Article Text

Abstract
Objective The fact that population with type 2 diabetes mellitus and bodyweight of patients are increasing but diabetes care is improving makes it important to explore the up-to-date rates of achieving treatment targets and prevalence of complications. We investigated the prevalence of microvascular/macrovascular complications and rates of achieving treatment targets through a large-scale multicenter-based cohort.
Research design and methods A cross-sectional nationwide survey was performed on 9956 subjects with type 2 diabetes mellitus who consecutively attended primary care clinics. The prevalence of nephropathy, retinopathy, neuropathy, and macrovascular complications and rates of achieving targets of glycated hemoglobin (HbA1c) <7.0%, blood pressure <130/80 mm Hg, and lipids of low-density/high-density lipoprotein cholesterol <3.1/≥1.0 mmol/L and non-high-density lipoprotein cholesterol <3.8 mmol/L were investigated.
Results The rates of achieving targets for HbA1c, blood pressure, and lipids were 52.9%, 46.8% and 65.5%, respectively. The prevalence of microvascular complications was ∼28% each, 6.4% of which had all microvascular complications, while that of macrovascular complications was 12.6%. With an increasing duration of diabetes, the rate of achieving target HbA1c decreased and the prevalence of each complication increased despite increased use of diabetes medication. The prevalence of each complication decreased according to the number achieving the 3 treatment targets and was lower in subjects without macrovascular complications than those with. Adjustments for considerable covariates exhibited that each complication was closely inter-related, and the achievement of each target was significantly associated with being free of each complication.
Conclusions Almost half of the subjects examined did not meet the recommended targets. The risk of each complication was significantly affected by 1 on-target treatment (inversely) and the concomitance of another complication (directly). Total diabetes care including one-by-one management of modifiable risk factors and complications may be important for high-quality care. The future studies including more subjects and clinics with precise complication status are needed.
- Treatment
- Microvascular and Macrovascular Complications
- Type 2 Diabetes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
The up-to-date rates of achieving treatment targets and prevalence of complications were surveyed in this study and shown according to the duration of diabetes.
Almost half of the subjects did not meet the recommended targets, and especially the rate of achieving the HbA1c target markedly decreased with longer durations despite increases in the use of any diabetes medication.
Excess bodyweight was associated with deleterious effects on achieving therapeutic targets and prevalence of complications, especially of nephropathy.
Introduction
With the expected increase in the prevalence of type 2 diabetes mellitus (T2DM) in the population, due in part to increasing rates of obesity and decreased physical activity, the burden of microvascular complications, known as diabetic nephropathy, retinopathy, and neuropathy, may also increase.1–3 Diabetic nephropathy is the most common single cause of end-stage renal disease in the USA, Europe, and Japan.4 It is also the leading cause of blindness among working-aged adults worldwide.5 Diabetic neuropathy is associated with considerable morbidity, mortality, and diminished quality of life.6 The estimates of the prevalence of microvascular complications, as well as macrovascular complications, and their relationships with major risk factors are crucial for guiding public health education and the optimal management of diabetes. The prevalence of microvascular complications has been extensively examined; however, most studies have only referred to a single microvascular complication. Few studies have investigated the three microvascular complications simultaneously in the same subjects at the same time point. The prevalence of the overlap of two or three microvascular complications, and its association with macrovascular complications, are important for estimating the future risk of other complications and mortality; however, these issues have not yet been investigated in detail until now.
On the other hand, quality of care for individuals with T2DM may have improved in the past two decades,3 ,7–9 reflecting recent advances in treatments for blood glucose, blood pressure (BP), and lipids. However, the bodyweight of subjects with T2DM is increasing7 ,10 and excess bodyweight is a significant risk factor for increased morbidity and mortality.10 The adverse effects of excess bodyweight on the management of blood glucose, BP and lipids, as well as on the prevalence of microvascular/macrovascular complications in T2DM, have not been sufficiently elucidated. Therefore, it is important to obtain the up-to-date rates of achieving therapeutic targets in association with bodyweight levels and their relationships with diabetic microvascular complications as well as macrovascular complications. The aim of the present study is to investigate the prevalence of three microvascular complications in the same subject with T2DM at the same time, and simultaneously examine the rates of achieving targets in glycated hemoglobin (HbA1c), BP, and lipids through an updated large-scale multicenter-based cohort. Cross-sectional associations between therapeutic target achievements and microvascular/macrovascular complications in association with bodyweight were also examined.
Methods
Study population
Seventeen medical clinics (ie, general practitioners (GPs) specializing in diabetes care) volunteered to participate in this study. These clinics were located in different areas in Japan and used the same software to incorporate patient records in the Japan Diabetes Clinical Data Management (JDDM) Study Group.11 The group consists of medical doctors who have dedicated their time to recording clinical data of their patients during daily clinical practice for scientific analyses. The study was performed in primary care settings. Subjects were at first enrolled from those who consecutively attended these clinics in 2013 and had urinary albumin and serum creatinine (Cr) measured within a year (N=13 039). Among them, subjects who had retinopathy and neuropathy evaluated within a year were registered in this study (N=9956). This covered about 20% of subjects attending the clinics in the JDDM study group. Subjects were treated with the aim of achieving the targets recommended by the Japan Diabetes Society (JDS) of a HbA1c value of <7.0% (53 mmol/mol), BP<130/80 mm Hg, and serum concentrations of low-density lipoprotein (LDL) cholesterol <3.1 mmol/L (120 mg/dL), high-density lipoprotein (HDL) cholesterol ≥1.0 mmol/L (40 mg/dL),12 and non-HDL cholesterol <3.8 mmol/L (150 mg/dL). The most common treatment practices during the study period included dipeptidyl peptidase-4 inhibitors with metformin for blood glucose, angiotensin II receptor blockers for BP, and statins for lipids. The study protocol was approved by the Ethics Committees of the JDDM. All patients provided informed consent and the study was performed in accordance with Helsinki Declaration II.
Measurements
BP was measured with an appropriately sized cuff in the sitting position after resting for at least 5 min, using an automated standardized BP device. Non-fasting blood samples were drawn and analyzed to measure serum Cr and lipids at local laboratories. HbA1c was measured by high-performance liquid chromatography, which has been certified by the American National Glycohemoglobin Standardization Program. Serum and urinary concentrations of Cr were measured by an enzymatic method. Urinary albumin was measured using random urine samples, in the absence of menstruation and urinary tract infection, by a turbidimetric immunoassay. The urinary albumin excretion rate was recorded as the albumin-to-creatinine ratio (ACR). Normoalbuminuria, microalbuminuria, and macroalbuminuria were defined as ACR<30, ACR≥30 and <300, and ACR≥300 mg/g Cr, respectively. Glomerular filtration rate (GFR) was estimated using the following equation by the Japanese Society of Nephrology: estimated glomerular filtration rate (eGFR) (mL/min/1.73 m2)=194×serum creatinine (Scr)−1.094×Age−0.287×0.739 (if female).13 Chronic kidney disease (CKD) was defined by ACR≥30 mg/g Cr or eGFR<60 mL/min/1.73 m2. LDL cholesterol was calculated by Friedewald's formula. Regarding the treatment of diabetes, subjects were divided into groups treated by diet alone, hypoglycemic tablets, tablets with insulin, and only insulin. Macrovascular complications, that is, cardiovascular diseases (CVD) of coronary artery disease (CAD), ischemic stroke, and peripheral artery disease (PAD), including coronary, cerebrovascular, and carotid revascularization, were noted. PAD was diagnosed when intermittent claudication occurred, with the confirmation of an ankle-brachial pressure index <0.9 or significant peripheral artery stenosis by angiography, or leg amputation above the ankle as a result of diabetes.
Subjects attended the clinic every 1–2 months. This prevalence study focused on the presence of microvascular complications and conditions related to diabetes in the early stages. In order to assess diabetic retinopathy, subjects were referred to an eye clinic at least once a year. Diabetic retinopathy was diagnosed after pupillary dilation by an ophthalmologist using ophthalmoscopy. According to the Early Treatment Diabetic Retinopathy Study grading standards,14 background retinopathy was defined as the presence of one or more retinal microaneurysms or retinal blot hemorrhages and proliferative retinopathy was diagnosed as the presence of new vessels in the retina or vitreous hemorrhage. In order to assess diabetic peripheral neuropathy, subjects underwent an annual physical examination. Diabetic neuropathy, which is referred to as diabetic symmetrical sensorimotor polyneuropathy, diabetic polyneuropathy, or diabetic peripheral neuropathy, was diagnosed in patients with two or more of three components, as recommended in the simplified diagnostic criteria proposed by the Diabetic Neuropathy Study Group in Japan:15 (1) subjective symptoms in the bilateral lower limbs or feet; (2) loss of or decreased ankle jerk reflex and (3) decreased vibration perception, assessed using a C128 tuning fork and bilaterally measured at the medial malleoli.
Statistical analysis
Data were expressed as the mean±SD if normally distributed. The significance of differences between groups was assessed by χ2 tests for categorical variables and analysis of variance (ANOVA) for continuous variables. A multivariate logistic regression analysis was performed to investigate the clinical variables associated with the presence of nephropathy, retinopathy, neuropathy, and CVD. The covariates were sex, age, duration of diabetes, body mass index (BMI), HbA1c on target, BP on target, lipids on target, and eGFR in model A. Model B additionally included nephropathy, retinopathy, and neuropathy. A p value of <5% (two-tailed) was considered significant. All analyses were performed with the statistical software package SPSS (SPSS Japan, Tokyo, Japan).
Results
Rates of achieving treatment target and prevalence of microvascular and macrovascular complications
The clinical characteristics of subjects with T2DM are shown in table 1. Of the 9956 subjects with an average age of 65 years, duration of 14 years, BMI of 24.9 kg/m2, BP of 126/72 mm Hg, and HbA1c of 7.04%, 29.5% had nephropathy including 23.9% with microalbuminuria and 5.6% with macroalbuminuria, 26.4% had any retinopathy, and 27.7% had neuropathy. According to the duration of diabetes, the proportions of the use of insulin, antihypertensive and lipid-lowering agents, albuminuria, retinopathy, neuropathy, and macrovascular complications of CAD and stroke increased significantly. The values of HbA1c, systolic BP, HDL cholesterol, and serum Cr increased with a longer duration of diabetes, whereas the values of BMI, diastolic BP, LDL cholesterol, non-HDL cholesterol, and eGFR decreased. According to the duration, the rate of achieving HbA1c target decreased significantly, whereas the rate for BP was unchanged and that for lipids increased.
Clinical characteristics of subjects with T2DM
Figure 1 shows the rates of achieving the targets for HbA1c, BP, and lipids (figure 1A) and prevalence of microvascular complications (figure 1B) in the 9956 subjects. A total of 20.8% achieved all three targets, whereas 11.8% achieved none of the targets. Among all subjects, 6.4% had all three microvascular complications, whereas 45.7% had none. The relationships between achieving treatment targets with the presence/absence of each complication are shown in online supplementary table S1. A clear correlation was found between achieving each target and the absence of each complication except for lipids with retinopathy.
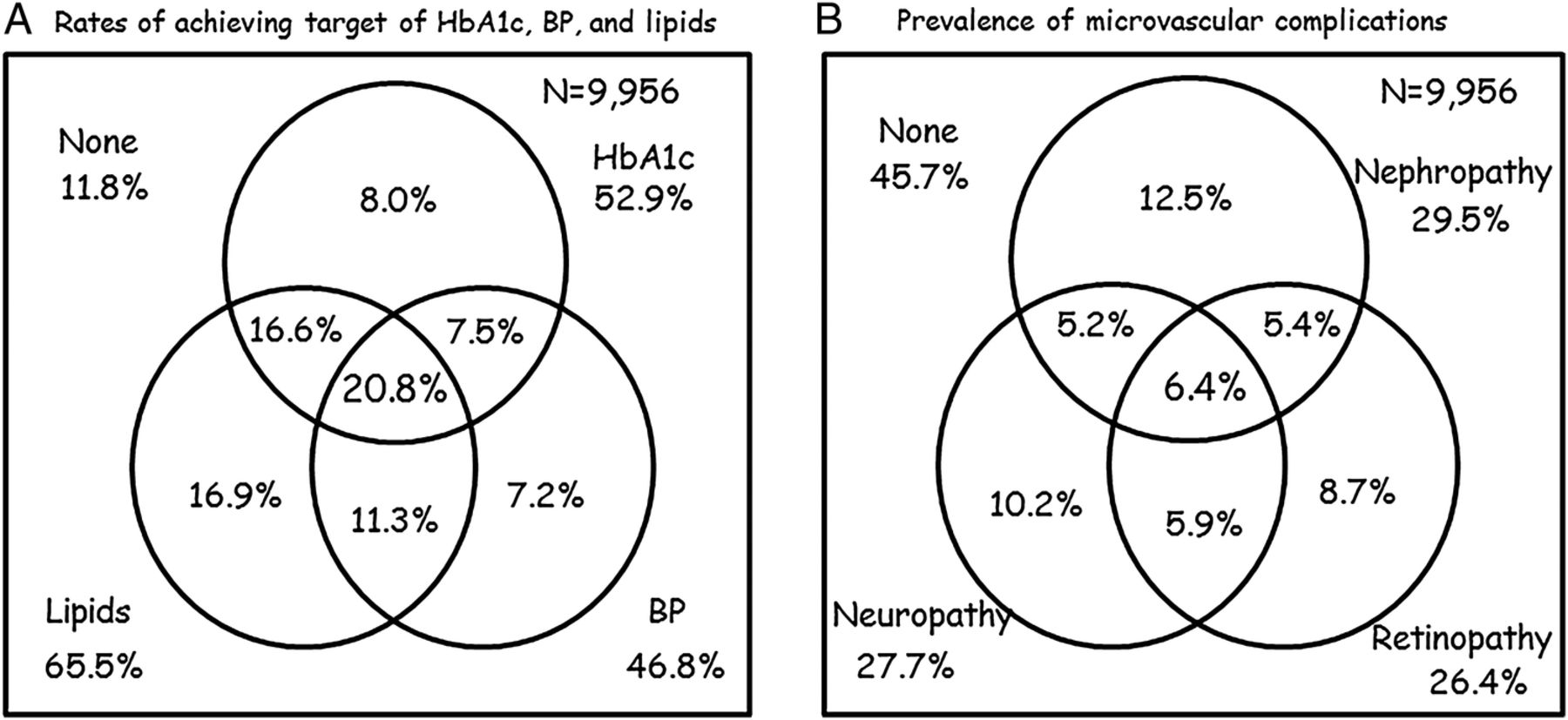
(A) Rate of achieving targets for glycated hemoglobin (HbA1c), blood pressure (BP), and lipids in all subjects and (B) prevalence of nephropathy, retinopathy, and neuropathy in subjects with type 2 diabetes mellitus (n=9956).
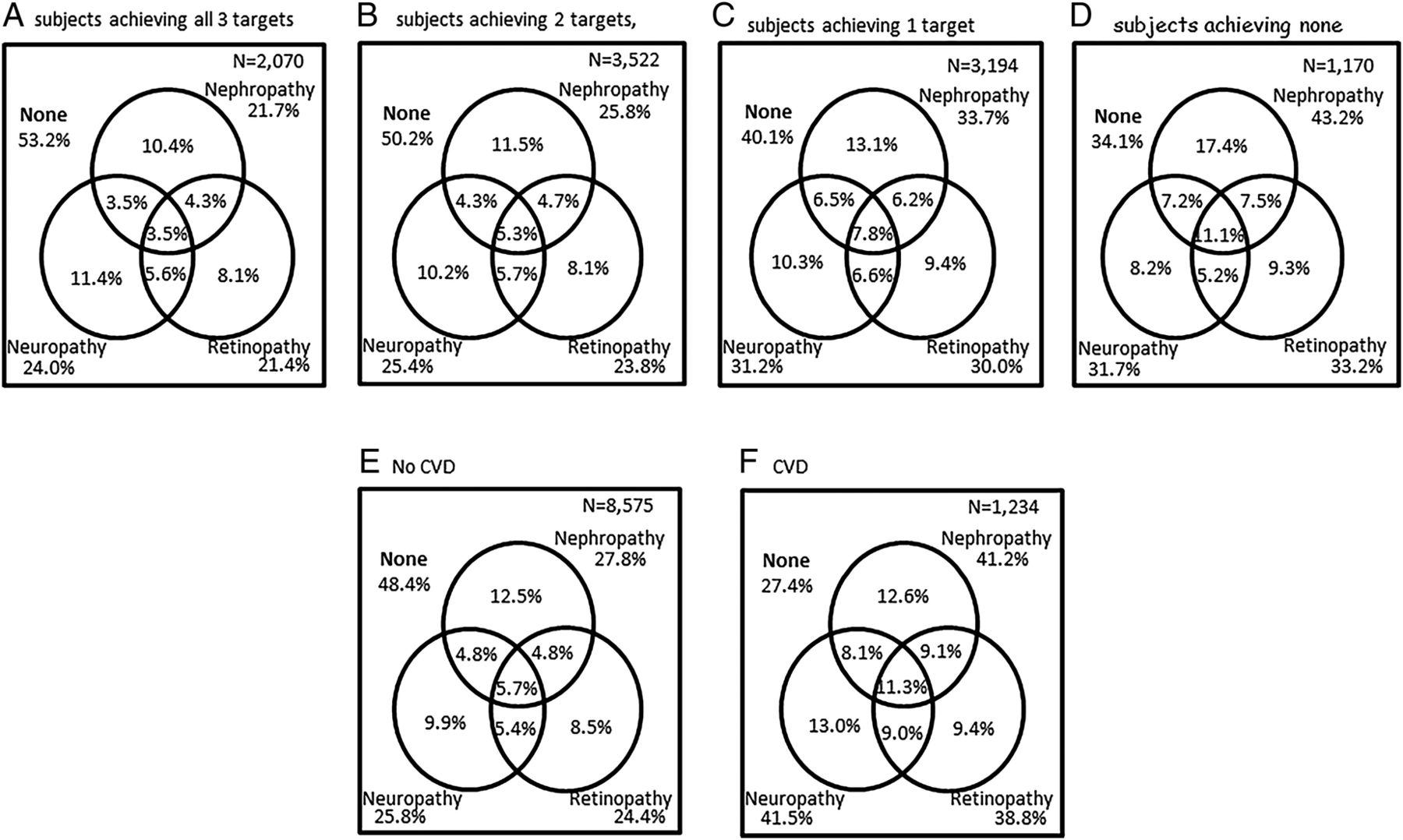
Figure 2 indicates the prevalence of the three microvascular complications by the number of achievements out of the three treatment targets (figure 2A–D) and between subjects with and without CVD (figure 2E, F). The proportion free from any complication was highest at 53.2% in subjects achieving three treatment targets, and decreased step by step, reaching 34.1% in subjects achieving no targets (χ2 score 179.4, p<0.001). In contrast, the prevalence of all three microvascular complications was the lowest at 3.5% in subjects achieving three treatment targets, and increased to 11.1% in subjects achieving no targets (χ2 score 89.9, p<0.001). Subjects with CVD evidently had a higher prevalence of nephropathy, retinopathy, and neuropathy than those without CVD (p<0.001, respectively).
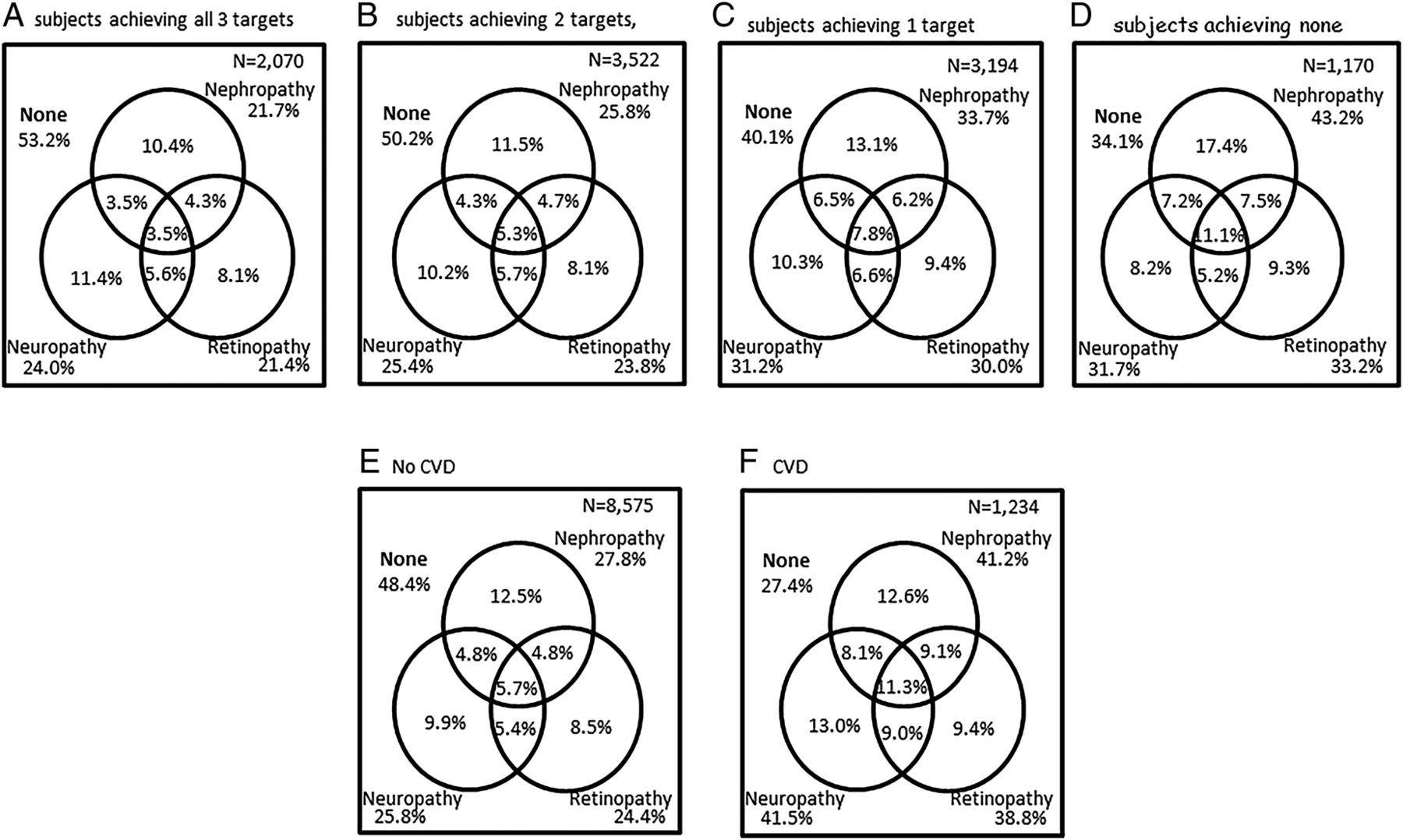
Prevalence of nephropathy, retinopathy, and neuropathy in subjects achieving all (A) three targets, (B) two targets, (C) one target, and (D) none, and in subjects (E) without cardiovascular diseases (CVD) and (F) with CVD.
Effects of BMI on microvascular and macrovascular complications
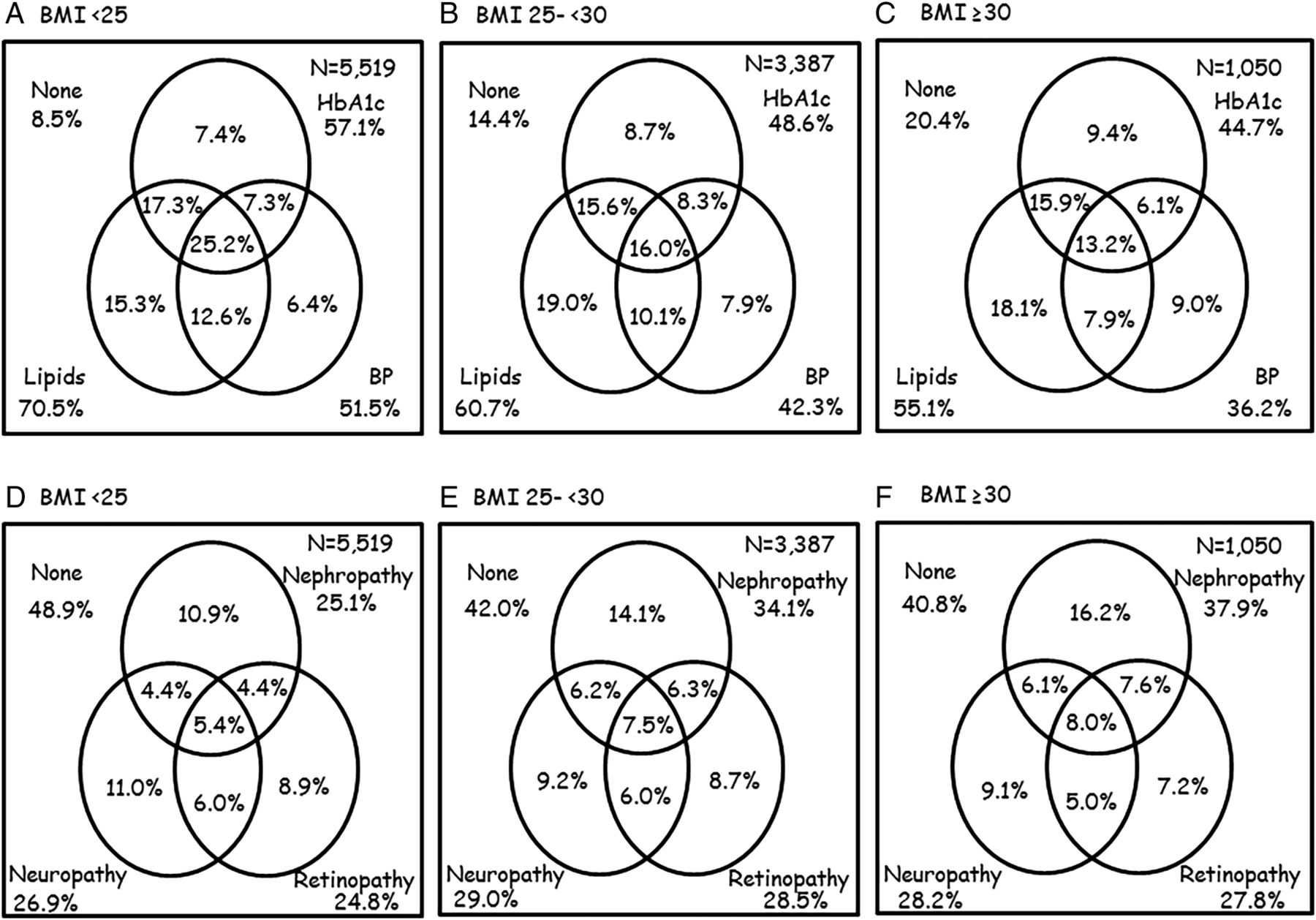
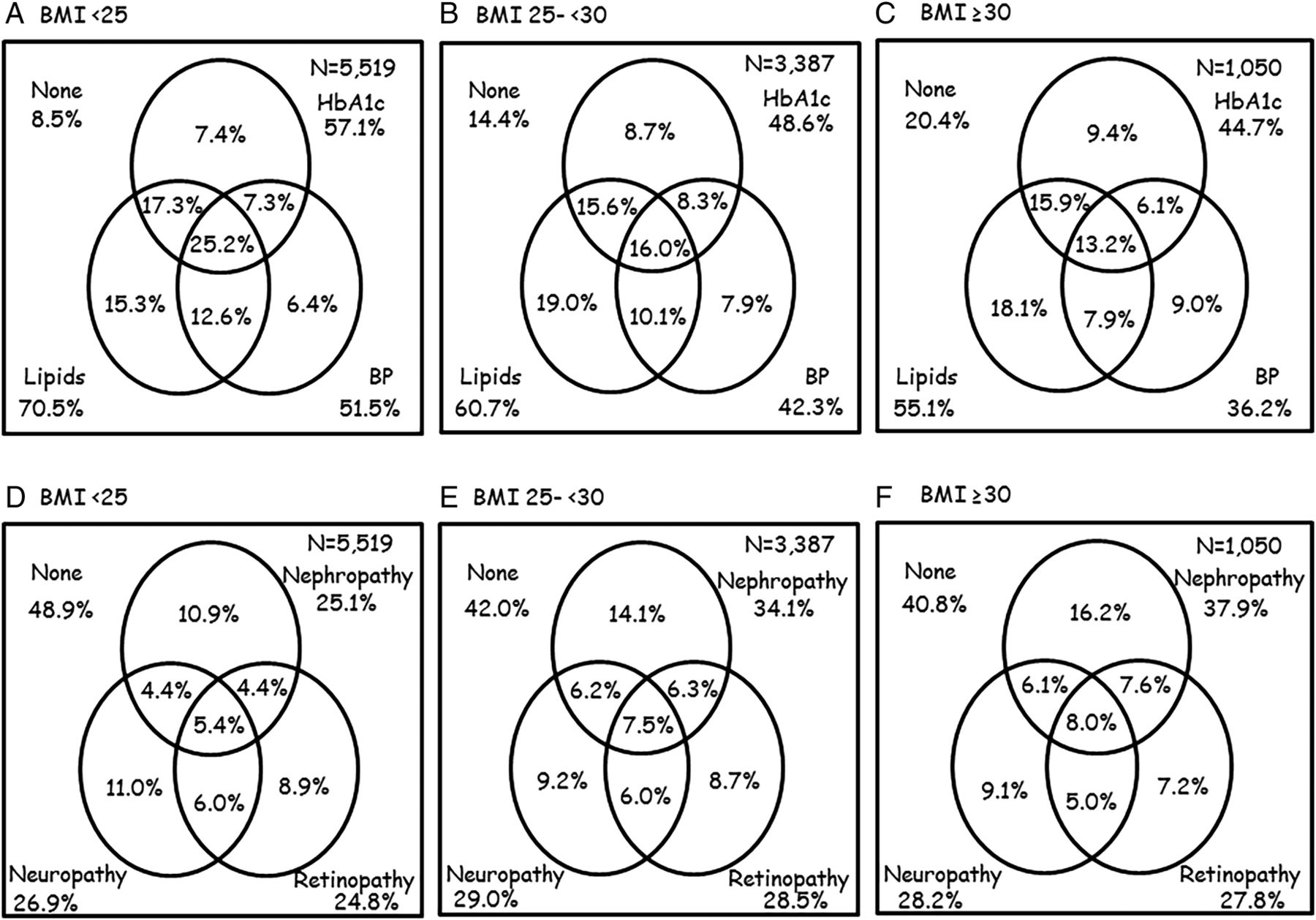
The relationships of BMI levels with achieving targets for HbA1c, BP, and lipids, and prevalence of nephropathy, retinopathy, and neuropathy are shown in figure 3. Increasing BMI levels correlated with decreasing rates of all three target achievements (p<0.001, respectively). The prevalence of nephropathy and retinopathy increased significantly with higher BMI levels (χ2 score 122.0, p<0.001; χ2 score 15.6, p<0.01, respectively), whereas neuropathy was not associated with BMI levels (χ2 score 4.7, not significant).
{kind=link}
{kind=link}
{kind=link}
Associations of body mass index (BMI) levels with achieving targets for glycated hemoglobin (HbA1c), blood pressure (BP), and lipids in the upper panels A, B, and C, and with the prevalence of nephropathy, retinopathy, and neuropathy in the lower panels of D, E, and F.
Risk analyses for microvascular and macrovascular complications
We investigated whether the levels of albuminuria and eGFR are associated with the prevalence of retinopathy, neuropathy, and CVD, and the results obtained are shown in online supplementary table S2. The higher levels of albuminuria and lower levels of eGFR significantly increased the prevalence rates of retinopathy, neuropathy, and CVD. To explore variables associated with nephropathy, retinopathy, neuropathy, and CVD, multivariate logistic regression analyses were performed, as shown in table 2. Regarding microvascular complications, achieving treatment targets for HbA1c and BP were significantly associated with nephropathy and retinopathy independent of the effects of sex, age, duration, BMI, and eGFR, whereas achieving the treatment targets for lipids was significantly associated only with nephropathy and neuropathy. Regarding CVD, nephropathy, retinopathy, and neuropathy were independently associated with CVD after adjustments for the effects of sex, age, duration, BMI, and eGFR, whereas achieving targets for BP and lipids were not.
Multivariate logistic regression analysis to examine variables associated with nephropathy, retinopathy, neuropathy, and CVD
Discussion
This study provides the latest estimates of the prevalence of nephropathy, retinopathy, and neuropathy in association with putative risk factors including achievement of the treatment targets for HbA1c, BP, and lipids, CVD, and weight excess, for subjects with T2DM attending GPs in the JDDM study in Japan. In a large-scale multicenter-based survey conducted in 2013, we found that 52.9% achieved HbA1c<7.0%, 46.8% achieved BP<130/80 mm Hg, and 65.5% achieved the target for lipids, which yielded 20.8% that met all three treatment targets and 11.8% that achieved none of the targets. On the other hand, the prevalence of nephropathy, retinopathy, and neuropathy was ∼30% each, 6.4% of which had all three microvascular complications and 45.7% had no microvascular complications. Notably, when a subject had a complication, the overlap rates of other microvascular complications were high; for instance, out of subjects with retinopathy, 67% (17.7/26.4%) had other microvascular complications. This was prominent when subjects had CVD. The prevalence of microvascular as well as macrovascular complications became higher with increases in the duration of T2DM. Importantly, the rate of achieving the HbA1c target markedly decreased with longer durations despite increases in the use of any diabetes medication (tablets or insulin), whereas the rate of achieving the BP target remained unchanged. The rate of achieving the lipids target increased with longer durations; this may partly be explained by the lower BMI and higher use of lipid-lowering agents.
The proportions that met the treatment targets in this study are similar to those reported among 1444 subjects with adult diabetes from the National Health and Nutrition Examination Survey (NHANES) data surveyed in 2010.9 The findings showed 52.2% with HbA1c<7.0%, 51.3% with BP<130/80 mm Hg, 56.8% with LDL cholesterol <130 mg/dL, and 14.3% that met all three targets. Regarding the prevalence of microvascular complications, the JDDM study reported that those of normoalbuminuria/albuminuria were 69.7/30.3% in 2004,16 which were similar to the present survey. There have been many studies on the prevalence of retinopathy. Previous studies, with the number of subjects with T2DM being ∼10 000 or more and published in the past decade, showed the prevalence of any retinopathy to be 30.3% (26 216/86 390) in Wales,17 16.3% (8584/52 736) in Portugal,18 12.3% (13 387/108 723) in Catalonia,19 19.3% (8409/43 523 in newly diagnosed T2DM) in Scotland,20 and 25.3% (16 094/63 622) in Norfolk.21 Compared with the studies on retinopathy, there have been fewer studies on the prevalence of neuropathy, and the number of subjects examined was also smaller. The previous reports showed the prevalence of neuropathy to be 29.2% (586/2006) in India,22 30.5% (1100/3591) in Verona,23 33.1% (1113/3359) in China,24 and 33.5% (1338/4000) in Korea.25 The prevalence rates described above were subject to population characteristics such as the duration of diabetes, ethnicity, and risk factors including blood glucose and BP control; however, these factors were not sufficiently considered in the above studies and referred to only a single microvascular complication.
In this cross-sectional design, we found strong relationships between achieving targets for HbA1c, BP and lipids and being free of nephropathy, retinopathy, and neuropathy. After adjustments for gender, age, duration, BMI, and eGFR in the multivariate logistic regression analysis, achieving each target independently correlated (inversely) with nephropathy, retinopathy, and neuropathy, except for the effect of lipids control on retinopathy. This result appears to support glycemic control as well as BP and lipid controls, being essential for preventing the three microvascular complications. Furthermore, we found that the number achieving the treatment targets correlated inversely with the prevalence of microvascular complications. This result indicates the importance of achieving treatment targets one by one. These inhibitory effects were not observed with CVD; the reason for this may be that BP and lipids are aimed at stricter levels than before the onset of CVD. Nevertheless, HbA1c on target correlated with being free of CVD. The absence of a relationship between lipids and retinopathy was supported by other studies, in which serum lipids were associated with severe macular edema but not with retinopathy.26 ,27 The underlying mechanism suggested that lipid extravasation is restricted in the retina by the blood–retinal barrier and disruption of this barrier, rather than increased lipid levels, is required for lipid-induced retinal injury.28
Higher BMI levels were associated with the reduction of the rates of achieving therapeutic targets for HbA1c, BP, and lipids. This deleterious impact of excess bodyweight on blood glucose, BP, and lipids is consistent with the concept that excess bodyweight is now the sixth most important risk factor contributing to the overall burden of diseases worldwide.29 ,30 The pathological mechanisms underlying obesity-related resistance to each treatment include insulin resistance in the nitric oxide pathway, the stimulatory effects of hyperinsulinemia on sympathetic drive, smooth muscle growth, and sodium–fluid retention, and increased angiotensin II.31 ,32 The smaller number of achieving therapeutic targets in subjects with higher BMI may reflect the increasing prevalence of nephropathy and retinopathy. The marked increase observed in the prevalence of nephropathy may be associated with the incremental involvement of obesity-related kidney disease, in which increased angiotensin II activity is suggested to play a central role in hypertension, dyslipidemia, and insulin resistance.32 BMI per se was found to be an independent risk of nephropathy, retinopathy, and neuropathy in the present multiple logistic regression analyses. This may suggest a causal role of higher BMI in the pathogenesis of microvascular complications that should be investigated in the future.
This study identified close and strong links as well as inter-relationships between each complication, that is, one microvascular complication was closely related to another microvascular complication and a macrovascular complication. Furthermore, the elevated albuminuria and decreased eGFR levels were closely related to retinopathy, neuropathy, and macrovascular complications. This cross-sectional study is unable to refer to the causal relationship; however, these results would indicate that one microvascular complication or abnormal levels in albuminuria or eGFR strongly increase the risk of developing other microvascular and macrovascular complications. Several reports support our findings of the close association of retinopathy with albuminuria,33 ,34 GFR,34 ,35 and CVD,36 and that of CVD with albuminuria and GFR,37 ,38 whereas few studies described the association of neuropathy with albuminuria and GFR.39 Our findings were supported by a recent study which indicated the clear associations of the number of microvascular complications with the onset of CVD in the prospective manner.40 Endothelial cells, if exposed to chronic hyperglycemia, develop intracellular hyperglycemia, because they cannot downregulate glucose transport.41 A common pathological trait of diabetic microvascular disease is progressive narrowing and eventual occlusion of vascular lumina,42 and hyperglycemia may trigger and initiate endothelial dysfunction leading to macrovascular disease.43 Taken together, it is important to emphasize that multifactorial treatments for and the assessment of each complication including albuminuria and GFR are essential for high-quality diabetes care.
Our study is subject to several limitations. First, a selection bias may have been caused by participating GPs specializing in diabetes care that influenced the results; the prevalence might be lower with a higher rate of achieving treatment targets than in real-world practice. In contrast, a possibility that severely complicated subjects were referred to these participating GPs because they were specializing in diabetes care cannot be excluded, which might have led to worse outcomes. For subjects with severe complications, the GPs consult with cardiologists, nephrologists, ophthalmologists, and specialists at tertiary care centers, but mostly continue to take care of the patients depending on the severity, even after discharging the hospitals. Second, we should acknowledge that we did not extensively investigate severity in terms of proliferative retinopathy and autonomic neuropathy because we focused on the presence of a microvascular complication and conditions related to diabetes in their early stages. Third, analyses were restricted to individuals in whom complete information was available on prevalent microvascular diseases, and thus may have been subject to a selection bias. An examination of the rates of achieving treatment target and prevalence of complications, as well as the association between risks and microvascular/macrovascular diseases, among individuals with data missing on all three diseases showed no qualitative difference with the complete cohort. Fourth, macrovascular complication data were missing in 147 subjects (1.5%), which was trivial. The strength of this survey is that it was based on patient records provided by physicians, which is more accurate than self-reported data from patients. In the absence of a nationally registered system in Japan, this largest multicenter-based study is likely to be representative of subjects with T2DM.
In conclusion, almost half of the subjects did not meet the recommended targets. In the absence of a nationally registered system in Japan, this largest survey is likely to represent and provide a robust estimate of the national target achieving rates and prevalence of complications in T2DM. The risk of each complication was significantly affected by one on-target treatment (inversely) and the concomitance of another complication (directly). Total diabetes care including one-by-one management of modifiable risk factors and complications may be important for high-quality care. The future studies including more subjects and clinics with precise complication status are needed.
Acknowledgments
Ms Sanae Horiguchi-Watanabe and Mr Suguho Takahashi (Jiyugaoka Medical Clinic) are thanked for their skilful data collection and analyses. The following clinics from the JDDM study group contributed to this study: Fukumoto Clinic (Kagoshima), HEC Science Clinic (Kanagawa), Hikari Clinic (Nara), Hotaruno Central Clinic (Chiba), Iizumi Clinic (Ibaraki), Iwasaki Clinic (Yamaguchi), Jiyugaoka Medical Clinic (Hokkaido), Kawai Clinic (Ibaraki), Kurihara Clinic (Hokkaido), Mirai Kunitachi Clinic (Tokyo), Oishi Clinic (Kyoto), Okuguchi Clinic (Miyagi), Sugimoto Clinic (Fukuoka), Takai Clinic (Kanagawa), Takamura Clinic (Tokyo), Tama Center Mirai Clinic (Tokyo), Wakamatsu Memorial Hospital (Kagoshima), and Yagi Clinic (Okinawa).
References
Footnotes
Contributors HY, MO, HT, and YK designed the study. HY generated data in collaboration with the study group office. HY and SA performed statistical analyses. All authors contributed to the interpretation of the data and drafting of the manuscript. HY takes responsibility for statistical method and organized for performing multivariate analysis. All authors critically reviewed the manuscript. HY is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Ethics approval The study protocol was approved by the Ethics Committees of the JDDM.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are shared by HY, MO, HT, KY, SS, DU, HS, YK, and the study group office.