Article Text

Abstract
Objective Obesity is associated with increased risk of diabetes, hypertension and cardiovascular mortality. Several studies have reported increased length of hospital stay and complications; however, there are also reports of obesity having a protective effect on health, a phenomenon coined the ‘obesity paradox’. We aimed to investigate the impact of overweight and obesity on complications and mortality in hospitalized patients with hyperglycemia and diabetes.
Research design and methods This retrospective analysis was conducted on 29 623 patients admitted to two academic hospitals in Atlanta, Georgia, between January 2012 and December 2013. Patients were subdivided by body mass index into underweight (body mass index <18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2) and obese (>30 kg/m2). Hyperglycemia was defined as a blood glucose >10 mmol/L during hospitalization. Hospital complications included a composite of pneumonia, acute myocardial infarction, respiratory failure, acute kidney injury, bacteremia and death.
Results A total of 4.2% were underweight, 29.6% had normal weight, 30.2% were overweight, and 36% were obese. 27.2% of patients had diabetes and 72.8% did not have diabetes (of which 75% had hyperglycemia and 25% had normoglycemia during hospitalization). A J-shaped curve with higher rates of complications was observed in underweight patients in all glycemic groups; however, there was no significant difference in the rate of complications among normal weight, overweight, or obese patients, with and without diabetes or hyperglycemia.
Conclusions Underweight is an independent predictor for hospital complications. In contrast, increasing body mass index was not associated with higher morbidity or mortality, regardless of glycemic status. There was no evidence of an obesity paradox among inpatients with diabetes and hyperglycemia.
- Obesity
- Type 2 Diabetes
- Hyperglycemia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Underweight status was found to be an independent predictor for inpatient complications.
Obesity was not associated with a higher morbidity or mortality in hospitalized patients when compared to normal weight, regardless of glycemic status.
No ‘obesity paradox’ was observed in the hospital setting among patients with diabetes and hyperglycemia.
Introduction
Obesity and diabetes mellitus are major burdens on the US healthcare system. Despite public health efforts, over two-thirds of US adults were overweight or obese in 2011–2012.1 Similarly, the worldwide prevalence of obesity has more than doubled since 1980 and according to the WHO, more than 1.9 billion adults aged 18 years and above (38% of men and 40% of women) were overweight in 2014.2 Several studies have reported on the negative impact of obesity on health, including increased risk of diabetes, hypertension, dyslipidemia, cardiovascular disease, osteoarthritis, cancer, and overall mortality.3–6 Despite the known negative health effects of obesity, recent prospective studies have reported a U-shaped or J-shaped relationship between body mass index (BMI) and mortality, with lower mortality rates observed in individuals with higher BMI compared to lower BMI.7–12 This phenomenon has been coined the ‘obesity paradox’ and has been recognized in several conditions, including cardiovascular8 ,11 ,12 and kidney disease.10
A large body of evidence suggests that the presence of hyperglycemia in hospitalized patients with and without diabetes is associated with poor clinical outcomes.13–20 Inpatient hyperglycemia has been associated with increased risk of complications, longer hospital stay, higher admission rates to intensive care and death.13–19 In general medicine and surgery patients, hyperglycemia has also been associated with a higher risk of postoperative infection, prolonged hospital stay and a higher chance of requiring nursing home care after discharge.14 ,17 ,21 ,22
Few studies have investigated the association between BMI and clinical outcomes in hospitalized patients. In the surgical population, mixed results have been reported with some studies showing longer operation times, increased length of stay, and worse perioperative outcomes,23–26 while other studies have shown improved operative outcomes and mortality.9 ,27 Numerous studies in medicine patients have also reported a protective effect against morbidity and mortality, suggesting the presence of an obesity paradox.7 ,8 ,10–12 Despite the lack of consensus on the association between obesity and hospital complications, obese patients are generally considered to be at higher risk of complications compared to their normal weight counterparts. Given the high prevalence of diabetes, hyperglycemia, and obesity in hospitalized patients and the inconsistencies in evidence regarding their impact on hospital outcomes, we performed an observational database analysis investigating the interplay between obesity and hyperglycemia and its impact on hospital outcomes.
Methods
We reviewed the medical records of 29 623 patients admitted to Emory University Hospital and Emory Midtown Hospital between January 2012 and December 2013. Patients were subdivided by BMI into categories of underweight (BMI <18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25–29.9 kg/m2), obesity grade 1 (BMI 30–34.9 kg/m2), obesity grade 2 (BMI 35–39.9 kg/m2), and obesity grade 3 (BMI >40 kg/m2). Patients were categorized according to glycemic status into diabetes, no diabetes with hyperglycemia, and no diabetes with normoglycemia. Hyperglycemia was defined as a maximum blood glucose (BG) >10 mmol/L. We excluded patients who were undergoing outpatient procedures, had an admission glucose >22 mmol/L, ICD-9 diagnoses for diabetic ketoacidosis, hyperosmolar hyperglycemic state and end-stage renal disease. Patients with an estimated glomerular filtration rate <15 mL/min were also excluded.
Patient information was obtained from the Clinical Data Warehouse infrastructure programme from the Emory University Hospital electronic health record and billing systems. The following variables were extracted for each patient: age at admission, gender, race, BMI, history of diabetes, admission service (medicine vs surgery), intensive care unit (ICU) treatment, comorbidities, hospital complications, insulin usage and glucose measures on admission and during hospitalization. Admission diagnoses were extracted using ICD-9 codes and were categorized into the following groups: cardiovascular, gastrointestinal, endocrinology, rheumatology, hematology/oncology, infectious, neurology, pulmonary, renal and miscellaneous disorders. Diagnosis of diabetes mellitus, complications, and comorbidities were identified based on ICD-9 codes except for acute kidney injury (AKI). AKI was determined by a rise in serum creatinine of 50% during hospitalization, above the admission value. ICD-9 codes necessary to calculate Charlson comorbidity index28 were evaluated in order to take into account severity of illness.28 Hospital complications included a composite of mortality, pneumonia, acute myocardial infarction, respiratory failure, AKI and bacteremia. Comorbidities were determined using ICD-9 codes for the following chronic conditions: coronary artery disease, hypertension, chronic kidney disease, malignancy, chronic obstructive pulmonary disease and dyslipidemia. Since some patients had multiple hospitalizations, only the first hospitalization during the study time period was included in the analyses.
Statistical analysis
The primary objective of the study was to determine the association between BMI and in-hospital composite of complications and mortality by diabetes/glycemic status. We examined the association via logistic regression models. In unadjusted and adjusted analyses, BMI was included as a categorical variable (<18.5, 18.5–24.9 (reference group) compared to 25–29.9, 30–34.9, 35–39.9, and ≥40 kg/m2). In the adjusted analysis, we sequentially added demographics including age, gender, and race, and then clinical characteristics including comorbidities, hospital setting (ICU vs non-ICU), admission service (medicine vs surgery), admission diagnosis, Charlson comorbidity index and admission glucose into the models.
Inpatient complications, demographics and comorbidities were compared across different BMI and glycemic groups. Continuous variables were compared using analysis of variance or Kruskal-Wallis test and expressed as mean±SD or median (IQR). Categorical variables were compared by χ2 test and expressed as frequency and proportion. All the analyses were also performed in patients with diabetes and in patients without diabetes with normoglycemia and hyperglycemia. Hosmer-Lemeshow test was applied to examine the fit of all the models. A two-tailed p<0.05 was considered to be statistically significant. Statistical analyses were performed with the Statistical Analysis System, V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
The study population included 29 623 patients. Of them, 1235 patients were underweight (4.2%), 8743 normal (29.6%), 8960 overweight (30.2%), 5665 obesity grade 1 (19.1%), 2734 obesity grade 2 (9.2%) and 2276 obesity grade 3 (7.7%). There were 8046 (27.2%) patients with diabetes and 21 577 (72.8%) without diabetes. Of the patients without diabetes, 5368 (25%) were hyperglycemic and 16 209 (75%) were normoglycemic during their hospital stay. Patient demographics and clinical characteristics by glycemic status and BMI are shown in table 1. Patients with diabetes tended to be older than patients without diabetes, but patients with obesity grade 3 were younger than those of other BMI categories (see table 1). There was a relatively even ratio of male to female patients, except for those with obesity grade 3 who were more likely to be women. There were also more African-American patients with diabetes when compared to those without diabetes, particularly among normal BMI, overweight and obesity grade 1 patients. Among patients with diabetes, admission and mean BG were lower in underweight patients than in higher BMI groups; however, there was no significant difference in the maximum in-hospital BG across all BMI groups.
Patient demographics by BMI and glycemic status
Patient comorbidities by BMI are shown in table 2. Obese patients had significantly higher rates of pre-existing coronary artery disease, hypertension, and hyperlipidemia. However, chronic obstructive coronary disease and malignancy were more frequently seen in the lower BMI groups, in patients with and without diabetes.
Prevalence of comorbidities by BMI and diabetes status
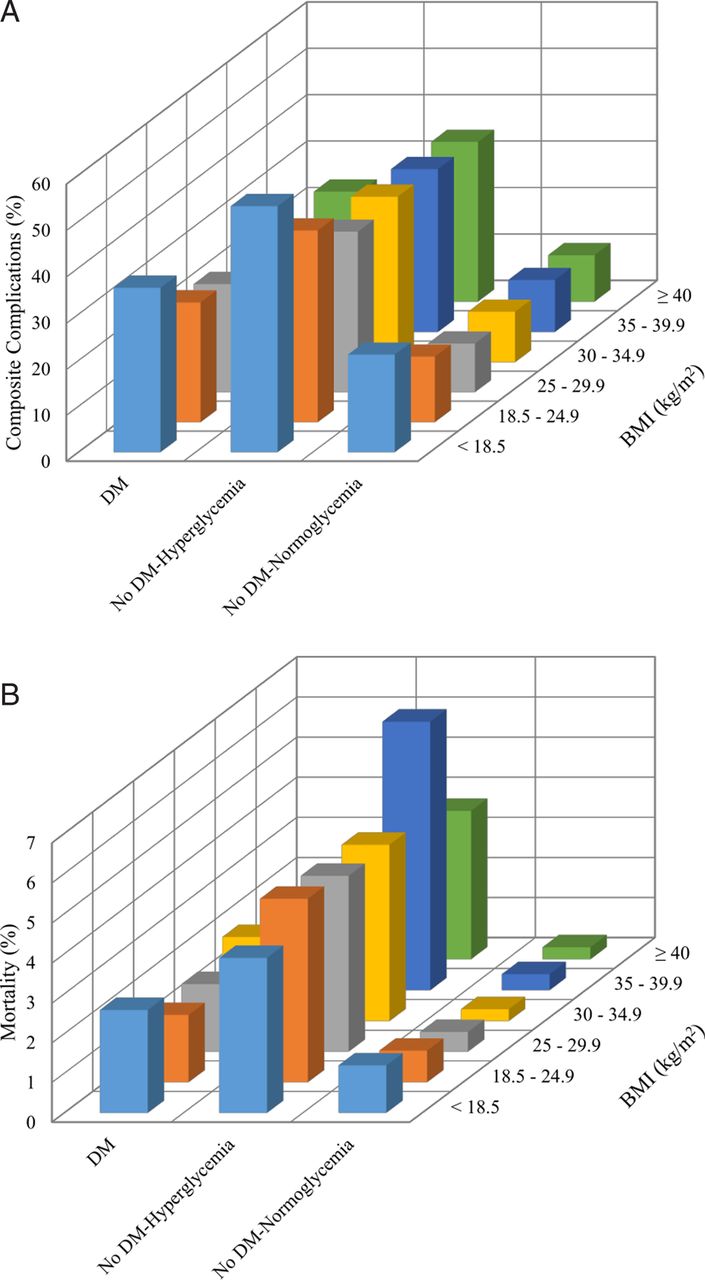
Figure 1 shows the rate of in-hospital complications and mortality across BMI and glycemic groups. Hyperglycemic patients with and without diabetes had higher rates of hospital complications compared to normoglycemic patients without diabetes. In unadjusted analysis, a J-shaped curve was observed with higher rates of hospital complications and mortality in underweight patients. In multivariate analyses adjusted for patient demographics and clinical characteristics including comorbidities, severity of illness, admission diagnosis, hospital setting (ICU vs no ICU), and service (medicine vs surgery), we found that being underweight was independently associated with higher rates of composite complications among all patients (table 3). When stratifying by glycemic status, only patients without diabetes with hyperglycemia had significantly increased complications in underweight compared to normal weight (adjusted OR 1.66 (1.15 to 2.38)) (table 4). Otherwise, across all glycemic groups, BMI was not associated with higher rates of complications or in-hospital mortality.
{kind=link}
(A) Inpatient complications by BMI and glycemic status. (B) In-hospital mortality by BMI and glycemic status. BMI, body mass index; DM, diabetes mellitus.
Adjusted ORs for complications and mortality by BMI including all glycemic groups
Adjusted ORs for complications and mortality by BMI and glycemic status
Discussion
This study aimed to determine the combined impact of obesity and hyperglycemia on inpatient complications and mortality rates. In agreement with previous studies,13–17 we observed that inpatient hyperglycemia is common and is associated with poor outcomes, with the highest rates of complications seen in hyperglycemic patients without diabetes, even compared to patients with diabetes. Also consistent with the literature was our finding that being underweight conferred a worse prognosis compared to normal, overweight, or obesity.29 ,30 After adjusting for patient demographics and clinical characteristics, no significant improvement in clinical outcomes was observed in patients who were obese compared to those with normal BMI.
Several studies have investigated the relationship between obesity, diabetes and clinical outcomes in ambulatory populations.29–34 Emerging evidence suggests that obesity may have a protective effect against morbidity and mortality, a phenomenon referred to as the ‘obesity paradox’.7–12 ,31 Despite a plethora of data, the effect of diabetes and glycemic status on the perceived obesity paradox remains unclear. Carnethon et al34 prospectively analyzed a population of 2625 at the time of diabetes diagnosis and observed much higher mortality rates in patients with normal BMI when compared to overweight or obese patients (categorized as BMI >25). There are multiple studies that have found similar results, with a J-shaped or U-shaped association between BMI and mortality among patients with diabetes.31–33 ,35 However, some limitations of these studies included broad BMI categories,33 ,34 small number of deaths,29 ,33 ,34 and lack of analyses of patient comorbidities.31–34 Our results were more consistent with those of Tobias et al,30 who analyzed data from two large, prospective cohort studies and found no evidence of an obesity paradox in 11 427 patients with diabetes. Conflicting data regarding the obesity paradox extends beyond the population with diabetes, and whether a paradox truly exists is an ongoing topic of debate.
To the best of our knowledge, this is the first study to explore the interplay between BMI and glycemic status and its impact on mortality and complications in hospitalized patients. Our results did not show the presence of an obesity paradox among patients with diabetes. In-hospital mortality, bacteremia, and acute myocardial infarction were complications that did not appear to be affected by BMI or glycemic status in our study. The literature remains mixed regarding the link between obesity and coronary atherosclerosis.36–40 In a recent prospective cohort study by Costanzo et al,37 clinic patients with type 2 diabetes who were overweight and obese had a higher risk of nonfatal cardiovascular events but not mortality. We did not observe higher rates of acute myocardial infarction with increasing BMI, but perhaps these patients remained at higher risk of nonfatal cardiovascular events beyond their hospital stay, which was not accounted for in our retrospective study. Additional prospective studies would be beneficial in determining long-term risk of cardiovascular events in patients across different glycemic and BMI groups.
There are a number of limitations in our study. This is a retrospective analysis, which relied on ICD-9 codes. As a result, we may have missed some diagnoses due to lack of documentation. We also used BMI as the single measure of obesity; however, fitness and waist circumference have been shown to better predict mortality compared to BMI.41–43 As with many observational studies, selection bias is another potential limitation, seeing as patients are selected based on a factor which is to be analyzed (diabetes) that is affected by an exposure (obesity), both of which share risk factors for the outcome (mortality). The only sure way to avoid such selection bias is to ensure that exposure and start of follow-up coincide.44 One of the major strengths of our study was its large sample size, which provided unique insight into how obesity relates to hospitalized patients. In addition, we adjusted for patient demographics and key clinical characteristics that included comorbid conditions, severity of illness, admission diagnosis, hospital setting (ICU vs no ICU), and service (medicine vs surgery). We did not, however, adjust for smoking or alcohol consumption which may have confounded our results, as smoking in particular has been linked to low BMI status and increased risk of mortality.30 ,45
In summary, we found that underweight represents an independent predictor for hospital complications; however, there was no evidence of an obesity paradox in hospitalized patients with hyperglycemia and diabetes. We also found no association between increasing BMI and mortality regardless of glycemic status.
Acknowledgments
The abstract of this study was previously presented at Endo Society, March 2015.
References
Footnotes
Contributors A-SA and GEU designed the study and wrote the proposal and manuscript. MF, LB, DS, FJP, PV, and JSH contributed to the analysis and interpretation, as well as reviewing the manuscript. JW was in charge of data collection and LZ from the School of Public health conducted the statistical analysis. All listed authors were involved in critically revising the manuscript and approved the final version of the paper to be published.
Funding This study was supported by the Jacobs Family Research Funds (GEU). GEU is supported in part by research grants from the American Diabetes Association (1-14-LLY-36), and Public Health service (PHS) grant from the Clinical Translational Science Award Program (M01 RR-00 039), National Institutes of Health, National Center for Research Resources.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.