Article Text

Abstract
Objective Selenium is an essential micronutrient for human health. Although many observational and interventional studies have examined the associations between selenium and diabetes mellitus, the findings were inconclusive. This study aimed to investigate the relationship between serum selenium levels and prevalence of diabetes, and correlated the relationship to insulin resistance and central obesity.
Research design and methods This was a hospital-based case–control study of 847 adults aged more than 40 years (diabetes: non-diabetes =1:2) in Northern Taiwan. Serum selenium was measured by an inductively coupled plasma-mass spectrometer. The association between serum selenium and diabetes was examined using multivariate logistic regression analyses.
Results After adjusting for age, gender, current smoking, current drinking, and physical activity, the ORs (95% CI, p value) of having diabetes in the second (Q2), third (Q3), and fourth (Q4) selenium quartile groups were 1.24 (95% CI 0.78 to 1.98, p>0.05), 1.90 (95% CI 1.22 to 2.97, p<0.05), and 5.11 (95% CI 3.27 to 8.00, p<0.001), respectively, compared with the first (Q1) quartile group. Further adjustments for waist circumference and homeostatic model assessment-insulin resistance (HOMA-IR) largely removed the association of serum selenium levels with diabetes but not in the highest quartile (compared with Q1, Q3: 1.57, 95% CI 0.91 to 2.70, Q4: 3.79, 95% CI 2.17 to 6.32).
Conclusions We found that serum selenium levels were positively associated with prevalence of diabetes. This is the first human study to link insulin resistance and central obesity to the association between selenium and diabetes. Furthermore, the association between selenium and diabetes was independent of insulin resistance and central obesity at high serum selenium levels. The mechanism behind warrants further confirmation.
- Adult Diabetes
- Obesity
- Insulin Resistance
- Metabolic Syndrome
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Serum selenium levels are positively associated with the prevalence of diabetes.
This is the first human study to link insulin resistance and central obesity to the association between selenium and diabetes.
The association between selenium and diabetes was removed mostly after adjusting for insulin resistance and central obesity, but not in the highest quartile of the selenium group.
Introduction
Selenium is an essential trace mineral known for its antioxidant function, leading to the expectation that selenium would play a protective role against diabetes mellitus.1 ,2 However, evidence from observational studies on selenium and diabetes is inconclusive. While few studies identified positive associations between selenium exposure and fasting glucose or prevalence of diabetes,3–5 some investigations showed no significant association6 or negative association.7 One meta-analysis examined the association between serum selenium levels and diabetes and found a U-shaped non-linear dose–response relationship between selenium and diabetes.8 Since observational findings could not clarify casual effect between selenium and diabetes, there were few randomized controlled trials focusing on the association between selenium supplementation and the risk of diabetes. One study showed that the incidence of diabetes was significantly higher in the selenium-supplemented group than in the placebo group.9 Two other randomized trials found that selenium had no effect on risk of developing diabetes or on assessing by serum glucose level or plasma adiponectin.10 ,11 Two short-term interventional studies reported that selenium supplementation for 6–8 weeks significantly lowered fasting serum insulin and HOMA-IR.12 ,13
Both from observational studies and randomized controlled trials, suprasupplemented selenium and high serum selenium levels were probable risk factors for development of type 2 diabetes.14 To unseal the mechanism behind the association between selenium exposure and diabetes, animal studies focused on diabetogenic effect and insulin resistance of selenium flourished. Early studies indicated that selenium acted as an insulin-mimic and antidiabetogenic parameters.15 ,16 Recent animal experiments declared that overproduction of selenium-related compounds induced hyperglycemia in mice.17 ,18 The dual role of selenium was triggered by selenoprotein P and glutathione peroxidase, regulating diabetes-associated hepatokine and reactive oxygen species, respectively.19 ,20 Until now, there was no large study that compared patients with diabetes with patients without diabetes in serum selenium levels and insulin resistance. Therefore, the study aimed to investigate the association between serum selenium levels and prevalence of diabetes and link the association to central obesity, insulin resistance, and metabolic factors.
Materials and methods
Study population
We conducted a case–control study to compare serum selenium levels between patients with diabetes and patients without diabetes (with diabetes:non-diabetes=1:2) from 2007 to 2014 at one medical center in Taipei. A total of 847 ambulatory males or females, aged more than 40 years, were invited to participate in our study by advertisements. Patients who were diagnosed with diabetes, defined as serum glycated hemoglobin ≥6.5% or under treatment of any antidiabetic agent, and capable of understanding and signing the informed consent document were enrolled and assigned to case groups. Patients who came to clinic for other chronic diseases and were capable of understanding and signing the informed consent document were enrolled and assigned to control groups. Information about age, sex, cigarette smoking, alcohol consumption, physical activity, and previous diseases was obtained by individual interview through questionnaires. Current smokers were defined as those smoking for more than 6 months prior to this study. Former smokers were defined as those quitting for more than 1 year. Former smokers and never-smokers were grouped together as non-current smokers for further analysis. Current alcohol drinkers were defined as those drinking more than 1 oz of alcohol per week for 6 months. Former drinkers were defined as those quitting for more than 1 year. Former drinkers and never-drinkers were grouped together as non-current drinkers for further analysis. Physical activity was recorded as the exercise hours per week. Weight, height, systolic blood pressure (BP), and diastolic BP were measured using a standard electronic scale of stadiometer and sphygmomanometer, respectively. Waist circumference (WC) was measured by the same operator. Diabetes, hypertension, and hyperlipidemia were defined based on a self-reported history or current medication use for those conditions.
Definition of metabolic syndrome
Participants were considered to have metabolic syndrome if they met ≥3 of the following criteria: WC ≥90 cm in men or ≥80 cm in women; serum triglycerides ≥1.69 mmol/L; high-density lipoprotein cholesterol (HDL-C) <1.03 mmol/L in men or <1.29 mmol/L in women; systolic BP≥130 and/or diastolic BP≥85 mm Hg; and fasting glucose ≥5.56 mmol/L. Participants with medications for diabetes were sorted into the group which met the criteria for fasting glucose ≥5.56 mmol/L. Those with medications for hypertension were sorted into the group which met the criteria for BP≥130/85 mm Hg. Participants with medications for hyperlipidemia were sorted into the group which met the criteria for serum triglycerides ≥1.69 mmol/L.
Measurement of serum selenium level and other biomarkers
Venous blood samples were taken after a minimum 8-hour fast. Serum glucose, total cholesterol, HDL-C, low-density lipoprotein cholesterol, and triglycerides were assessed by an automatic spectrophotometric assay (HITACHI 7250, Japan). Fasting insulin level was measured by a microparticle enzyme immunoassay using an AxSYM system (Abbott Laboratories, Dainabot Co, Tokyo, Japan). The homeostatic model assessment-insulin resistance (HOMA-IR) was applied as an indirect measure of the degree of insulin resistance (HOMA-IR=fasting insulin×fasting plasma glucose/22.5, with glucose in mmol/L and insulin in mU/L).21 Serum selenium was measured using inductively coupled plasma mass spectroscopy. Serum samples were diluted 1:24 with diluents of 0.1% nitric acid and 0.1% Triton X-100. The calibration standards were prepared in a blank matrix and run using the standard addition calibration type. The serum samples were analyzed in the peak-jumping mode for 82Se, with the detection limit set at 0.01 μmol/L. Accuracy of the analysis was checked against Seronorm Trace Element Human Serum (batch 704121; Nycomed AS, Oslo, Norway) as reference material.22 This study has been approved by the Ethics Committee of National Taiwan University Hospital, and written informed consent was obtained from all participants.
Statistical analysis
Participants were divided into quartiles according to the serum selenium levels. Data were presented as means and SDs (mean±SD) and percentages. Analysis of variance was used for continuous variables and χ2 test was used for categorical variables to analyze interquartile differences. Multivariate logistic regression analyses were performed to estimate the odds of having diabetes among the quartiles of selenium after adjusting for age, gender, current smoking, current drinking, physical activity, WC, and HOMA-IR. The least square (LS) means of WC, glucose, insulin, HOMA-IR, metabolic factors, metabolic syndrome, and prevalence of diabetes were computed by general linear models adjusted for several confounders among the four selenium quartile groups. Statistical analyses were performed using the SPSS statistical software (V.17, SPSS, Chicago, Illinois, USA). A p value of <0.05 was considered to be statistically significant.
Results
The basic characteristics of the participants are shown in table 1. The average age of the participants was 63.9±9.9 years and 69.2% were male. The mean serum selenium concentration was 88.2±21.2 µg/L, and the interquartile cut-off values of selenium were 71.4, 86.8, and 104.5 µg/L. The means of body mass index, WC, total cholesterol, triglycerides, fasting glucose, insulin, and HOMA-IR were significantly different among the four selenium quartiles. The percentage of each metabolic factor and prevalence of metabolic syndrome were also significantly different and showed an increased trend as serum selenium levels increased.
Characteristics of the study population by quartiles of serum selenium levels
The association of serum selenium levels and prevalence of diabetes by multivariate logistic regression analyses are shown in table 2. In model 1, the results showed that a higher serum selenium level was correlated with a higher risk of diabetes after adjusting for age, gender, current smoking, current drinking, and physical activity. The ORs of having diabetes in the second, third, and fourth selenium quartile groups were 1.24 (95% CI 0.78 to 1.98, p>0.05), 1.90 (95% CI 1.22 to 2.97, p<0.05), and 5.11 (95% CI 3.27 to 8.00, p<0.001), respectively, compared with the first quartile group of serum selenium level. In model 2, after further adjusting for WC, the ORs of risk for diabetes in the second, third, and fourth selenium quartile groups were 1.11 (95% CI 0.68 to 1.80), 1.71 (95% CI 1.07 to 2.73), and 4.30 (95% CI 2.69 to 6.87), respectively, compared with the first quartile. In model 3, after further adjusting for HOMA-IR, the ORs of risk for diabetes in the second, third, and fourth selenium quartile groups were 0.69 (95% CI 0.37 to 1.27), 1.57 (95% CI 0.91 to 2.70), and 3.79 (95% CI 2.17 to 6.32), respectively, compared with the first quartile. After stratification by gender and age, the ORs of risk for diabetes after adjustment in the highest selenium quartile groups were 3.65 (95% CI 1.81 to 7.36) and 4.78 (95% CI 2.20 to 10.40) in males and females, respectively; 10.65 (95% CI 4.06 to 27.94) and 2.03 (95% CI 0.96 to 4.31) in young age (<65 years old) and old age (≧65 years old), respectively, compared with the first quartile.
ORs of having diabetes mellitus derived from multiple logistic regression analyses in quartiles of serum selenium levels
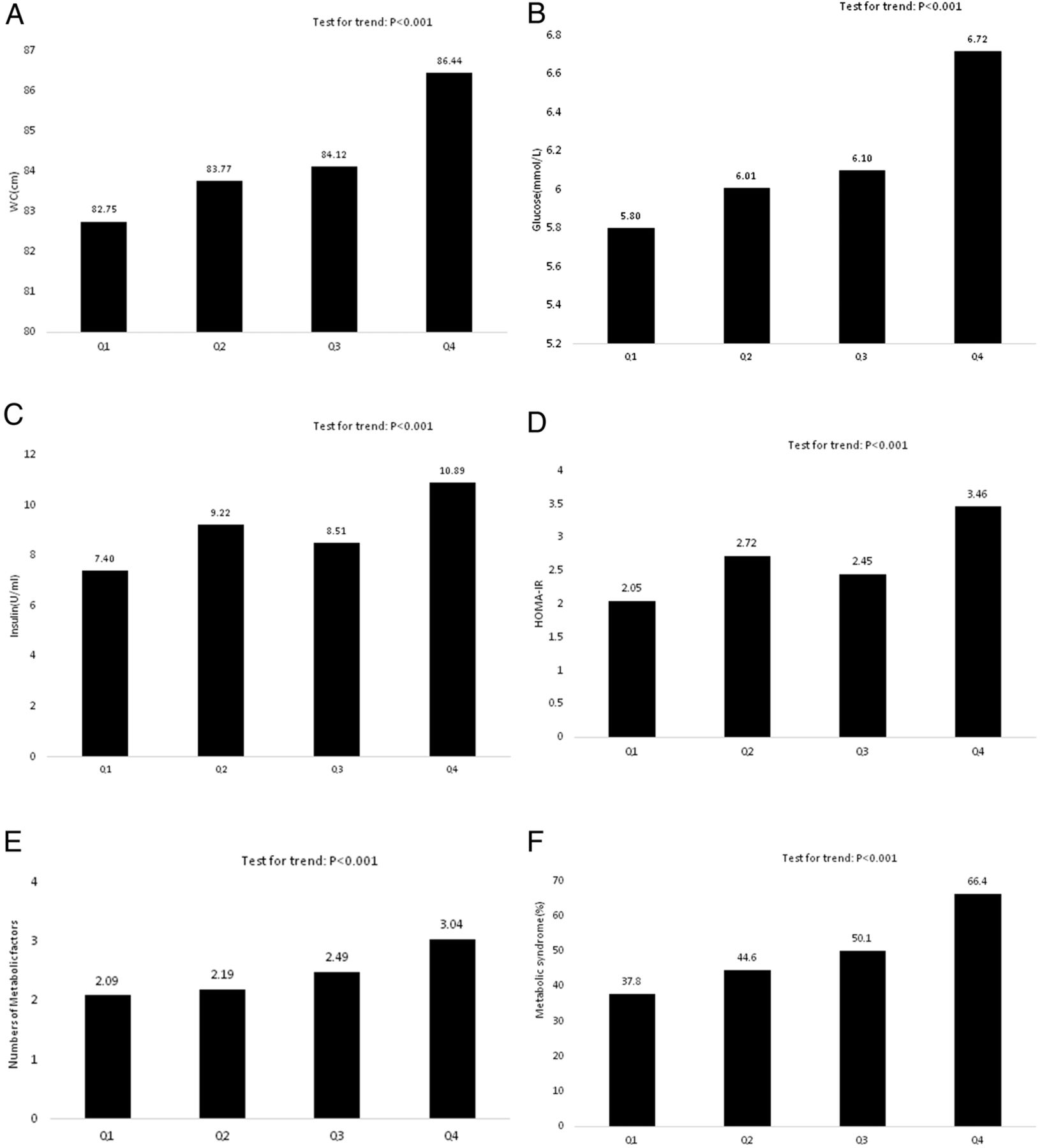
The LS means (±SDs) of the WC, fasting glucose, insulin, HOMA-IR, numbers of metabolic factors, prevalence of metabolic syndrome, and prevalence of diabetes in relation to quartile of serum selenium levels were shown in figures 1 and 2. All of the diabetogenic parameters, that is, insulin resistance factors, increased with increasing serum selenium concentrations in the linear multivariate regression models after adjusting for age, gender, current smoking, current drinking, and physical activity (test for trend: p<0.001).
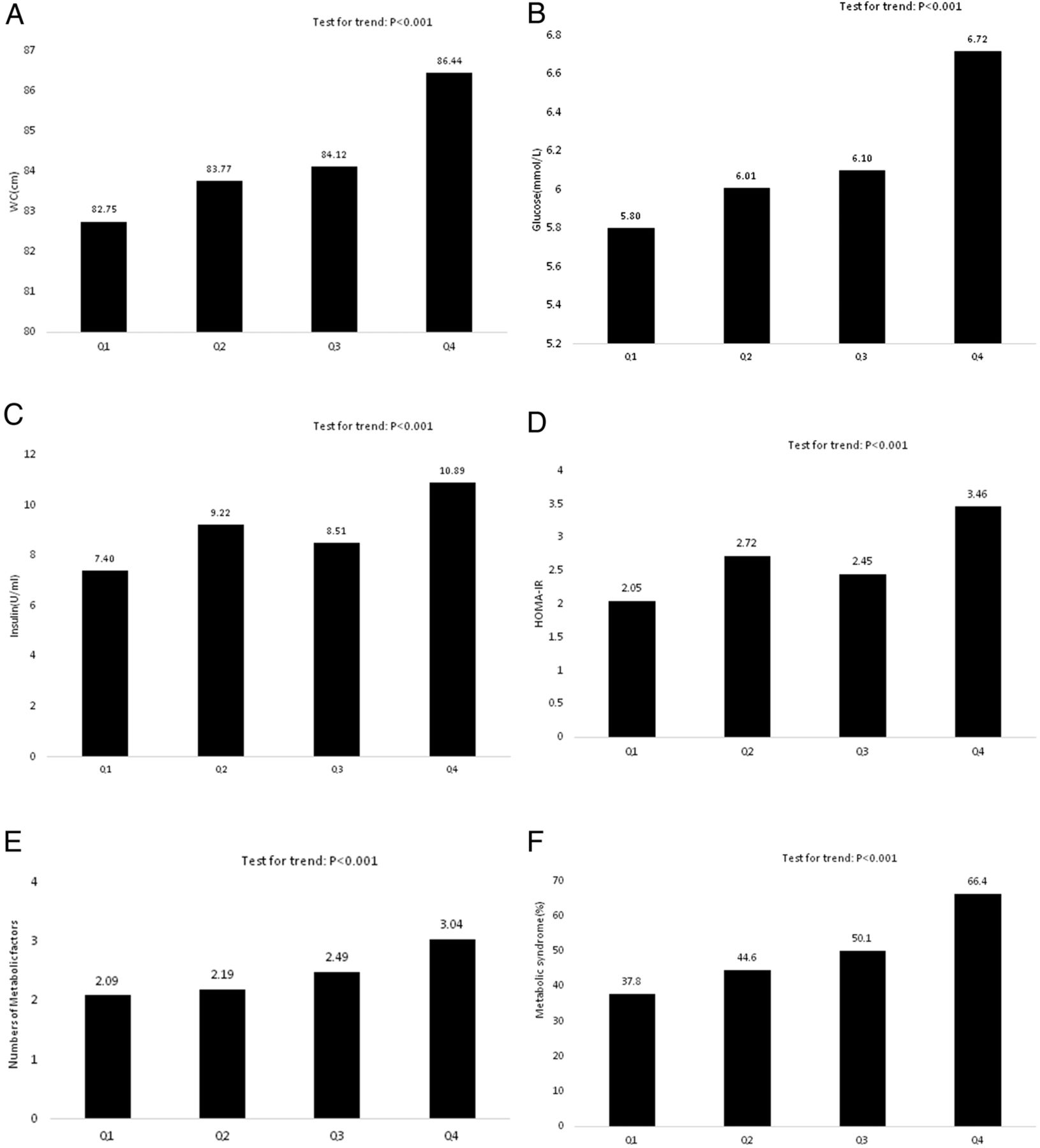
Comparison of (A) WC, (B) fasting glucose, (C) insulin, (D) HOMA-IR, (E) numbers of metabolic factors, and (F) prevalence of metabolic syndrome in relation to quartile of serum selenium levels. The means±SD were calculated by the LS method using a general linear model after adjusting for age, gender, current smoking, current drinking, and physical activity. Q1: N=213, serum selenium concentration <71.4 µg/L; Q2: N=211, serum selenium concentration=71.4–86.7 µg/L; Q3: N=212, serum selenium concentration=86.8–104.5 µg/L; Q4: N=211, serum selenium concentration >104.5 µg/L. The LS means of (A) to (F) increased with the increments of serum selenium (p for trend<0.001). HOMA-IR, homeostasis model assessment of insulin resistance; LS, least square; WC, waist circumference.

{kind=link}
{kind=link}
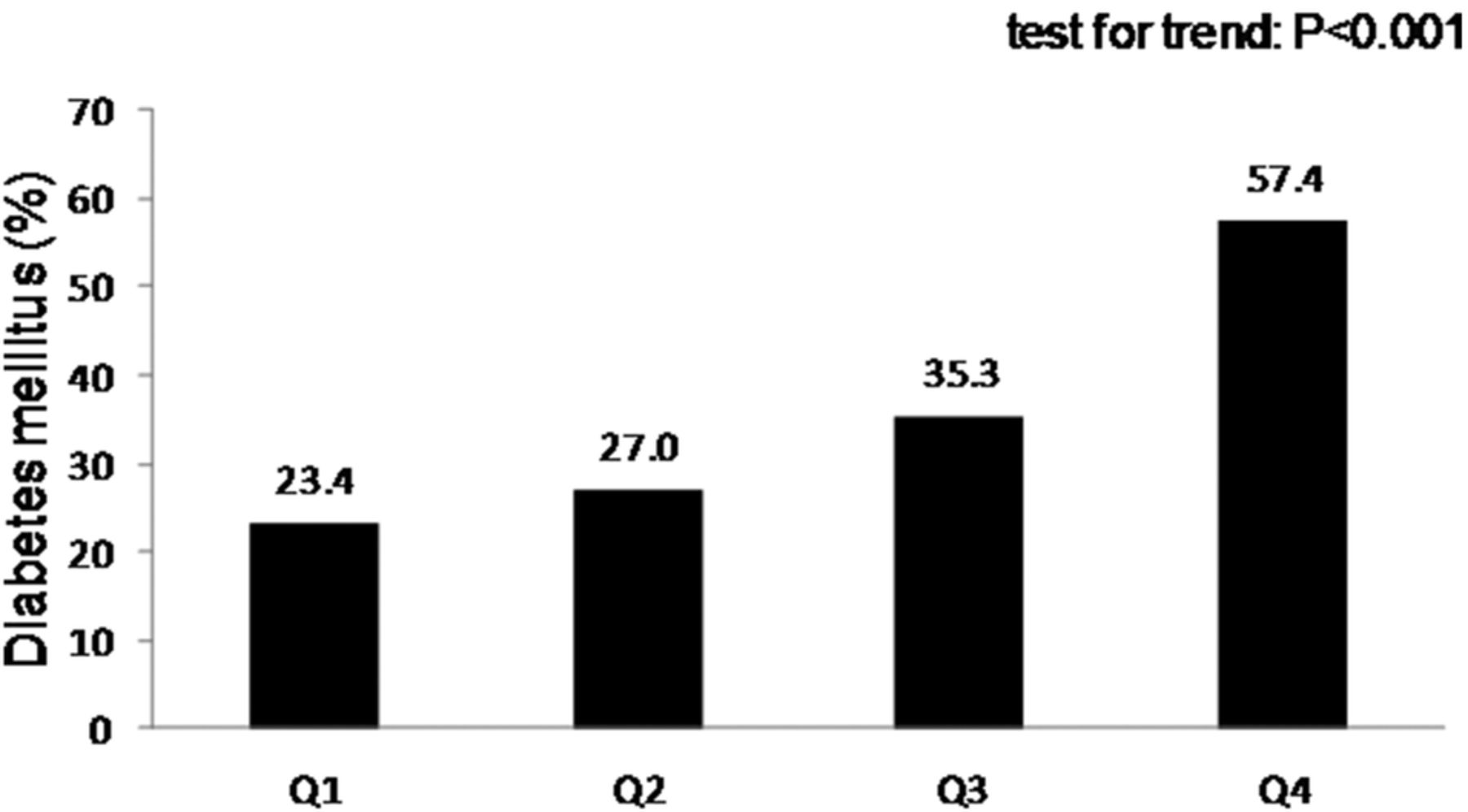
Comparison of prevalence of diabetes mellitus in relation to quartile of serum selenium levels. The means±SD were calculated by the LS method using a general linear model after adjusting for age, gender, current smoking, current drinking, and physical activity. Q1: N=213, serum selenium concentration <71.4 µg/L; Q2: N=211, serum selenium concentration=71.4–86.7 µg/L; Q3: N=212, serum selenium concentration=86.8–104.5 µg/L; Q4: N=211, serum selenium concentration >104.5 µg/L. The LS means increased with the increments of serum selenium (p for trend<0.001). LS, least square.
Discussion
In our study, serum selenium concentrations were positively associated with WC, fasting glucose, insulin, HOMA-IR, numbers of metabolic factors, and prevalence of metabolic syndrome and diabetes (test for trend: p<0.001), implying a dose–response relationship in relation to metabolic factors and risk of diabetes across quartiles of serum selenium levels. Besides, the participants in the highest selenium quartile had a 3.79-fold risk of diabetes compared with those in the lowest quartile after adjusting for demographic confounders WC and HOMA-IR. After stratifying by age or gender, the excessive risk of diabetes in high selenium exposure were persistent in each gender and young age group. These findings supported that central obesity and insulin resistance were either a cause or a consequence between serum selenium gradients and diabetes. The persistence of a direct relation between selenium exposure and risk of diabetes even after adjusting for insulin resistance and central obesity implies that the causal role of additional mechanisms, possibly triggered by selenium overexposure, is independent of central obesity and insulin resistance. The independent association was not reported before and warrants further investigation.
Selenium is incorporated into a series of selenoproteins that has been reported to be vital for antioxidant properties, anti-inflammation roles, and contributed to an antidiabetic effect.23 In early animal studies, selenium supplementation improved plasma glucose, insulin, and reverse abnormal expression of gluconeogenesis in rats with diabetes.15 ,16 ,24 Nevertheless, findings from observational and interventional studies reported inconsistent results. Five epidemiological investigations reported that selenium exposure and selenium supplementation were positively associated with fasting plasma glucose or prevalence of type 2 diabetes,3–5 ,25–27 whereas three studies declared no significant association or negative association.6 ,7 ,28 In Asia, only one China study investigated the association between cognitive function and serum selenium level and found that high serum selenium level was crudely associated with high prevalence of diabetes, which was similar with our findings.26 For the antioxidative and anti-inflammatory properties of selenium, there were three large randomized controlled trials in cancer prevention to figure out whether and what dosage of selenium supplementation reduced the incidence of cancer.9 ,11 ,29 ,30 To explore the relation between selenium supplement and diabetes risk, there were few post hoc analyses of these randomized controlled trials. In a secondary analysis of the Nutritional Prevention of Cancer (NPC) trial, 1202 patients were administrated 200 µg/L selenium or placebo. After 7.7 years of follow-up, 58 selenium recipients and 39 placebo recipients developed diabetes (HR 1.55, CI 1.03 to 2.33).9 In SELECT (the Selenium and Vitamin E Cancer Prevention Trial), selenium supplementation was not related to diabetes risk (relative risk 1.07, p=0.16) after 5.5 years of follow-up.29 ,30 In the PRECISE pilot trial (Prevention of Cancer by Intervention with Selenium), 501 elderly volunteers were treated with 100, 200, 300 µg/L selenium or placebo for 6 months. Using adiponectin as an independent predictor of diabetes, there was no effect of selenium supplementation on plasma adiponectin.11 These trials concluded that high-dose selenium supplementation has no benefit on diabetes prevention. Nevertheless, there were few limitations of these trials. First, diabetes risk was either evaluated by surrogate end points or was a secondary outcome in these trials. Second, these participants were treated with adequate to high-dose selenium, which might alter the functions of selenoprotein.31 Third, only men were included in the SELECT, and in the PRECISE trial, the sample size was small and the treatment duration was only 6 months, which restricted the statistical power. Furthermore, there was no record of insulin-mimic or diabetogenic parameters to clarify the mechanism behind the association between selenium and diabetes.
Linking insulin resistance to selenium and diabetes, the association could be a consequence of pathophysiological changes or might be affected by behind factors. In animal studies, few hypotheses developed to explain the discrimination between animal studies, clinical trials, and observational studies. One study suggested that both maximal expression of selenoproteins and selenoprotein deficiency can promote development of type 2 diabetes-like phenotype in mice.31 High selenium intake may alter the regulation of β cells and impair insulin signaling in rats.32 In previous study, the appropriate plasma selenium concentration to maximize the activity of the antioxidant selenoenzyme was around 95 (range 89–114) µg/L.8 ,33 However, the serum selenium level was low-to-adequate (88.2±21.2 µg/L) in our study, which did not meet the hypothesis of overexpression of selenium in animal model nor exceeded the appropriate exposure of selenium in human study. Another hypothesis focused on different effects of serum selenium level in varied genotype in rats.20 This corresponds to different serum selenium levels noted in different areas; for example, the serum selenium level is low in Europe and adequate in Japan.34 Therefore, the cut-off value of serum selenium in the Asian group needs further investigation. From current findings, we deduced that a higher serum selenium level is associated with a higher prevalence of diabetes. The hypothesis was supported by the National Health and Nutrition Examination Survey (NHANES) for serum selenium concentrations and diabetes in the USA,4 post hoc analysis of NPC trial, and our study. This is the first human study to link insulin resistance and central obesity to the association between selenium and diabetes.
There are some limitations to this study. First, we were not able to establish the causal relationship between serum selenium and diabetes because of the case–control design of the study. Second, although we collected and adjusted for probable confounders in our study, there might be unmeasured factors indicating a possible residual effect. For example, there were potential influences of long-term disease on lowering serum selenium levels over time, but we did not collect time elapsed from disease diagnosis among diabetic individuals. Third, our measurement of insulin resistance was not based on accurate dynamic techniques such as with euglycemic clamps but through HOMA-IR, an indirect measure of the degree of insulin resistance. This is the first human study to link insulin resistance and central obesity to the association between selenium and diabetes. Adjusting for WC and HOMA-IR removed the association of serum selenium levels with diabetes mostly but not the highest quartile of the selenium group, which implied that unsealed factor(s) independent of insulin resistance might influence glucose metabolism through a different pathway. Except for the evidence of a direct association between serum selenium level and diabetes risk, which is mediated by central obesity and insulin resistance, there might be some other unidentified factors and mechanisms that need further investigation.
Acknowledgments
The authors would like to thank Ms Wen-Chao Weng, Ms Yi-Ju Chen, and Ms Yi-Fang Hsieh for help in questionnaire collection, data archiving, and administrative support.
References
Footnotes
Contributors C-WL analyzed the data and wrote the manuscript. C-WL, H-HC, K-CY, C-SK, L-TL, and K-CH researched the data, reviewed and edited the manuscript, and contributed to the discussion. K-CH takes responsibility for the integrity and accuracy of the data analysis.
Funding This work was supported in part by the National Health Research Institutes, Taiwan (grant numbers: PH-104-PP-27).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of National Taiwan University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.