Article Text

Abstract
Objectives To determine if a diabetes prevention program (DPP) delivered by a commercial weight management provider using a UK primary care referral pathway could reduce the progression to type 2 diabetes (T2D) in those diagnosed with non-diabetic hyperglycemia (NDH—being at high risk of developing T2D).
Research design This is a quasi-experimental translational research study.
Methods 14 primary care practices identified, recruited and referred patients with NDH (fasting plasma glucose ≥5.5 to ≤6.9 mmol/L and/or glycated hemoglobin (HbA1c) ≥42 to 47 mmol/mol (6.0%–6.4%)) and a body mass index (BMI) ≥30 kg/m2 to a DPP. Eligible patients were asked to contact Weight Watchers to book onto their DPP, an intensive lifestyle intervention which included a 90 min activation session followed by the offer of 48 weekly Weight Watchers community group meetings. Patients’ blood tests were repeated by primary care, weight change plus self-reported data was recorded by Weight Watchers.
Results 166 patients were referred to the program and 149 were eligible. 79% of eligible patients attended an activation session (117 eligible patients) and 77% started the weekly sessions. The study sample was primarily female (75%), white (90%), with 5% living in the most deprived quintile in the UK. Using intention-to-treat analysis, the DPP resulted in a mean reduction in HbA1c of 2.84 mmol/mol at 12 months (from 43.42±1.28 to 40.58±3.41, p<0.01). 38% of patients returned to normoglycemia and 3% developed T2D at 12 months. There was a mean weight reduction in BMI of 3.2 kg/m2 at 12 months (35.5 kg/m2±5.4 to 32.3 kg/m2±5.2, p<0.01).
Conclusion A UK primary care referral route partnered with this commercial weight management provider can deliver an effective DPP. The lifestyle changes and weight loss achieved in the intervention translated into considerable reductions in diabetes risk, with an immediate and significant public health impact.
- diabetes prevention programme
- non-diabetic hyperglycaemia
- type 2 diabetes
- intensive lifestyle intervention
- weight and blood glucose
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- diabetes prevention programme
- non-diabetic hyperglycaemia
- type 2 diabetes
- intensive lifestyle intervention
- weight and blood glucose
Significance of this study
What is already known on this subject?
Type 2 diabetes is a major cause of morbidity and mortality. The risk of developing type 2 diabetes is strongly influenced by lifestyle factors; there is a significant reduction in the risk of developing T2D achieved via weight loss.
What are the new findings?
The evidence for reducing type 2 diabetes risk is well established; there is a need to investigate how to implement these prevention programs in the real world utilizing existing referral pathways. This study found that patients referred by primary care in the UK to a diabetes prevention program delivered by a commercial weight management provider achieved a significant reduction in diabetes risk.
How might these results change the focus of research or clinical practice?
This study informs clinicians that a UK primary care referral route was successful in referring patients to a diabetes prevention program and that partnering with a commercial weight management diabetes prevention program translated into considerable reductions in diabetes risk.
Introduction
Type 2 diabetes (T2D) is a significant public health challenge.1 The risk of developing T2D is strongly influenced by lifestyle factors, the risk of developing T2D is significantly reduced via weight loss, specifically a 7% reduction in starting weight achieved via a lower energy diet2 and an increase in physical activity (PA).3 Early diagnosis of T2D is important because poor management of glycemic control is linked to poor health outcomes such as irreversible microvascular damage to vision (retinopathy) and circulation (neuropathy).4 It is estimated that the risks of macrovascular disease such as cardiovascular disease (CVD) and stroke are more than five times greater in diabetic individuals than non-diabetic individuals and life expectancy is on average 10 years shorter.5
A new diagnosis of T2D is made every 2 min in the UK.6 Both incidence and prevalence in the UK are rising. Since 1996, the number of people diagnosed with diabetes has increased from 1.4 to 2.9 million.6 By 2025, it is estimated that five million people will have diabetes, around one in seven adults.6 The increase in prevalence of those at risk of developing T2D is closely linked to the increasing prevalence of obesity, with 80% of people with T2D classified as overweight or obese.7 A 1 kg/m2 increase in body mass index (BMI) increases the risk of developing T2D by 8.4%.8 Prevalence modeling undertaken in 2015 estimated that there are currently a further five million people (11.4% of the 16+ population in England) meeting the criteria for non-diabetic hyperglycemia (NDH) in the UK (NDH is defined as a fasting plasma glucose (FPG) ≥5.5 to ≤6.9 mmol/L and/or HbA1c between ≥42 and 47 mmol/mol (6.0%–6.4%)) which means they are at high risk of developing T2D.9
A recent systematic review by Public Health England (PHE)10 demonstrated that modest weight loss,11 improvements in diet quality,12 and increases in PA levels3 can reduce incidence of T2D by more than 50% for individuals with NDH.2 Until recently, most DPPs have focused on establishing the efficacy of lifestyle interventions on risk reduction in randomized controlled trial (RCT) settings. With the evidence now well established there is a need to investigate how to implement these findings in wider healthcare settings to reach the significant numbers at risk in the general population. Interventions for weight loss have demonstrated that commercial weight management providers are more effective and efficient at achieving weight loss than interventions delivered by primary care alone.13 The UK’s National Institute for Health and Care Excellence (NICE) recommends that for maximal weight loss, certain commercial weight management providers have been proven effective in the long term, one of which includes Weight Watchers (WW).14 Evidenced by RCTs, they meet the requirements for intensive lifestyle interventions for weight management and have achieved significant weight loss outcomes.13 In the USA, a recent trial used an augmented commercial weight management program (WW) in the intervention arm of an RCT for a community-based DPP.15 Intervention participants (n=112) lost significantly more weight than controls (n=113) at 12 months; −5.51 kg (±0.63) versus −0.22 kg (±0.69) (p<0.001), with greater improvements in HbA1c −0.25% (±0.03) versus controls −0.18% (±0.03) (p<0.068) and an increase in high-density lipoprotein (HDL) cholesterol level +6.29 mg/dL (±1.05) versus controls +2.99 mg/dL (±1.14) (p<0.36). This suggests that commercial weight management programs could significantly increase the availability of DPPs making an immediate and significant public health impact. However, the effectiveness of such interventions using UK clinical primary care settings has not been fully evaluated.
This study aims to evaluate the effectiveness of a Local Authority commissioned DPP delivered by this commercial weight management provider for patients with NDH being identified and referred by primary care in the UK to reduce the risk of developing T2D. This paper presents findings at 12 months only; patients are being followed up for 24 months.
Methods
Study design
This is a quasi-experimental translational research study. This study is reported in accordance with the Standards for QUality Improvement Reporting Excellence guidelines.16 The study was performed in accordance with the Declaration of Helsinki Protocols and received ethics approval (the University of Westminster, ethics number: VRE1516-0978). Patients gave informed consent before taking part. The efficacy of lifestyle modification treatments have been well established by earlier diabetes prevention trials.2 Therefore, taking account of ethical considerations, all patients identified by primary care were offered the program. Consequently, the study did not have a control group.
Patient involvement
A qualitative study arm was conducted alongside this evaluation to obtain feedback on patient expectations, experiences and preferences. As qualitative data were gathered from completers and dropouts, it was anonymized and fed back to the implementation team. In addition, Bromley Public Health held two patient participation events during the evaluation to enable current and completed patients to reflect on progress and areas for improvement. This patient engagement will shape the future delivery of the Weight Watchers Diabetes Prevention Program (WWDPP). The results of both the qualitative and quantitative research will be disseminated to study participants.
Eligibility criteria
Eligibility: inclusion criteria were as follows:
Registered with a Bromley general practitioner (GP).
Diagnosed with NDH. NDH was defined as a fasting plasma glucose ≥5.5 to ≤6.9 mmol/L and/or HbA1c between ≥42 and 47 mmol/mol (6.0%–6.4%).
BMI ≥30 kg/m2.
Or a BMI≥27.5 kg/m2 for those with a comorbidity (such as hypertension, hyperlipidemia (uncorrected by maximum tolerated doses of statins) and/or severe osteoarthritis (eg, requiring listing for joint replacement or in severe pain uncontrollable with analgesics),
Or a BMI≥27.5 kg/m2 for those from an ethnic minority origin such as African, Asian or Caribbean origin.
Eligibility: exclusion criteria were as follows:
Previously diagnosed with T2D (patients referred to the diabetes pathway).
Currently attending or wanting to be referred to the Stop Smoking Service.
If pregnant.
Aged 17 years old or under.
Unwilling or unable to give informed consent.
Unwilling to attend group-based interventions.
Routine clinical judgment was used by primary care to assess whether a patient should be excluded if,
Patient was being examined for having an eating disorder or was undergoing treatment for having an eating disorder according to NICE guidance.17
Primary care and the patient agreed they would benefit from more intensive one to one personal supervision either with a dietitian or clinical management or from bariatric surgery rather than the group-based WWDPP intervention.
If the patient declined the offer of the intervention it was deemed the patient not motivated to change lifestyle behaviors at the time of recruitment and excluded.
Sample size
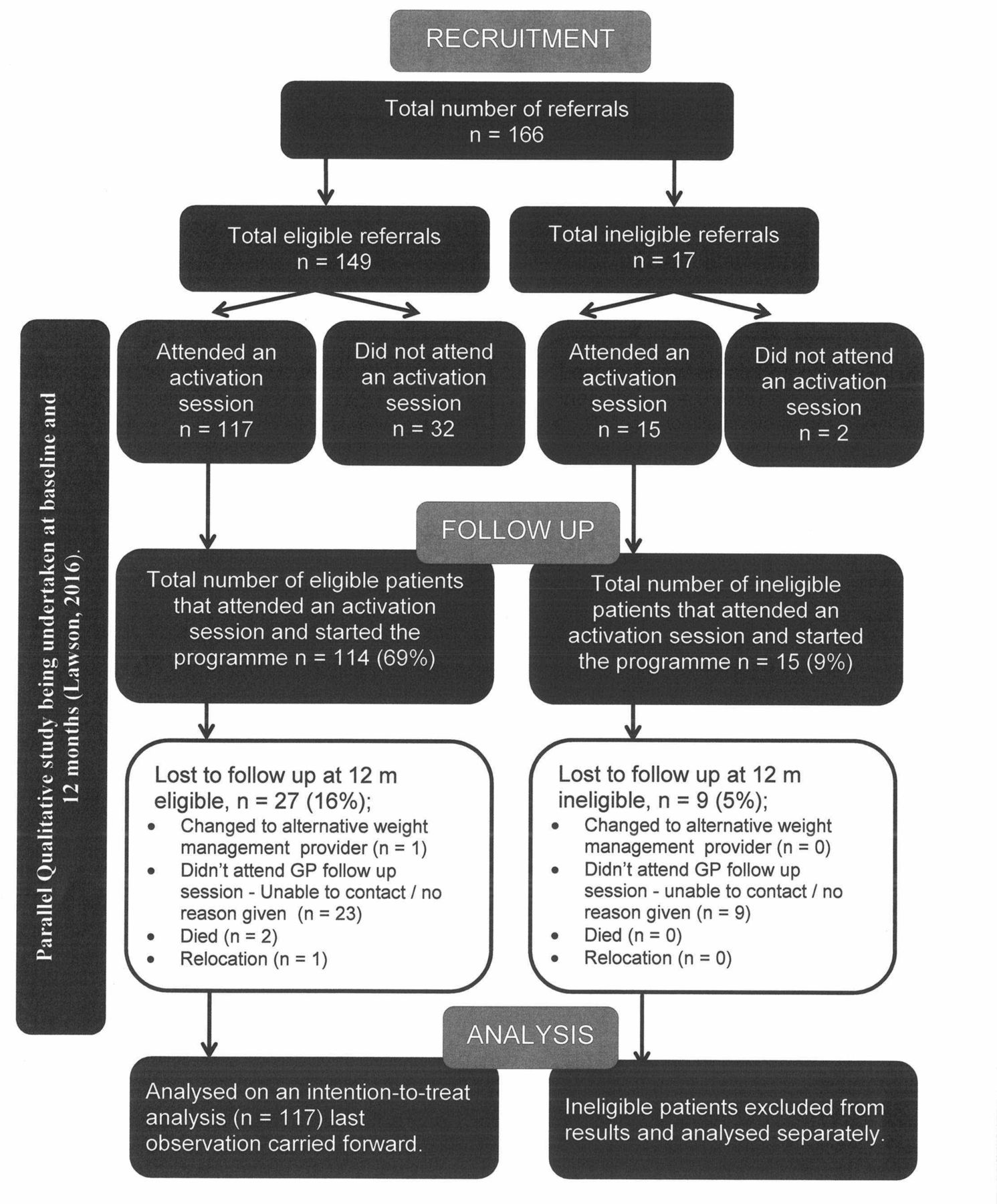
Sample size was calculated with G*Power. Using a power of 0.90, significance level of 0.05 and a moderate effect size of 0.3, 109 patients were needed to treat. One hundred and seventeen patients received the intervention and were analyzed via intention-to-treat (ITT) analysis. Based on the previous literature, the estimated dropout rate was between 10% and 30%; in order to treat 109 patients, a minimum of 120–142 patients needed to be referred to the program, but the actual number of patients referred was 166 patients.18. The referral pathway flow diagram illustrates the referral pathway, recruitment and adherence of patients (figure 1).

Referral pathway flow diagram. Referral, take up and adherence to the Weight Watchers Diabetes Prevention Program (WWDPP).
Primary care recruitment and referral process
Twenty-five GP practices were invited to take part in this WWDPP (out of 45 practices in Bromley); they were invited to an information evening where they could find out more about the WWDPP and how to take part and refer patients. Of these 25 practices invited, 14 practices (56%) went onto identify, recruit and refer patients with NDH to the WWDPP. Patients were recruited opportunistically on diagnosis of NDH, via a practice register search to identify NDH patients (GP operating system used was EMIS Web) or via an NHS Health Check19 where a diabetes risk assessment is undertaken. In an NHS Health Check patients who met the diabetes filter (ie, had a blood pressure ≥140 systolic and/or ≥90 diastolic and/or a BMI ≥30 kg/m2 (BMI ≥27.5 kg/m2 for those from an ethnic minority origin such as African, Asian or Caribbean origin)) were sent for a HbA1c or FPG blood test. Primary care staff assessed patients against the eligibility criteria, then explained the program, gained informed consent and took baseline measurements. Patients were given a referral form with WWDPP information included and asked to contact the WW call center. When the patient phoned the call center, they were given further information about the intervention and, if still interested, booked into an activation session. The patient had access to the program at the point of referral; therefore, an ineligible patient could attend if primary care referred a patient that does not fit the inclusion criteria if referred within their consultation. A lifestyle intervention has multiple health benefits for any patient, so ineligible patients were allowed to continue so that the GP—patient relationship was not negatively affected. The average number of days the patient took to attend WWDPP session after they attended the activation session was 11 days (ranged from 1 to 98 days). Figure 2 illustrates the WWDPP design.

Weight Watchers diabetes prevention program design.
Description of the intervention
The intervention comprised a structured 90 min activation session on diabetes prevention plus the standard evidence-based WW program for 48 weeks. The aims of the activation session were to set two goals.
First, to lose and maintain a weight loss of at least 7% of starting weight at 12 months by following the WW plan focused on improving diet quality and reducing portion size.15 WW leaders advised each patient how many kilograms they needed to lose to achieve a 7% weight loss.
Second, to work towards achieving 150 min of moderate intensity PA per week.20
In addition these activation sessions served to
Motivate a commitment to change and increase individuals’ confidence in ability to change.
Provide an opportunity for patients to meet others in a similar situation, thereby encouraging peer support, addressing possible stigma and reducing isolation.
Teach the patients how to measure their waist circumference (WC) and record their PA minutes undertaken.
The activation session was an interactive psychoeducation group that gave an introduction to diabetes prevention. The sessions were facilitated by upskilled WW staff (who are trained lay people employed by WW to deliver community-based support to all members). Local leaders were selected as high performers in delivering WW curriculum content, who achieved good WW member retention and successful weight loss. Those leaders received specific 1-day training from a registered dietitian to gain an understanding of T2D and NDH and how to deliver the activation session curriculum (this was in addition to the initial and ongoing learning and development that WW Leaders receive to deliver the WW program and facilitate supportive group meetings). A manual for the training and the activation session curriculum with associated patient facing materials were developed. In the activation session, patients learned about T2D, the meaning of NDH, how the condition increases risk of developing T2D and what patients can do to reduce their risk. The session focused on raising awareness of the benefits and types of lifestyle changes needed to achieve and maintain a healthy weight. It was built on patients’ existing knowledge and reinforced the patients’ confidence that they could make the changes required. Role modeling was provided by the WW Leaders and other group members, providing ongoing peer support. At the activation session, patients were signposted to their geographically most convenient WW meeting or a WW meeting of their choice. Patients could choose to attend any WW group session and were free to switch both time and location as best fitted their schedules. Patients were given vouchers that enabled them to attend for 48 weeks for free.
On attending the WW meetings, the WW plan was explained to the patient; program materials were provided and patients were given access to a WW online App. The WW plan is based on a Weight Loss System, which is a point system that creates an energy deficit for a healthy rate of weight loss personalized for every patient (based on gender, height, current weight and age). Dietary modifications seek to increase consumption of wholegrains, vegetables and other foods that are high in dietary fiber, reduce the total amount of fat in the diet by eating less saturated fat and reduce the amount of refined carbohydrates consumed. Promotion of regular, enjoyable and convenient PA is encouraged. Their DPP goals of 7% weight loss and increasing activity were encouraged throughout.
The standard weekly WW sessions already have a core curriculum that uses an evidence-based lifestyle modification program appropriate for diabetes prevention.15 This includes tailored advice, support and encouragement to help patients be more physically active, eat a healthier diet, lose weight and maintain a healthier weight. The behavioral change strategies employed within the program include, but are not limited to, self-monitoring strategies (utilizing digital-based and/or paper-based tools to track weight, food intake and activity), stimulus control (use of impulse control techniques to improve management of food cravings), development of weekly personal coping plans (for relapse prevention), problem solving, goal setting and strategies to garner social support. Table 1 illustrates the WWDPP core curriculum topics addressed and behavior change strategies employed.
Weight Watchers Diabetes Prevention Program (WWDPP) core curriculum topics addressed and behavior change strategies employed
The fidelity of the intervention was maintained via quality assurance protocols already embedded within the WW organization, including visiting sessions with standardized assessments, completing spot checks that leaders are adhering to the curriculum, regularly tracking and reviewing patient outcomes, completing leader management and training needs analysis and reviewing the qualitative research. All WW services were commissioned by the Local Authority and provided free of charge to patients for the duration of the study (figure 2).
Data collection
Physiological baseline measures were taken by NHS employed GPs, nurses or healthcare assistants, who followed NHS standards and used authorized NHS equipment (table 2). Standard NHS operating procedures and guidelines were followed to analyze and determine blood glucose via a fasting HbA1c or FPG blood glucose test, including diagnosing NDH, T2D and cholesterol. Validated sphygmomanometers are used in primary care to measure blood pressure (BP). The GP referral form (GP operating system EMIS Web) was used to refer patients and return blood results at 6 and 12 months. Weight measurements were taken by trained WW Leaders each week they attended using calibrated scales (Marsden M-560 Portable Scale) as an indicative proxy measure of whether they had adhered to the healthy lifestyle plan that week and an opportunity for the leader to give feedback to the patient. WW leaders trained patients at the activation session on how to self-measure WC via the WHO STEPwise approach to Surveillance protocol.21 Patients were taught how to self-report PA minutes (patients given definition of PA for health benefits; Chief Medical Officer Guidelines: Complete at least 150 min of moderate intensity PA per week to achieve health benefits).20 Self-reported data were collected by WW coordinator every 12 weeks via telephone or email. Patients received additional support and motivation via telephone calls, anyone who stopped attending was encouraged to re-engage with the program. These phone calls were not scripted; they were an opportunity to listen to the patient and provide personalized advice and support to stay engaged. Adherence was measured by attendance at the intervention.
Diabetes prevention program quantitative evaluation measurements
Outcome measures
The primary outcome measures were mean change in HbA1c and FPG, mean weight loss (kg), mean BMI change and percentage body weight change at 6 and 12 months from baseline.
Secondary outcome measures were number of sessions attended, incident rates of T2D, mean change in cholesterol, cholesterol/HDL ratio, HDL, LDL, triglycerides, blood pressure (BP), WC and PA minutes completed at 6 and 12 months from baseline.
Statistical analysis
All baseline continuous variables were summarized by mean and SD, categorical variables with frequency counts and percentages. Analysis was performed to compare the risk of developing diabetes before and after the intervention for patients who matched the eligibility criteria and attended an activation session. Analysis of treatment effects measured the direction and magnitude of the WWDPP on all outcome variables. A linear mixed effect (LME) model (covariance type; autoregressive (1): heterogeneous) was performed to test the effect of the intervention on HbA1c variation at 6 and 12 months on an ITT basis, considering the appropriate correlation structure and time interaction. LME has the advantage of allowing adjustment for confounding and of dealing with missing values, whereby subjects on which observations are missing can still be included in the analysis. Missing weight data equated to 15% at 6 months (18 patients) and 27% at 12 months (32 patients).
Bivariate correlation analysis was carried out in order to examine the relationship of the independent variables on the main dependent variable, HbA1c at 12 months. All independent variables were continuous variables except ethnicity, gender and social deprivation which were included as categorical variables. All models were adjusted for baseline BMI and weight lost at 12 months (kg); ethnicity and age were forced into the analysis as suggested by previous literature.10
A p value of <0.05 (two-sided) was considered statistically significant. For patients who prematurely discontinued their follow-up visits before 12 months the last observation carried forward was used. IBM SPSS Statistical software V.23 was used for data analysis.
Results
There were 166 referrals, of which 149 met the eligibility criteria. Of these, the 117 who attended an activation session form the study cohort. Table 3 shows that the study sample was primarily female (75%), white (90%), with 5% living in the most deprived quintile in the UK.22 Patients were aged on average 58 (SD ±9) years, which ranged from 36 to 80 years old. Baseline HbA1c was 43.42 mmol/mol (SD=1.28), baseline FPG was 6.12 mmol/L (SD=0.37), baseline weight 96.3 kg (SD=16.9) and BMI of 35.5 kg/m2 (SD=5.4).
Patient cohort demographic characteristics
Clinical, anthropometric and PA measures at baseline, 6 and 12 months are shown in table 4. There was a significant reduction in HbA1c between baseline and 6 and 12 months (p<0.01), using ITT analysis. There was a mean reduction in HbA1c of 2.84 mmol/mol at 12 months (from 43.42±1.28 to 40.58±3.41). There was a significant reduction in FPG at 6 months but this failed to reach significance at 12 months. Of the 117 patients with NDH at baseline, 44 (38%) had returned to normoglycemia, 18 (15%) had reduced their risk of T2D by reducing their blood glucose and 4 (3%) patients developed T2D by 12 months (figure 3). Two patients died before the end of the study of unrelated causes (cancer).
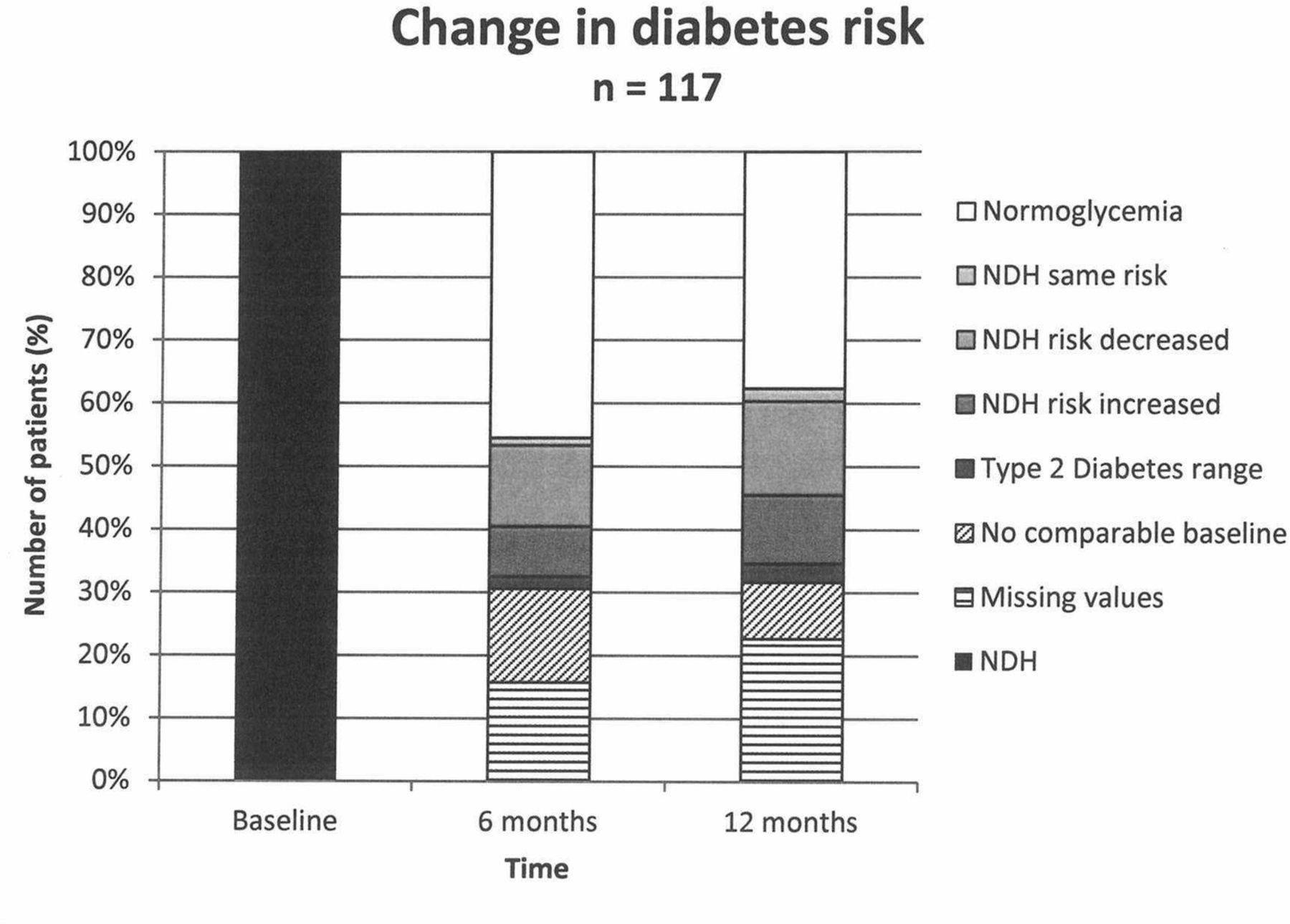
Diabetes risk at baseline, 6 and 12 months.
Clinical, anthropometric and PA measures at baseline, 6 and 12 months
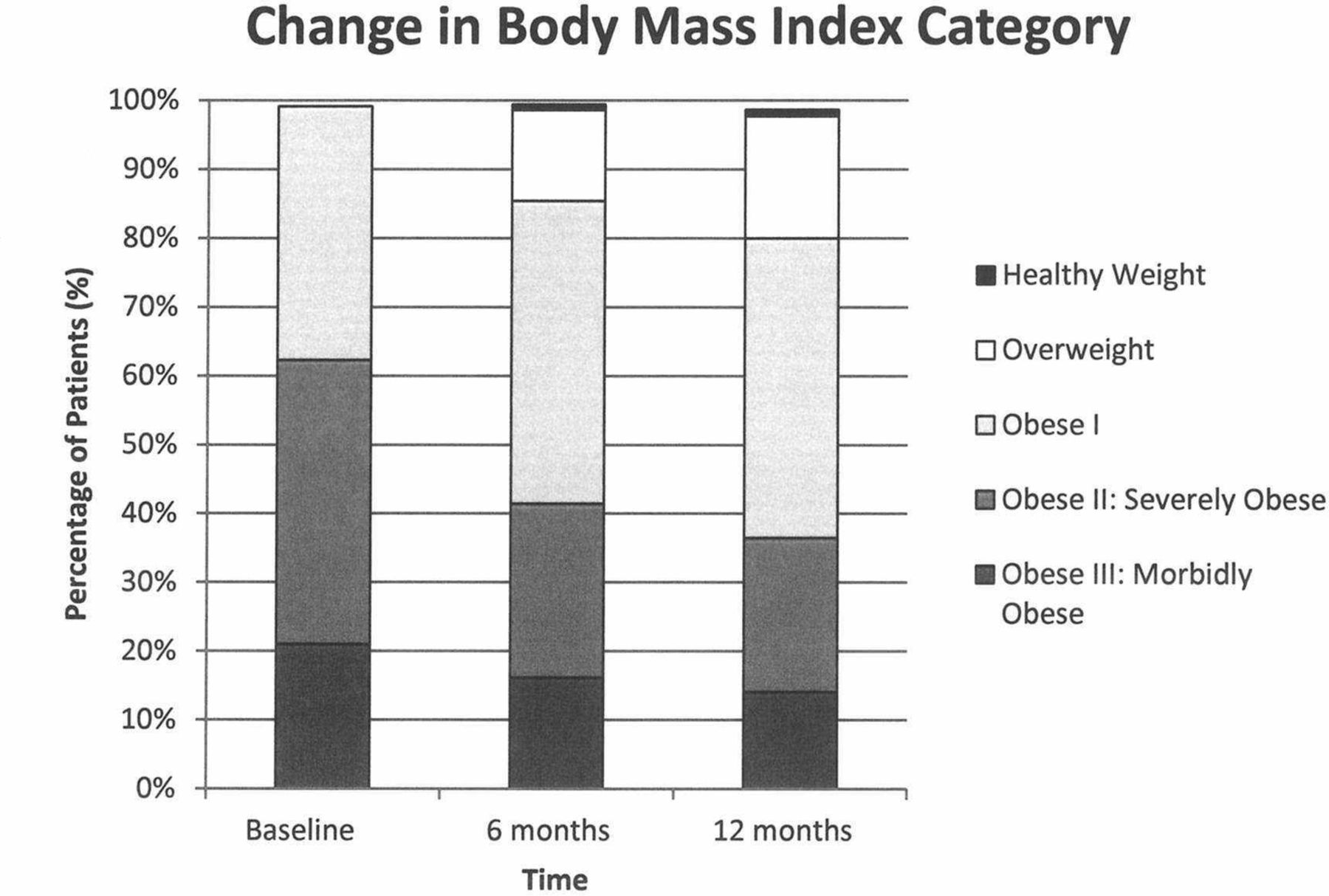
At 12 months, mean weight loss was 10 kg and there was a mean BMI reduction of 3.2 kg/m2 (p<0.001, figure 4). In addition, 54% of patients achieved a greater than a 7% reduction in body weight at 6 and 12 months, which defines the range in which risk reduction is evidenced to occur. At 6 and 12 months, respectively, 14% and 11% of patients reduced their body weight by more than 5% but less than 7%, and 32% and 35% lost less than 5% weight, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Body mass index (kg/m2) at baseline, 6 and 12 months.
Among the secondary outcomes, there was an overall improvement in lipid levels, with significant reductions in triglycerides (p<0.01) and cholesterol/HDL ratio (p<0.05) and a significant increase in HDL cholesterol in males (p<0.05) at 12 months. Both systolic and diastolic BPs significantly improved at 12 months (p<0.01). There was a significant mean reduction in self-reported WC at 12 months in both sexes. There was a mean increase in PA minutes at 12 months of 2 min per week (from 111 to 113 min). Attendance at the program decreased as length of time on the program increased, the average attendance was 29 sessions out of a maximum 48 sessions, attended across an average of 40 weeks.
Discussion
Using an NHS GP referral pathway into a 1 year DPP delivered by this commercial weight management provider achieved statistically significant reductions in measures of T2D risk.
The WWDPP achieved a significant reduction in HbA1c of 2.84 mmol/mol at 12 months (from 43.42±1.28 to 40.58±3.41, p<0.01). The results of this study match optimal interventions and represent clinical success according to the findings of PHE’s meta-analysis which found interventions that halt the upward trajectory of blood glucose but show no overall change could represent considerable clinical success, while, optimal interventions show a reduction in HbA1c of 2 mmol/mol or a reduction in FPG of 0.2 mmol/L or more.10 Although this study evidenced a 0.2 mmol/L reduction in FPG at 12 months, it was not statistically significant. However, given the potential issues with validity and reliability of measuring FPG, the significant HbA1c reduction may be considered a more reliable measure of success.23 It is acknowledged that not all patients at high risk go onto develop T2D; it is predicted that 5%–10% of people per year with NDH will progress to diabetes, with the same proportion converting back to normoglycemia.24 In this study, four patients (3%) developed T2D by 12 months.
The WWDPP achieved a significant mean reduction in weight of 10 kg and a mean reduction in BMI of 3.2 kg/m2. PHE’s meta-analysis found that compared with usual care the pooled mean weight loss of optimal interventions resulted in a mean weight loss of 2.46 kg.10 There was a statistically significant mean reduction in self-reported WC at 12 months; abdominal adiposity is argued to be a stronger predictor of T2D than BMI.25 PA is important especially for NDH patients as PA produces positive secondary outcomes such as improving beta cell function, insulin sensitivity and preventing CVD and depression.3 However, it is difficult for a non-exerciser to understand and define frequency and intensity of PA. Often when patients start exercising, they start to understand the definition of ‘moderate’ intensity and this could explain the large SD in activity reported.20 There were overall improvements in CVD risk,26 with significant reductions in BP (p<0.01), triglycerides (p<0.01) and cholesterol/HDL ratio (p<0.05) and a significant increase in HDL cholesterol in males (p<0.05) at 12 months.
The main strength of this study was that it was successful in addressing the complexities of implementing prevention programs in the real world; patients attended the program and achieved clinically significant results using ITT analysis. Of the eligible referrals, 77% attended the activation session (figure 1), while the PHE’s meta-analysis found that 37% of people who are eligible and referred will take up an intervention.10 The meta-analysis stated that adherence levels of 16 hours across 13 sessions over a 9-month period is optimal for diabetes risk reduction.10 The average compliance in this study was attendance at 29 out of 48 sessions, attended across an average of 40 weeks, as opposed to only 13 sessions across 9 months. However, there was an overall decline in attendance towards 12 months, and consequently the improvements in blood glucose and weight were not as rapid from 6 to 12 months. Therefore, long-term follow-up is needed to see if the results achieved in this 12-month study would be realized in the longer term. Flexibility of the program was important; most international DPPs are curriculum based and use a sequential curriculum in which each session is only offered once, if the session is missed it is difficult to make it up. In the WWDPP, these specifically designed sessions are theme lead, based on participant involvement and often repeated. Sessions are hosted at a variety of times and widely available locations, alongside the digital offerings. The program does not rely on reaching a critical mass to start and patients can attend any session of their choice.
A weakness of real world studies is that selection bias is inherent in uncontrolled, non-randomized and unblinded studies. In this study, there were low referral numbers, and therefore participation by; males, Black or minority ethnic (BME) groups and lower socioeconomic status populations. A higher proportion of the patients were women (75%), from white backgrounds (90%), with only 5% living in the most deprived quintile in the UK. It is likely that some of these features were because only a third of practices in the borough chose to participate in the study, and these were located in areas of lower deprivation and lower proportions of ethnic minorities. Due to ethical considerations, the study did not have a control group; without having a control group, it is difficult to assess if the significant impact on reducing diabetes risk was due to the WWDPP intensive lifestyle intervention or other variables the patient may have been exposed to. Therefore, consideration is needed when interpreting these findings to other populations. This study suffered from missing or inaccurate data; 32 patients’ (27%) weight measures and 27 patients’ (23%) blood glucose measures were lost to follow-up at 12 months, of which 10 patients had no comparable baseline, for example, referred patient based on FPG, followed up patient using HbA1c measurement. GPs also referred 32 (21%) unmotivated patients who did not engage in the program and 17 (10%) ineligible patients who did not match the inclusion criteria.
The Department of Health’s NHS Five Year Forward View strategy (2014) states that the UK will become the first country to implement at scale a national evidence-based DPP.27 The evidence for reducing T2D has been well established for a number of years using gold standard methodology such as RCTs, control groups with large sample sizes.2 This study evidences how to roll out prevention programs in the real world utilizing existing referral pathways. There is a need to spread the findings of what works to ensure the successful delivery of the Five Year Forward View, at a time when public sector budgets are being increasingly squeezed. A strength of this study was that it utilized an existing GP referral pathway rather than expensive outreach recruitment teams or costly letters to patients. There are advantages to utilizing a UK primary care referral mechanism; the GP–patient relationship is important, and trust and rapport are viewed as enablers for patients to engage in referral programs.28 Primary care is best placed to refer patients; GPs have access to practice registers and so can identify retrospective NDH cohorts,29 can refer patients opportunistically and via the NHS Health Checks program and will continue to routinely see patients. NDH and T2D are underdiagnosed nationally6 and still not routinely assessed and coded. Identifying patients within a GP practice for the study increased awareness, diagnosis and referrals. GPs provide continuity of care; there is a seamless transition if patients go onto develop T2D and patients are less likely to be lost to follow-up. The GP referral mechanism into the WWDPP has the potential to have a public health impact at a population level in a relatively short period of time, if scaled up. However, a consideration for clinicians and policymakers is how to engage underrepresented groups such as men, BME and deprived communities.
There are future research opportunities to explore a number of unanswered questions in relation to delivering the best DPP. An RCT to measure the effectiveness of different types of referral routes should be conducted, such as comparing direct to consumer approaches, versus NHS Health Check referrals or primary care referral mechanisms. Analysis should be undertaken to investigate the most effective inclusion criteria, for example, what is the optimal baseline BMI or blood glucose reading for achieving the best results from a DPP. What cohort of patients is a DPP most likely to be effective for? For example, should BME patients, patients with complex mental health needs, vulnerable groups, prisoners, recent migrants, attend specially adapted programs? In-depth analysis into digital technology to prevent T2D is needed. In today’s digital world, research is needed to investigate whether patients would readily accept online delivery of the educational element of the lifestyle intervention and track their lifestyle behavior monitoring via an app.
References
Footnotes
Contributors Carolyn Piper, Agnes Marossy and Zoe Griffiths designed the referral pathway and interface with Weight Watchers, created the data collection tools and undertook data collection. Carolyn Piper and Amanda Adegboye analyzed the data. Zoe Griffiths designed the WWDPP intervention. All authors contributed to the interpretation of data. Carolyn Piper drafted the article and all authors contributed to the critical revision of the article. Carolyn Piper is the guarantor of this work and, as such, takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was funded by the London Borough of Bromley Local Authority Public Health Central Government Grant. Funding was received from Weight Watchers® to publish the research article.
Competing interests Zoe Griffiths is a Registered Dietitian for Weight Watchers and was part of the steering group mobilising this project. The Registered Dietitian was responsible for the training of staff and implementation of the Weight Watchers Diabetes Prevention Programme.
Patient consent Obtained.
Ethics approval The study was performed in accordance with the Declaration of Helsinki Protocols, subjects gave informed consent. The study protocol was approved by the ethics committee of the University of Westminster, (ethics number: VRE1516-0978) and permission obtained by the London Borough of Bromley Public Health Department to access non-patient identifiable data.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full dataset is available from the corresponding author at carolyn.piper@hotmail.co.uk. Participants gave informed consent for annoymised data sharing.