Article Text

Abstract
Objective To evaluate the weight loss efficacy of a novel mobile platform delivering the Diabetes Prevention Program.
Research Design and Methods 43 overweight or obese adult participants with a diagnosis of prediabetes signed-up to receive a 24-week virtual Diabetes Prevention Program with human coaching, through a mobile platform. Weight loss and engagement were the main outcomes, evaluated by repeated measures analysis of variance, backward regression, and mediation regression.
Results Weight loss at 16 and 24 weeks was significant, with 56% of starters and 64% of completers losing over 5% body weight. Mean weight loss at 24 weeks was 6.58% in starters and 7.5% in completers. Participants were highly engaged, with 84% of the sample completing 9 lessons or more. In-app actions related to self-monitoring significantly predicted weight loss.
Conclusions Our findings support the effectiveness of a uniquely mobile prediabetes intervention, producing weight loss comparable to studies with high engagement, with potential for scalable population health management.
- Behavioral Interventions
- Body Weight
- Pre-Diabetes
- Telemedicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
To the best of our knowledge, this study is the first fully mobile translation of the Diabetes Prevention Program.
A National Diabetes Prevention Program (NDPP) intervention delivered entirely through a smartphone platform showed high engagement and 6-month transformative weight loss, comparable to the original NDPP and comparable to traditional in-person programmes.
This pilot shows that a novel mobile NDPP intervention has the potential for scalability, and can address the major barriers facing the widespread translation of the NDPP into the community setting, such as a high fixed overhead, fixed locations, and lower levels of engagement and weight loss.
Introduction
Lifestyle interventions,1 including the National Diabetes Prevention Program (NDPP) have proven effective in preventing type 2 diabetes.2 ,3 Online delivery of an adapted NDPP has resulted in high levels of engagement, weight loss, and improvements in glycated hemoglobin (HbA1c).4 ,5 Prechronic and chronic care efforts delivered by other means (text and emails,6 nurse support,7 DVDs,8 community care9) have also been successful in promoting behavior change, weight loss, and glycemic control. One study10 adapted the NDPP to deliver the first part of the curriculum in-person and the remaining sessions through a mobile app, and found 6.8% weight loss at 5 months. Mobile health poses a promising means of delivering prechronic and chronic care,11 ,12 and provides a scalable, convenient, and accessible method to deliver the NDPP.
The weight loss efficacy of a completely mobile delivery of a structured NDPP has not been tested. The main aim of this pilot study was to evaluate the weight loss efficacy of Noom's smartphone-based NDPP-based curricula with human coaching in a group of overweight and obese hyperglycemic adults receiving 16 weeks of core, plus postcore curriculum. In this study, it was hypothesized that the mobile DPP could produce transformative weight loss over time.
Research design and methods
A large Northeast-based insurance company offered its employees free access to Noom Health, a mobile-based application that delivers structured curricula with human coaches. An email or regular mail invitation with information describing the study was sent to potential participants based on an elevated HbA1c status found in their medical records, reflecting a diagnosis of prediabetes. Interested participants were assigned to a virtual Centers for Disease Control and Prevention (CDC)-recognized NDPP master’s level coach.
Hyperglycemic males and females (HbA1c between 5.7% and 6.4%) between the ages of 18 and 75 years old who signed-up for Noom's NDPP (figure 1, n=121) between 6/22/2015 and 9/7/2015 were included in the study. Of 121, individuals were considered ‘interested’ (n=62) if they performed at least one in-app action during the first week of the curriculum. From 62 interested participants, those having <2 weigh-ins (n=8) past baseline and who did not read more than one article per week for 4 or more weeks were considered non-starters and were excluded from final analyses. An additional subject did not provide any information. Participants who read at least one article during any 4 of the 16 initial weeks were considered to have started, in accordance with the CDC's definition. ‘Starters’ (n=43) must have also messaged the coach at least one time within the first month. ‘Completers’ (n=36) read at least one article per week during any 9 of the 16 weeks.
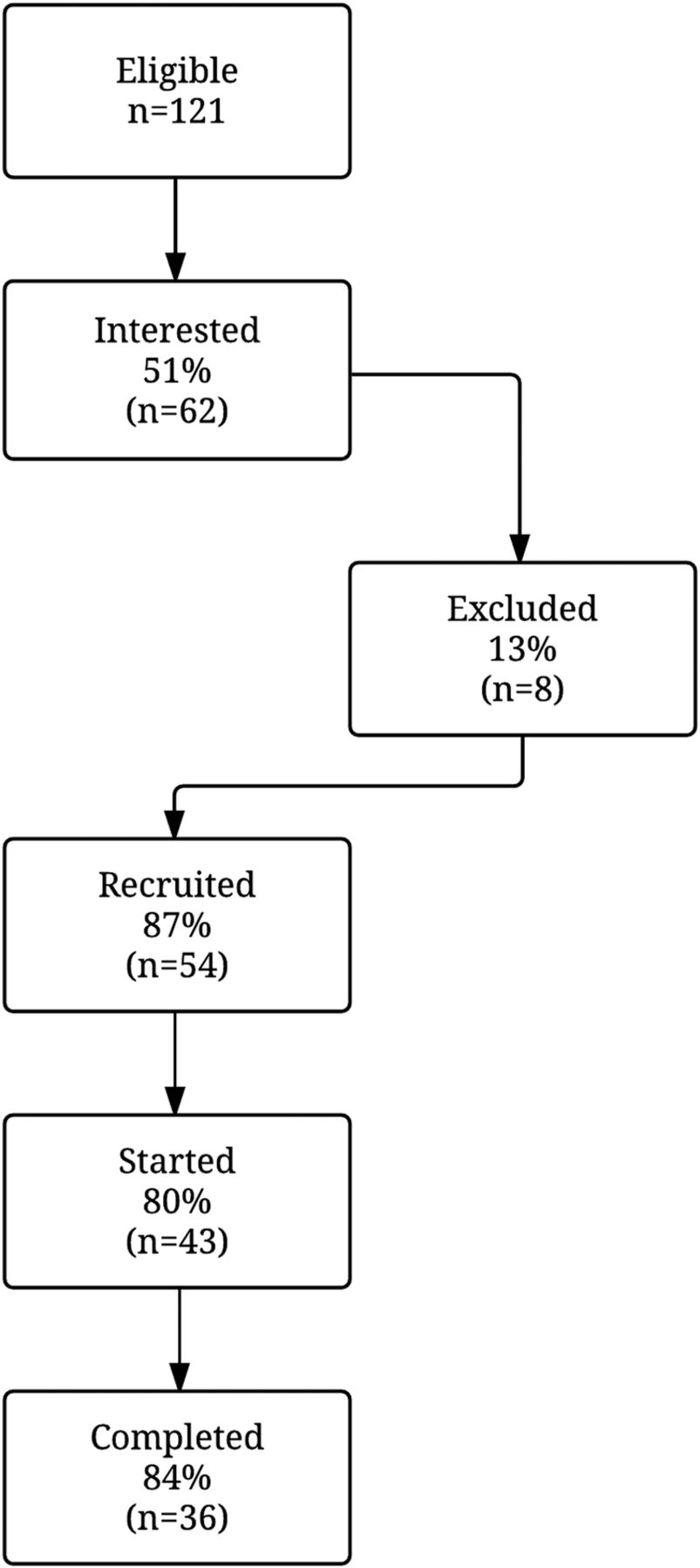
Flow chart for study recruitment, starting and completion status. Eligible, participants who signed-up and were included in the study; interested, individuals that performed at least one in-app action during the first week of the NDPP curriculum; recruited, participants who read at least one article during any 4 of the 16 initial weeks and also messaged the coach at least one time within the first month; completers, read at least one article per week during any 9 of the 16 weeks; excluded, participants who had <2 weigh-ins (n=8), none of which were considered ‘starters’.
During the first week of the study, participants received orientation on what the DPP entails, and learnt how to use the Noom app, interact with their coach, and the importance of maintaining motivation throughout the programme. Participants received daily DPP content through informative articles and interactive challenges, and were asked to log their weight, meals, and physical activity in-app on a weekly basis. The NDPP coach communicated with the participants daily via in-app private and group messages, and brief telephone calls approximately two times per month. Coaches securely monitored participant progress through a dashboard. The present study reports 24-week (6 month) results, including the16-week core DPP phase, followed by the first 8 weeks of the postcore DPP phase.
Statistical analysis
Descriptive statistics, expressed as means±SD, were calculated for subject baseline characteristics. Independent samples t-test compared descriptive baseline characteristics among non-starters and starters. Repeated measurements analysis of variance (ANOVA) distinguished the effect of time on weight change. This method extracts the contribution of the subjects from the error term. A post hoc ANOVA method, the pairwise Fisher's exact test, examined differences from baseline for the 16-week and 24-week weights. Ad hoc ANOVA tests examined the effect size of the change in weight from baseline to 16 and 24 weeks. Backward regression analyses examined whether engagement variables predicted weight loss at 16 and 24 weeks. Further mediation regression analyses explored potential influence of engagement variables on other independent variables, to understand the prediction of weight change, and a Sobel test examined the significance of the mediation. Significance tests were two-sided at significance p<0.05. Statistical analyses were performed using Minitab V.17 and SPSS V.21 software.
Power analysis
Sample size was determined by using the estimated SD of change in body mass index (BMI) from an intervention study of patients with hyperglycemia (n=75). A SD of 1.49 kg/m2 and α of 0.05 produced a final sample of study participants of 44 at 90% power, to identify a minimum detectable difference in change in BMI of 0.8 kg/m2 in a one-sample t-test.
Results
Baseline characteristics of recruited participants, non-starters, starters, and completers are shown in the table 1. Of 121, 78 were non-starters. In both groups, non-starters and starters, the majority of the sample was female, but the proportion was significantly higher in the starters. Starters were also significantly older than non-starters. Baseline weight and height were not different between groups. Approximately 85% of the starters were female, with a mean age of 51 years at recruitment. All starters were overweight or obese at baseline, with mean weight of 96 kg and BMI of 35 kg/m2. No significant differences were observed between starters and completers.
Baseline, weight change, and engagement characteristics of study starters and completers
Weight loss and BMI change at 16 and 24 weeks were significant (table 1), with 56% of starters and 64% of completers losing over 5% body weight at 24 weeks (6.58% and 7.5% mean weight loss, respectively). Weight loss increased steadily over time, but there was no significant difference between 16 and 24 weeks. Ad hoc ANOVA tests indicated that weight loss was significant at 16 weeks for starters (M=−5.40, SD=4.43, p<0.001, d=1.22) and completers (M=−6.00, SD=4.34, p<0.001, d=1.38). Weight loss was also significant at 24 weeks from baseline in starters (M=−6.22, SD=5.00, p<0.001, d=1.24) and completers (M=−7.01, SD=4.83, p<0.001, d=1.45). Participants showed a high level of engagement, with 84% of the sample completing nine lessons or more (CDC standard).
In-app activities reflecting engagement significantly predicted weight loss among starters and completers. Backward regression analysis examined the impact of various in-app actions on percent weight loss at 6 months for starters (table 1). User actions that significantly predicted these variables were the number of weekly weigh-ins and the number of meals logged. Number of group posts remained in the second-to-last model as an insignificant predictor of percent weight loss. The significant variables explained 43% of the variance. For every SD increase in meals logged, percent weight loss increased by 0.36 SDs (β=0.357, p=0.016). Every SD increase in weigh-ins increased weight loss by 0.39 SDs (β=0.389, p=0.009). Mediation regression analyses further explained the chain of relations between group posts, meals logged and percent weight loss.
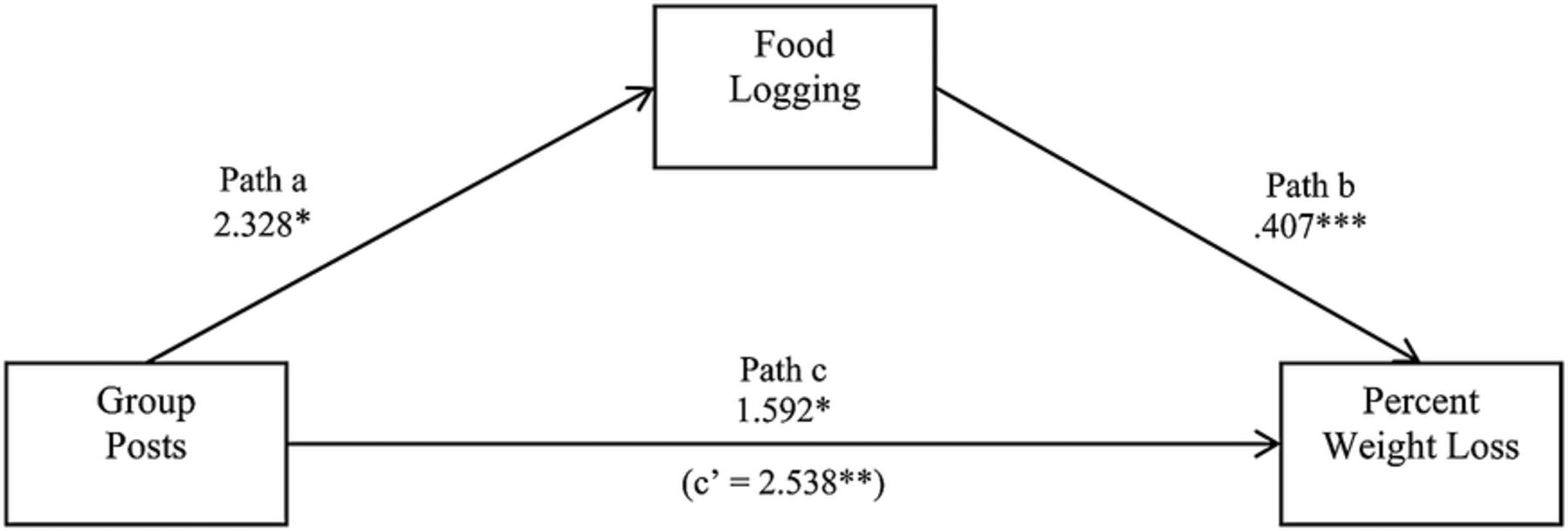
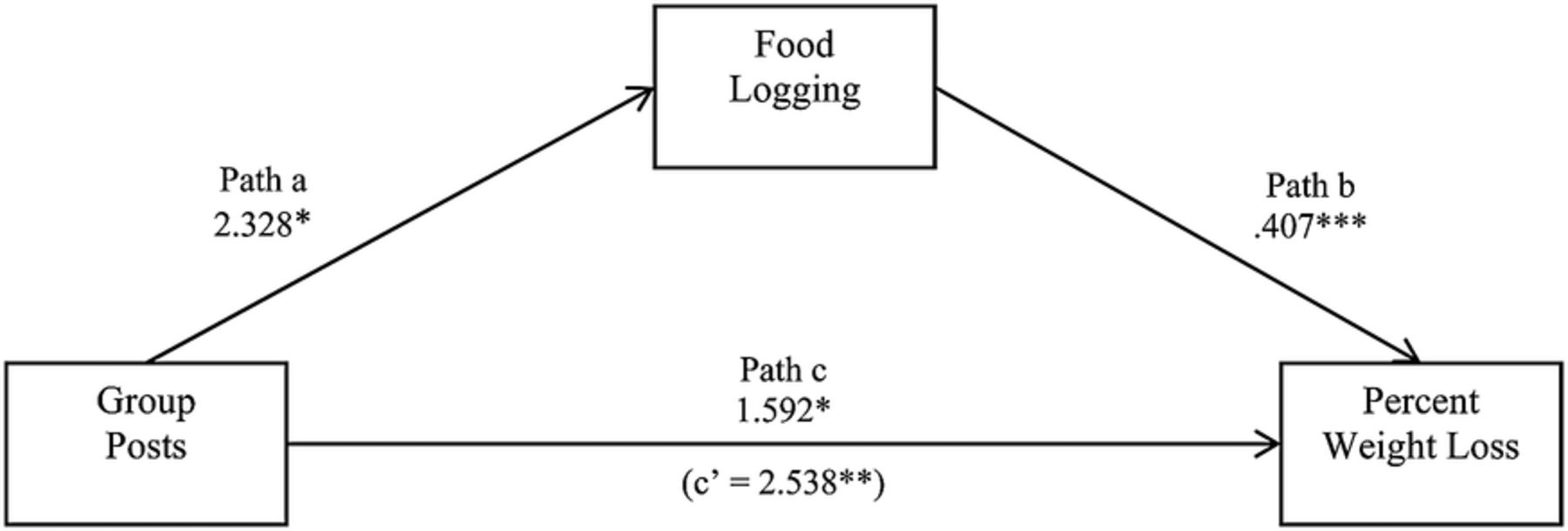
Mediation results are illustrated in figure 2. In the first model, path a, group posts were significantly associated with food logging (F(1:42)=4.99, R2=0.11, p=0.031), such that those who made group posts logged 2.33 additional meals. Group posts were significantly associated with percent weight loss (F(1:41)=8.84, p=0.005) in path c. Approximately 17% of the variance in percent weight loss is explained by group posts, where group posts were a significant unique predictor of percent weight loss (β=2.54, p=0.005). In the final model, partial mediation was shown (path b and c), (F(2,40)=12.24, p<0.001), where the model accounted for 38% of the percent weight loss, and group posts became a marginally significant predictor of percent weight loss (β=1.59, p=0.052), but meals logged remained significant (β=0.407, p=0.001). A Sobel test was marginally significant (p=0.057), suggesting that meal logging partially mediated the relationship between group posts and percent weight loss.
{kind=link}
{kind=link}
Food logging mediation of group posts on percent weight loss. *p<0.05, **p<0.01, ***p<0.001.
Conclusions
This pilot study, designed to evaluate weight loss by means of a novel NDPP intervention delivered entirely through a smartphone platform, showed 6-month weight loss comparable to the original NDPP and traditional in-person programmes.13 ,14 Completers represented 84% of the sample and lost 7.01 kg (15.45 lbs, 7.50%) body weight at 24 weeks, surpassing 5–7% weight loss recommended by the CDC,15 and showing a high level of acceptance and programme feasibility. Completers also showed a trend toward higher general engagement and weight loss.
For all users, weekly weigh-ins and meals logged were the main predictors of weight loss, supporting the importance of self-monitoring in weight loss. Group posts alone were a significant predictor of percent weight loss. Since it also remained in the second-to-last backward regression model predicting percent weight loss, further mediation regression analyses were performed. The analyses revealed that meals logged partially mediated the group posts–weight loss relationship. This suggests that meal logging is influenced by group behavior, which ultimately impacts weight loss. Thus, it is important to provide individuals enrolled in a NDPP with not only an extensive food database and ability to log meals with ease, but also with the social support to maximize logging behavior.
To the best of our knowledge, this is the first fully mobile translation of the DPP. Web-based delivery of an adapted NDPP resulted in high levels of engagement, improvements in HbA1c, and similar but smaller degrees of weight loss.4 ,5 Mobile health implementation of NDPP appears to be comparable to current community-based programmes and more flexible than web-based implementations. It addresses the major barriers facing the widespread translation of the NDPP in the community setting; including high fixed overhead, fixed locations, and lower levels of engagement and weight loss. Only one study10 adapted the NDPP to deliver the first part of the curriculum in-person and the remaining sessions through a mobile app, and found 6.8% weight loss at 5 months. Our findings support the effectiveness of a uniquely mobile intervention, producing weight loss comparable to studies with high engagement with potential for scalable population health management.
A limitation of this study is the absence of a control group and a limited 6-month duration. However, our results are comparable to 6-month outcomes (weight loss and glucose) in the DPP, which have been shown to be predictive of 3-year diabetic risk reduction.16 Second, this study did not measure HbA1c, but others have found no significant changes in HbA1c at 165 or 24 weeks.10 ,16 A larger clinical trial of mobile DPP with an in-person NDPP control group is recommended to establish intervention efficacy, identify behaviors that increase participant engagement, and assess physiological markers of diabetes risk longitudinally.
In conclusion, this pilot demonstrates scalability and feasibility of a novel mobile NDPP intervention with weight loss comparable to online and gold standard in-person core and postcore interventions. Future longitudinal studies are warranted to verify this study’s findings.
Acknowledgments
The authors would like to thank all the participants in this study. This study would not have been possible without the coaches Peter Athans, MS; Jennifer Major, MS, RD; and Steven Keem, MS (Noom). The authors are also grateful to David González-Barreto, PhD (University of Puerto Rico—Mayagüez) for his assistance and input with statistical analyses, and to Kayla Reynolds, MS (Curriculum and Content Department at Noom) for her editorial assistance.
References
Footnotes
Contributors TT-R wrote the manuscript and conducted data analyses. AM is the principal investigator. AM co-wrote the manuscript and conducted data analyses. AM is also the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. CR is the research coordinator, reviewed the manuscript, and oversaw the conduct of the study. MW is the coach manager, provided oversight to coaching and training with AM, and reviewed the manuscript. KF provided medical input in the study development, and co-wrote and reviewed the manuscript.
Competing interests None declared.
Ethics approval An advisory review Institutional Review Board (IRB) letter was obtained after study completion stating the study protocol would have been approved.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Owing to confidentiality agreements with research collaborators, supporting data can only be made available to bona fide researchers subject to a non-disclosure agreement on agreement by both parties. Details of the data and how to request access are available by contacting research@noom.com.