Article Text

Abstract
Introduction
The United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) is the main primary healthcare provider and provides assistance and protection to around 5 million Palestine refugees in Jordan, Lebanon, Syria, West Bank and Gaza. Diabetes mellitus (DM) is a common problem among Palestine refugees, with a prevalence of 11.0%. In 2014, UNRWA embarked on a diabetes campaign to assist both patients with DM and staff in improving diabetes care management, by building the capacity of UNRWA’s health staff and improving the knowledge and lifestyle behaviors among Palestine refugees with DM.
Method
Using a quasiexperimental study, we randomly selected 50 patients with diabetes from the 32 largest UNRWA health centers (HC); a total of 1600 participants were enrolled. Each HC conducted weekly group sessions for 6 months, including education, healthy cooking, and physical exercise. Body measurements, 2-hour postprandial glucose test, blood pressure and session attendance were collected on a weekly basis. Demographical data, pre/postquestionnaires and cholesterol levels were collected before and after the campaign. Paired t-test in SPSS V.21 was used.
Results
Out of 1600 patients, 1598 (1186 (74.0%) females and 412 (26.0%) males) completed the campaign; 576 (36.0%) patients had diabetes type 2 (DMII), 960 (60.0%) had DMII and hypertension and 62 (4.0%) had diabetes type 1 (DMI). After the campaign, the average weight loss was 2.6 kg (95% CI 2.4 to 2.7). In addition, 22% lost ≥5%, 25% lost 3%–5%, and 30% lost 1%–3% of their weight. Significant improvements were seen in blood glucose, cholesterol and waist circumference (WC) (p≤0.001 for all). The session attendance rate was 70.6% in total.
Conclusions
This campaign focused on raising healthy lifestyle awareness and practices among Palestine refugees with DM. It was associated with reduction cardiometabolic risk factors. Similar campaigns need to be sustained and expanded. Local community and non-governmental organization partnerships observed during the campaign should be strengthened and sustained.
- UNRWA
- Palestine refugees
- diabetes mellitus
- campaign
- healthy lifestyle
- weight loss
- group sessions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Lifestyle intervention studies are successful in leading to weight loss in patients with diabetes.
According to the United Nations Relief and Works Agency for Palestine Refugees in the Near East’s clinical audit results the prevalence of diabetes is 11%. It was revealed that over 90% of patients with diabetes mellitus (DM) are overweight or obese, with the majority (64%) being obese.
What are the new findings?
This campaign had positive impact on body measurements and blood glucose in Palestine refugees with DM.
How might these results change the focus of research or clinical practice?
More studies should be done to study the effect of using variety of educational sessions, specially cooking and exercise session, in the refugee camp settings.
Introduction
Mandated by the United Nations (UN) General Assembly, the United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA) started its operations in 1950. It provides humanitarian assistance and protection to the registered Palestine refugees in the five fields, including West Bank, Jordan, Lebanon, the Gaza Strip and Syria. Funded entirely by voluntary contributions by different donors, UNRWA’s humanitarian services and human development encompass education, primary healthcare, relief and social services, camp improvement and emergency response in situations of armed conflict. It is the main primary healthcare provider for Palestine refugees.1 2 Palestine refugees represent the largest refugee population in the world.2
UNRWA has been providing healthcare for patients with diabetes mellitus and hypertension (DM&HTN) in its health centers (HC) since 1992. UNRWA’s diabetes care includes screening of high-risk groups, diagnosis and treatment. In 2014, UNRWA had more than 231 000 registered Palestine refugee patients with non-communicable disease (NCD). The increased burden of NCDs presents a tremendous challenge for the agency accounting for 41% of its total budget spent on medications. With an ageing population, the primary challenge is no longer communicable diseases; rather, it is actually in dealing with comorbidities associated with NCDs.DM, cardiovascular diseases and other NCDs are now responsible for 70.0% of deaths in UNRWA’s population.2
Heart diseases, cerebrovascular diseases, and cancers are the major causes of morbidity and mortality for the population in occupied Palestinian territory and some of the neighborhood countires.3 According to UNRWA’s 2014 records, the prevalence of diabetes among the general population where Palestine refugees live is known to be 10.1% in Jordan; 7.8% in Lebanon; 8.6% in Palestine; and 10.8% in Syria.4 The urbanization and continuing nutritional change from a healthy Mediterranean diet to an increasingly Western-style diet are associated with a decrease in physical activity, obesity, and a loss of the traditional diet benefits.4 As seen throughout all of UNRWA’s areas of operation, specifically for Palestine refugees, they experience a high level of stress due to many environmental stressors: the ongoing political tension and conflict, lack of security, high rate of unemployment, and poor infrastructure in refugee camps. Consequently, there has also been a rise in NCDs, especially diabetes, HTN, and mental disorders.3
Obesity is recognized as one of the most important risk factors for DMII, as it induces insulin resistance and pancreatic beta-cell dysfunction.5 Studies have demonstrated that lifestyle interventions are successful in leading to weight loss in patients with diabetes.6 There are different challenges that UNRWA faces when dealing with diabetes care,1 2 therefore, to acquire information on the diabetes care in the UNRWA HC, the agency has performed a clinical audit in 2012. It was revealed from this clinical audit that over 90% of patients with DM are overweight or obese, with the majority (64%) being obese. UNRWA’s clinical audit had recommended many action steps to be taken, such as: developing a comprehensive package of lifestyle support activities that can be implemented in HCs at no additional cost. It also recommended that UNRWA should change the involvement of nurses and paramedical staff in diabetes care delivery to be more proactive, in order to improve health promotion, education and adherence.7
Responding to the above results, in 2013 UNRWA’s health department embarked on a campaign titled ‘Life is Sweeter with Less Sugar’ which aimed to assist both patients and healthcare providers in changing their attitude and behavior to prevent and control diabetes among Palestine refugees attending UNRWA HCs. Additionally, within Palestine refugee camps, it included efforts to raise the local community’s awareness of the risk factors that can lead to one’s development of diabetes and stressed the importance of healthy lifestyle practices. Funded by the World Diabetes Foundation, this campaign consisted of two prongs: first, outreach and screening activities for detecting new cases of diabetes within the local community; and second, conducting educational group sessions for the registered patients with DM at UNRWA HCs in Jordan, West Bank, Gaza and Lebanon. Also, on a weekly basis for 6 months, 30 HCs conducted educational, healthy cooking, and exercise group sessions for its local communities.
Body measurements, blood tests, and patients’ attendance records were collected monthly. There were 1174 (951 females, 223 males) who completed the diabetes campaign (out of 1300 who were recruited). After the campaign, 185 (16%) lost ≥5%, 226 (22%) has lost between 3% and 5% and 377 (33%) has lost between 1% and 3% of their weight. Waist circumference (WC) mean decreased from 108.5±13.1 cm to 106±13.2 cm with (−2.6±4.9 cm) reduction in the total mean. Also, significant improvements were seen in blood glucose and cholesterol (p<0.001).8
Social networks play a strong role in people’s health behavior, especially in a refugee camp setting. Since diabetes management requires behavioral changes and adherence to healthy lifestyle practices, social support is considered to be one of the influential and important factors for performing self-care and for adherence to the treatment and disease control.9 In order to validate this model of care delivery in refugee camps, UNRWA’s health department has expanded this campaign and replicated it in 32 UNRWA HCs, with the objectives of improving the cardiometabolic risk factors, knowledge and lifestyle behaviors of diabetes care management among Palestine refugees with DM, and enhancing the capacity and technical skills of UNRWA’s health staff for better delivery of diabetes care management to the Palestine refugees who attend UNRWA HCs.
Methodology
In a quasiexperimental design without control group,10 we aimed to to expand on the model used in 2013 for diabetes care among refugees.8 The intervention, labeled as DM campaign, took place in UNRWA HCs across four fields (Jordan, the West Bank, Lebanon, and Gaza). The intervention consisted of three components: (1) physical activity session, (2) healthy cooking session, and (3) disease management session.
Due to the complexity of the refugee setting, we used a quasiexperimental design as we cannot have a control group in refugee camp settings. We think it was not feasible or ethical for a UN agency such as UNRWA to conduct a randomized controlled study on their beneficiaries.
Patient enrollment and HCs selected
Inclusion and exclusion criteria
Patients attending the selected HCs with confirmed (based on the diagnostic criteria in HCs) fasting blood glucose (FBG) reading above 126 mg/dL, or two positive readings of 2-hour postprandial blood glucose (2hrPPG) above 180 mg/dL, or oral glucose tolerance test if the FBG is between 110 and 125 mg/dL.
DM, both DMI (with or without HTN) and DMII (with or without HTN), and had received care at UNRWA NCD clinics for at least 1 year.
Patients were willing and committed to participatinge in all planned activities and gave verbal informed consent.
Our exclusion criteria were non-Palestine refugees with DM or Palestine refugees who are not registered in UNRWA HCs.
Sampling
For the DM campaign sampling, we followed the same procedure used in UNRWA’s clinical audit,7 as it included 1600 patients with diabetes which were selected from the 32 largest UNRWA HCs in four of UNRWA’s fields: Gaza, Jordan, Lebanon and West Bank. For this second diabetes campaign, we followed the same clinical audit sampling methodology as follows: eight of the largest HCs in each field were chosen to be included in the campaign and each selected HC was instructed to randomly select 50 patients with DM or DM&HTN from their NCD clinics. Therefore, the total number of participants enrolled was 1600 (50 patients from the eight largest HCs in four fields of UNRWA’s operation) for 6 months.
After verbal consent, patients were selected to be part of the campaign activities. Before starting the activities, all selected HCs were provided with posters and brochures to promote the launch of the campaign and its activities.
Activities conducted
The campaign took place from May 2014 to February 2015, we scaled up its activities compared with the first campaign in 2013.8 An intensive preparation phase had taken place, with more focus on handling the obstacles that might face UNRWA HCs, before launching the campaign. An active communication channel between health departments in the headquarter, field offices, camp offices, local non-governmental organizations (NGO), and high members of the camp community was in place. A 3-day Training of Trainers (ToT) had taken place for the selected number of UNRWA’s health staff, who are directly involved in the campaign across the four fields. Staff were trained on standardized educational material for diabetes care management that was delivered to the patients. They were also trained on standardized methods for the campaign’s weekly activities, logistics, patients’ assessments, reporting, and most importantly counseling skills and presentation skills for conducting the educational sessions. It was then followed by an intensive NCD technical training for UNRWA’s physician done by recruited diabetes specialists across the five fields. The training included advance diabetes care management treatment that was in adherence with UNRWA’s NCD technical instructions. These ToTs carried out a 3-day training on the same materials for their colleagues in their HCs.
HCs conducted a variety of group sessions interactively and excitingly as possible. As such, based on the schedule of every HC, the following three main activities were conducted on a regular basis in every HC: first, the educational session that aimed to improve the knowledge on diabetes management of patients with diabetes, considering: diagnosis, symptoms, risk factors, medication, lifestyle, foot care, early and late complications, and dental care. It was conducted on average of twice a month by the UNRWA’s trained health staff in UNRWA HCs. Second was the cooking sessions which were held once a month. These sessions were with the partnership of community kitchens at UNRWA’s women program centers or vocational schools. It aimed to advocate for healthy cooking practices of the traditional Palestinian recipes. The participants and the medical staff, along with the local partners, have cooked and tasted different Palestinian recipes in a healthier way. The third sessions were focused on exercise and physical activity, and they were conducted in the local NGOs, UNRWA schools and HCs on average of twice a month. UNRWA’s sports teachers and local physical trainers have volunteered in conducting the sessions.
Data collection
Demographics (age, gender, DM category (DMI, DMII or DMII&HTN) and status control), body measurements (height, weight, and WC), blood tests (2-hour postprandial glucose tests (2hrPPGT), total cholesterol), blood pressure (BP) and their attendance for every session were collected first at baseline and then on monthly basis for 6 months. Each participant had a specific code, and all data were collected on a standardized Excel sheet, then consolidated from field offices to the headquarter. Also, questionnaires on knowledge and practice of diabetes care were administrated before and after the campaign (6 months). online supplementary questionnaire is available.
Supplemental material
Data handling and statistical analysis
Data were entered in Excel and then transferred into SPSS V.21.0 for the statistical analysis. Descriptive analysis was done for participant demographics, disease pattern and the knowledge/behavior before and after the campaign. The pre/postcampaign data of weight, WC, body mass index (BMI), weight-to-height ratio (WHtR), PPGT, cholesterol and BP were assessed using the paired t-test. The analysis was performed for the complete sample, as well as for different patient categories; these categories were classified according to WHO guidelines for both BMI and WC.11–13 For example, baseline WC for male was: normal <94 cm, risk (94–102) cm and high risk (≥102) cm and for female was: normal (<80) cm, risk (80–88) cm and high risk (≥88) cm.13 Also, weight change was categorized as follows: weight reduction by ≥5% (or 3%–5%, or 1%–3%), weight increase by ≥5% (or 3%–5%, or 1%–3%) or no change by +1% to −1%.5 13 Baseline BMI was categorized as <30 (non-obese) or ≥30 kg/m2 (obese).11–13 Baseline WHtR,14 as we took the highest category, for males was categorized as >63 or ≤63, WHtR for females as >58 or ≤58. Baseline PPGT was ≤180 mg/dL (normal) or >180 mg/dL (abnormal).15 Total cholesterol baseline levels were classified as <200 mg/dL (normal) or ≥200 (abnormal)16 and BP was considered to be in the hypertensive range ≥140 mm Hg for systolic and ≥90 mm Hg for diastolic.12
Results
Patient demographics
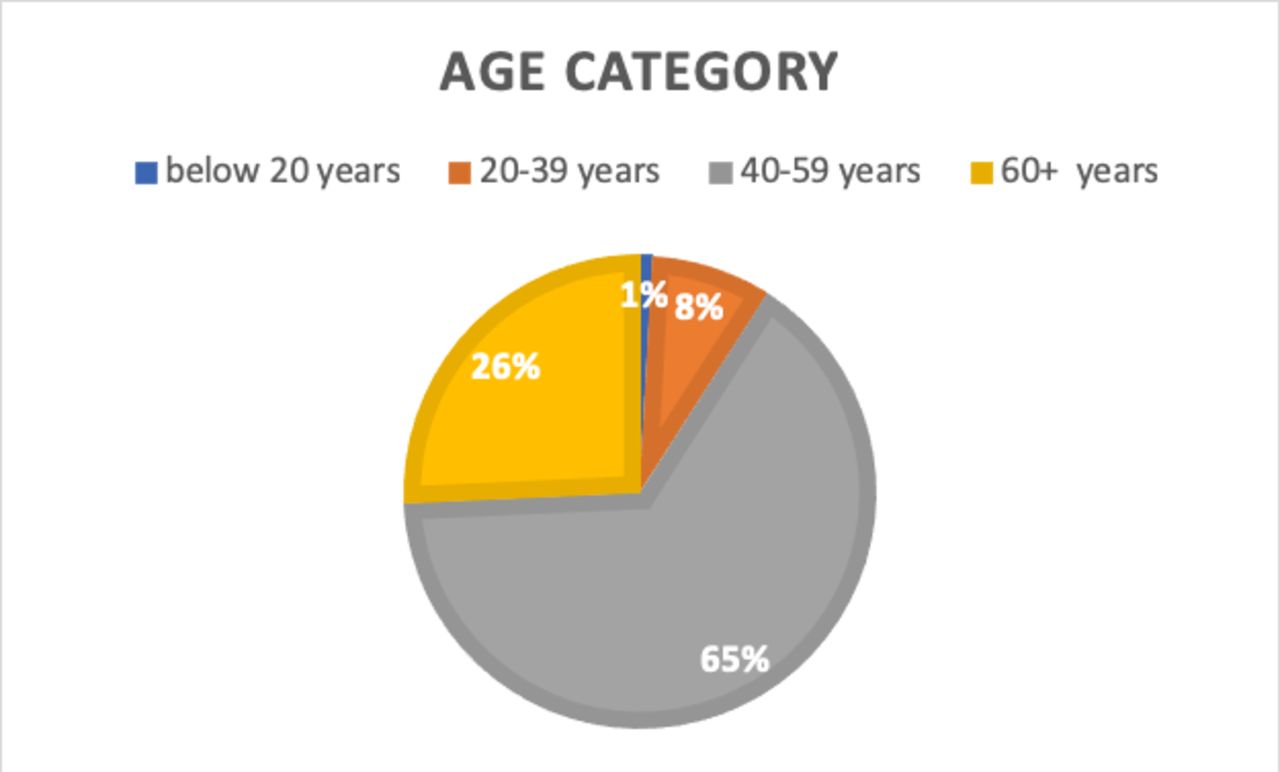
Out of the 1600 initial sample number, 1598 have completed the campaign, the average age was 52.9±10.8 years figure 1, and the percentage of females was 74.0%. Of those 1598 who completed the campaign, there were only 26 who had some missing data.

Age category.
Disease pattern
According to participants who were categorized as DM&HTN status, 62 (4%) of them had DMI, 576 (36.0%) had DMII, and 960 (60.0%) had both conditions of DMII&HTN.
Body measurements
Body weight
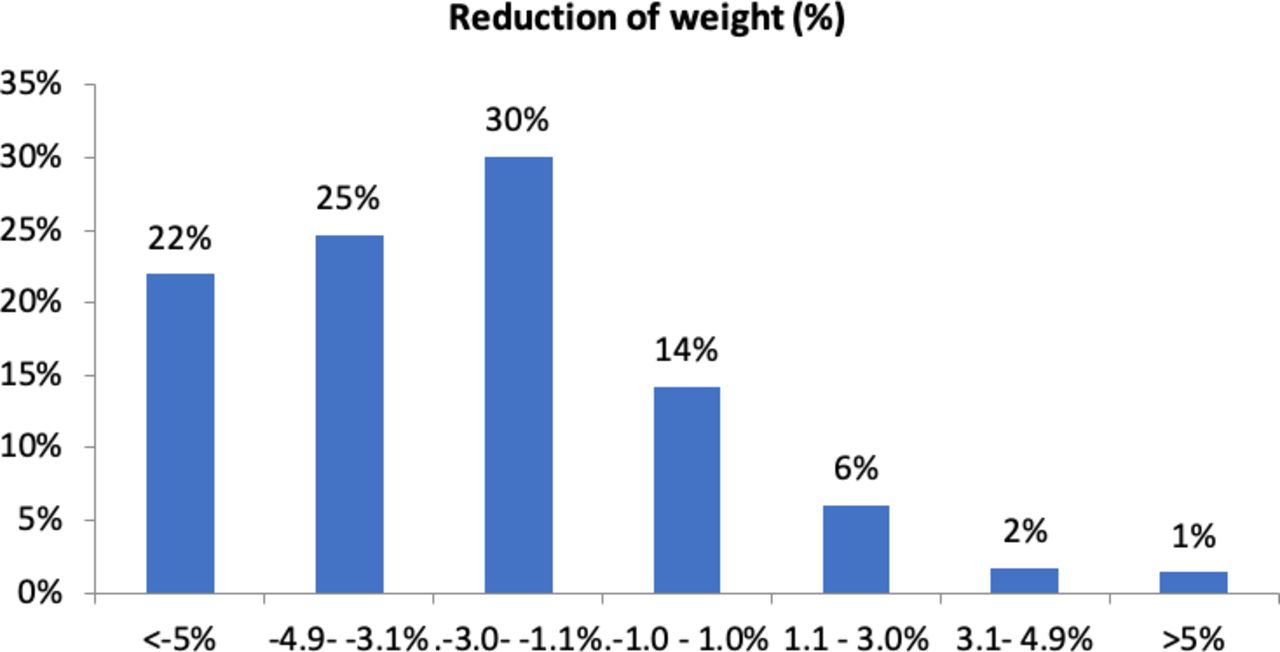
After the 6-month campaign, the average weight loss was −2.6 kg (95% CI 2.4 to 2.7)table 1. Of all 1573 patients who completed the campaign, 345 (22%) lost ≥5%, 388 (25%) lost 3%–5%, and 472 (30%) lost 1%–3% of their weight. However, 223 (14%) had no major change in their weight (−1% to +1%), and more than 114 (9%) had an increase in their weight.figure 2
Changes in body measurements from baseline to the end of the campaign
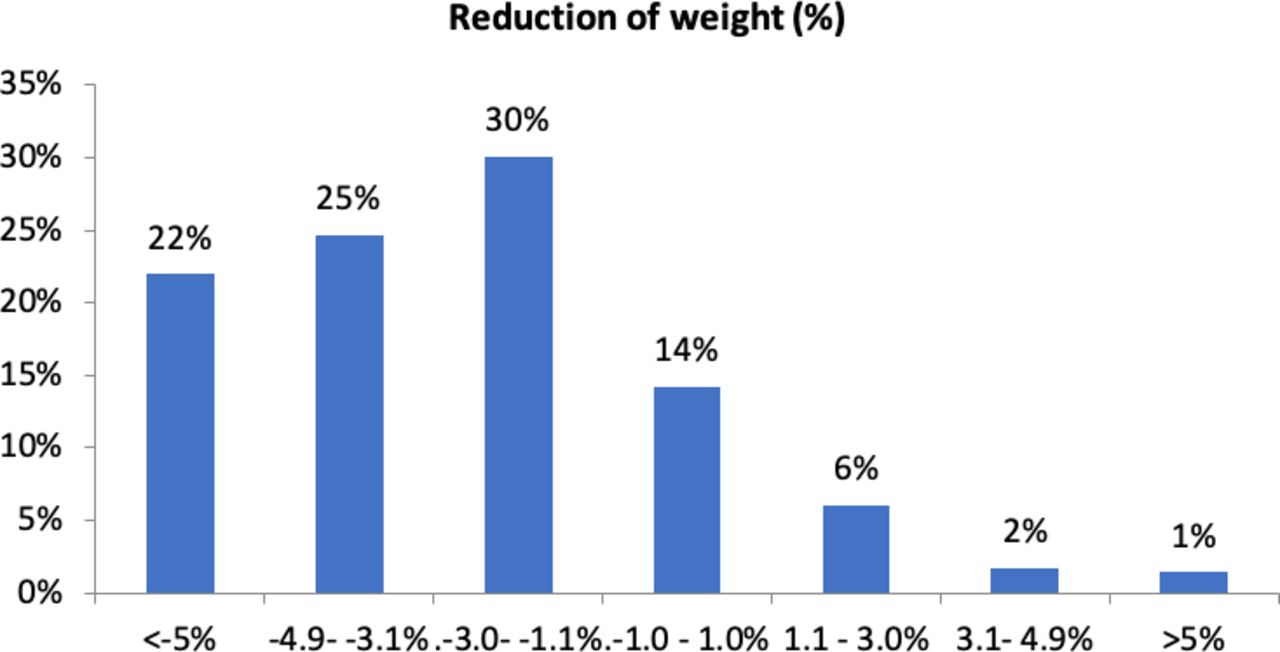
Percentage of weight change after the campaign.
Body mass index
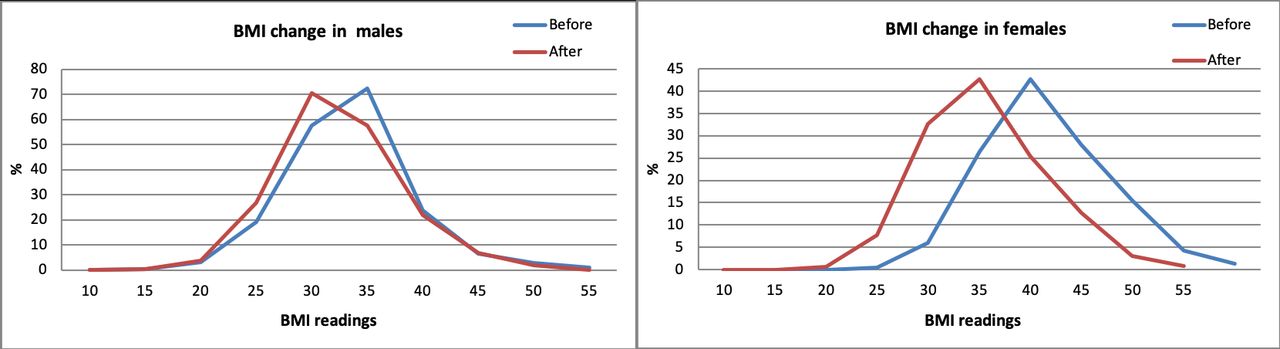
After the 6-month campaign, the total BMI was reduced by 0.78 (95% CI 0.41 to 1.2), a reduction of 0.76 (CI: 0.22–1.3) for females and 0.8 (CL: 0.71–0.94) for males figure 3. A significant change was observed in the BMI category of those who were obese (BMI ≥30) (reduced from 36.4±5.9 to 35.6±11.4), and those who were non-obese (BMI <30) (reduced from 26.7±2.7 to 26.1±2.8).
{kind=link}
{kind=link}
{kind=link}
Percentage of change in all body mass index (BMI) categories before and after the campaign for both genders.
Waist circumference
From the 1574 participants with full WC data, it was shown that WC significantly reduced from 108.7±14.1 to 104±13.3. table 2, describs the high-risk WC for both gender.
High-risk waist circumference before and after the campaign in both genders
Biomarkers before and after the campaign
Of all participants who have completed the campaign, a total of 1574 had completed their PPGT, cholesterol and BP readings table 3. A significant reduction (p<0.005) was detected for those who were above the normal cut-off of point PPGT >180, cholesterol >200 and BP (systolic/diastolic) ≥140/90 mm Hg.
High-risk PPGT, cholesterol, and BP before and after the campaign
Patients’ behavior and knowledge before and after the campaign
We have observed improvements in the knowledge and lifestyle practices among the 1598 patients. Such developments were seen in the participants’ cooking practices. For example, the practice of adding oil during cooking was reduced, and more participants have stated that they are using a measuring spoon for adding oil, for minimizing the amount of oil used during cooking. The percentages of participants having late night dinner (after 20:00) have decreased from 831 (52%) before the campaign to 165 (10%) after the campaign. We have observed an increase in the number of participants having the small and frequent healthy meals (three meals and two snacks) instead of the large fatty meals from 4% (69 patients) to 18% (277 patients). Also, the number of participants walking for 30 min/three times a week has increased from 779 (49%) to 1229 (78%). We are noting that the above practices were highly advocated during the campaign sessions.
Patients’ attendance during the campaign
The percentage of attendance was 75.0% for education, 62.7% for cooking, and 73.5% for exercise sessions. These percentages are considered reasonably high, especially given the poor camp settings, infrastructure, and facilities provided for the campaign activities.
Discussion
Globally, there have been many efforts to promote healthy lifestyle changes for patients with diabetes, with investment in modifiable factors, including diet, physical activity, and weight.17 Many studies indicated that patients with diabetes do not manage their disease on their own, even after receiving education about diabetes care. However, receiving diabetes education group-based intervention results in improvements in clinical, lifestyle and psychosocial outcomes.18–20 Other studies have shown that group-based training on self-management strategies for people with DMII is similarly effective.21
We believe that the diabetes campaign ‘Life is Sweeter with Less Sugar,’ which UNRWA has conducted by using a variety of clinical and behavioral interventions, was an effective tool in improving the clinical outcomes of patients with diabetes.
Patients’ adherence and attendance level were considerably high, given the fact that they live in impoverished refugee camp setting; as they struggle with poor health, exacerbated by substandard housing, inadequate supplies of healthy food, and poor infrastructure for outdoor activities.22 Some explanationson the level of commitment that was observed could be due to the type and diversity of the campaign activities and the positive experience coming from the group support. This patient adherence is unique compared with similar interventions, where the adherence is usually suboptimal.23 We think that many positive outcomes were related to the social gathering during the education, exercise and cooking sessions. Such results were seen in studies with evidence-based trends for achieving weight loss and increased physical activity an application for diabetes prevention and treatment, which indicated that group classes and campaigns focusing on a variety of nutrition, behavior, and exercise topics were also offered to help sustain adherence and motivation.24
However, sustaining such positive outcomes of these interventions is a challenge, especially with the shortage of funding that UNRWA usually faces.25 From that perspective, the UNRWA’s health department has been working on the NCD way forward for integrating such intervention within its primary healthcare program.
Weight loss with diet and exercise regimens has been shown to improve glycemic control effectively. Importantly, it has been demonstrated that in patients with DMII even a modest sustainable reduction of the initial body weight (5%–10%) can reduce diabetes-related complications by improving glycemic control, lipid profiles and BP.26 From UNRWA’s DM campaign weight loss results, it was found that 22% of patients have reduced ≥5%, 25% have lost 3%–5%, and 30% have reduced 1%–3% of their weight, with an average of a 2.6 kg decrease in weight. However, this amount of weight loss is not enough for an obese patient with diabetes.5 11 15 Moreover, maintaining weight reduction after completing the campaign can come with a struggle. To prevent weight regain after the campaign, UNRWA had put a sustainable follow-up plan for the participants after the campaign.27
WC is an independent risk factor for DMII.28 It is one of the best anthropometric predictors of abdominal fat. A WC higher than 102 cm for males and ≥88 cm for females is considered to be a risk factor for DM, cardiovascular diseases and other chronic diseases.28 29 Therefore, we chose to measure the changes in WC before and after the campaign, which had a significant decrease of −4 cm.
2hrPPG shows how tolerant the body is to glucose; therefore, it is a one-time level of blood glucose only. UNRWA used the 2hrPPG results for diabetes monitoring and control during the campaign time. Back then, according to UNRWA’s technical instructions, diabetes control is achieved when 2hrPPG becomes equal or less than 180 mg/dL (≤10.0 mmol/L). Therefore, 2hrPPG was used as a blood glucose monitoring tool during the campaign. It has shown a significant reduction after the campaign. However, patients can impact results by not eating 2 hours before the test, heavy exercise, or having a meal or a snack right before the test.30 During UNRWA’s clinical audit, it was shown that when using the HbA1c tests, patients with DM had lower results compared with that measured using 2hrPPG (28% vs 45%). Thus, estimating diabetes control through 2hrPPG may be misleading as it overestimates control rates.7 Despite the financial constraints that UNRWA was and is facing, UNRWA has developed a stepwise implementation plan for the introduction of modern technologies (HbA1c) for patients who need and would benefit from it the most.2 (
Although there were missing data from a few sessions, the overall completion rate was high. We believe that the interactive campaign activities that were tailored to the refugee camp settings and patient’s Palestinian heritage had an impact on the high participation rates. For instance, the cooking and exercise sessions were very tailored to the tradition and culture of the Palestinian refugees, especially the elder ones.
Resources are limited within a humanitarian agency such as UNRWA, so it is difficult to provide multiple weight management programs for a specific subpopulation of patients with various disease conditions, especially when such patients are scattered across a wide geographic radius. Yet, the results of such a campaign indicate that using an existing NCD care program embedded in UNRWA primary HCs is a feasible way to implement combined diabetes care management and weight loss. The adaptation of a variety of group sessions, such as cooking, education and exercise sessions, with local NGOs and community partnership has shown a positive impact on reducing weight, WC, 2hrPPGT, cholesterol and BP.
Limitations
This campaign had more standardized methods and procedures compared with the first campaign conducted in 2013. However, there are some limitations to this campaign, which some were out of our control and others we will be addressing in future awareness campaigns:
There were missing data from a few sessions. However, the percentage of missing data is minimal, and we do not believe that these data will be significantly different from the rest of the cohort. Reasons reported for missing data from the health staff are: some patients could not attend a few sessions due to their family engagements, or they could not find suitable transportation from outside camps.
Similar to the first campaign, the number of females was higher than males, 74.2% female and 25.8% male. This might be because most males were at work during the time the sessions were conducted. Therefore, the future campaign should incorporate more male participation.
This study is quasiexperimental, therefore it is subject to validity issues due to lack of control group and randomization, but it is not feasible or ethical for a UN agency such as UNRWA to conduct a randomized controlled study on their beneficiaries.
Conclusion and recommendations
We have conducted a diabetes campaign for Palestine refugees with diabetes attending UNRWA HCs that focused on improving the level of awareness about diabetes care management and healthy lifestyle behaviors among Palestine refugees with DM, by using a variety of educational sessions. This campaign had a positive impact on body measurements and blood glucose in Palestine refugees with DM. Thus, use of existing NCD care resources in UNRWA HCs to deliver the principles of effective behavior change in the areas of weight loss, healthy eating, physical activity, DM status control and prevention of the disease deterioration could be more efficient in the areas of time, cost, and counseling.
In order to sustain the impact of this campaign, diabetes education and awareness about healthy lifestyle should be systematically integrated into the UNRWA NCD program. They could also help sustaining and empowering the local community involvement and NGO partnerships. Further follow-up studies (ie, cohort study or longitudinal) should be done to evaluate the long term effect of participants’ DM status control and weight maintenance.
Acknowledgments
Acknowledgement goes to all UNRWA health staff who participated in the DM campaign in the headquarter and across the four fields of operation (Jordan, Lebanon, West Bank and Gaza strip), also to the NGOs and local communities in the four fields.
References
Footnotes
Contributors NAK designed the study, collected and interpreted the data, carried out the data management, and wrote the article. YS designed the study, interpreted the data and revised the article. JM was responsible for critical editing of the text. YT interpreted the data and revised the article. WZ analyzed the data and produced the tables and figures. AS supervised the study and the data.
Funding This work was supported by the World Diabetes Foundation.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.