Article Text

Abstract
Objective To estimate age-specific and sex-specific all-cause mortality among adults with and without type 2 diabetes (T2D) in Germany.
Research design and methods The German National Health Interview and Examination Survey 1998 (GNHIES98) included a mortality follow-up (median follow-up time 12.0 years) of its nationwide sample representative of the population aged 18–79 years. After exclusion of participants with type 1 diabetes, age- and sex-stratified mortality rates (MR) were calculated for 330 GNHIES98 participants with diagnosed T2D (self-reported diagnosis or antidiabetic medication), 245 with undiagnosed T2D (no diagnosed T2D, glycated hemoglobin A1c ≥6.5% (≥48 mmol/mol)), and 5975 without T2D. Mortality rate ratios (MRR) comparing MR of persons with and without T2D were estimated. Age-/sex-standardized MR and MRR were calculated including persons aged 45 years or older. MRR were used to estimate the number of years of life lost (YLL) due to diagnosed diabetes in 2010.
Results Over 75 994 person-years, 73 persons with undiagnosed T2D, 103 with diagnosed T2D, and 425 persons without T2D died. MRR were significantly higher in younger age groups, except for analyses limited to women or diagnosed T2D. Age- and sex-standardized MRR (95% CI) among persons aged 45 years or older were 1.96 (1.41 to 2.71) for undiagnosed, 1.68 (1.26 to 2.23) for diagnosed, and 1.82 (1.45 to 2.28) for total (undiagnosed or diagnosed) T2D. Sex-stratified analysis revealed similar age-standardized MRR for undiagnosed (1.56 (0.79 to 3.06)) and diagnosed T2D (1.56 (1.03 to 2.37)) among women, and a higher age-standardized MRR for undiagnosed (2.06 (1.43 to 2.97)) than diagnosed T2D (1.70 (1.10 to 2.63)) among men. YLL due to diagnosed diabetes in Germany in 2010 were 164 600 (35 000 to 279 300) among women and 169 900 (28 300 to 328 300) among men.
Conclusions In Germany, age- and sex-standardized all-cause mortality is almost twice as high for adults with T2D as for adults without T2D. The T2D-associated excess risk of mortality appears to be most pronounced in younger adults and among men unaware of their T2D.
- mortality
- type 2 diabetes
- public health/surveillance
- national health surveys
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
All-cause mortality is significantly higher among persons with type 2 diabetes compared with those without.
Excess mortality in association with type 2 diabetes is a core indicator for diabetes quality of care surveillance, but information stratified by age, sex, and diagnosed versus undiagnosed diabetes is scarce.
What are the new findings?
Excess risk of all-cause mortality among persons with undiagnosed type 2 diabetes is at least as high as among persons with diagnosed type 2 diabetes and about twofold higher compared with persons without diabetes.
Excess risk of death in association with type 2 diabetes is higher among younger than older age groups, with no sex difference observed among persons with diagnosed type 2 diabetes and higher risk among men than women with undiagnosed type 2 diabetes.
How might these results change the focus of research or clinical practice?
Population-based surveillance of excess mortality in association with type 2 diabetes needs to consider differences according to sex, age, and undiagnosed versus diagnosed diabetes.
Younger persons with type 2 diabetes, in particular men with undiagnosed diabetes, need specific attention in secondary prevention.
Introduction
Reducing the increased risk of death associated with diabetes mellitus is a priority goal of national diabetes quality of care initiatives following the 1989 St Vincent Declaration.1 Although type 2 diabetes (T2D) has become a worldwide public health issue, only few countries have been able to evaluate achievement of this goal at the national level by comparing population-based mortality rates (MR) among persons with diabetes with those among the general population or persons without diabetes.2–9 MR derived from official health statistics are of limited use, mainly because coding of the underlying cause of death lacks validity.3 10 Diabetes registers or follow-ups of national health surveys applying valid diagnostic criteria provide a more reliable database. However, registers are limited to diagnosed diabetes and can be run efficiently only in countries with a strong health data infrastructure, including options for data linkage.2 4 5 Population-based cohort studies open the perspective to estimate mortality in relation to diagnosed as well as undiagnosed diabetes, but may face other methodological constraints, such as selection bias, small sample size, or limitation to specific subgroups of the population.
In Germany, standardized mortality ratios (SMR) comparing mortality among persons with diagnosed diabetes with mortality rates of the general population have been reported by the national diabetes registry of the former German Democratic Republic (GDR) amounting to 1.9 in 1961 and 1.7 in 1987.11 More recent estimates are limited to point estimates from population-based cohort studies, including two regional cohort studies and one national cohort study.12–14 While these studies were able to differentiate between persons with diagnosed and undiagnosed diabetes, results are inconsistent with regard to the extent of relative risk of death associated with diabetes and differences between persons with undiagnosed and diagnosed diabetes. This may be explained by differences in diagnostic criteria, composition of the study population regarding age and sex, and study period.15 Moreover, no previous cohort study in Germany provided age- and sex-specific estimates of absolute and relative mortality, although there is evidence from various other countries that relative risk of mortality may decline with increasing age4 5 8 9 16 17 and results on sex differences are inconsistent.2
Against this background the present analysis aimed to assess age- and sex-specific absolute and relative risk of death from all causes associated with T2D based on a mortality follow-up of adults participating in the German National Health Interview and Examination Survey 1998 (GNHIES98). We specifically aimed to assess whether relative risk of death associated with T2D differs between persons with undiagnosed and diagnosed T2D, and whether estimates differ by age or sex. Information on relative risk of death was used to calculate years of life lost (YLL) due to diagnosed diabetes in Germany in 2010.
Research design and methods
Study design and study population
German National Health Interview and Examination Survey 1998
The GNHIES98 is a nationally representative survey of the German-speaking, non-institutionalized, resident population aged 18–79 years in Germany conducted by the Robert Koch Institute (RKI) in 1997–1999.18 A two-stage, probability cluster sampling procedure was applied by first selecting 120 German municipalities reflecting community size and structure of Germany, and second drawing age- and sex-stratified random samples of adults aged 18–79 years from the local population registries.18 The survey included a computer-assisted personal interview (CAPI) administered by a study physician, standardized assessment of medication taken in the past 7 days using the unified product code (Pharmazentralnummer) on medication packaging and coding according to the WHO ‘Anatomical-Therapeutic-Chemical’ classification system (ATC Code),19 20 and an examination including laboratory analyses.21 The GNHIES98 sample included 7124 adults (response rate 61.4%).18
Mortality follow-up
Among GNHIES98 study participants, all but 145 persons had agreed to be contacted again (n=6979). These persons were invited to participate in the National Health Interview and Examination Survey for Adults in Germany 2008–2011 (DEGS1) between October 2008 and October 201122 in order to enable a survey panel component. During the invitation process, vital status was obtained from the local population registries. GNHIES98 participants who did not participate in DEGS1 were censored at the date of the last inquiry at the registry if alive or the date of death (n=671) was obtained. GNHIES98 participants also participating in DEGS1 were censored at the date of the telephone interview, the return date of the questionnaire, or at the date of their visit to the study center (for those attending the examination). Thus, the mortality follow-up could be completed for 98.0% of the original GNHIES98 sample (n=6979/7124).14 22
Study sample and definition of T2D
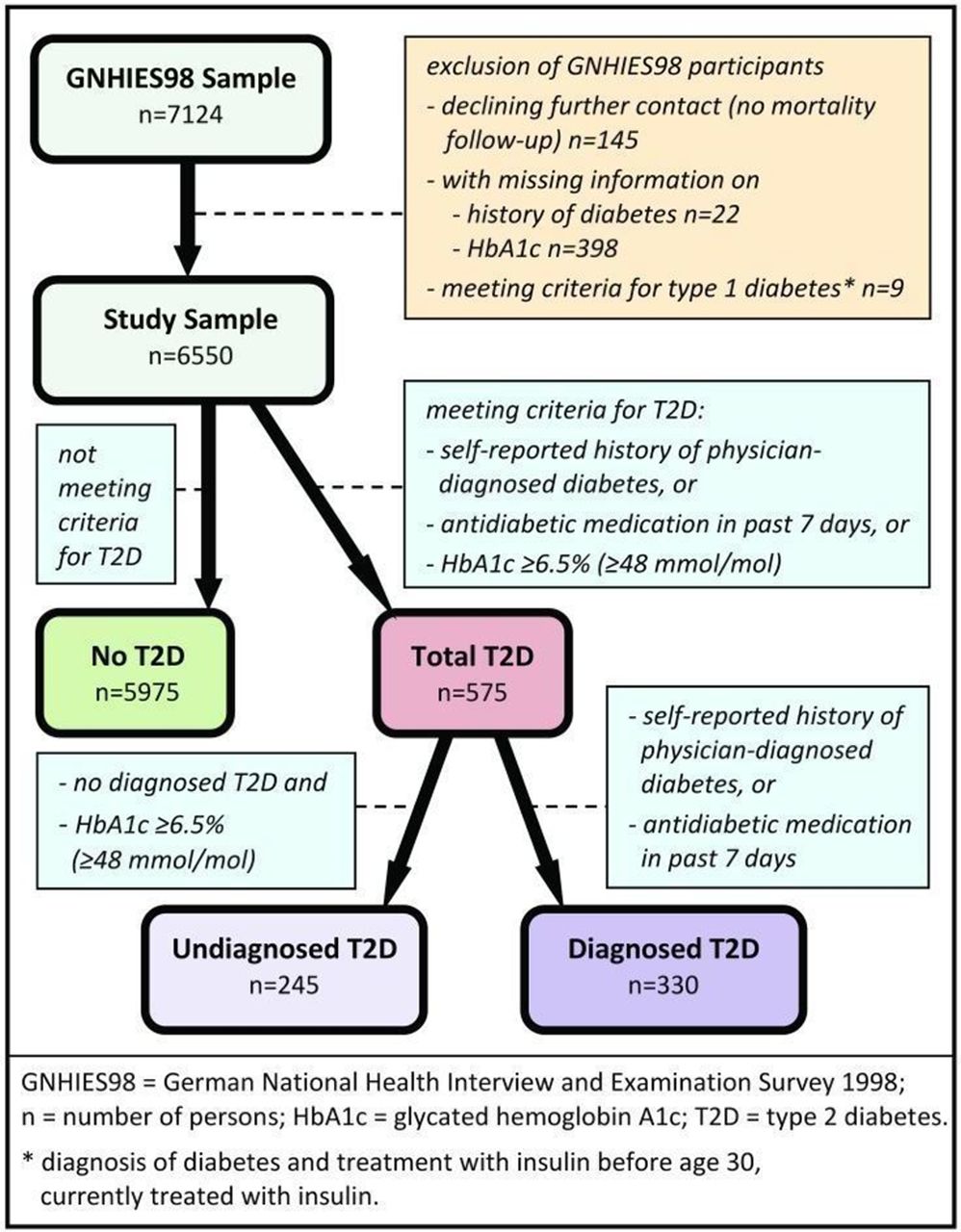
Exclusion of participants from analyses due to missing values or meeting criteria of type 1 diabetes (T1D) is illustrated in figure 1. The final study sample comprised 6550 participants.
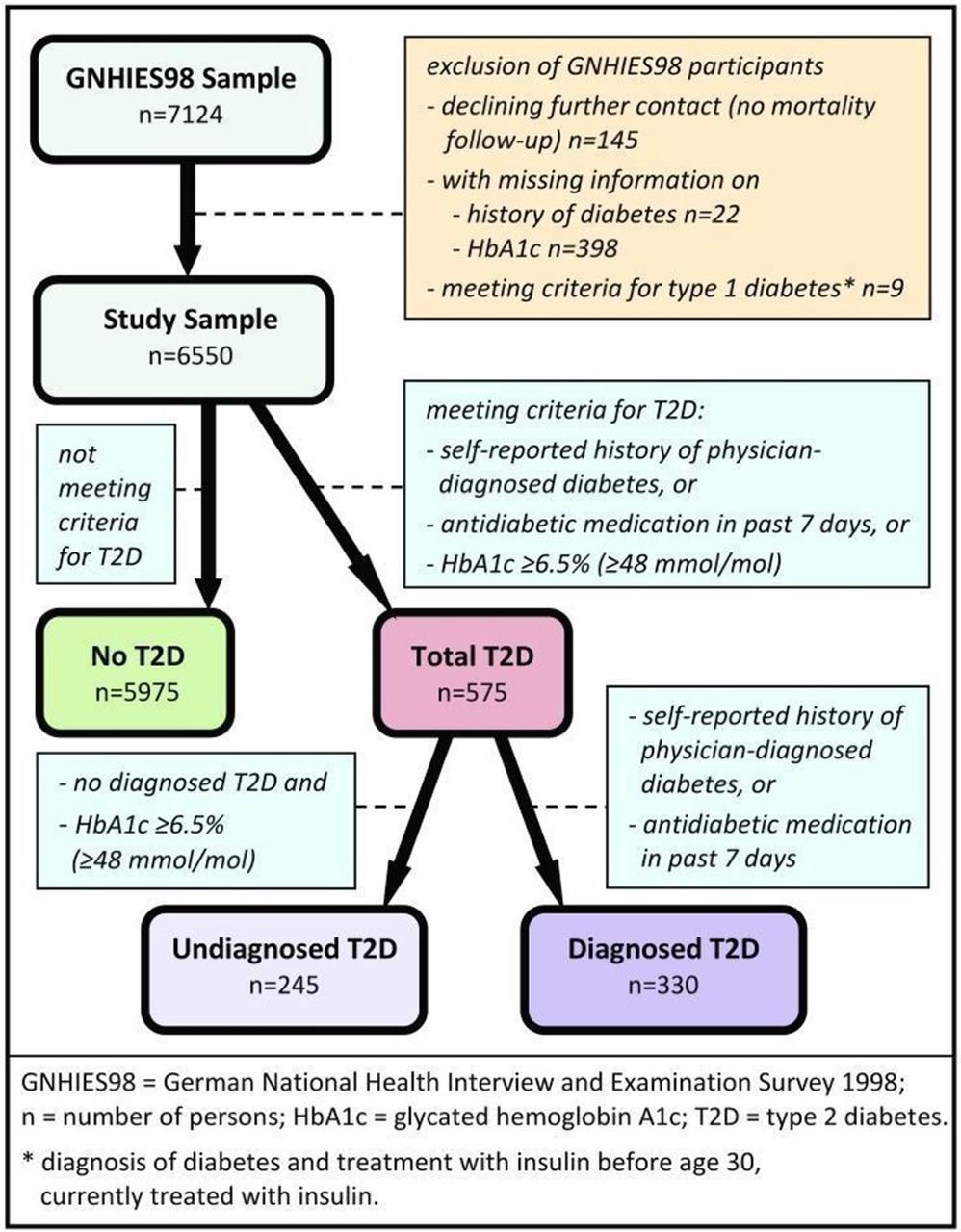
GNHIES98 sample and definition of type 2 diabetes.
Participants meeting the criteria for T1D23 were excluded (figure 1), but identification of other types of diabetes including gestational diabetes was not possible with the information collected in the present study. Thus, persons with diabetes remaining in the study population were assumed to have T2D. Participants were defined at baseline as having diagnosed T2D if they reported a history of physician-diagnosed diabetes in the CAPI or if current use of antidiabetic medication (ATC Code A10A or A10B) was documented. Participants were defined as having undiagnosed T2D if they did not meet the criteria for diagnosed T2D, but had a measure of glycated hemoglobin A1c (HbA1c) of ≥6.5% (≥48 mmol/mol), consistent with established guidelines.24 As previously described,14 HbA1c was measured in whole blood using a Diamat high-performance liquid chromatography analyzer (Bio-Rad Laboratories, Munich, Germany) and reagents from Recipe Chemicals and Instruments (Munich, Germany) in the RKI Central Epidemiological Laboratory.
Statistical analysis
Assignment to age groups
Current age as a time-varying covariate, that is, the actual age at risk of dying instead of age at baseline examination, was used for the assignment to age groups. Lexis expansion25 was performed to split the record of each participant into the periods during which the participant contributed to the corresponding age groups, resulting in multiple records per participant with changing values for the time-varying covariate age group.26 Age groups were chosen to cover 10-year strata except for the youngest (18 to <25 years) and oldest age group (85 to <92 years).
Mortality rates and rate ratios
Age-specific MR were calculated for participants without T2D, with total T2D, with undiagnosed T2D, and with diagnosed T2D by sex as well as for women and men combined. Mortality rate ratios (MRR) comparing age-specific MR of participants with and without T2D were calculated by sex and, controlling for sex by using Mantel-Haenszel estimates, for women and men combined. In order to test for heterogeneity of MRR across age groups, χ2 tests for unequal MRR (effect modification) over age groups were performed.
Crude MR by T2D status were directly standardized to the age and sex distribution of the German population as of December 31, 1997 based on official population statistics,27 and the corresponding MRR were calculated.28 Because of the limited number of participants and events in the younger age groups, standardization was only performed for persons with a current age of 45 years or older, and persons aged 45 to <65 years were pooled into one age group for standardization. Due to the lack of detailed reference data for ages ≥90 years, the German population aged 85–89 years was used as reference weight for the oldest age group (85 to <92 years). Data of the whole German population (women and men) were used as the reference population for sex-specific standardized estimates to permit comparison between women and men.
For crude MR and MRR, 95% CI were calculated using the jackknife estimation method, in order to account for the clustering of records due to the Lexis expansion.29 30 However, for standardized MR and MRR, the jackknife method could not be applied, and 95% CI were obtained using the Wald method.
Years of life lost
In order to provide insight into the burden of disease due to diabetes, YLL due to diagnosed diabetes in Germany in 2010 among adults aged 18 years or older were calculated stratified by sex. The official number of deaths in Germany in 2010 was compared with the number of deaths expected in the absence of excess mortality for diabetes, as previously described.31 Excess mortality was stratified by sex and age and was defined as the difference between the mortality in the population with diabetes compared with the mortality in the population without diabetes.
The calculation of YLL due to diagnosed diabetes was based on the age and sex structure27 and age- and sex-specific mortality32 of the general population in 2010 as reported by the Federal Statistical Office (Destatis). It further required reliable age- and sex-specific prevalence estimates of diagnosed diabetes without upper age limit for the same time period. Pooling of three cross-sectional national health interview surveys of the German population aged 18 years or older (German Health Update, GEDA) conducted in 2009, 2010, and 2012 provided a large (n=62 554) sample for the calculation of these prevalence estimates. Diagnosed diabetes was defined as a lifetime history of self-reported physician-diagnosed diabetes of any type, as information on diabetes type as well as on undiagnosed diabetes was not collected in GEDA.33 34 Relative risk of death associated with diabetes was integrated into the estimation of YLL in the form of age- and sex-specific MRR for diagnosed T2D obtained from the present analysis, which were smoothed by a linear fit of log(MRR) versus age following Gompertz-Makeham law of mortality. Uncertainty of YLL, resulting from sampling errors in the data used for estimation of prevalence of diagnosed diabetes and MRR, was estimated by a bootstrap with 5000 replicates.
Weighting and accounting for complex survey design
For the GNHIES98 sample a composite weighting factor was computed, including a design weight as the reciprocal of sampling probabilities as well as an adjustment weight accounting for deviations between the GNHIES98 sample and the official German population statistics as of December 31, 1997 regarding sex, age, education, nationality (German/non-German), municipality size, federal state, and East/West Germany.18 This weighting factor was applied to all analyses of GNHIES98 data except for descriptive analyses related to the mortality follow-up (sum and median of follow-up time, number of deceased persons; table 1).
Descriptive characteristics of GNHIES98 participants
Given the clustered study design, simple variance estimates will underestimate estimation error. Therefore, survey procedures (SAS procedures surveymeans and surveyfreq) were applied to descriptive analyses not related to the mortality follow-up. Since no survey procedures were available for calculation of MR and MRR, variance of these estimates was presumably underestimated.
Software
Data management, descriptive analyses, and calculation of standardized MR with corresponding MRR were performed using SAS V.9.4, (SAS Institute Inc., Cary, NC, USA). Lexis expansion as well as age-specific and crude overall MR and MRR were conducted using Stata V.14.0, (StataCorp, College Station, TX, USA). YLL were calculated using the statistical software R V.3.2.1, (The R Foundation for Statistical Computing, Vienna, Austria). P values <0.05 based on two-sided tests were considered to indicate statistical significance.
Results
A total of 6550 GNHIES98 participants aged 18–79 years at baseline were followed for vital status over a median follow-up time of 12.0 years (IQR 11.0–12.8). The youngest participant died at 21.3 years of age and the oldest participant was censored at 91.7 years of age.
Descriptive characteristics of the study population from the GNHIES98 by T2D status are provided in table 1, and additionally stratified by sex in online supplementary table S1. Participants with undiagnosed T2D as well as diagnosed T2D were significantly older than participants without T2D. Among adults with T2D, the proportion of undiagnosed T2D tended to be larger among men than among women (45.35% vs 37.57%, p=0.075 in χ² test).
Supplementary file 1
Mortality rates and rate ratios
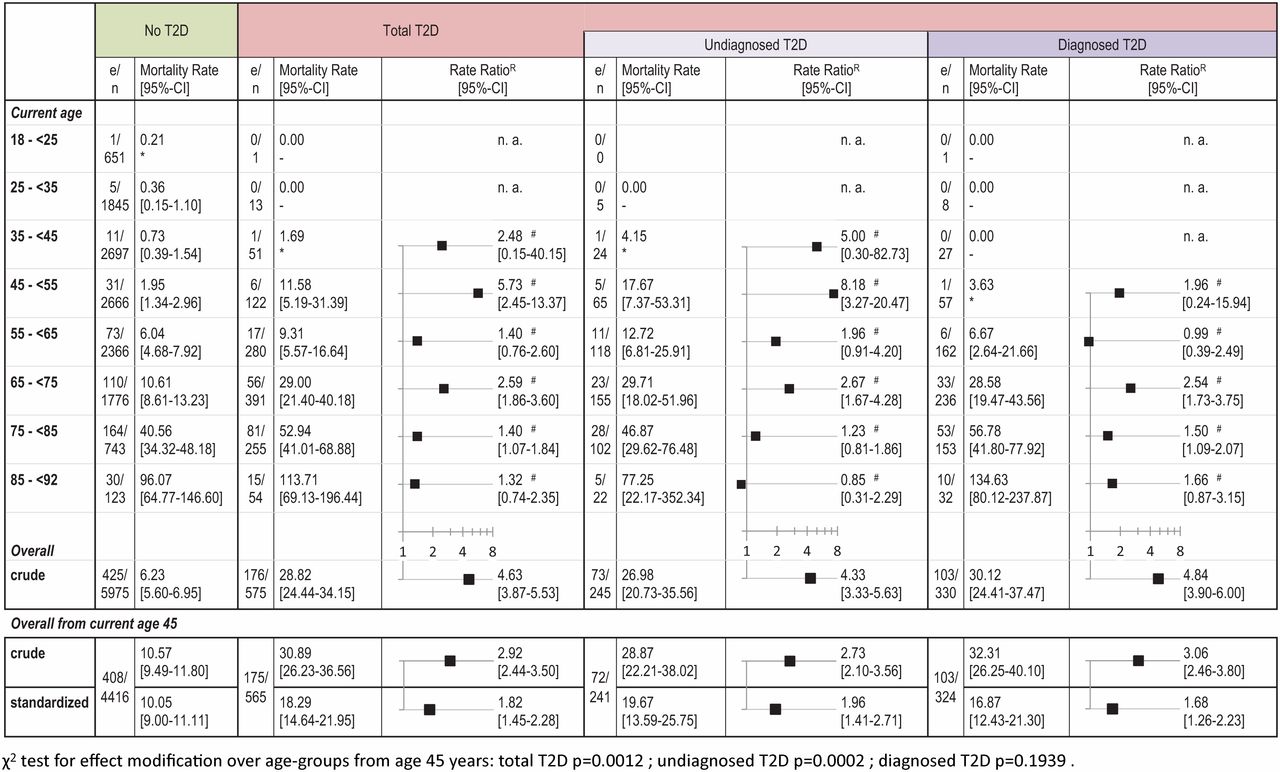
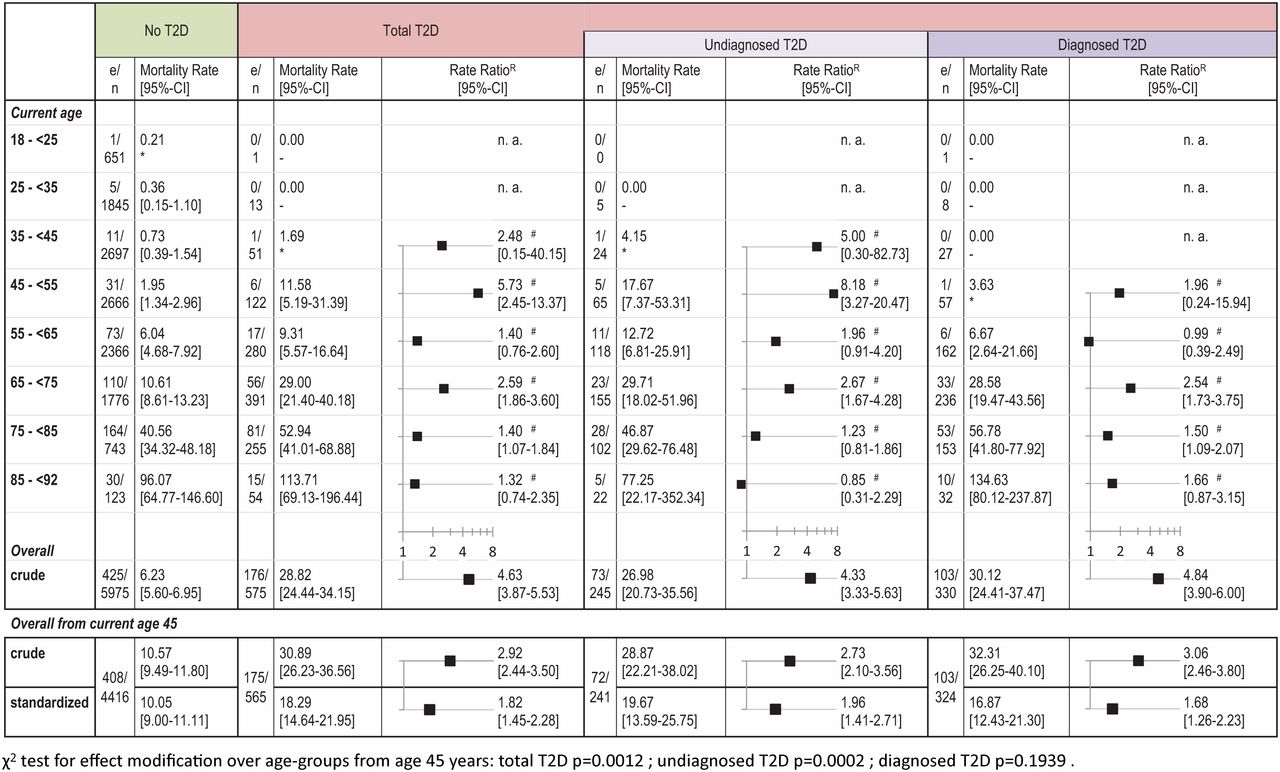
Figure 2 shows MR by T2D status with corresponding MRR for women and men combined calculated from the GNHIES98 study sample. Among persons with T2D younger than 45 years, there was only one death (undiagnosed T2D). MR increased with increasing age regardless of T2D status, while sex-standardized MRR were generally higher among younger than older persons. However, tests for effect modification of MRR across age groups starting from age 45 years were statistically significant only for undiagnosed T2D and total T2D. Age- and sex-standardized overall mortality of persons aged 45 years or older was twofold higher among persons with undiagnosed T2D and 70% higher among persons with diagnosed T2D compared with those without T2D, but 95% CI of MRR were overlapping.
{kind=link}
{kind=link}
Mortality rates by T2D status with rate ratios for German National Health Interview and Examination Survey 1998 participants. Mortality rates as deaths per 1000 person-years with corresponding rate ratios comparing persons with and without T2D. Diagrams with logarithmic scale. e, number of events (deaths); n, number of persons; n.a., not assessable due to low numbers; T2D, type 2 diabetes. RReference: no T2D; #controlled for sex; *95% CI missing because of ≤1 event in stratum. All data except e and n are weighted to the German population as of December 31, 1997. Standardized estimates are age-and sex-standardized to the German population as of December 31, 1997. Age groups for standardization: 45 to <65, 65 to <75, 75 to <85, and 85 to <92 years of current age. Data of the German population 85–89 years were used as reference weight for the age group 85 to <92 years.
In sex-stratified analyses (online supplementary table 2), age-specific MRR also were generally higher among younger than older persons, but tests for effect modification across age groups starting from age 45 years were significant only among men with undiagnosed and total T2D. Age-standardized overall MRR from age 45 years were similar among women with diagnosed T2D and those with undiagnosed T2D (online supplementary table 2A); point estimates indicated a 60% higher risk of death from all causes compared with women without T2D, although 95% CI included one for undiagnosed T2D. In contrast, among men aged 45 years or older, relative risk of all-cause mortality was higher in those with undiagnosed T2D than with diagnosed T2D (age-standardized MRR 2.06 (1.43 to 2.97) vs 1.70 (1.10 to 2.63)), although 95% CI were overlapping (online supplementary table 2B).
Supplementary file 2
Years of life lost
Prevalence of diagnosed diabetes in the pooled GEDA surveys weighted to the German population of 2011 has formerly been reported to amount to 9.2% among women and 8.7% among men.34 Based on prevalence of diagnosed diabetes from GEDA data, the MRR for diagnosed T2D reported above, and official German population data,27 32 YLL due to diagnosed diabetes among adults in Germany in 2010 amounted to 164 600 (35 000 to 279 300) among women and 169 900 (28 300 to 328 300) among men.
Discussion
In our analyses based on a population-based sample nationally representative for Germany, mortality was almost twice as high among adults with T2D as among adults without T2D. Relative risk of death associated with T2D was significantly higher in younger age groups, except for analyses limited to women or diagnosed T2D. The T2D-associated increase in mortality risk tended to be higher for men than women in the case of undiagnosed T2D. YLL due to diagnosed diabetes among adults in Germany in 2010 amounted to approximately 334 000 years without a relevant sex difference.
Results in the context of other studies
Germany
No age-specific estimates of relative mortality associated with T2D from previous German cohort studies are available for comparison with our results. However, corresponding overall estimates from previous studies and this study are compatible despite methodological differences concerning age and sex structure of the samples, diabetes definitions, reference groups, follow-up time, and statistical methods.
The ERFORT study, comprising 1125 men aged 40–59 years from the city of Erfurt, reported age-adjusted hazard ratios (HR) comparing men with diagnosed diabetes with those with normal glucose tolerance (NGT) ranging from 1.86 (1.22 to 2.84) to 2.22 (1.36 to 3.63), depending on duration of follow-up.12 These estimates are slightly higher than our age-standardized MRR for men aged ≥45 years with diagnosed T2D (1.70 (1.10 to 2.63)). The older age range in our sample could explain this difference, as excess mortality declined with age.
The KORA S4 study, comprising a population-based sample of 1466 adults aged 55–74 years from the Augsburg region, reported an age- and sex-adjusted HR comparing persons with diagnosed diabetes with those with NGT amounting to 2.6 (1.7 to 3.8),13 which tends to be higher than the corresponding MRR in our study (1.68 (1.26 to 2.23)).
In the ERFORT study relative mortality was lower among persons with undiagnosed diabetes (HR from 1.48 (1.09 to 1.99) to 1.81 (1.10 to 2.97), depending on duration of follow-up) than among those with diagnosed diabetes, while it was higher for undiagnosed diabetes in the KORA S4 study (HR 2.8 (1.7 to 4.4)) and our analysis (MRR 1.96 (1.41 to 2.71)). A rather unusual definition of undiagnosed diabetes (plasma glucose of >200 mg/dL (>11.1 mmol/L) at 1 hour on oral glucose tolerance testing (OGTT)) in the ERFORT study contrary to definitions of established guidelines applied in KORA S4 (plasma glucose after fasting or at 2 hours on OGTT) and our study (HbA1c) may contribute to this difference.
International
Due to different age and sex structures, comparability of MR and MRR from different countries is limited. Tancredi et al4 followed 435 369 persons with T2D aged ≥18 years in the Swedish National Diabetes Register from 1998 to 2011, a time period corresponding to the follow-up of our study, and compared their mortality with matched controls from the general Swedish population. Lind et al16 used healthcare databases in Ontario, Canada, and The Health Improvement Network database of primary care practices in the UK to calculate annual MR for large samples of adults aged ≥20 years with and without diabetes for the years 1996–2009.
To augment comparability of results, we standardized age-specific MR for adults aged 18/20 to <75 years with and without diabetes published by Tancredi et al and Lind et al and from our data all to the age structure of the official German population as of December 31, 1997 and calculated the corresponding MRR. For the MRR from our data, we compared persons with diagnosed T2D with those without T2D or with undiagnosed T2D to best parallel the condition of register and healthcare databases in the other analyses. Comparison of the standardized MRR thus obtained still needs to consider differences in data sources (register, healthcare database, practice database, survey), diabetes definition, age ranges and groups, and statistical methods. However, the MRR recalculated from our data (1.78 (1.04 to 3.04)) was very similar to that from Sweden (1.77 (1.03 to 3.04)). The MRR obtained for the UK and Ontario using MR averaged for 1998–2009 were higher (2.68 (1.51 to 4.74) and 2.41 (1.28 to 4.53), respectively), yet 95% CI were overlapping between all countries.
Sex differences
Our analysis revealed similar age-standardized MRR for diagnosed T2D among women and men. This might seem surprising, as relative risk of mortality associated with diabetes, especially due to cardiovascular disease, has formerly been reported to be larger among women.3 7 35 36 However, other meta-analyses contradict such sex differences37 38 and SMR in the diabetes registry of the GDR in 1987 did not differ by sex.11 More recently, analyses of excess mortality among US adults between 1997 and 2006 showed no relevant sex difference,6 SMR for women and men in the Danish National Diabetes Register between 1995 and 2006 were almost identical,5 and no interaction between T2D and sex was observed in mortality analyses of data from the Swedish National Diabetes Register.4
Relative mortality associated with total T2D tended to be higher in men than in women in this study. Sex-stratified analyses differentiating between undiagnosed and diagnosed T2D implied that this was mainly due to a higher relative mortality associated with undiagnosed T2D for men than women. A possible explanation for this observation could be a diagnosis earlier in the course of the disease among women than men due to gender differences in the organization and the utilization of preventive healthcare services for younger adults. In Germany, screening for gestational diabetes has been implemented in 2012.39 Among adults 35–44 years of age, men are also significantly less likely than women to participate in free biennial health check-ups for cardiovascular risk factors, offered to people 35 years of age and older who are covered by the statutory health insurance system.40
It has to be considered that the sample size was very small for multiply stratified analyses. Howsoever, young men with undiagnosed T2D might be an important target group for secondary prevention, although further data are needed to clarify potential sex differences in relative mortality associated with undiagnosed and diagnosed T2D.
Variations over age
Several studies in Sweden,4 Denmark,5 the UK,8 16 Canada,9 16 the US,17 and Australia3 reported relative mortality associated with diagnosed diabetes to decrease with increasing age, identifying younger persons to be at especially high risk. Our analyses showed a corresponding trend, although not statistically significant in all subgroups, which was possibly due to the limited number of participants with events resulting in considerable variability especially among younger age groups.
Years of life lost
Our estimates of YLL due to diagnosed diabetes among adults in Germany in 2010 correspond to those from other studies. The Global Burden of Disease, Injuries, and Risk Factors Study (GBD 2013)41 reports YLL due to diabetes in year 2010 in Germany of 111 497 (98 812 to 136 318) for women and 132 803 (125 687 to 140 868) for men. Using KORA S4/F4, Brinks et al42 extrapolated YLL in Germany due to undiagnosed and diagnosed T2D in year 2010 to have been 137 000 (55 000 to 243 000) for women and 166 000 (81 000 to 278 000) for men. These numbers are of similar magnitude as our estimates of 164 600 (35 000 to 279 300) YLL among women and 169 900 (28 300 to 328 300) among men. The ratio of YLL among women and men was similar across studies (0.84 in the GBD 2013, 0.83 in the KORA S4/F4 study, and 0.97 in our analysis).
Strengths and limitations
As a major strength, the present study was based on a large population-based sample representative of the adult population in Germany with a nearly complete 12-year follow-up for all-cause mortality. Highly standardized interview and examination instruments including HbA1c measurement permitted estimates of diabetes-associated mortality risk for diagnosed and undiagnosed T2D with stratification by age and sex, which so far have not been reported for Germany.
The study also shows limitations. First, the limited number of participants with T2D and events, especially in younger age groups, limits the statistical power and informative value of the study particularly in the stratified analyses.
Second, a weight correcting for several sociodemographic parameters including education was used18 to counteract the selection bias inherent to health surveys. Nonetheless, parts of the population are probably misrepresented, as additional factors (eg, severe illness) may affect survey participation and persons aged 80 years or older or living in institutions (eg, nursing homes, hospitals) were not included in the survey, representing groups with a presumably high mortality and T2D prevalence. Exclusion of participants due to missing data might further have reduced representativeness, although a sensitivity analysis that did not exclude participants without HbA1c measurement in the case of diagnosed T2D did not suggest a relevant bias of results for persons with diagnosed T2D due to exclusions for missing HbA1c measures.
Third, misclassification of T2D status cannot be excluded. To exclude participants with diagnosed T1D, we used an epidemiological definition, for which a previous study showed a high positive predictive value.43 However, exclusion of participants with gestational diabetes or other diabetes types was not possible with the available information. Definition of T2D based on self-reported information without external validation may have resulted in misclassification, although validity of self-reported diabetes has been shown to be high.44–46 Furthermore, among asymptomatic patients, repeat testing is required to confirm the diagnosis of diabetes in the clinical setting.24 In the present study this was not possible and the definition of undiagnosed T2D was based on a single HbA1c measurement. Applying a highly standardized analytic method, as was the case in the present study, overall specificity of HbA1c testing at a diagnostic threshold of ≥6.5% (≥48 mmol/mol) is considered to be high.24 47 It is therefore unlikely that we identified a substantial proportion of false-positive cases. Mortality associated with undiagnosed as well as diagnosed T2D was possibly underestimated, because changes in T2D status over time could not be captured in the present study. Consequently, mortality in relation to incident T2D was attributed to the reference group without T2D at baseline. Furthermore, intervention bias may have contributed to underestimation of diabetes-associated mortality. GNHIES98 study participants received information on baseline examination results, including HbA1c measures; this may have resulted in earlier diagnosis and treatment.
Fourth, YLL could only be calculated for diagnosed T2D as we chose to use recent data without upper age limit from national health interview surveys (GEDA) 2009–2012 for calculation of prevalence data, which are required for estimation of YLL.
Finally, since no detailed reference data for age ≥90 years were available for standardization, the oldest age group (85 to <92 years) of the study sample was standardized to the official German population aged 85–89 years, possibly leading to an overestimation of T2D-associated mortality because the oldest age group with a relatively low excess mortality thus received a relatively low weight.
Implications for future research and health policies
Mortality follow-up based on nationally representative German health surveys permits estimates of mortality associated with T2D in German adults, which cannot be obtained from official mortality statistics or diabetes registers in Germany. The results of the present study demonstrate the importance of improvement in diabetes prevention and quality of care in Germany. As of 2010, adults with diagnosed T2D still had an up to 70% higher all-cause mortality risk compared with persons without diabetes, with an estimated 334 000 YLL due to diagnosed diabetes, which accounts for about 2% among YLL due to all-causes of death.41 In addition, the increase in all-cause mortality risk appears to be at least as high for persons with undiagnosed as for those with diagnosed T2D.
Our estimates provide a baseline for surveillance of diabetes epidemiology and quality of care. In addition to the lifetime lost, the amount and quality of lifetime spent with the disease should also be considered in future analyses. This becomes all the more important as several countries report declining MRR in association with diabetes, suggesting improved survival into old age and hence a potential increase in years spent in disability.2 48
Nationwide initiatives to tackle T2D already exist in Germany, such as the implementation of a disease management program for T2D.49 Further effort is needed to fight risk factors, prevalence, complications, comorbidities, and mortality of T2D, in order to reduce the growing burden of diabetes on health economics, society, and individuals. Effective prevention of diabetes remains a major challenge. Population-based strategies for primary prevention will have a key role in order to foster healthy living and healthy environments. In addition, recently published results of randomized trials have refueled discussion on screening for T2D, as early detection and treatment of diabetes appear to reduce complications and risk of premature death among persons with previously undiagnosed diabetes.50 51 Studies evaluating the impact of T2D screening imbedded in the primary care setting will be crucial in order to ensure effective secondary prevention and hereby reduce mortality risk associated with T2D.
Acknowledgments
The authors would like to thank Ingrid-Katharina Wolf and Michael Lange for conducting the mortality follow-up.
References
Footnotes
Contributors SR helped conceptualize the study, calculated mortality rates and rate ratios, conducted standardization of published mortality rates from international studies to the German population 1998 for comparison with results of the present study, and drafted figures, tables, text, and supplementary material of the manuscript. RB helped conceptualize the study, supported the calculation of mortality rates and rate ratios, calculated years of life lost, reviewed and edited the manuscript, and contributed to the discussion. JB supported the calculation of mortality rates and rate ratios, as well as standardization of published mortality rates to the German population 1998, reviewed and edited the manuscript, and contributed to the discussion. CH helped conceptualize the study, reviewed and edited the manuscript, and contributed to the discussion. RP supported descriptive data analysis, reviewed and edited the manuscript, and contributed to the discussion. YD contributed the calculation of diabetes prevalence to the estimation of years of life lost, reviewed and edited the manuscript, and contributed to the discussion. CSN conceptualized and supervised the study and substantially contributed to the writing of the manuscript. CSN is the guarantor who takes full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the manuscript. All authors read and approved the final version of the manuscript.
Funding This work was supported by a research grant from the Federal Ministry of Health Germany (grant number: GE 2015 03 23). The conduction of national health surveys in Germany is funded by the Federal Ministry of Health as part of the continuous national health monitoring.
Competing interests CSN reports grants from the Federal Ministry of Health, Germany, grant number GE 2015 03 23, during the conduct of the study.
Ethics approval Federal Commissioner for the Protection of Data and Freedom of Information.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors confirm that some access restrictions apply to the data underlying the findings. The data set cannot be made publicly available because informed consent from study participants did not cover public deposition of data. However, the minimal data set underlying the findings is archived in the ’Health Monitoring' Research Data Centre at the Robert Koch Institute (RKI) and can be accessed by all interested researchers. On-site access to the data set is possible at the Secure Data Center of the RKI’s ’Health Monitoring' Research Data Centre. Requests should be submitted to the ’Health Monitoring' Research Data Centre, Robert Koch Institute, Berlin, Germany (e-mail: fdz@rki.de).