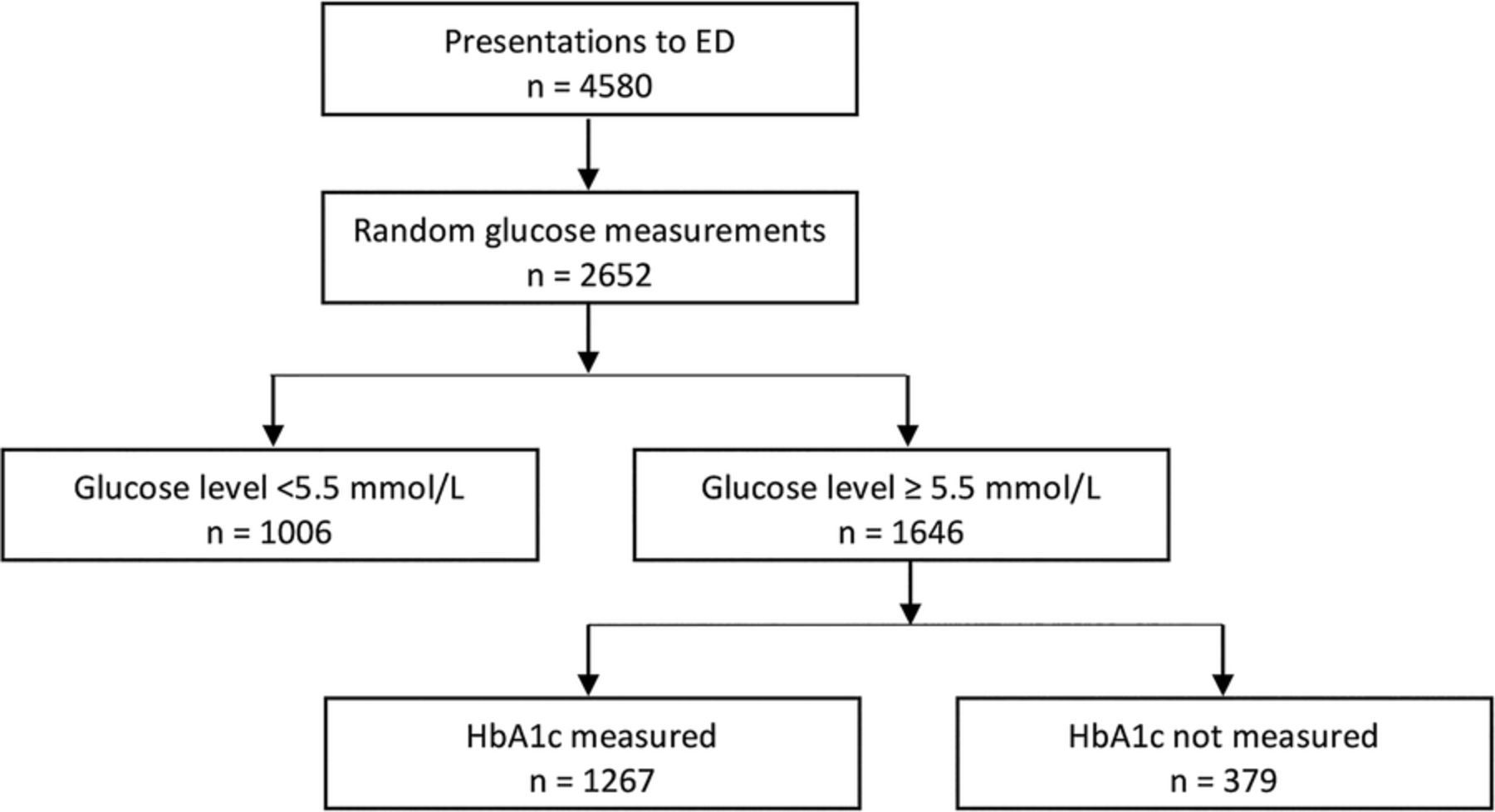
There were 4580 presentations to the ED. Using the methodology described, 1267 HbA1c measurements were available (figure 1). Female patients accounted for 47.3% of results obtained. Three hundred and seventy-nine HbA1c tests were not performed due to multiple presentations, insufficient blood sampling or issues related to the automation of HbA1c measurement. In this cohort, diabetes was present in 38.4% (HbA1c≥6.5% or a prior diagnosis if HbA1c<6.5%; table 1).
Levels of dysglycemia based on glycated hemoglobin (HbA1c) measurements with subset analysis of individuals newly diagnosed with diabetes
{kind=link}
Study profile. ED, emergency department; HbA1c, glycated hemoglobin.
Of the patients identified with diabetes, 45.2% were female and 32.2% (157/487) were newly diagnosed. Of newly diagnosed patients, 61.8% had mild diabetes (HbA1c of 6.5–6.9% or 48–52 mmol/mol). Three hundred and forty-seven (27.4%) of HbA1c sampled patients had levels consistent with prediabetes (HbA1c 5.7%–6.4% or 39–46 mmol/mol). The sampling protocol resulted in HbA1c being measured in 59% (n=751) of admitted patients, and, of these, diabetes was present in 42.4%. Analysis of coding information revealed that 28% of admissions who were known to have diabetes (either by HbA1c assessment or previously noted in the medical record) were not coded for the diagnosis of diabetes. Of this group, 11% were previously known to have diabetes, 81% were newly diagnosed, and the remaining 8% were coded as impaired glucose regulation.
Discussion
The key finding from this ED study is that almost two in every five patients tested on available HbA1c samples had diabetes. This is consistent with other studies that indicate a high risk of diabetes in Western Sydney's ethnically diverse, low socioeconomic population.4 ,6 Importantly, one in three patients found to have diabetes were previously unaware of their condition. Additionally, a further 27.4% had prediabetes, meaning that 65.7% of patients tested with HbA1c had either diabetes or prediabetes. The use of HbA1c for diabetes case finding in the ED had a high yield in our patient population, but these findings may not necessarily be replicated in locations with a lower prevalence of diabetes. In an Australian tertiary referral hospital's ED in Melbourne, Jelinek et al7 noted similar rates of dysglycemia but, despite a high diabetes prevalence, the authors did not find screening a feasible exercise due to their reliance on a 75 g OGTT to confirm the diagnosis.
Diagnosis of diabetes was not confined to the mild end of the spectrum—with a severely elevated HbA1c level (>9% or 75 mmol/mol) seen in 7.3% of the entire cohort, and in 10.2% of newly diagnosed patients. Rapidly identifying admitted patients with poor glycemic control utilizing a test on a single blood sample that does not require any pretest preparation provides an ideal opportunity for intervention by hospital diabetes services. The majority of the newly diagnosed patients had early stage diabetes with HbA1c levels of 6.5–6.9% (48–52 mmol/mol), providing the ideal opportunity for early intervention to take place before the onset of complications. Almost a third of the individuals diagnosed as having diabetes were not aware of their diagnosis, reflecting the hidden burden of diabetes in our community. This may indicate that current screening practices in primary care are insufficient and further supports opportunistic HbA1c testing in individuals presenting to hospital, a population seemingly enriched with cases of diabetes. In Australia, universal health insurance (Medicare) covers the cost of HbA1c testing to diagnose diabetes in ‘high-risk’ individuals.8 Our data suggest that a high proportion of patients presenting to ED and requiring blood collection would meet this definition. Use of blood glucose alone for diabetes diagnosis is problematic because of the presence of ‘stress hyperglycemia’, a pitfall avoided by use of the HbA1c test.
The use of HbA1c to identify prediabetes is supported by the American Diabetes Association.1 Progression to diabetes may be prevented if these individuals were provided with achievable lifestyle intervention. This has been shown to be beneficial in prediabetes in several studies such as the Diabetes Prevention Program9 and the Finnish Diabetes Prevention Program.10 One such lifestyle intervention programme in Australia is the government run Get Healthy initiative.11
A novel feature of this study is the use of HbA1c to diagnose diabetes in a non-primary care setting. Previous studies have demonstrated that diabetes screening in an outpatient and a GP setting is feasible.12 The visit to ED is an opportunity for us to detect diabetes in individuals who infrequently seek routine medical care, and who may otherwise go undetected. An earlier ED study of a tertiary referral hospital in Adelaide, Australia, noted a prevalence of undiagnosed diabetes of 11%,5 compared with 32.2% in this study. This may be because of the highly multicultural population in our study, compared with the overwhelmingly Caucasian population of Adelaide (table 2).
Comparison of the top 10 cultural groups (based on country of birth) between the study population and the postcodes within which the respective hospitals are located
For the purpose of funding and performance review, all clinical data on admitted patients are coded using the International Classification of Disease codes. In our cohort, 28% of patients diagnosed with diabetes based on an elevated HbA1c were not coded as having diabetes, leading to an underestimate in the coded data, and potential underfunding relative to true case complexity. Coding inaccuracies can also result in an overestimation of the number of newly diagnosed individuals as this calculation is dependent on whether they had previously been coded as having diabetes.
The use of HbA1c to diagnose diabetes has limitations as any factor affecting the quantity or quality of the hemoglobin molecule can result in measurement inaccuracies. This has not been accounted for in our study, but would tend to result in an underestimate of diabetes cases. Sampling was only undertaken in individuals who had blood collected, and this introduces a source of bias. It could be argued that the pickup rate for diabetes could be further improved by advocating routine testing in all individuals presenting to the ED.
Another limitation of using HbA1c to diagnose diabetes is the existence of ethnic variability in the measurement that is not explained by glycemic state, structural abnormalities or quantity of the hemoglobin molecule.15–17 This is relevant in our multiethnic population where the diagnosis of diabetes can be based on a slight elevation in the HbA1c level. Our study used glucose level as the initial screening step and this would have limited the diagnostic inaccuracies that might have occurred had this not been undertaken.
Diabetes case finding in the ED is justified as there is a significant population with known and undiagnosed diabetes. Following the findings of this pilot, it is intended that routine HbA1c testing will be the norm in the ED at Blacktown Hospital.
Acknowledgments
The authors acknowledge the assistance of Pathology West for HbA1c assessment and data retrieval, the Health Information Record Service for coding information, and the Executive of Blacktown/Mt Druitt Hospital for supporting the study, particularly for the costs of HbA1c measurements.
References
Footnotes
Contributors T-MH assisted in study design and database development, contributed to the discussion, researched and analyzed data, and wrote the manuscript. AH assisted in study design, researched, collected and analyzed data, and wrote the manuscript. SR collected data and assisted with correspondence. XF analyzed data, contributed to the discussion, and reviewed/edited the manuscript. JL collected data. TA-B contributed to the discussion and reviewed/edited the manuscript. DC contributed to the discussion and concept. MM contributed to the study design and discussion, and reviewed/edited the manuscript. GM conceived the idea, secured institutional support, contributed to the discussion, and reviewed the manuscript.
Competing interests None declared.
Ethics approval Human Research and Ethics Committee of the Western Sydney Local Health District.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.