Article Text

Abstract
Background Contemporary treatment guidelines advise statin use in all patients with diabetes for reducing coronary risk. Use of statins in patients with type 2 diabetes has not been reported from India.
Methods We performed a multisite (n=9) registry-based study among internists (n=3), diabetologists (n=3), and endocrinologists (n=3) across India to determine prescriptions of statins in patients with type 2 diabetes. Demographic and clinical details were obtained and prescriptions were audited for various medications with a focus on statins. Details of type of statin and dosage form (low, moderate, and high) were obtained. Patients were divided into categories based on presence of cardiovascular risk into low (no risk factors, n=1506), medium (≥1 risk factor, n=5425), and high (with vascular disease, n=1769). Descriptive statistics are presented.
Results Prescription details were available in 8699 (men 5292, women 3407). Statins were prescribed in 55.2% and fibrates in 9.2%. Statin prescription was significantly greater among diabetologists (64.4%) compared with internists (n=53.3%) and endocrinologists (46.8%; p<0.001). Atorvastatin was prescribed in 74.1%, rosuvastatin in 29.2%, and others in 3.0%. Statin prescriptions were lower in women (52.1%) versus men (57.2%; p<0.001) and in patients aged <40 years (34.3%), versus those aged 40–49 (49.7%), 50–59 (60.1%), and ≥60 years (62.2%; p<0.001). Low-dose statins were prescribed in 1.9%, moderate dose in 85.4%, and high dose in 12.7%. Statin prescriptions were greater in the high-risk group (58.0%) compared with those in the medium-risk (53.8%) and low-risk (56.8%) groups (p <0.001). High-dose statin prescriptions were similar in the high-risk (14.5%), medium-risk (11.8%), and low-risk (13.5%) groups (p=0.31).
Conclusions Statins are prescribed in only half of the clinic-based patients in India with type 2 diabetes. Prescription of high-dose statins is very low.
- Asian Indians
- Lipid-Lowering Drugs/Medication
- Atorvastatin
- Health Service Delivery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
There are no contemporary data on statin prescriptions among patients with type 2 diabetes in India.
In a multisite study in India, we observed suboptimal prescription of statins in patients with diabetes. A prescription of high-dose statins was low in all patients with diabetes, including those at high risk.
Statin prescriptions were significantly less by endocrinologists and physicians compared with diabetologists.
Introduction
Diabetes is an epidemic in India.1 It is also associated with a greater prevalence of macrovascular and microvascular disease and these patients have a higher long-term mortality as compared with patients in developed countries.2 ,3 Multiple factors are responsible for greater morbidity and mortality from diabetes in India and include low awareness, treatment, and control of glycemia in patients with diabetes.4 ,5 Greater prevalence and low awareness, treatment, and control of cardiovascular risk factors (smoking, hypertension, dyslipidemia, and unhealthy lifestyles), especially in lower socioeconomic status patients, is also important.6
Control of cardiovascular risk factors such as hypertension and hypercholesterolemia in patients with diabetes can prevent complications. It has been reported that appropriate use of statins can prevent symptomatic coronary heart disease as well as acute coronary events in patients with type 2 diabetes in all populations including South Asians.7 ,8 Patients with type 2 diabetes have a long-term risk of cardiovascular mortality similar to patients without diabetes and overt cardiovascular disease.8–12 Based on these epidemiological observations and primary prevention trials, many international guidelines recommend routine use of statins in patients with type 2 diabetes.8 ,13–15 The American College of Cardiology/American Heart Association (ACC/AHA) 2013 statement classified diabetes as a coronary risk equivalent and recommended high-dose statin therapy in all patients with diabetes.8 Diabetes registries in developed countries, for example, the Swedish National Diabetes Register, have reported a high use of statins in patients with type 2 diabetes.16 No similar data are available from developing countries, including India. Previous studies that reported treatment patterns in type 2 diabetes in India were published before the recent recommendations17–20 and a review reported suboptimal quality of diabetes management in India.21 Therefore, to document the extent of prescriptions of statins and their types in patients with type 2 diabetes and to correlate this with vascular risk status of these patients, we performed a multisite registry-based study.
Methods
We performed a multisite (n=9) registry-based study in eight cities across India to determine the prescription pattern of statins in patients with type 2 diabetes. The Institutional Ethics Committee at the central coordinating center at Jaipur, India, approved the study. Requirement of informed consent from each patient was waived by the Ethics Committee because anonymized data were used for analyses. We obtained data on successive patients attending the outpatient department at respective centers until the target of 500 patients was reached at each site. A larger sample size was available at the primary site where the pro forma was piloted.20
Demographic and clinical details were obtained that were similar to the previous India Heart Watch study.4 An abbreviated version useful for a disease registry was used in the present study.20 Sociodemographic factors were education, occupation, and socioeconomic status and lifestyle factors included details of smoking and tobacco use, physical activity patterns and diet. Details of concomitant risk factors—overweight or obesity (body mass index ≥25 kg/m2), hypertension, hypercholesterolemia (total cholesterol ≥200 mg/dL), hypertriglyceridemia (triglycerides ≥150 mg/dL), and low high-density lipoprotein (HDL) cholesterol (<40 mg/dL in men, <50 mg/dL in women)—as well as duration of diabetes were also obtained. Presence of microvascular diseases was ascertained from medical records with a focus on diabetic retinopathy, chronic renal disease (serum creatinine ≥2.0 mg/dL), and overt diabetic foot disease. We did not obtain details of the presence of microalbuminuria, proteinuria, albumin–creatinine ratio, or ankle–brachial index due to lack of uniform data at all sites. Presence of macrovascular disease was obtained from the patients and included history of overt coronary heart disease, history of stroke, or symptomatic peripheral arterial disease with claudication.
Physicians were divided by specialization into specific type of care provider as internists (n=3), diabetologists (internists with primary interest in diabetes, n=3), and board-certified endocrinologists (n=3). Patients were also subdivided accordingly into internists (n=2301), diabetologists (n=3299), and endocrinologists (n=3099). Patients were also categorized based on the presence of cardiovascular risk into low, medium, and high risk. Risk factors other than diabetes were used in classification and were either smoking or tobacco use, hypertension, or hypercholesterolemia. Details of overt microvascular disease (retinopathy, chronic renal failure, serum creatinine ≥2.0 mg/dL, diabetic foot) or macrovascular disease (coronary heart disease, history or presence of stroke, symptomatic peripheral vascular disease) were also recorded. Low-risk patients had no risk factor other than diabetes (n=1506), moderate-risk patients had any one of these risk factors (n=5425), and high-risk patients were participants with microvascular or macrovascular disease (n=1769).
Prescriptions were audited for various medications including lipid-lowering, antidiabetic, and antihypertensive drugs. We obtained details of type of statin (atorvastatin, rosuvastatin, other statins) and daily dose in mg/day. Frequency of prescription of fibrates (fenofibrate) was also obtained. Low-dose statin prescription was defined as atorvastatin <10 mg/day, simvastatin <20 mg/day, or rosuvastatin <5 mg/day; moderate dose as atorvastatin 10–20 mg/day, simvastatin 20–40 mg/day, or rosuvastatin 5–10 mg/day; and high dose as atorvastatin 40–80 mg/day or rosuvastatin 20–40 mg/day according to the ACC/AHA guidelines.8
Statistical analyses: All the data were computerized and quality checks were performed to reduce duplicate and redundant data. Statistical analyses were performed using SPSS for Windows (SPSS, V.13.0). Descriptive statistics are presented with unadjusted data and proportions. Intergroup comparisons were performed using χ2 test. p Values <0.05 were considered significant.
Results
We obtained detailed prescriptions for 8699 patients with type 2 diabetes (men 5292, women 3407). Recruitment at different sites was Jaipur (3 sites, n=3714, 42.7%), Nagpur (n=1536, 17.7%), Madurai (n=971, 11.2%), Dibrugarh (n=796, 9.2%), Lucknow (n=792, 9.1%), Udaipur (n=548, 6.3%), and Jodhpur (n=342, 3.9%). Patients were subdivided according to level of care into the internists' group (n=2301, 26.5%), diabetologists' group (n=3299, 37.9%), and endocrinologists' group (n=3099, 35.6%). Demographic and clinical details of the study participants are shown in table 1. Twelve per cent of the study participants were <40 years of age. Most of the patients had diabetes for >2 years and a third for >5 years. Risk factor details were available for most patients (table 1). Smoking and/or tobacco use was one-fifth while moderate-to-high physical activity in less than half. Hypertension was present in 51.5%, with total cholesterol ≥200 mg/dL in 34.9%, low-density lipoprotein cholesterol ≥100 mg/dL in 50.0%, triglycerides ≥150 mg/dL in 35.2%, and low HDL cholesterol in 48.9%. Hypothyroidism was present in 9.2% and was more in women (13.0%). Coronary heart disease was present in 15.4% and others (stroke, large vessel peripheral arterial disease in 5.2% while microvascular complications such as retinopathy, diabetic foot or advanced chronic renal disease (creatinine ≥2.0 mg/dL) was in 6.1%, 13.9%, and 6.8%, respectively.
Demographic and clinical characteristics of the study cohort
Use of lipid-lowering drugs and others is shown in table 2. Statins were prescribed in 4802 (55.2%) patients, significantly more in men (57.2%) compared with women (52.1%; p<0.001). Use of fibrates was low (9.2%). Insulins were used in 15.8%, more in men (16.8%) as compared with women (14.2; p=0.016). Use of antihypertensive drugs is also shown in table 2. The most frequently used drugs were renin angiotensin system blockers, ACE inhibitors, or angiotensin receptor blockers in 36.4% of patients, while diuretics (31.8%), β-blockers (27.6%), and calcium channel blockers (23.7%) were prescribed in lesser proportions.
Prescription audit of drug therapies in the study cohort
Statin prescription was significantly greater by diabetologists (n=2126/3299, 64.4%) compared with internists (n=1227/2301, 53.3%) and endocrinologists (n=1449/3099, 46.8%; p<0.001; table 2). It was also lower in patients <40 years of age (34.3%), compared with those aged 40–49 years (49.7%), 50–59 years (60.1%), or ≥60 years (62.2%; p<0.001; figure 1). Statin prescriptions were significantly greater in high-risk patients (58.0%) compared with medium-risk (53.8%) and low-risk (56.8%) patients (p <0.001; table 2).

Statins in men and women with diabetes at different age groups show lower prescriptions at younger age groups.
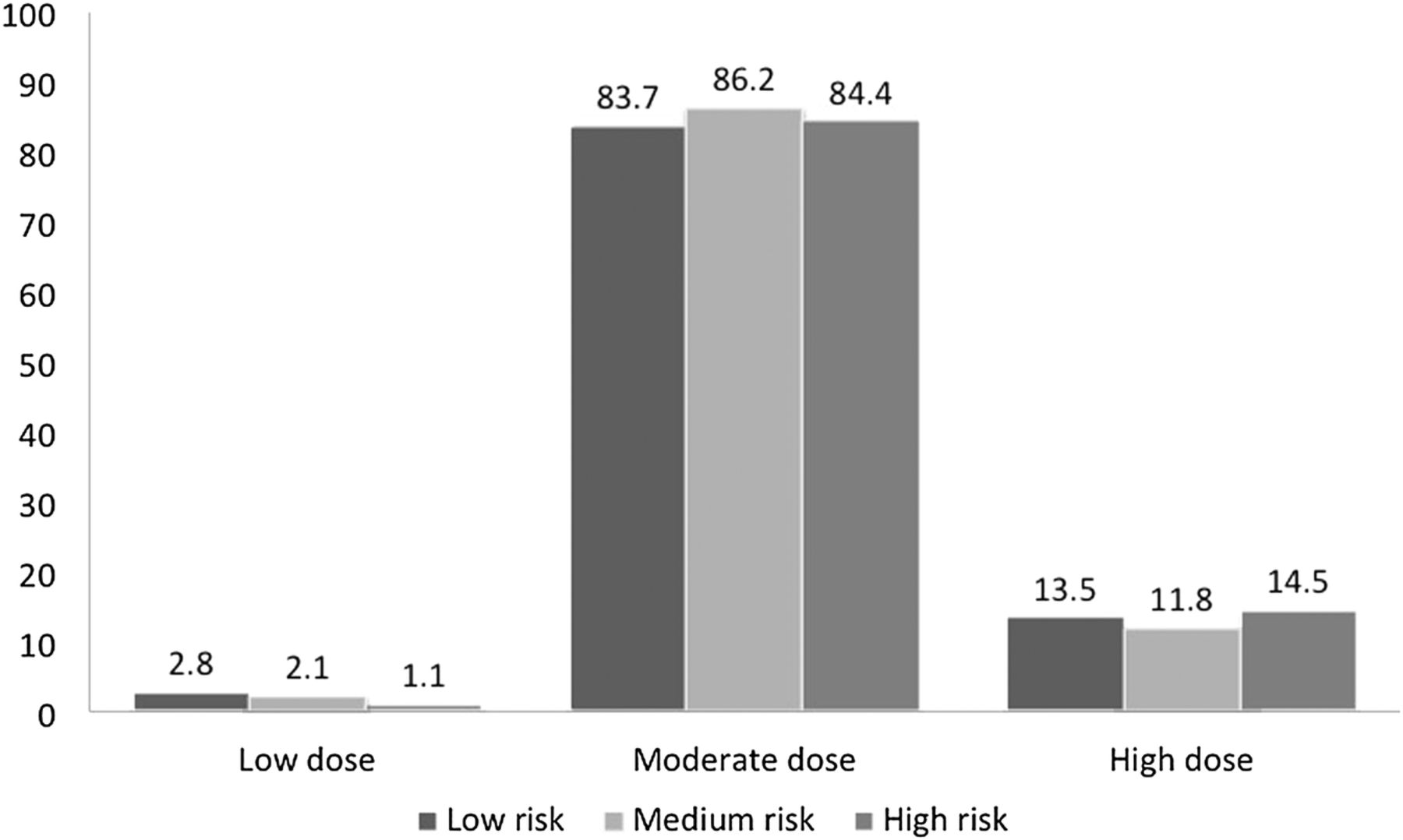
Atorvastatin was the most prescribed statin (n=3560, 74.1% of statin prescriptions), as compared with rosuvastatin (n=1098, 22.9%) or others (simvastatin or pitavastatin; n=144, 3.0%). Of the patients prescribed statins (n=4802), high-dose statins (atorvastatin >20 mg/day or rosuvastatin >10 mg/day)8 were in 610 (12.7%), moderate dose (atorvastatin 10–20 mg/day or rosuvastatin 5–10 mg/day)8 in 4100 (85.4%) and low-dose (atorvastatin <10 mg/day, rosuvastatin <5 mg/day)8 in 92 (1.9%; table 2). Use of high-dose statins was not significantly different in low-risk (13.5%), medium-risk (11.8%), or high-risk (14.5%) patient groups (figure 2).

{kind=link}
{kind=link}
No significant differences in prescriptions of low-dose, moderate-dose, and high-dose statins in low-risk, medium-risk, and high-risk patients with diabetes. Low-risk patients had no cardiovascular risk factors—smoking/tobacco, hypertension; medium-risk patients had diabetes with any one of the above risk factors; and high-risk patients had diabetes with clinical evidence of microvascular or macrovascular disease.
Discussion
This multisite prescription audit and clinical study shows that statins are prescribed in <60% of clinic-based patients with type 2 diabetes in India. High-dose statins, which are recommended in all the patients with diabetes,8 are prescribed in less than one-sixth of patients prescribed statins. Although the prescriptions of statins are significantly greater in high-risk patients with diabetes, the overall prescriptions of statins as well as high-dose statins are suboptimal and much lower than the guidelines.8
Diabetes has long been considered a cardiovascular risk equivalent.22 A Finnish study initially reported that patients with diabetes without manifest coronary heart disease had long-term (7-year) risk of events and mortality similar to patients without diabetes with manifest coronary heart disease.10 Subsequently, a number of observational studies in Australia and Europe reported similar associations.11 ,12 Based on these studies, as well as randomized controlled trials that demonstrated lowering of coronary risk with statins in patients with diabetes,23 the 2013 AHA/ACC guidelines on lipid management recommended that all patients with diabetes should receive high-dose statins irrespective of cholesterol levels.8
Registry-based studies in developed countries have reported increasing statin prescriptions in patients with type 2 diabetes since the guidelines endorsed their use. Prescriptions of statins in patients with diabetes have been reported in a few countries and examples include the Swedish National Diabetes Register,24 US National Health and Nutrition Evaluation Surveys (NHANES),25 British National Health Service (NHS),26 and Australian general practice,27 and the proportion of patients with diabetes prescribed statins varied from 25% to 65%. Studies have also reported that the prescriptions are significantly greater in diabetologists' practices (75%).26 ,27 Targets are more than 90%.14 In our study, statins were prescribed in 55% of patients and, although, are lower than the Swedish and Australian registries and NHANES where these drugs are prescribed in 70–90% of patients,24 ,25 ,27 but, are higher than the British NHS-Check programme.26 However, in our study, the high-dose statins are prescribed in less than a sixth of patients prescribed statins (12.7%) and this is clearly suboptimal. Moreover, our study shows that statin prescriptions are much lower than optimal in patients with type 2 diabetes with known cardiovascular disease (high-risk group, figure 2). It has been recommended that all patients with coronary heart disease should be on a statin.8 ,28 We did not inquire regarding the intake of these drugs by the patients and this is a study limitation. It is well known that even after prescriptions, many patients do not take the statins and other medications for chronic diseases,29 especially in India.30 ,31
The study has multiple strengths as well as limitations. This is one of the largest contemporary registries on diabetes management from India and is especially relevant because it was performed after the publication of AHA/ACC Lipid Guidelines.8 Moreover, we have performed the study at clinics of qualified endocrinologists, as well as of diabetologists and internists who manage the majority of patients with diabetes in India.32 Limitations of the study include lower proportions of patients from the southern and eastern regions of the country and greater proportions from the northern and western regions, non-representation of secondary and primary care physicians who treat the majority of patients with diabetes in India, lack of systematic collection data on microvascular complications (especially renal disease), pragmatic risk classification of the patients which is different from the suggested criteria,33 and lack of patient-level consumption and adherence data. Other limitations include absence of baseline cholesterol levels of these patients to justify high-dose therapies and lack of data on the side effect profile of statins. Moreover, we did not perform a qualitative study to determine causes of low prescriptions of statins by physicians.
In conclusion, this study shows that prescriptions of statins in clinic-based patients with type 2 diabetes in India are suboptimal. Efforts to increase use of these drugs to all patients with diabetes to prevent cardiovascular complications are urgently required. These results are all the more important after the publication of the HOPE-3 study where statin use has been associated with a significant decrease in cardiovascular mortality and acute events in intermediate-risk patients including those with diabetes.34 Strategies to optimize prescriptions are better clinician awareness of guidelines and continuing medical education as well as periodic prescription audits and dissemination of results to improve quality of preventive care among patients with type 2 diabetes.
References
Footnotes
Contributors RG conceived and designed the study, researched the data, and wrote and edited the manuscript. SL, KKS, SKS, SG, and RSK contributed to intellectual discussion and reviewed and edited the manuscript. SL, KKS, SKS, SG, AJA, BNM, AM, DCS, and ASM researched the data. RG is the guarantor.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Ethics Committee, Eternal Heart Care Centre and Research Institute, Mount Sinai New York Affiliate, Jaipur, India.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.