Article Text

Abstract
Objective To quantify the association between diabetes and the risk of incident infections by conducting a systematic review and meta-analysis.
Research design and methods Two reviewers independently screened articles identified from PubMed, EMBASE, Cochrane Library, IPA, and Web of Science databases. Cohort studies (CS) or case–control studies (CCS) evaluating the incidence of infections in adults with diabetes were included. Infections were classified as: skin and soft tissue, respiratory, blood, genitourinary, head and neck, gastrointestinal, bone, viral, and non-specified infections. Study quality was assessed using the Newcastle-Ottawa Quality Assessment Scale. Summary crude and adjusted OR with 95% CIs were calculated using random effects models, stratified by study design. Heterogeneity was measured using the I2statistic and explored using subgroup analyses.
Results A total of 345 (243 CS and 102 CCS) studies were included. Combining adjusted results from all CS, diabetes was associated with an increased incidence of skin (OR 1.94, 95% CI 1.78 to 2.12), respiratory (OR 1.35, 95% CI 1.28 to 1.43), blood (OR 1.72, 95% CI 1.48 to 2.00), genitourinary (OR 1.61, 95% CI 1.42 to 1.82), head and neck (OR 1.17, 95% CI 1.13 to 1.22), gastrointestinal (OR 1.48, 95% CI 1.40 to 1.57), viral (OR 1.29, 95% CI 1.13 to 1.46), and non-specified (OR 1.84, 95% CI 1.66 to 2.04) infections. A stronger association was observed among CCS: skin (OR 2.64, 95% CI 2.20 to 3.17), respiratory (OR 1.62, 95% CI 1.37 to 1.92), blood (OR 2.40, 95% CI 1.68 to 3.42), genitourinary (OR 2.59, 95% CI 1.60 to 4.17), gastrointestinal (OR 3.61, 95% CI 2.94 to 4.43), and non-specified (OR 3.53, 95% CI 2.62 to 4.75).
Conclusion Diabetes is associated with an increased risk of multiple types of infections. A high degree of heterogeneity was observed; however, subgroup analysis decreased the amount of heterogeneity within most groups. Results were generally consistent across types of infections.
- Diabetes
- infection
- observational studies
- systematic review
- meta-analysis.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Immune system dysfunction in people with diabetes is thought to make these individuals more liable to infections. Certain infections appear more prevalent in patients with diabetes.
What are the new findings?
This study extends the current state of knowledge about the association between diabetes and the incidence of common infections. Furthermore, gaps within the literature are identified.
How might these results change the focus of research or clinical practice?
The knowledge generated from this review will help further inform physicians and researchers and aid in a better understanding of the magnitude and precision of the association between diabetes and developing infections.
Introduction
The International Diabetes Federation estimates that there were almost 400 million people living with diabetes throughout the world in 2014. The prevalence of diabetes is expected to increase to more than 590 million people by the year 2035.1 Well-known complications of diabetes include both microvascular (retinopathy, neuropathy, nephropathy) and macrovascular (coronary heart disease, cerebrovascular disease, and peripheral vascular disease)2; however, there are numerous lesser known complications including effects on immunity.3–5 Immune system dysfunction in people with diabetes may be mediated through impaired migration, phagocytosis, intracellular killing, and chemotaxis.4–8 Indeed, several studies have suggested that people with diabetes are at an increased risk of infection-related mortality9 10; however, not all studies support such an association.11 12 Furthermore, patients with diabetes tend to be hospitalized for infections more frequently than those without.3
Although previous studies suggest that certain infections are more prevalent in patients with diabetes,13 there is still lack of substantive and consistent evidence regarding whether diabetes is associated with an increase in the incidence of infections.14–16 To our knowledge, there has not been an attempt to thoroughly summarize the existing evidence of the association between diabetes and incident infections and quantify the association across a spectrum of infectious diseases. Therefore, we conducted a systematic review and meta-analysis to provide a comprehensive summary of the current state of the evidence surrounding the relationship between diabetes and incident infections.
Research design and methods
Study design
This systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) and MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines during all stages of design, implementation and reporting.17 18
Eligibility criteria
This review included observational studies assessing the association between diabetes and incident infections. Study designs that were eligible for inclusion were cohort studies (CS), case–control studies (CCS), nested case–control or case–cohort studies. Other study designs such as systematic reviews and meta-analyses, case series, case reports, or cross-sectional studies were excluded from this review as the temporality between exposure and outcome is uncertain. Studies were included if the population studied was 18 years and older. We excluded younger population due to the fact that the immune system of this category is still developing, and this could affect our outcome of interest. Studies were required to report the number of incident infections in patients with diabetes and in patients without diabetes. Classification of the type of diabetes was based on the definition used in each study. Studies including any type of diabetes were eligible including type 1 diabetes, type 2 diabetes, gestational diabetes, other, and unspecified diabetes. We categorized outcomes into the following categories: infection (not specified), respiratory tract infections (RTI; upper and lower), genitourinary tract infections, skin and soft tissue infections (SSTI), gastrointestinal infections, head and neck infections (H&NI), viral infections, and any other infections not classified here.
Data sources and searches
The search strategy was carried out in collaboration with a research librarian experienced in systematic reviews. We searched the following biomedical databases from inception to December 31, 2013: PubMed, EMBASE, the Cochrane Library, International Pharmaceutical Science, and Web of Science. MeSH and free-text terms were used to search PubMed. EMTREE and free-text terms were used to search EMBASE. In searching the Cochrane Library, MeSH terms were used as well as free-text terms to capture items not indexed with MeSH. The remaining databases were searched using free-text terms. The search was restricted to English language. See Appendix A for a sample of the search strategy.
Study selection
Two independent reviewers (WAA, AR) screened titles and abstracts, and then went on to screen full-text manuscripts. Identification of relevant studies was through the use of a standardized study eligibility/relevance form. Discrepancies were resolved by consensus. If consensus was not achieved, a third reviewer was consulted.
Data extraction and quality assessment
Data were extracted by one reviewer onto a predesigned form that included first author, contact details, journal citation, year of publication, study design, funding, sample size, data set used, study location and duration, duration of follow-up, study population characteristics, statistical analysis used, the study-specific measure of association, and type of exposure. Two independent reviewers (JD, PH) verified the accuracy of the extracted data. The quality of the observational studies was appraised through the Newcastle-Ottawa Quality Assessment Scale (NOS)19 according to the procedures recommended in the Cochrane Handbook of Systematic Reviews. One author assessed the methodological quality of all the selected studies. The NOS includes a ‘star system’ in which a study is judged on three domains: selection of the study groups (four items); comparability of the groups (two items); and ascertainment of either the exposure or outcome (three items). If any item of the NOS (eg, case definition or exposure ascertainment) is not reported, a zero score is given. Studies score one star for each area addressed, with scores between 0 and 9 (the highest level of quality). We classified study quality according to the study score into poor (score 0–3), moderate (score 4–6) and high quality (score 7–9).
Data synthesis and analysis
Characteristics of included studies were described and stratified by study design. DerSimonian-Laird random effects models were used to pool results from included studies for each outcome within CS and CCS. Furthermore, unadjusted and adjusted results were pooled separately. Adjusted results were pooled from measures of association reported from the most adjusted statistical model from each study (covariates used in the models varied across included study and are reported in Appendix C). For dichotomous data, the results are expressed as OR with corresponding 95% CI. For continuous data, the results are expressed as weighted mean difference (WMD) with 95% CIs, or as standardized WMD if applicable (ie, outcomes are conceptually the same but measured differently).
Supplementary Material
Supplementary Appendix 2As this review included only observational studies, a greater level of heterogeneity was expected. Heterogeneity was tested using the χ2 test and measured using the I2 test. Sensitivity analyses were undertaken to explore the influence of different variables on the overall estimate of effect and as potential sources of heterogeneity including specific types of infections within categories and study quality (low, moderate, high NOS score). Analysis was conducted using STATA/SE V.12.0.
Results
The study selection process is shown in figure 1. There were a total of 345 studies included, 243 CS and 102 CCS. Study characteristics and the types of infections reported in the included trials are listed in table 1. Most of studies were conducted in North America (55%) followed by Europe (29%). The mean age of the participants was 61 years old and ranged from 26 to 80 years. Of all infections measured in the analysis, almost 45% were SSTI, followed by RTI (9%) and genitourinary infections (8%). According to the NOS, most of the studies included were of moderate quality (score 4–6) (80.9%).

Study selection process.
Study characteristics summary of observational studies evaluating the association between diabetes and infection
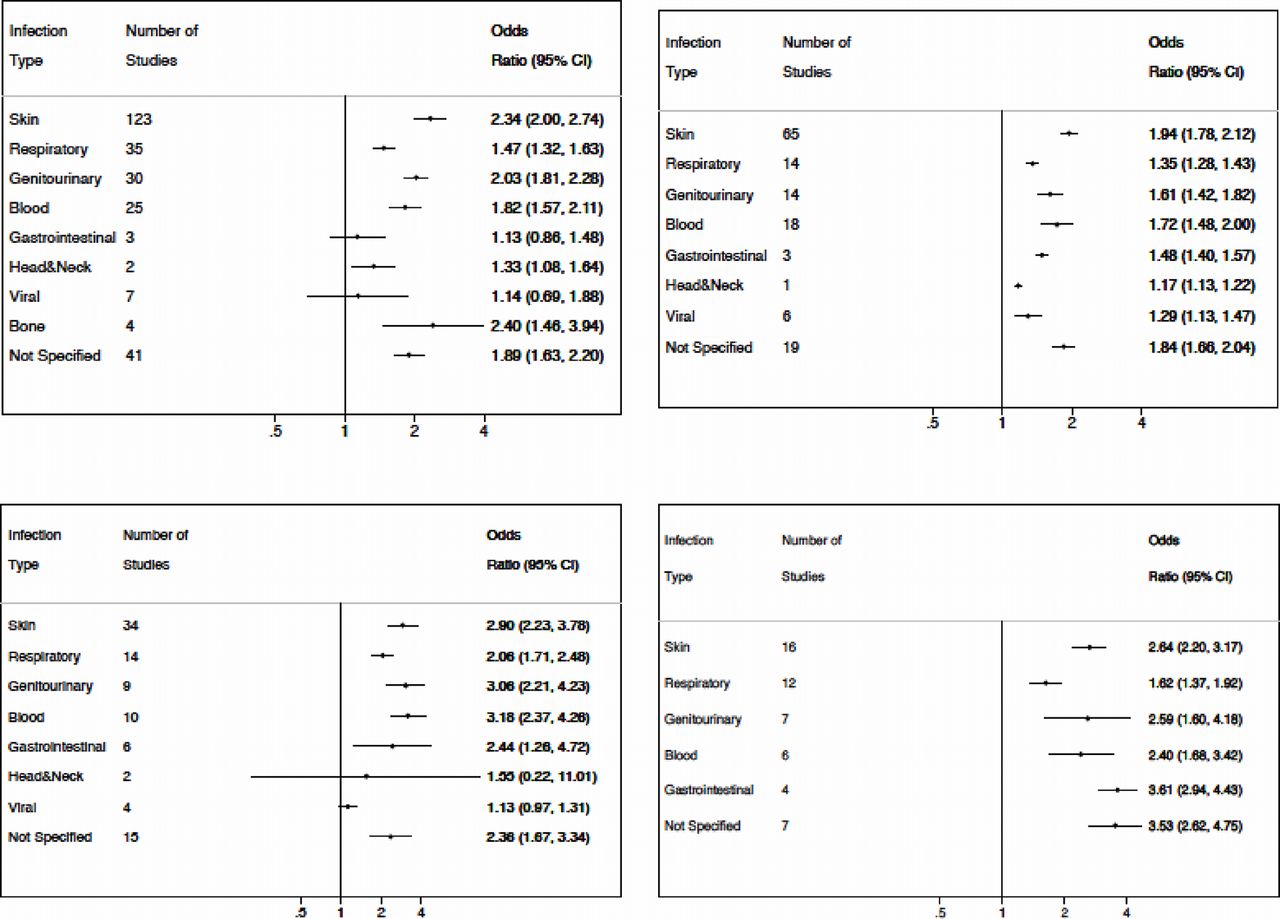
Figure 2A–D shows the number of studies, pooled ORs, and 95% CI for our main categories of infections. Individual characteristics of included studies are present in Appendix C. Forest plots for individual studies of crude and adjusted results are shown in Appendix D.
{kind=link}
{kind=link}
Pooled crude (A) and adjusted (B) OR for cohort studies and pooled crude (C) and adjusted (D) OR for case–control studies by infection type.
Skin and soft tissue infections
Our review found 176 studies (140 CS, 36 CCS) that evaluated the association between diabetes and SSTI (table 2; Appendix D1). The pooled crude OR for an SSTI from CS was 2.34 (95% CI 2.00 to 2.74; I2=98.8%), with a comparable pooled adjusted OR of 1.94 (95% CI 1.78 to 2.12; I2=92.5%). As for CCS, the crude OR was 2.90 (95% CI 2.23 to 3.78; I2=75.7%), and the adjusted OR was 2.64 (95% CI 2.20 to 3.17; I2=0%). To explore potential sources of heterogeneity between studies, we further categorized these infections to surgical site infections (SSI) and other SSTI. As shown in table 2, the results showed a positive association with diabetes, with decreased heterogeneity for both subgroups (SSI: crude OR 2.35, 95% CI 1.97 to 2.80, I2=98.9%, adjusted OR 2.03, 95% CI 1.84 to 2.25, I2=86.6%; other SSTI: crude OR 2.23, 95% CI 1.67 to 2.96, I2=91.8%, adjusted OR 1.83, 95% CI 1.74 to 1.93, I2=46.5%), and was less for the CCS (SSI: crude OR 3.13, 95% CI 2.37 to 4.15, I2=74%, adjusted OR 2.66, 95% CI 2.18 to 3.23, I2=0%; other SSTI: crude OR 1.69, 95% CI 1.05 to 2.72, I2=55.8%). SSI were further stratified according to type of surgery into nine categories.
Skin and soft tissue, respiratory and genitourinary infections
Respiratory tract infections
Meta-analyses of the 49 study results of RTI (CS=35, CCS=14) showed a positive association with diabetes (table 2; Appendix D2). For CS, the crude OR was 1.47 (95% CI 1.32 to 1.63) with considerable heterogeneity (I2=82.7%), and the adjusted OR was 1.35 (95% CI 1.28 to 1.43) with higher heterogeneity (I2=97.8%). Pooled results from CCS suggest a stronger association (crude OR 2.06 (95% CI 1.71 to 2.48; I2=95%); adjusted OR 1.62 (95% CI 1.37 to 1.92; I2=85.9%)).
Genitourinary tract infections
Thirty-three CS found a positive association between diabetes and genitourinary tract infections (crude OR 2.03 (95% CI 1.81 to 2.28, I2=92.4%); adjusted OR 1.61 (95% CI 1.42 to 1.82, I2=99.2%)) (table 2; Appendix D3). Similarly, pooled results from 11 control studies found genitourinary tract infections more commonly develop in people with diabetes compared with those without (crude OR 3.06 (95% CI 2.21 to 4.23, I2=81.2%); adjusted OR 2.59 (95% CI 1.60 to 4.17, I2=86.0%)).
Bloodstream infections
An association was apparent between diabetes and incident bloodstream infections (Appendices A and D4). Pooled results from 31 CS (crude OR 1.82 (95% CI 1.57 to 2.12, I2=88.4%); adjusted OR 1.72 (95% CI 1.48 to 2.00, I2=94.3%)) and 10 CCS (crude OR 3.18 (95% CI 2.37 to 4.26, I2=72.1%); adjusted OR 2.40 (95% CI 1.68 to 3.42, I2=71.7%)) showed a higher chance of developing bloodstream infections for patients with diabetes compared with without.
Viral infections
We identified 14 studies (CS=10, CCS=4) reporting associations between diabetes and viral infections (Appendices A and D5). Pooled effect estimates from CS (crude OR 1.14 (95% CI 0.69 to 1.87, I2=99.1%); adjusted OR 1.29 (95% CI 1.13 to 1.46, I2=97.6%)) and CCS (crude OR 1.32 (95% CI 1.14 to 1.54, I2=89.9%)) showed a positive association.
Head and neck infections
Five studies (CS=3, CCS=2) reported H&NI (Appendices A and D6). Pooled effects from CS (crude OR 1.33 (95% CI 1.08 to 1.65, I2=29.9%); adjusted OR 1.17 (95% CI 1.13 to 1.22, I2=45.4%)) and CCS (crude OR 1.55 (95% CI 0.22 to 11.10, I2=80.7%)) showed an association.
Gastrointestinal infections
There were four CS and six CCS that reported a gastrointestinal infection (Appendices A and D7). CS gave a (crude OR) of 1.13 (95% CI 0.86 to 1.47, I2=83.3%), with the (adjusted OR) of 1.48 (95% CI 1.40 to 1.57, I2=64.5%). However, CCS showed a stronger association with a (crude OR) of 2.44 (95% CI 1.26 to 4.71, I2=89.9%) and an (adjusted OR) of 3.61 (95% CI 2.94 to 4.43, I2=0%).
Bone infections
Seven studies (CS=5, CCS=2) reported bone infections (Appendix D8). Pooled results from CS showed a positive association between diabetes and bone infections (crude OR 2.40 (95% CI 1.46 to 3.94, I2=0%)). There were insufficient data to pool results from CCS.
Not specified infections
There were 67 studies (CS=52, CCS=15) that reported infections with no specification of type as the outcome (Appendices A and D9).
We further pooled the results from high score quality studies in both CS and CCS. The results were consistent across all types of infections (Appendix B).
Discussion
Although a possible association between diabetes and risk of developing different types of infections has long been speculated,13 20–22 our study provides the most extensive review to date examining the association between diabetes and incident infections. We identified 345 observational studies that reported on one or more types of infection. These studies were diverse in their source population, methods, and quality. Nonetheless, we found a positive association across all categories of infections, although the magnitude of association is variable, heterogeneity between studies is high, and the extent of evidence is vastly different for certain infections.
Our study supports the hypothesis that diabetes affects immunity leading to a higher chance of developing multiple types of infections. Indeed, our meta-analysis of adjusted results from both CS and CCS found statistically significant associations among all outcomes. These findings are supported by a large body of pathophysiological evidence across our outcomes of interest. In general, diabetes is known to affect healing,23 24 and hyperglycemia affects coagulation, fibrinolytic function,25 lipid metabolism and endothelial function.26 27 Moreover, hyperglycemia decreases function of neutrophils and monocytes by way of impaired chemotaxis, adherence, phagocytosis and other immune system impairment.5–7 In addition, people with diabetes are at higher risk of infections with certain microorganisms, mainly Streptococcus (Group A&B Streptococcus) and Staphylococcus.28 29
There are also specific factors that may predispose patients with diabetes to certain types of infections. For example, a predisposing factor for RTI may be present given patients with diabetes are often nasal carriers of Staphylococcus aureus and therefore may be at increased risk of associated pneumonia.30 31 Persons with diabetes are also susceptible to pulmonary infections because of an increased risk of aspiration secondary to gastroparesis, diminished cough reflex, and disordered sleep patterns.32 Impaired lung functions in these patients contribute to acquiring this type of infection as well.33 34 The pathophysiology of lung abnormalities in patients who have diabetes is believed to involve microangiopathic changes in the basement membrane of pulmonary blood vessels and respiratory epithelium, as well as non-enzymatic glycosylation of tissue protein.35–38
Similarly, several factors are thought to predispose diabetic subjects to urinary tract infections.20 21 39 40 Reduced sensitivity and altered distensibility of the urinary bladder due to autonomic neuropathy can result in stagnation of urine and higher rates of instrumentation.41 Moreover, glycosuria can enhance bacterial growth and impair phagocytosis. Genital infections might be linked to diabetes through certain potential mechanisms. It is well established that yeasts thrive in a sugar-rich environment, and therefore, it is logical to hypothesize that high glucose concentrations in patients with diabetes may be responsible for promoting the occurrence and recurrence of candidiasis. Candida albicans virulence is shown to flourish in a hyperglycemic environment.42–44
Poor glycemic control can increase the incidence and accelerate the progression of periodontal disease.45–47 The contributing factors involve higher salivary glucose, low salivary pH, microangiopathy, and abnormal collagen metabolism.20 21 45 47–49
The association between diabetes and viral infections is supported by various diabetes-specific in vitro defects in innate and adaptive immunity, and studies that showed that long-standing diabetes is often accompanied by impaired cell-mediated immunity, which increases the risk to more severe and widespread infections. This could also be the case for gastrointestinal infections and other types that were shown in the review.
Our review is not without limitations. First, a meta-analysis including observational studies is reliant on the validity of these studies; however, observational studies are methodologically challenging, difficult to interpret and susceptible to several types of bias and confounding. Furthermore, lack of uniformity of diagnosis for diabetes across studies may introduce bias. To mitigate these challenges, we used a validated scale to assess study quality wherein the majority of included studies were of moderate quality. Second, some of the included studies used self-reported assessments to identify diabetes. Self-reported measures of diabetes status have been previously shown to be over 99% specific and 66% sensitive compared with medical records.50 In addition, misclassification of patients with diabetes who did not know that they had the disease to the referent group of participants without diabetes is highly likely given that 46% of the estimated prevalence of diabetes is in people with undiagnosed disease.1 Third, some of the included studies were not specifically designed to quantify the association between diabetes and a particular infection or set of infections; however, the relevant data were reported to be included in our meta-analysis. In addition, although we understand the importance of presenting the relationship between the degree of glycemia and incidence of infection, hemoglobin A1C was seldom mentioned in most of the included studies. However, the degree of glucose control and antidiabetic medications use, if mentioned in the included studies, could be found under the definition of diabetes in the individual characteristics of included studies alongside other specific information as definition of infection with specific bacteriology if mentioned (Appendix C). Fourth, we recognize the limitation of having a single reviewer assessing the quality of each study. However, two independent reviewers verified data extraction. Moreover, although we do realize that most of the studies included in the review were of moderate quality, we further pooled the results of only high-quality studies to strengthen our conclusion. The results were consistent across all types of infections. Fifth, the heterogeneity in our main analyses was high. We explored heterogeneity across our results by grouping infections in several subtypes, and further grouping those into subcategories generally decreased the degree of heterogeneity. Sixth, many studies were conducted in specific clinical populations with various comorbidities present. It is possible that the association between diabetes and incident infections may be modified by the presence of certain comorbidities. Exploring effect modification was beyond the scope of this study. Lastly, we only included studies in English in our review. The reason for that is feasibility. However, our review managed to obtain a large number of studies, and others have reported that excluding non-English studies does not influence the results substantially.51 52
In conclusion, our extensive systematic review and meta-analysis showed that there is a positive association between diabetes and the development of several types of infection. The magnitude of the relationship varied according to type of infection. Our review identified gaps within the evidence for certain infections. More research is needed to explore the effect patient characteristics such as body mass index and glycemic control have on the risk of these types of infections.
Acknowledgments
JMG holds a New Investigator Award from the Canadian Institute of Health Research and a Clinician Scientist Award from the Canadian Diabetes Association.
References
Footnotes
Contributor WAA, LT, JV, and JMG were involved in the concept and design of the study. AR, JD, and PH were secondary reviewers who screened and verified data extraction. WAA was responsible for the data analysis and drafting the first version of the manuscript. All authors contributed to the interpretation of data and provided revisions to the manuscript. WAA will act as guarantor for the study.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Appendix C under supplementary information contains data for individual studies included in our review.