Article Text

Abstract
Objective The effects of regular exercise on the health promotion of patients with type 2 diabetes mellitus (T2DM) have been well documented. The present study investigated the long-term effects of regular exercise training on biological indicators among these patients.
Methods In this quasi-experimental trial with pretest-post-test design, 65 patients with T2DM aged 33–69 years (experiment (35), control (30)) participated. After 8 years of conducting the program, the data on 30 patients (experiment (15), control (15)) were entered into analysis. The training program included aerobic exercise three sessions per week, 90 min, 50%–80% VO2max. Before and after the intervention, the biological indicators (hemoglobin A1c (HbA1c), body mass index (BMI) and VO2max) were measured. Data were analyzed using multivariate analysis of covariance.
Results Our long-term exercise training program had a significant effect on HbA1C, BMI and Vo2max (P<0.05). Compared with patients in the control group, HbA1c was significantly reduced and BMI and VO2max were significantly improved among the experiment group.
Conclusions Long-term regular physical activity training was found to be helpful in improving glycemic control, body composition and cardiovascular fitness among patients with T2DM. Long-term continuous physical activity offsets the deteriorations of biological indicators found in the control group. Further research, with a particular focus on practical and real-world programming, is needed to determine the responsive health outcomes of such long-term programs on the patients.
- A1c
- Physical Exercise And Health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Obesity and insulin resistance, as the important components of metabolic syndrome are the results of reduced physical activity in daily life.
Increasing prevalence of obesity and sedentary lifestyle are considered important factors in the incidence of type 2 diabetes mellitus (T2DM) worldwide.
What are the new findings?
Long-term regular physical activity training had positive effects on glycemic control and body composition among patients with T2DM.
Long-term regular physical activity training promoted cardiovascular fitness among patients with T2DM.
Long-term continuous physical activity offsets the deteriorations of biological indicators found in the control group.
How might these results change the focus of research or clinical practice?
Regular physical activity training programs should be continued for >12 months among the patients with T2DM to investigate the long-term effects of the program on the biological indicators of the disease.
A particular focus on practical and real-world programming is needed to determine the responsive health outcomes of such long-term programs on the patients.
There is a need to investigate the effects of such long-term physical activity programs on controlling mental health outcomes (such as depression and anxiety symptoms) of the disease as well as quality of life among the patients with T2DM.
Introduction
Nowadays, there is an increasing rate in the incidence of lifestyle-related chronic physical and psychological problems, due to a decrease in the level of healthy behaviors like healthy nutrition and physical activity.1–3 A reduction in daily physical activity may result in obesity and insulin resistance, which are important components of metabolic syndrome.4 This syndrome predicts an increased risk of developing type 2 diabetes mellitus (T2DM) and cardiovascular diseases,5 as well.
According to WHO, the lack of physical activity may be considered as one of the 10 reasons for mortality and disability throughout the world. It is also well known that obesity and sedentary lifestyle are important factors in increasing the incidence of T2DM worldwide.6 7 Therefore, as body mass index (BMI) increases among populations, the higher risk for mortality may be expected.8
T2DM, with an increasing rate of prevalence in recent decades,9 has caused many health and socioeconomic problems throughout the world. Due to its various consequences and disabilities, T2DM has been known as a disabling disease, as well. Therefore, strategies for reducing the healthcare costs associated with the disease should be emphasized.10
Exercise, as one of above-mentioned strategies, has significant effects on the metabolism of nutrients. In particular, it diminishes the blood glucose levels, and plays an important role in the treatment of patients with diabetes.11 It has also been found that beside diet control and medical treatment, regular exercise may improve glycemic control, reduce cardiovascular risk factors, play a role in weight loss and, consequently, improve well-being among these patients. Regular exercise may also prevent the development of T2DM among high-risk individuals.12 Weight loss and the loss of visceral fat may be considered as the important benefits of exercise, which may lead to a significant improvement in the metabolic indices.13 Regular aerobic exercise may result in high insulin sensitivity, considerable weight loss and improved body composition. Weight loss by 10%–15% may lead to reduction in insulin resistance and may be most beneficial at the early stages of T2DM progression, when insulin secretion is still adequate.13
Evidence has shown that hemoglobin A1c (HbA1c), as the gold standard for monitoring glycemic control, may serve as an indicator for diabetes-related diseases.14 The epidemiological analyses have indicated that 1% reduction in the HbA1c value is associated with 14% reduction in myocardial infarction (MI) and 21% reduction in diabetes-related death and 37% reduction in microvascular complications.15 Furthermore, establishing glucose control at or below 7% can reduce the long-term complications of the disease up to 76%.16
Several previous studies have shown that regular exercise training can significantly reduce the values of HbA1c.17 According to a meta- analysis, chronic hyperglycemia is associated with an increased risk for cardiovascular disease among adults with diabetes adults.18 There is also evidence that among patients with T2DM, the maximal oxygen uptake (VO2max) values are lower compared with the healthy individuals.13 This phenomenon may be contributed to specific pathogenic mechanisms including hyperglycemia, low capacity density and alteration in oxygen delivery.13 Lemura et al, conducted a meta-analysis on the effects of training program on aerobic fitness in adults aged 46–90 years. The majority of the studies included in their meta-analysis showed significant improvements in aerobic fitness (VO2max). They concluded that despite the inevitable decline in Vo2max with aging, aerobic exercise training resulted in favorable adaptations in aerobic fitness among elderly people.19
As mentioned above, several previous clinical trials have indicated the effects of physical activity on the biological indicators of T2DM. The majority of these trials, however, have only engaged the patients in 6 weeks to 12 months of exercise training. In order to find better understandings of the long-term effects of regular physical activity training on the biological indicators of the disease, we conducted an 8-year trial among patients with T2DM in Tabriz, Iran. The aim of our study was to investigate the effectiveness of a long-term, regular exercise training program on the levels of BMI, glycosylated hemoglobin and VO2max among patients with T2DM.
Methods
Subjects
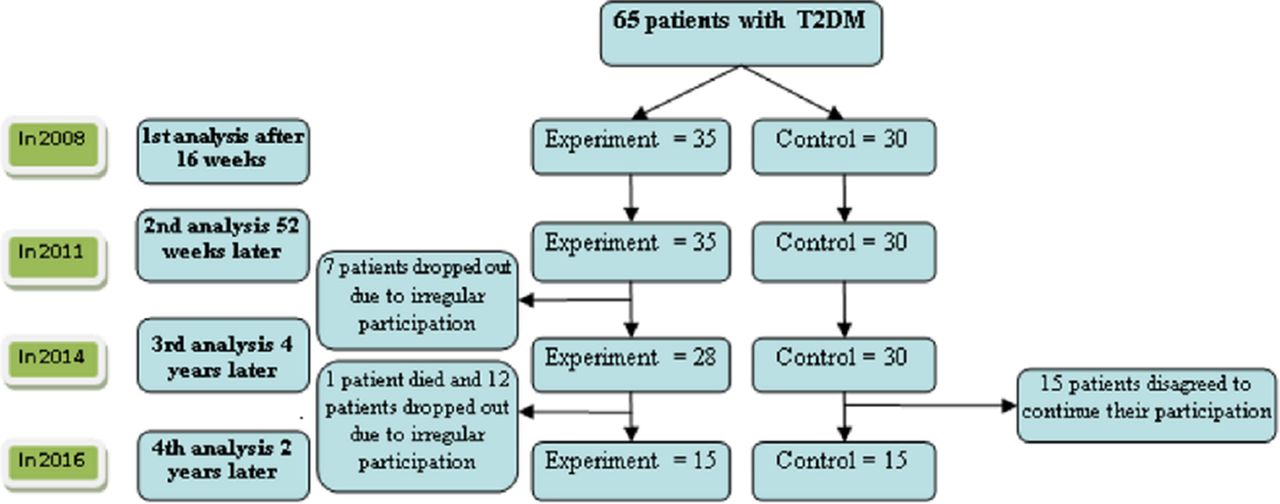
This was an experimental study with before-after design. The study population included patients with T2DM aged 33–69 years. In this 8-year clinical trial, 65 patients (35 were assigned to the experiment and 30 were assigned to the control group) from Endocrine and Metabolic Clinics, Tabriz University of Medical Sciences, Iran, agreed to be registered for participation in the study in October 2008. The results of conducting the first 16 weeks program were published in 2001.17 Then, after 52 weeks of conducting the exercise program on the subjects, the second series of the findings were published in 2001.12 Considering the interest of the research team as well as the consent and willingness of the subjects, we continued the study with the same program on the subjects for the next 4 years. In 2014, the data on 28 patients in the experiment group (who participated optimally in the program sessions) and 30 patients in the control group were analyzed and the findings were published.20 From 2014, the study was again continued through December 2016. During this period of time, one subject from the experiment group died due to car accident and 12 subjects dropped out due to irregular participation in the program. Fifteen out of 30 subjects in the control group disagreed to continue participation in the study. Therefore, analysis for the present paper was conducted on 30 subjects (15 in the experiment and 15 in the control group). The diagram of study design and the participants’ dropout are illustrated in figure 1.

Study design and the participants’ dropout. T2DM, type 2 diabetes mellitus.
Inclusion criteria for the samples were as follows: diagnosed with T2DM for more than 1 year, treated with oral hypoglycemic agents only (not taking insulin), having a previous sedentary lifestyle and HbA1c level <11%. Exclusion criteria were BMI >43 and 70 years of age and older, having severe retinopathy, nephropathy and neuropathy and the history of serious cerebrovascular or cardiovascular diseases, as well as severe musculoskeletal problems restricting physical activity.
Parameters
All the subjects in both groups were recommended to continue their previous routine medications and diets. Furthermore, the subjects in the control group were instructed to maintain their present lifestyle until the end of the project. Before and after the intervention, the levels of HbA1c and VO2max (mL/kg/min) were measured applying the HbA1c analyzer (Hitachi, model 704,902, Japan) and the Rockport 1600 m Walking Test, respectively. Estimation of VO2max from a timed one-mile track walk with duration, incorporating gender, age, body weight in pounds and heart rate at the end of the mile.21 The heart rate (monitored with PolarFT60, china) and BMI (kg/cm) of the patients were also measured before and after the experiment. A body composition monitor (model BF500, OMRON, 2007) was used to determine the basal metabolic rate (%BMR), body fat percentage (%BF), BMI (kg/m2) and muscular percentage (%).
Exercise programs
A 2-week run-in phase was performed three sessions per week (with duration of 15–40 min), based on the guideline of American College of Sports Medicine (ACSM).22 The activities of the sessions included warm-up movements, and doing aerobic exercise at a moderate intensity. At the first session, a time was considered for the patients to be familiarized with the exercise machines. The exercise program that was gradually progressed in duration (from 50% to 80% of maximum heart rate), included 10–15 min stretching movements to warm-up, followed by 40–50 min of aerobic training (treadmill, elliptical or bicycle ergometers), and finally 10–15 min of relaxation activities to cool down. The target heart rate was progressed from 50% to 80% of the maximum heart rate during the baseline treadmill testing. The implementing process of the exercise program was supervised by an exercise training expert with field experience in physical activity of patients with diabetes. This expert (as a supervisor) participated randomly in about half of the training sessions. After the end of each session, he consulted the trainer about the process of training.
Statistical analysis
In this study, descriptive statistics was used for obtaining central and variation measures. Moreover, Kolmogorov-Smirnov test was applied to determine the normality of data. Paired t-test was also used to compare the variables in each group before and after intervention. All statistical analyses were performed using SPSS software V.21 (SPSS, Chicago, Illinois, USA). The distribution of data was normal and P<0.05 was considered as statistically significant, a priori.
Results
The mean age of the subjects was 57.2±8.3 (33–69 years). The mean ages for the experiment and control groups were 57.6±8.7 and 57.9±8.2, respectively. Table 1 demonstrates the descriptive statistics of HbA1c, body composition and VO2max of the experiment and control groups before and after the intervention. According to this table, statistically significant differences were found in the three variables between subjects in the experiment and control groups.
Descriptive statistics
Regarding the study question on the effect of physical exercise program on biological variables (BMI, HbA1c, VO2max), multivariate analysis of covariance was used. Results of multivariate analysis of covariance showed that the training program had a significant effect on the dependent variables in a combined manner (F=33.45, P<0.05). Table 2 (univariate analysis of covariance) indicates the effects of the program on each of the dependent variables (BMI (F=17.15, P<0.05), HbA1c (F=11.08, P<0.05), VO2max (F=102.14, P<0.05)).
Tests of between-subjects effects
According to the results presented in table 3, the levels of BMI and HbA1c in the experimental group were lower than those in the control group. Also the level of VO2max in the experimental group was higher than that of the control group.
Pairwise comparisons
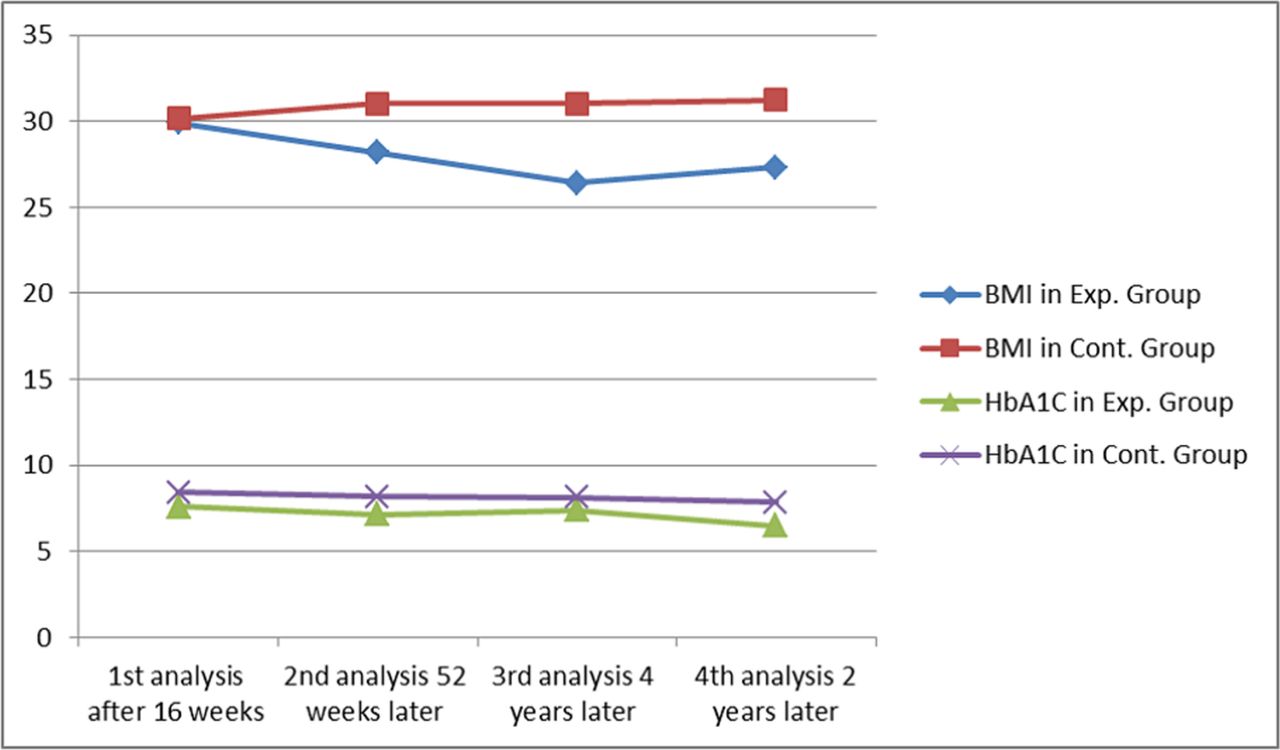
Changes in BMI and HbA1c during the 8 years of conducting the program on the patients with T2DM are shown in table 4. Moreover, timeline changes in the level of these two variables during the program are illustrated in figure 2.

{kind=link}
{kind=link}
Timeline changes in BMI and HbA1c of the patients with T2DM during the 8 years of study. BMI, body mass index; Exp., experiment group; Cont., control group; HbA1c, hemoglobin A1c.
Changes in BMI and HbA1c during the 8 years of study among patients with T2DM
Discussion
Our aim in the present study was to investigate the effectiveness of a long-term regular exercise training program on the levels of BMI, glycosylated hemoglobin and VO2max among patients with T2DM. We eventually found that such long-term exercise training program may improve the level of VO2max and reduce the levels of BMI and HbA1c among these patients. It is well known that regular exercise training to the patients with T2DM has positive effects on their level of glycemic control as well as the disease complications such as cardiovascular problems.12 In addition, the indirect effects of exercise on weight loss and the improvement of function in the beta-cells and insulin sensitivity have all been known.23
In the present study, after 8 years of regular exercise training, the experimental group revealed significant improvement in BMI. As shown in the results, there was a linear decrease in BMI during the first 6 years and an increase in the remaining 2 years of follow-up. In contrast, among the patients in the control group a slightly constant increasing pattern was observed in the level of BMI during the 8 years of follow-up. These findings are consistent with those reported by Balucci et al24 and Cuff et al.25 In the study conducted by Goldhaber-Fiebert et al,26 significant weight loss was observed in the experimental group. The training program in their study included exercise and diet, which might be a reason for the significant positive effects. A possibility for the increase found in the level of BMI at the eighth year of our study may be the confounding effect of the age of participants. Stevens et al,27 in a bi-ethnic cohort, found aging in association with an increase in BMI in white and African-American men and women. Considering that our study was a longtime intervention and as the patients were getting older and older during time, the level of their BMI may be affected by their age. In other studies conducted by Ahmadizad et al28 and Tokmakidis et al,29 no significant improvement was found in BMI after conducting 12 weeks aerobic and resistance training and 16 weeks combined exercise training programs, respectively. Furthermore, in a systematic study applying different types of exercise, Boulé et al did not find any significant change in BMI of the experiment group.30 In contrast, Krousel-Wood et al31 reported that home-based exercise improves BMI among patients with T2DM. A review on these studies shows that the majority have conducted the training program for <6 months, which may be a reason for the controversial findings. Our study, as a long-term trial may be considered as an affirmation for the effects of regular exercise training on the BMI of the patients with T2DM.
In the present study, significant decrease (1.39%) was found in the level of HbA1c among the experiment group after the last 2 years of intervention. Also, a constant decreasing pattern in the level of this variable was observed in the experiment group during the 8 years of follow-up, except for the value found in the sixth year. In the control group, the 8-year timeline change for HbA1c was also found to follow a slightly decreasing pattern. Despite the decreasing pattern of HbA1c in the control group, the values of this index were higher than those found in the experiment group during the 8 years of our program. In a meta-analysis on 12 aerobic training and 2 resistance training studies during 1989–2000, Boulé et al30 revealed that exercise may reduce HbA1c values by approximately 0.66%, which is an appropriate reduction to improve the glycemic control. Yan et al32 also reported that after a 12-week aerobic program, HbA1c level was reduced by 1.1% and VO2max was increased, as well. They, however, reported no significant change in BMI after the program. In another study, Rönnemaa et al33 reported that 4 months of exercise program has reduced HbA1c level from 9.6% to 8.6%. Sigal et al.,15 Shenoy et al.,16 Kelley and Kelley18 and Church et al34 also reported significant reductions in glycosylated hemoglobin. In our present study, the level of HbA1c among the patients was decreased by 0.73% and 1.33% after 16 weeks postintervention and 1-year follow-up, respectively. Also, in the third (6 years after initiation of intervention) and the fourth (8 years after initiation of intervention) analyses of our data, the levels of HbA1c decreased by 1.11% and 1.84%, respectively. As shown in figure 1 that, in contrast to control group, the level of HbA1c in the experiment group has decreased in a relatively constant pattern. It may be, therefore, concluded that having a stable level of physical activity during a long time may increasingly improve the level of HbA1c among the patients with T2DM. All these findings along with those reported in the present study affirm the direct relationship between long-term regular physical activity with the level of HbA1c and cardiovascular fitness, especially VO2max values and BMI.
Also, our results demonstrated that long-term regular aerobic training program may result in increasing the level of VO2max among patients with T2DM. Similarly, Boulé et al30 reported >10% improvement in VO2max values as a result of a rather low intense aerobic exercise program. Cauza et al35 and Alam et al36 also found significant increases in VO2max after aerobic and 6-month controlled exercise trainings, respectively. Inconsistent with those found in our study, Byrkjeland et al37 did not find a significant change in values of HbA1c and VO2max after a 52-week aerobic training program among patients with T2DM. They, however, found considerable increase in ventilation pulmonary threshold and time of fatigue in the training group compared with the control group. Differences in the variations of VO2max by increasing age may be described by the effective factors of aerobic fitness readiness. The difference in body composition changes during growth and the changes in daily physical activity could be attributed to these disorders.33 However, there is evidence that among patients with T2DM, VO2max value is lower than that among healthy individuals, which may be associated with specific pathological mechanisms such as hyperglycemia, low capacity density and alteration in oxygen delivery.15
Getting the patients with T2DM to engage in such a long period, regular physical activity program provided the researchers with an interesting experience of working with the patients. After 8 years of study, the relationships between the research team members and the patients have become so strong that the remaining subjects in the intervention group do not intend to terminate the program. They still come to the club (the place of conducting the program) three times per week and continue to their exercise along with some members of the research team. Also, 5 years after the initiation of study, a majority of the patients remained in the program (90%) was literate patients. This highlights the role of literacy in maintaining and promoting health among such populations.
Conclusion
Long-term regular physical activity training was found to be helpful in improving glycemic control, body composition and cardiovascular fitness among patients with T2DM. Long-term continuous physical activity offsets the deteriorations of biological indicators found in the control group. Further research, with a particular focus on practical and real-world programming, is needed to determine the responsive health outcomes of such long-term programs on the patients. It is also suggested to investigate the effects of such long-term physical activity programs on physiological adjustments, controlling mental outcomes (such as depression and anxiety symptoms) of the disease as well as quality of life among the patients with T2DM.
References
Footnotes
Contributors FN, MM, AY and AA researched the data; AY, NMA and MN contributed to discussion and wrote the manuscript; JHG, VS and HN reviewed/edited the manuscript and helped in researching the data.
Funding This work was supported by Tabriz University of Medical Sciences grant number 93-43-2211.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ehtics Committee in Tabriz University of Medical Sciences.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data are available at the website of BMJ Open Diabetes Research & Care.