Article Text

Abstract
Objective Type 1 diabetes mellitus rates are rising worldwide. The health benefits of physical exercise in this condition are many, but more than 60% do not participate, mainly from fear of hypoglycemia. This systematic review explores the effects of physical exercise modes on blood glucose levels in adults for hypoglycemia prevention.
Research design and methods Predefined inclusion criteria were randomized or non-randomized cross-over trials of healthy non-obese adults with type 1 diabetes mellitus. Exercise interventions used standardized protocols of intensity and timing. Outcomes included hypoglycemia during or after exercise, and acute glycemic control. Medline, Cumulative Index to Nursing and Allied Health Literature, Allied and Complementary Medicine Database, SPORTDiscus, CochraneCENTRAL (1990 to 11 January 2018), and Embase (1988 to 9 April 2018) were searched using keywords and Medical Subject Heading (MeSH) terms. Inclusions, data extraction and quality assessment using the Critical Appraisal Skills Programme checklists were done by one researcher and checked by a second. Review Manager (V.5.3) was used for meta-analysis where four or more outcomes were reported.
Results From 5459 citations, we included 15 small cross-over studies (3 non-randomized), 13 assessing aerobic (intermittent high-intensity exercise (IHE) vs continuous, or continuous vs rest) and 2 assessing resistance exercise versus rest. Study quality was good, and all outcome measures were reported. Thirteen gave hypoglycemia results, of which five had no episodes. Meta-analysis of hypoglycemia during or after IHE compared with continuous exercise showed no significant differences (n=5, OR=0.68 (95% CI 0.16 to 2.86), I2=56%). For blood glucose there was little difference between groups at any time point.
Conclusion IHE may be safer than continuous exercise because of lesser decline in blood glucose, but more research needs to demonstrate if this would be reflected in hypoglycemic episode rates.
Trial registration number CRD42018068358.
- systematic review
- type 1 diabetes mellitus
- exercise
- hypoglycaemia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Numerous studies have tried to find safe and effective strategies to maintain normal blood glucose level in people with type 1 diabetes mellitus (T1DM) during and following exercise.
It is currently unclear which types of exercise are best in order to avoid hypoglycemia during and/or after exercise.
What are the new findings?
This systematic review presents all available evidence about different exercise strategies and their effects on blood glucose and hypoglycemic events in people with T1DM to determine the best strategy to minimize the risk of these adverse outcomes.
How might these results change the focus of research or clinical practice?
Intermittent high-intensity exercise may be safer than continuous exercise because of lesser decline in blood glucose, but more research needs to demonstrate if this would be reflected in the number of hypoglycemic episodes.
More research is needed comparing aerobic and resistance exercise.
Introduction
The prevalence of diabetes mellitus has been increasing worldwide, with the number rising from 108 million to 422 million between 1980 and 20141 and estimated to be around 552 million by 2030.2 About 5%–10% has type 1 diabetes mellitus, an autoimmune disease with absolute deficiency of insulin due to beta-cell destruction,3 and the incidence of this type of diabetes mellitus is also increasing.4
Although insulin forms the conventional treatment for type 1 diabetes mellitus, a triad of insulin, balanced diet and better fitness level through regular physical activity is essential in maintaining a good blood glucose (BG) level and complication-free life.5
The health benefits of physical activity in type 1 diabetes mellitus are many, including improvements in insulin sensitivity of the whole body, reduced risk of cardiovascular diseases, hypertension, and malignancy, and increased overall life expectancy, along with increased self-esteem and sense of well-being.6 It is also observed that the frequency and severity of diabetic complications such as nephropathy, retinopathy, neuropathy and cardiovascular diseases are much less in individuals with type 1 diabetes mellitus who engage in more frequent and vigorous physical activity, depending on their fitness levels, compared with those leading a relatively sedentary life with little or no physical activity.7 It is recommended for individuals with type 1 diabetes mellitus to engage in a strategic and integrated exercise regimen.8 Many people with type 1 diabetes mellitus are also interested in participating in sports and are often motivated by famous athletes with diabetes mellitus such as Sir Steve Redgrave.9
More than 60% of people with type 1 diabetes mellitus do not participate in physical activity.10 The contributing factors toward this include lack of time, motivation, support from family and friends, and lack of knowledge regarding appropriate physical activity such as physical exercise,10 but the principal factor seems to be fear of hypoglycemia.11
Numerous studies have tried to find safe and effective strategies to maintain normal BG level during and following exercise.12–16 Carbohydrate supplements and insulin adjustments are effective ways to prevent hypoglycemia, although these are often difficult to regulate, come with potential side effects and used on a trial-and-error basis. Changes in BG level are different with each exercise type and intensity.17 It is currently unclear how best to avoid hypoglycemia during different modes of physical exercise in people with type 1 diabetes mellitus.
This systematic review explores the effects of different types and intensities of physical exercise on BG levels in adults with type 1 diabetes mellitus, during and up to 24 hours following exercise, to understand the most effective exercise-related strategy for hypoglycemia prevention.
Research design and methods
This study was registered with PROSPERO, trial registration number CRD42018068358. The predefined inclusion criteria were randomized or non-randomized cross-over trials or randomized controlled trials of healthy, physically active, non-obese adults (male and female) aged 18–50 years diagnosed with type 1 diabetes mellitus and taking insulin. We included both trained athletes and untrained participants to widen the generalizability of the systematic review. Obesity was excluded because of the possibility that participants might have signs of type 2 diabetes mellitus as well as type 1 diabetes mellitus.18 Participants had to be taking part in short-term exercise interventions consisting of a standardized exercise protocol with controlled intensity and timing. The type of exercise was classified into aerobic, intermittent high-intensity and resistance exercises. Aerobic exercise was defined as continuous exercise involving a large group of muscles in a repetitive manner, for example cycling, running and walking.19 Intermittent high-intensity exercise (IHE) entailed short repeated bouts of intense activity (such as sprints), interspersed with periods of moderate-intensity exercise or rest.16 Such exercise interventions simulate sports activities such as soccer, hockey and rugby, which involve continuous exercise as well as sprints. Resistance exercise incorporates anaerobic activities of short and intense nature (such as strength training and weightlifting). Comparators could be either rest or another type of short-term exercise. The primary outcome was hypoglycemia during, immediately after exercise sessions, or in the early or late recovery period (such as nocturnal hypoglycemia). Hypoglycemia can be defined as BG level below 4 mmol/L.20 Other outcomes included acute glycemic control and requirement of carbohydrate consumption.
Excluded were participants with markers of acute complications (ketonuria, microalbuminuria) to ensure participants had no conditions such as diabetic ketoacidosis, or with pre-existing chronic complications such as diabetic retinopathy, nephropathy or neuropathy because exercise can result in deterioration of these conditions.6 Also excluded were studies on animals, children or adolescents aged less than 18 years, people with type 2 diabetes mellitus or studies with a mix of both conditions. Excluded interventions were those involving prolonged exercise sessions, observing effects on chronic glycemic control as measured by glycosylated hemoglobin (HbA1C), exercise in free living conditions, where insulin was given during the exercise itself, or where BG levels were artificially manipulated.
We searched the following databases (platforms, dates): Medline (EBSCO, 1 January 1990–11 January 2018), Embase (Ovid, 1 January 1988–9 April 2018), Cumulative Index to Nursing and Allied Health Literature (EBSCO, 1 January 1990–11 January 2018), Allied and Complementary Medicine Database (EBSCO, 1 January 1990–11 January 2018), SPORTDiscus (EBSCO, 1 January 1990–11 January 2018) and CENTRAL (Cochrane Library, 1 January 1990–11 January 2018). We did keyword and MeSH searches for terms and synonyms for diabetes, exercise, hypoglycemia and BG, with no language restrictions. Search terms used are shown in .online supplementary appendix. We checked the reference lists of relevant reviews and meta-analyses for additional studies. We transferred all relevant titles and abstracts to EndNote (V.X8) for assessment.
Supplemental material
Data extraction and quality assessment
Two investigators (SH and CAM) checked the study eligibility. One independently extracted data from studies (SH) using a standardized, predesigned extraction form in Microsoft Excel 2007, and everything was checked by a second investigator (CAM). Disagreements were resolved through discussion. We assessed the quality of included studies with the criteria for randomized controlled trials set by the Critical Appraisal Skills Programme,21 focusing on randomization, allocation concealment, presence of masking, explanation of withdrawals, presence or absence of intention-to-treat analysis, and external validity. As the majority of the included studies had a cross-over design, risk of bias was analyzed by indicators in the Cochrane Handbook22: (1) suitability of cross-over design; (2) randomness in the allocation of treatments; (3) presence of carry-over effects as determined by washout periods; and (4) use of appropriate paired statistical analysis.
Statistical analysis
We tabulated the characteristics and results of all included studies; analysis was mainly narrative. We used Review Manager (V.5.3, Cochrane Library) for exploratory meta-analyses where four or more similar outcomes for the same type of exercise and comparator were reported. We used random-effects models because of heterogeneity of participants and interventions. The only outcome meta-analyzed was of categorical measures and we used ORs. Risk of publication bias was not assessed by funnel plot due to lack of studies reporting similar outcomes. There were insufficient studies to warrant exploration of heterogeneity of effectiveness using meta-regression.
Results
We identified 5459 titles and abstracts, from which we assessed 56 full-text articles for inclusion, and 15 studies were included in the systematic review (see table 1), all in English. Excluded studies after retrieving full text are shown in online supplementary table W1. The characteristics of the included studies are shown in table 1 and participant characteristics are in table 2. All included studies had cross-over designs, three were non-randomized, eleven were randomized and one was part-randomized (see online supplementary table W2). The number of included participants ranged from 7 to 13, with ages ranging from 18 to 50 years, and all participants were devoid of any complications and in good metabolic control, with a healthy body mass index. Across the studies, 80% of the participants were male. Four studies included only men,23–26 while the remaining studies included both men and women, with the percentage of women ranging from 7.7% to 56%. All studies recruited participants diagnosed with type 1 diabetes mellitus for at least 1 year who were on regular insulin therapy. Two studies included trained athletes,27 28 one included two trained and ten recreationally active participants,29 and the other studies included participants who were regularly active.
Study characteristics
Participant characteristics
The interventions consisted of short-term exercise sessions with controlled time and intensity. Six studies24 26 30–33 involved short-term continuous aerobic exercise sessions with resting control as comparator. Two studies30 33 involved walking on a treadmill, and the rest used cycle ergometers for the exercise intervention. The duration of exercise ranged from 30 to 60 min. Exercise intensity was determined by heart rate reserve in two studies24 30 and the remaining studies used maximal oxygen uptake (VO2max) to determine exercise intensity. All the exercise sessions were of moderate intensity, with one study having low (25% VO2max), moderate (50% VO2max) and high (75% VO2max) intensities of exercise. Exercise sessions were performed in the morning except in three studies: Maran et al 25 conducted them at approximately 14:00, while Iscoe and Riddell27 and Yardley et al 29 conducted experiments at 17:00. Moser et al 28 did not report on experiment timing.
Seven studies23 25 27 28 34–36 observed the effect of IHE (combined high-intensity exercise interspersed with moderate-intensity exercise or rest). The duration of exercise ranged from 30 to 90 min. All studies determined IHE protocol by maximal sprints interspersed by moderate continuous exercise on a cycle ergometer, except the study by Moser et al 28 which used three different workloads to determine intensities, using lactate turn-point thresholds. Campbell et al 34 also incorporated a different methodological approach for the exercise sessions, where the intervention protocol involved continuous treadmill running and intermittent exercise involved an intermittent running session based on the Loughborough Intermittent Shuttle Test, which was designed to simulate games-type activity.
Two studies observed the effect of resistance exercise on acute glycemic control.29 37 In the study by Yardley et al,29 both continuous and resistance exercises were performed against a resting control. The intensity of continuous exercise was quantified by VO2max and resistance exercise involved sets of weightlifting within certain time limits. Turner et al 37 quantified exercise intensity at 67%±3% of one repetition maximum (i.e. repetition of exercise at maximum intensity) with different amounts per session (one set=14 min, two sets=28 min and three sets=42 min). Hence, heterogeneity regarding study interventions can also be observed in the resistance exercise protocols.
Overall quality of the included studies was generally good, with clear and well-represented results, and with all participants being accounted for in each trial. Among the randomized trials, none mentioned the method of randomization, and only Bally et al 23 mentioned the method of allocation concealment (sealed opaque envelopes). In Yardley et al’s study,29 all control sessions happened first, then participants were randomly assigned to the two types of exercise, hence part-randomization. Three studies28 30 33 used non-randomized cross-over designs with fixed order of trial arms, which may have introduced a period effect. Three studies27 29 32 described participant blinding, and in another three trials lack of blinding was specifically stated,23 31 37 while the remaining trials provided no information regarding blinding. Risk of bias in cross-over studies was minimized by washout periods to avoid carry-over effects between trial arms (see online supplementary table W3 for details). Trial arms for most studies were separated by at least 1 week, although for Soo et al 32 the duration was 2 days.
Apart from the studies by Iscoe and Riddell27 and Moser et al,28 where they recruited only trained athletes for the trial, the other studies recruited non-trained physically active subjects, so results are likely to be applicable to a wide spectrum of fitness levels in the general population. Ten studies required participants to avoid exercise in the 12–48 hours pretrial (see online supplementary table W3), and in Soo et al 32 they were advised to maintain their usual lifestyle. Four studies did not provide any information regarding preintervention physical activity,24 26 28 33 and four studies gave no information about preintervention diet24 29 30 33 (see online supplementary table W4). Seven studies checked for hypoglycemia in the 24–48 hours preceding the trial, and it was postponed in participants in the event of preceding hypoglycemia.23–25 28 35–37 Online supplementary table W4 shows the use of carbohydrate to counterbalance hypoglycemia during exercise.
Participants were treated similarly and equally at the start of the trial for each study. Studies described how accurate measurement of outcomes was performed, and all outcome measures were reported in some way. Thirteen studies reported on whether participants had hypoglycemic events or not, the number of participants with hypoglycemic events, and the number of episodes or mean events per participant, while two studies33 37 did not report this outcome at all (see table 3). Not all studies measured late-onset postexercise hypoglycemia (LOPEH), so intervention effects on nocturnal hypoglycemia were not always reported (see table 3).
Results: hypoglycemia incidents in intervention compared with con
For hypoglycemic events during or just after IHE compared with continuous exercise, meta-analysis showed no significant difference between groups (n=5, OR=0.68 (95% CI 0.16 to 2.86), I2=56%; see figure 1). However, it is noticeable in the meta-analysis that four studies favored intermittent exercise and one favored continuous exercise,25 but it is unclear as to why this study showed opposite results.
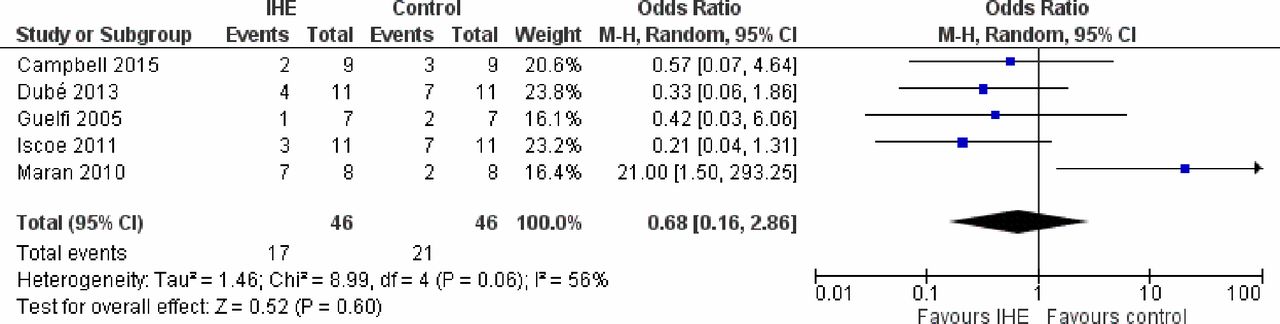
{kind=link}
Meta-analysis of hypoglycemic episodes in intermittent high-intensity exercise (IHE) versus continuous exercise control. M-H, Mantel-Haentzel.
For all studies, the glycemic profiles for the study population were expressed as means; individual patient data were not available so individually paired statistical analyses were not possible. Seven studies24 30–33 35 36 measured acute changes in BG during and immediately after exercise, with the recovery period ranging from 60 to 120 min, but not for longer (see online supplementary tables W5 and W6). However no BG changes during resistance exercise were reported by Turner et al 37; only data at rest and in the early and late postexercise recovery periods were available. Also, none of the studies comparing continuous exercise with rest measured nocturnal BG. The results show that, for IHE compared with continuous exercise, there was little difference between groups at any time point. In continuous exercise compared with rest studies, unsurprisingly, exercise resulted in lower BG levels during and after exercise.
Discussion
Summary of results
Searches identified 15 included studies, of which 7 evaluated IHE compared with continuous exercise, and 6 evaluated continuous exercise compared with rest. Two studies evaluated resistance exercise. All were of cross-over design and had few participants. Hypoglycemic episodes were not reported in three studies, none occurred in either arm in five studies, and there were mixed results in the remaining studies. It is unclear if the type of exercise influences the rate of hypoglycemia or not, and the meta-analysis of IHE compared with continuous exercise showed no significant difference. For BG levels there was little difference between groups at any time point for IHE compared with continuous exercise. In continuous exercise compared with rest studies, unsurprisingly, exercise resulted in lower BG levels during and after exercise.
Strengths and weaknesses
The strength of this systematic review is the meticulous approach toward finding all relevant literature and critical appraisal of their quality to obtain the best evidence for an exercise-related strategy for adults with type 1 diabetes mellitus. Previous reviews focusing on type 1 diabetes mellitus populations irrespective of age might have introduced some bias regarding applicability of results to adult population only, since the metabolic and hormonal response to exercise in adult populations differs from children and adolescents.38 Moreover, this systematic review aimed to obtain the most current literature and incorporated new studies absent from previous reviews, thereby strengthening the evidence base of this systematic review. However, studies with small sample sizes can have much more widely varying results than larger studies. When small study size is coupled with publication bias where studies with null results tend not to be published, it means that systematic reviews of small studies can lead to overestimation of results, and hence the power of the systematic review may be compromised.
There are a number of factors from the included studies that limit the outcome of this systematic review. Methodological heterogeneity was observed throughout the included studies, with varying exercise protocols for IHE, continuous exercise and resistance exercises. There was a lack of standardization or reporting of pre-exercise testing diet. Methods of glucose measurement varied between studies, which may have incorporated some bias in overall results. The most accurate method of glucose measurement is blood sampling and most studies used this technique. However two studies28 36 obtained capillary blood from earlobe, a method which is more inclined to produce erroneous results. Two studies used continuous glucose monitoring (CGM) devices to obtain BG values.23 27 As measurements are obtained from interstitial fluid, there is an obvious delay in detecting the changes in BG level (mean delay 6.7 min).39 Hence, measurements from CGM devices may be less accurate compared with venous or capillary measurements. There was also heterogeneity with regard to timing of blood sampling before, during and after exercise.
Another issue is that most experiments for the IHE were conducted in laboratory-based settings using a cycle ergometer, and only one study used an intermittent running protocol to simulate sports activities. Hence, most studies did not reflect accurately on the nature of team or field-based sports; hence, the generalizability of the results to individuals with type 1 diabetes mellitus involved in sports activities remains in question. Also, the study participants may have been rather fitter than average people with type 1 diabetes mellitus, so the results may not be generalizable to average people with type 1 diabetes mellitus.
Most of the included studies were randomized cross-over trials, but the method of randomization was not explicitly mentioned in any studies except Bally et al.23 Information regarding blinding of participants, study personnel and health workers was also not mentioned in most studies, which might have introduced some bias. However, blinding of participants in such experiments would be difficult due to the nature of the interventions.
Implications for practice
The findings of this systematic review suggest that IHE might attenuate the decrease in BG level during and following exercise, without causing an increased risk of LOPEH, compared with continuous aerobic exercise, but there is insufficient evidence to be certain. It is important for practitioners and patients to understand the different effects of each exercise type on BG level in type 1 diabetes mellitus, for better management of exercise-related BG excursions and to encourage individuals with type 1 diabetes mellitus to participate in physical activity.
Implications for research
The results of this review are based on primary studies with small sample size, with participants with well-controlled, complication-free, type 1 diabetes mellitus. Future research should encompass larger sample sizes and involve participants with complication-free, poorly controlled type 1 diabetes mellitus (HbA1C>10%) to increase the generalizability of the results. If the aim is to improve exercise rates in people reluctant to exercise, then studies should endeavor to recruit people with these characteristics. Such studies should employ rigorous standardization protocols. Future research should also investigate whether gender differences contribute to different results for each exercise type and intensity, In addition, IHE protocols should be used that reflect team sports or field activities and involve real-life situations. BG changes and potential hypoglycemia during a full game, including half-time breaks, could also be observed. If there was more research available, differences between subgroups of trained athletes compared with recreationally active participants could be evaluated. Variations in exercise protocols for IHE and resistance exercises, especially in terms of sprint durations, frequency of repetition, intensity and volume of exercise, are evident in the current systematic review. Hence, research incorporating a more consistent and homogeneous exercise protocol for both IHE and resistance exercise is necessary. Definitions of hypoglycemia should be standard across research.
References
Footnotes
Contributors The project was started as a masters degree dissertation by SH. SMS assisted SH to develop the question for the dissertation and supervised SH to write the dissertation. CAM worked with SH to convert the dissertation to a journal article, including duplicate searches and inclusion decisions. CAM checked the data extraction and conducted the meta-analysis. LHG and CJK assisted with drafting the manuscript and provided internal peer review. CAM and SH responded to external peer review comments. LHG, SMS and CJK edited the final manuscript and approved the submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Not applicable as this is a systematic review.