Article Text

Abstract
Objective: Low sodium intake may trigger sympathetic nervous system (SNS) activation and endothelial dysfunction. Studies have not explored these associations along the glucose continuum. Accordingly, we compared endothelial function and SNS activity in individuals with low sodium intake and differing categories of metabolic risk along the glucose continuum. We hypothesized that low sodium intake is associated with (1) impairment of endothelial function and (2) higher SNS activity in individuals with higher metabolic risk. Research Design and Methods: In this prospective observational study, participants (n=54) with low sodium intake (single 24 hours urine sodium excretion <150 mmol/24 hours) were categorized based on oral glucose tolerance testing as: normal glucose tolerance (NGT, n=10), impaired glucose tolerance (IGT, n=15), treatment naive type 2 diabetes (T2D−) (n=12) or treated type 2 diabetes (T2D+) (n=17). We assessed endothelial function using pulse amplitude tonometry (PAT) derived reactive hyperemic index and PAT ratio; arterial stiffness via augmentation index; muscle sympathetic nerve activity (MSNA) using microneurography; cardiac baroreflex; heart rate; blood pressure; glycosylated hemoglobin A1c (HbA1c) and lipid profile. Results: Mean (SD) sodium excretion was 110.6 (26) mmol/24 hours. Compared with NGT, IGT and T2D−, the T2D+ group had lower MSNA (p=0.005), PAT ratio (p=0.04) and baroreflex sensitivity (p=0.0002) and an augmented heart rate (p=0.02). The T2D+ group had appropriate mean (SD) glycemic (HbA1c 7.2 (1.72)%), total cholesterol (4.2 (1.0) mmol/L), low-density lipoprotein (2.2 (1.0) mmol/L) and blood pressure (systolic 136 (13), diastolic 78 (12)) (mm Hg) control. Conclusions: Individuals with T2D+ have impaired endothelial and baroreflex function, despite low sodium intake, appropriately managed cardiometabolic risk factors and lower SNS activity, compared with others along the glucose continuum. Whether low sodium intake is associated with modulation of the sympathovascular profile in T2D requires further investigation.
- cardiovascular disease
- endothelial dysfunction
- impaired glucose tolerance
- microneurography
- pulse amplitude tonometry
- sympathetic nervous system
- twenty four hour urinary sodium excretion
- type 2 diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cardiovascular disease
- endothelial dysfunction
- impaired glucose tolerance
- microneurography
- pulse amplitude tonometry
- sympathetic nervous system
- twenty four hour urinary sodium excretion
- type 2 diabetes
Significance of this study
What is already known about this subject?
Reduction in sodium intake is believed to lead to a reduction in blood pressure and has been advocated by public health bodies as a strategy to reduce progression of cardiovascular disease (CVD). However, these recommendations have recently been questioned as emerging observational and experimental evidence has shown the paradoxical association between a low sodium intake and adverse cardiovascular outcomes in individuals with type 2 diabetes, possibly through mechanisms such as increased sympathetic nervous system activity and endothelial dysfunction. However, it is not known whether low sodium intake has effects on cardiovascular health outcomes along the glucose continuum.
What are the new findings?
The findings demonstrate that compared with other groups along the glucose continuum, individuals with treated type 2 diabetes who had low sodium intake presented with worse endothelial and baroreflex function.
This was despite a better sympathetic profile and being appropriately managed for cardiometabolic risk factors.
To the best of our knowledge, we are the first to report such observations.
Significance of this study
How might these results change the focus of research or clinical practice?
By determining endothelial function and sympathetic nervous activity in individuals with a varied range of sodium intake (ie, low, average and high sodium intake) along the glucose continuum, we may be able to provide an optimal and practical level of sodium intake to optimize cardiovascular health outcomes.
Future research is required to: (1) assess the association between the renin-–angiotensin aldosterone system and sodium intake on cardiovascular health outcomes along the glucose continuum and. (2) determine if differences in insulin levels or other unmeasured factors such as fitness levels may have played a role in the findings.
Introduction
The burden of type 2 diabetes is rising due to its increasing prevalence and the associated higher likelihood of this population acquiring cardiovascular disease.1 As cardiovascular disease is the leading cause of death worldwide,2 its prevention has become a global health priority.3 The WHO has urged a targeted strategic approach3 to reduce this cardiovascular burden. Lessons learnt from randomized controlled trials assessing intensified glycemic control on macrovascular complications4–6 suggest that in older people with longstanding type 2 diabetes at high risk of cardiovascular disease, intensive glycemic control may not significantly improve cardiovascular health outcomes.4–6 Therefore, optimization of other cardiovascular risk factors, outside of glycemic control, may be as important, or in some individuals more important, for cardiovascular risk reduction.7 Hypertension is one such modifiable risk factor with a reduction in blood pressure being considered capable of reducing the progression to cardiovascular disease.8 Blood pressure lowering may be achieved by lowering dietary sodium intake.8 Not surprisingly, population-wide lowering of sodium intake is recommended,8 with the current sodium intake targets set at less than 2300 mg per day (100 mmol/24 hours).9
In spite of these and other preventative strategies, cardiovascular disease continues to rise.2 Furthermore, our group10 and others11 have previously demonstrated that paradoxically, a lower habitual sodium intake was associated with higher all cause and cardiovascular mortality in individuals with diabetes.10 11 Studies aimed at underpinning the mechanisms responsible for the association between low sodium intake and poor cardiovascular health have been called for by the Institute of Medicine in order to improve overall cardiovascular health in high-risk individuals,12 such as those with diabetes.
Mechanistic studies exploring the sympathetic nervous system seems plausible given chronic sympathetic activation is associated with end organ damage and an adverse clinical prognosis.13 Moreover, as autonomic dysfunction can be detected early on in the progression of diabetes,14 preferentially targeting the sympathetic nervous system may be valuable in lowering cardiovascular disease-related risk in this population. Additionally, studies investigating for the presence of underlying endothelial dysfunction, the precursor to atherosclerosis and cardiovascular events15 are needed, given the potential for earlier intervention strategies. Importantly, as an impaired autonomic reflex is associated with a higher incidence of endothelial dysfunction and mortality in individuals with diabetes,16 targeting both these systems simultaneously may have added benefit in potentially reducing cardiometabolic risk.
However, while sodium is known to have pleotropic effects on sympathetic activity17 and endothelial function,15 there is paucity in data exploring the effect of dietary sodium intake on these systems along the glucose continuum. Therefore, the aim of this study was to compare sympathetic nervous system activity and endothelial function in the setting of low sodium intake along the glucose continuum in individuals who had (1) normal glucose tolerance, (2) impaired glucose tolerance, (3) treatment naive diabetes or (4) treated type 2 diabetes with established cardiometabolic risk factors. We hypothesized that low sodium intake is associated with (1) poorer endothelial function and (2) higher sympathetic nervous system activity in individuals with higher metabolic risk across the glucose continuum.
Methods
Study design and recruitment of participants
In this prospective observational study, individuals who participated in previous studies at two centers (Department of Endocrinology at Austin Health and Human Neurotransmitters Laboratory at the Baker Heart and Diabetes Institute18) with similar experimental methodologies, were selected if they fulfilled the following criteria: age 50–75 years, body mass index (BMI) 25–35 kg/m2, systolic blood pressure <140 mm Hg and/or diastolic blood pressure <80 mm Hg, and absence of acute systemic illness. Additionally, individuals with type 2 diabetes with a history of cardiovascular or cerebrovascular disease were included given these individuals represent the population at highest cardiovascular risk. A low dietary sodium intake was defined as 24 hours urinary sodium excretion (24hUNa) measuring <150 mmol/24 hours from a single collection during the relevant study visit. This cut-off was chosen as we have previously demonstrated sodium intake in the lowest tertile (24hUNa <150 mmol/24 hours) was associated with adverse cardiovascular outcomes in people with type 2 diabetes.10 Given that approximately 90% of sodium intake is excreted by the kidney,19 24hUNa was chosen to provide more accurate estimates of sodium intake. Furthermore, we have previously demonstrated that a single measurement of 24hUNa is able to predict habitual dietary sodium intake in people with type 2 diabetes.20
Exclusion criteria comprised a history of peripheral or autonomic neuropathy; cardiovascular, cerebrovascular, liver or thyroid disease; cancer within the past 5 years; an estimated glomerular filtration rate (eGFR) <45 mL/min/1.73 m2, two or more antihypertensive agents, hormone replacement therapy and sodium-glucose linked transporter 2 inhibitors.
Participants were categorized into four groups: normal glucose tolerance (NGT), impaired glucose tolerance (IGT), treatment naive type 2 diabetes (T2D−) and well established, treated type 2 diabetes (T2D+), based on biochemical results (oral glucose tolerance test (OGTT) or glycosylated hemoglobin A1C (HbA1c))21 or a known history of type 2 diabetes.
Participants in the NGT, IGT or T2D− groups were not taking any medications or dietary supplements. The individuals with T2D+ were expected to be on antihypertensive agents. Agents that could affect the renin–angiotensin-aldosterone system (RAAS) and sympathetic nervous system such as ACE inhibitors, angiotensin II receptor blockers, mineralocorticoid receptor antagonists, centrally acting sympatholytic agents or beta blockers, required a washout period of 6 weeks prior to the participant entering the study for which they were enrolled. These agents were substituted so that participants received calcium channel blockers such as lercanidipine or diltiazem as they are less likely to interfere with the sympathetic nervous system and RAAS.22
All participants provided written informed consent. The previous aforementioned studies were registered as follows: The Department of Endocrinology at Austin Health study was registered with the Australian and New Zealand Clinical Trials Registry, identifier ACTRN12613000127707. The Human Neurotransmitters Laboratory at the Baker Heart and Diabetes Institute18 study was registered with Clinical trials.gov, identifier NCT00408850.
Endpoints
The primary endpoints were to characterize the differences in (1) endothelial function, using pulse amplitude tonometry (PAT) derived measures of reactive hyperemic index and PAT ratio and (2) sympathetic nervous activity, using microneurography to assess muscle sympathetic nerve activity (MSNA), in individuals with a low sodium intake along the glucose continuum. The secondary endpoints were to assess cardiac baroreflex sensitivity, arterial stiffness as measured by the augmentation index, heart rate and blood pressure.
Plasma and 24-hour urine biochemical measurements
Participants without an established diagnosis of diabetes had an OGTT using a 75 g glucose load. A diagnosis of normal glycemic control (fasting ≤6.0 mmol/L or 2 hour <7.8 mmol/ L), impaired glucose tolerance (fasting plasma glucose 6.1–6.9 mmol/L or 2-hour plasma glucose 7.8–11.0 mmol/L) or diabetes (fasting ≥7.0 mmol/L or 2 hour ≥11.1 mmol/ L) was made according to established criteria.21 During baseline study visits, fasting blood samples were analyzed for serum hematological parameters, electrolytes, glucose, creatinine, HbA1c, high sensitivity C-reactive protein, and lipid profile. The 24-hours urine specimens were collected by participants the day prior to clinical investigations and returned on the day of testing. Participants were given prior instructions and advice on the importance of accuracy of 24 hours urine collection. The 24-hours urine specimens were analyzed for sodium, potassium and creatinine excretion.
Clinical investigations
All clinical investigations were performed at the Human Neurotransmitter Laboratory, Baker Heart and Diabetes Institute and were carried out without the influence of caffeine, exercise and alcohol 18–36 hours prior to eliminate any acute effects on investigations. Participants were assessed in the fasting state in a quiet room with an ambient of temperature 22°C. Anthropometric measurements comprised: body weight using a digital scale with bare feet and light clothing, height and BMI. Supine blood pressure was measured after 5 min of rest using a Dinamap monitor (Model 1846SX, Critikon, Tampa, Florida, USA) and recorded as the average of five consecutive measurements.
Assessment of MSNA was performed using microneurography and was performed and analyzed by one investigator (EL). A tungsten microelectrode was inserted directly into the right peroneal nerve at the fibular head.23 A subcutaneous reference electrode was positioned 3 cm away from the recording site. The nerve signal was amplified (×50 000), filtered (bandpass: 700–2000 Hz), and integrated. Simultaneous blood pressure measurements from a finger cuff (Finometer; Finapres Medical System, Amsterdam, the Netherlands) and heart rate via an ECG were made. The blood pressure, ECG and MSNA measurements were digitalized with a sampling frequency of 1000 Hz (PowerLab recording system, model ML 785/8SP, ADI Instruments).23 When a satisfactory nerve-recording site was attained, resting measurements were recorded over a minimum period of 15 min.23 LabChart software (ADInstruments, Sydney, Australia) extracted the beat-to-beat values for MSNA, as well as for R–R interval, systolic and diastolic pressure. Results are expressed as burst frequency (bursts per minute) and burst incidence (bursts per 100 heartbeats).18
Endothelial function was assessed using the EndoPAT 2000 device (Itamar Medical, Israel) that can identify individuals at increased risk of cardiovascular events24 by measuring the reactive hyperemic index and PAT ratio. Additionally, augmentation index was used to measure arterial stiffness. The PAT device was placed on the top of each index finger. Measurements were obtained for 5 min at baseline, followed by 5 min of occlusion of one arm by inflating a cuff on the upper arm to supra systolic blood pressure (60 mm Hg above systolic blood pressure or 200 mm Hg), and then, after releasing the cuff to induce reactive flow-mediated hyperemia, measurements were recorded for a further 5–10 min23 which yielded the reactive hyperemic index. The PAT ratio was then calculated with the calculation used to assess endothelial function in the Framingham Heart Study.23 25
Baroreflex function was determined by measuring the baroreflex slope (ms/mm Hg) and baroreflex effectiveness index using the sequence method of Parati.26 While there is no gold standard technique for the quantification of baroreflex function, the Oxford Method, has been considered as ‘gold standard’ which involves the infusion of vasoactive drugs such as phenylephrine or sodium nitroprusside to alter blood pressure. The reasons for not adopting this technique for the present study was that apart from it being invasive in nature, it may alter autonomic responses during the procedure with an increased risk of profound hypotension.27 For these reasons, our study focused on using the sequence method of Parati. In brief, in this non-invasive technique, sequences were based on the identification of three or more cardiac cycles for which there was a consecutive rise or fall in systolic blood pressure followed by consecutive lengthening or shortening of the R–R interval. Three or more sequences were required for analysis. The slope between cardiac interval and systolic blood pressure was calculated for each validated sequence and averaged over 15 min for the resting recording.
Statistics and data analysis
A one-way analysis of variance was conducted to compare the differences in EndoPAT, MSNA, cardiac baroreflex sensitivity and biochemical characteristics in individuals with low sodium intake and the various metabolic risk conditions of NGT, IGT, T2D− and T2D+. A Tukey post-hoc test was performed if there was a statistically significant difference between groups. Data is represented as mean±SD as indicated. Statistical analyses were performed using STATA V.14.2. Correlations were assessed using Pearson’s correlation coefficient for measuring statistical dependence between clinical investigations and biochemical parameters. A p value of <0.05 was regarded as statistically significant.
Results
Participants
Screening of databases for suitability to enter the study identified 99 eligible participants. As 45 participants had incomplete clinical investigations, a total of 54 participants were therefore included in the final analysis. Participants were then categorized accordingly into the following groups: NGT (n=10), IGT (n=15), T2D− (n=12) and T2D+ (n=17) (online supplementary figure 1).
Supplemental material
Anthropometric, hemodynamic, and biochemical characteristics of the participants
Participants were similar in age and anthropometric measurements (table 1). Hemodynamic measurements revealed that the T2D+ group had higher systolic blood pressure (p=0.04) and heart rate (p=0.002) and demonstrated a trend for higher diastolic blood pressure (p=0.05) compared with the other groups. The mean (SD) sodium excretion for the entire cohort was 110.6 (26) mmol/24 hours with no significant differences between groups (table 1). As expected, the high-density lipoprotein was lower in the T2D+ group as compared with the other groups (p=0.001). Triglyceride levels were similar across groups (p=0.6). Serum cholesterol and low-density lipoprotein (LDL) were lower in the T2D+ group compared with all other groups (p=0.0001 and p=0.002, respectively). These differences in total cholesterol and LDL are likely to be reflective of the high percentage of statin use (82%) in the T2D+ cohort (table 2). The detailed characteristics of the T2D+ group are summarized in table 2. These participants were predominately on metformin (94%) or sulfonylurea (23%) agents and achieved good glycemic control as evidenced by an HbA1c of 7.2% (55 mmol/mol) (table 2).
Demographic and biochemical characteristics between groups (n=54)
Detailed demographic characteristics of treated diabetes participants (n=17)
Assessment of sympathetic activity, endothelial and cardiac baroreflex function, along the glucose continuum
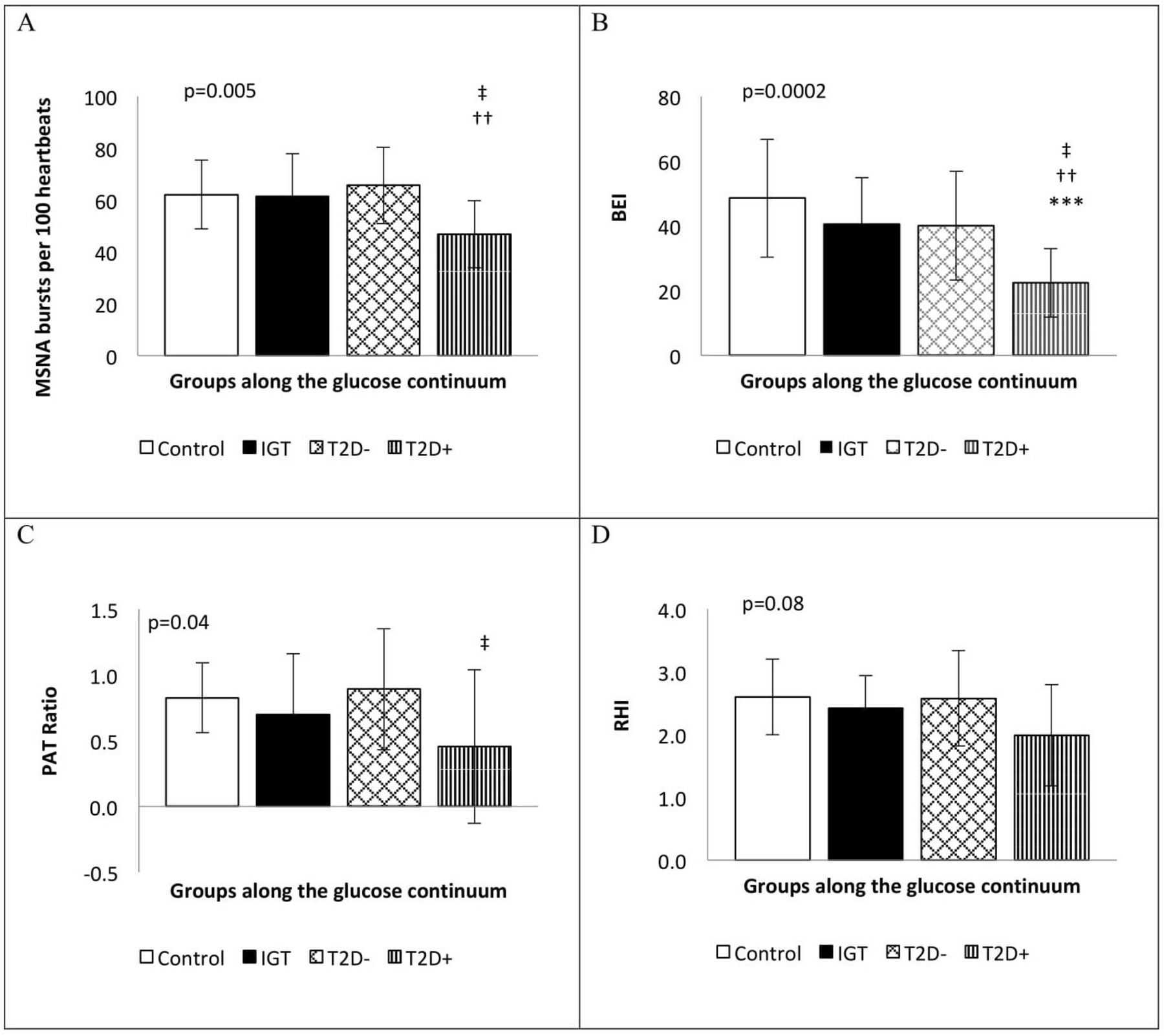
The analysis of MSNA demonstrated that burst incidence was lower in the T2D+ group (p=0.005) (figure 1A) as compared with other groups. As shown in the online supplementary table 1, a Tukey post hoc test revealed that the T2D+ group had lower burst incidence as compared with the IGT (p=0.03) and T2D− group (p=0.006) and trended towards having lower burst incidence as compared with the NGT group (p=0.05). The burst frequency however was not statistically different among groups (p=0.6) (online supplementary table 1).
Supplemental material

{kind=link}
Comparison of sympathetic activity, endothelial function and baroreflex sensitivity between differing metabolic risk categories (n=54). Data is expressed as the mean (±SD). (A) MSNA incidence. (B) Baroreflex function. (C) Endothelial function PAT ratio. (D) Endothelial function RHI. The p values are derived from one-way analysis of variance. Bold values indicate statistical significance. The following symbols indicate Tukey post hoc significance: (*) NGT versus IGT; (**) NGT versus T2D-; (***) NGT versus T2D+; (†) IGT versus T2D−; (††) IGT versus T2D+; (‡) T2D− versus T2D+. BEI, Baroreflex Effectiveness Index; IGT, impaired glucose tolerance; MSNA, muscle sympathetic nerve activity; PAT, pulse amplitude tonometry; RHI, Reactive Hyperemic Index; T2D−, treatment naive type 2 diabetes; T2D+, treated type 2 diabetes.
The endothelial function derived measure of PAT ratio (p=0.04) (figure 1C) was lower in the T2D+ group and the reactive hyperemic index trended towards being lower in the T2D+ group (p=0.08) (figure 1D). There was no difference in arterial stiffness across the glucose continuum (p=0.12) as assessed by the augmentation index (online supplementary table 1).
Despite the lower burst incidence, the baroreflex effectiveness index was shown to be lower in the T2D+ group as compared with all the other groups (p=0.0002) (figure 1B). The baroreflex mean slope, however, was not different among groups (p=0.4) (online supplementary table 1).
Discussion
Key findings
The most important finding in the current study was that despite adhering to a low sodium diet, being appropriately managed for cardiometabolic risk factors and demonstrating a better sympathetic profile, individuals with T2D+ presented with worse endothelial and baroreflex function compared with the other individuals along the glucose continuum.
Individuals with treated type 2 diabetes with low sodium intake demonstrated lower sympathetic activity
In individuals with a low sodium intake, MSNA levels were lower in those with T2D+ as compared with those with NGT, IGT and T2D−. These findings were surprising given we have previously demonstrated that individuals in the early phase of type 2 diabetes had an augmented muscle sympathetic drive characterized by higher MSNA levels.18 These differences in MSNA levels between the current and previous study18 are unlikely to be due to differences in the duration of diabetes as in a separate study; MSNA was demonstrated to be higher in individuals, with established type 2 diabetes,28 with a duration of 22 years, regardless of blood pressure status,29 compared with the non-diabetes population. Sodium intake was, however, different between the current and previous studies.18 28 Sodium intake in the present study was lower, in order to be in line with current dietary recommendations,9 in comparison to the previous studies.18 29 Differences in insulin levels or other unmeasured factors such as fitness levels may have played a role.
Overall, the role of sodium on the sympathetic nervous system remains largely unresolved. Previously, in the non-diabetes population, a low sodium intake has been associated with an increase in MSNA.30 31 Additionally, in studies utilizing other methodologies to assess sympathetic activity, such as catecholamines, results are again inconsistent with the demonstration of low sodium intake either increasing plasma catecholamines17 and renal norepinephrine spillover to plasma32 or being associated with no significant alterations in plasma norepinephrine.33 The observation from this study, of MSNA being lower in the more established diabetes group as compared with the other groups in the setting of a low sodium intake, adds to the uncertainty surrounding the role of sodium on sympathetic activity and deserves further evaluation. Using a combination of the MSNA and urinary or plasma catecholamines, to assess cause and effect would be prudent to further validate our findings.
Endothelial, baroreflex and heart rate function were impaired in the treated diabetes group in the setting of low sodium intake
Despite the low sodium intake and the enhanced sympathetic activity as aforementioned, the T2D+ group demonstrated a lower PAT ratio and a trend for a lower reactive hyperemic index, suggestive of endothelial dysfunction.24 Additionally, a lower baroreflex effectiveness index was observed in the T2D+ group, suggestive of an impaired baroreflex function. This is consistent with previous reports demonstrating a reduced baroreflex function in individuals with type 2 diabetes.18 However, the impaired baroreflex function comes as a surprise as physiologically baroreflex function usually decreases in the presence of sympathetic hyperactivity; yet, in the present study, we demonstrated lower sympathetic activity in the T2D+ group. Likewise, while expecting a lower heart rate in the T2D+ group given the lower sympathetic activity, in the present study, heart rate was higher in the T2D+ group which is consistent with previous reports of individuals with higher fasting glucose demonstrating higher resting heart rate.34 As possible adverse health outcomes may be associated with low sodium intake in individuals with diabetes10 11 and given an impaired endothelium15 and baroreflex35 as well as an increased heart rate34 are known to be independent risk factors for increased cardiovascular and all-cause mortality, the observations from the present study are important to further characterize in future studies.
Unraveling the answers to the above mechanistic concerns remains difficult. Previously, Dickinson et al suggested that a low sodium diet increased flow-mediated dilatation36 in the non-diabetes population. However, reactive hyperemic index was unaffected.37 Similarly, the role of dietary sodium is unclear on baroreflex function. While previous findings have demonstrated reduced baroreflex sensitivity occurred in those with a high sodium intake, based on dietary recall,38 Couruzi et al39 demonstrated the opposite, in that a high sodium diet improved spontaneous arterial baroreflex sensitivity. Concerning heart rate, former studies, in individuals without diabetes, have demonstrated similar findings of a low sodium intake leading to higher rate40 and a high sodium intake was found to lower heart rate in hypertensive39 individuals. However, other studies have demonstrated no significant increase in heart rate with lowering of sodium intake.30 Overall, the differences in methodology and assessment of sodium intake as well as paucity of studies evaluating the high-risk diabetes population need to be addressed in larger cross-sectional or interventional trials to further elucidate the role of sodium on endothelial and baroreflex function.
The impact of pharmacological agents used in the treated type 2 diabetes group on the clinical investigations
As we have previously demonstrated an association between circulating lipid species and central sympathetic outflow41 and others have shown that statin therapy is capable of reducing sympathetic nervous activity,42 the high use of statin therapy in the T2D+ group, as compared with no use of statin therapy in the other groups, may have contributed to their lowered MSNA levels observed in this study.42 Additionally, the use of antidiabetic therapy in the T2D+ group, which was an unavoidable difference, may have impacted the findings. However, participants in the study by Huggett et al29 were also mainly treated with metformin; yet, no differences in MSNA were observed in those with or without metformin therapy. Additionally given and metformin43 and statin therapy44 may be associated with improved endothelial function, it would therefore be expected for the T2D+ group to have had better endothelial function parameters than were observed. Thus, overall, in the present study, it is deemed unlikely that statin therapy or metformin use played a significant role in lowering sympathetic activity.
Strengths and limitations of the study
The study being cross-sectional in design limits insight into causality. As sodium intake was required to meet the public health guidelines criteria of less than 2300 mg per day (100 mmol/24 hours),9 many people did not meet these criteria. This is not surprising given the challenges faced in achieving population-wide sodium restriction targets, especially in people with type 2 diabetes.20 We acknowledge that we did not have an average or a high sodium intake group as a comparator. However, this study was conducted to help understand endothelial function and sympathetic nervous activity in individuals with low sodium intake along the glucose continuum given we have previously demonstrated the association of lower sodium intake and adverse cardiovascular outcomes when 24hUNa excretion was <150 mmol/24 hours in people with type 2 diabetes.10 Measurement of aldosterone and plasma renin levels to further assess the effect of RAAS and plasma catecholamines to assess sympathetic nervous system activity would have been advantageous. Other important factors that may influence the sympathetic nervous system activity and heart rate, such as fitness levels and fasting and postprandial insulin levels, would have been ideal to have available for all groups. While these measurements were available from our previous study18 in the NGT, IGT and T2D− group, they were not available in the T2D+ group. These aforementioned factors could be incorporated into future studies in this area.
While autonomic dysfunction can be estimated from indirect measurements such as heart rate variability, we utilized microneurography in the present study, which is considered to be the reference method for assessing sympathetic activity.45 Only a few other studies, such as those from our group18 and others,28 29 have utilized this technique in people with diabetes. However, as we only examined sympathetic outflow to skeletal muscle, we cannot translate these findings to other organs. Utilizing 24hUNa is considered a further strength given it is considered the most reliable method for estimating sodium intake.46 Endothelial function was measured in the peripheral digits rather than the coronary circulation; however, EndoPAT has been shown to provide a high degree of sensitivity and specificity when compared with the assessment of coronary artery endothelial function cardiovascular events.24
Conclusions
The present study makes noteworthy contributions, demonstrating that despite the lower sympathetic activity in individuals with treated type 2 diabetes, endothelial function, baroreflex function and heart rate were impaired as compared with those with NGT, IGT and treatment naive type 2 diabetes. This occurred even though individuals with treated type 2 diabetes were appropriately managed for their cardiometabolic risk factors and, importantly, adhered to recommended sodium intake guidelines. Interventional studies aimed at looking at the association between the sympathovascular systems are required, if the debate surrounding the role of sodium on cardiovascular health is to be moved forward.
Acknowledgments
We thank our study participants, the Endocrinology Department at Austin Health and the Human Neurotransmitter Laboratory, Baker IDI for access to the databases and the respective pathology laboratories for blood and urine biochemical analysis. We are grateful to Ms Carolina Saki and Ms Robyn Hemmes for assistance provided to Dr Lambert during microneurography and EndoPAT testing.
References
Footnotes
Contributors SB, EIE and EL conceived the study and selected participants from the Department of Endocrinology, Austin Health and the Human Neurotransmitter Laboratory, Baker IDI databases respectively and interpreted the data. SB, NS and YWK collected clinical data. EL performed microneurographic recordings and analyses. SB performed the statistical analyses, wrote and revised the manuscript. All authors critically read and approved the final content of the manuscript. SB is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding EIE was supported by an NHMRC Early Career Research Fellowship (#1054312), Viertel Clinical Investigatorship, Sir Edward Weary Dunlop Medical Research Foundation grant, Royal Australian College of Physicians fellowship and Diabetes Australia Research Program Grant. SB was supported by a National Heart Foundation Health Professional Scholarship (100287).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Human Research Ethics Committee at the Austin Health as well the Baker Heart and Diabetes Institute and Alfred Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no additional data from this study.