Article Text

Abstract
Objectives We postulate that performance feedback is a prerequisite to ensure sustained improvement in diabetic ketoacidosis (DKA) management.
Design The study was based on ‘theory of change’ concept that suggests changes of primary drivers determine the main outcome. A set of secondary drivers can be implemented to achieve improvements in these primary drivers and thus the main outcome.
Setting This study was conducted at a large tertiary care center in the West Midlands, UK. The region has above average prevalence of diabetes and DKA admissions in the country.
Participants All participants diagnosed with DKA as per national guidelines, except those managed in intensive care unit from April 2014 to March 2018, were included in this study.
Interventions Monthly feedback of performance was the main intervention. Development of a real-time live DKA audit tool, automatic referral system of DKA to the specialist team, electronic monitoring of blood gas measurements and education and redesigning of local (trust) guidelines were the other interventions in this study.
Main outcome measures Total DKA duration, appropriateness of fixed rate intravenous insulin infusion, fluid prescription, glucose monitoring, ketone monitoring and referral to specialists.
Results There was a significant reduction in the duration of DKA postintervention compared with baseline results. However, in the absence of regular feedback, the duration of DKA showed an upward trend nearing baseline values. Similar trends were noted in secondary drivers influencing DKA duration.
Conclusion Based on these results, we recommend regular audit and feedback is required to sustain improvements in DKA management.
- Endocrinology/Diabetology
- Insulin-Deficient Type 1 Diabetes
- Ketoacidosis
- Quality Improvement Measures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Though diabetic ketoacidosis (DKA) audits have resulted in a transitory improvement in its management, continuous and ongoing improvement has been difficult to establish.
What are the new findings?
We were able to reduce DKA duration with tailored interventions and sustain the improvement with regular feedback. The trend of DKA duration headed toward baseline in the absence of regular feedback.
How might these results change the clinical practice?
Incorporating regular feedback to end users may help provide better care to patients with DKA.
Problem
Diabetic ketoacidosis (DKA) is an acute endocrine emergency requiring rapid assessment and treatment.1 The Joint British Diabetes Societies produced guidance standardizing DKA management for inpatients in 2010 and subsequently revised them in 2013.2 These guidelines served as the standard for several audits conducted at our institution. Though these audits may have resulted in a transitory improvement in DKA management, continuous and ongoing improvement in DKA management was difficult to establish. Ivers et al3 reported that feedback of audit generally induces small improvement in clinical practice, but a professional behavioral change is best brought about by the combination of continuous education, feedback and auditing.4–7 We previously reported that our interventions using the plan–do–study–act cycle reduced the mean duration of DKA from 22.0 to 10.2 hours.8 9 We hypothesize that performance feedback is required to ensure sustained improvement in DKA management and that loss of this feedback would lead to a longer duration of DKA.
Background
DKA is characterized by the triad of hyperglycemia (blood glucose >11 mmol/L), acidosis (pH <7.3 or bicarbonate <15 mmol/L) and ketogenesis (serum ketones>3 mmol/L).2 10 11 Although mediated primarily by insulin deficiency (relative or absolute), it can be precipitated by systemic disease, non-compliance with treatment, or previously undiagnosed disease.11 The prevalence of DKA varies with regions: 50–100 per 1000 in the USA,12–14 103–128 per 1000 in Canada15 16 and 39 per 1000 in patients with type 1 diabetes in Germany and Austria.17 In their recent study, Fazeli Farsani et al18 have summarized the incidence and prevalence of DKA in various regions of the world.
While prevalence rates of DKA in the UK are currently unavailable, incidence data of DKA in the UK has improved from 51.3 per 1000 person-years to 8 per 1000 person-years.19 20 It should be noted these are single-center reports based on patient medical records. In 2019, an estimated 9.5% of the population in the West Midlands had diabetes, compared with the rest of the UK population (8.7%).21 General practice data from 2016/2017 revealed that Birmingham has an high prevalence rate of diabetes mellitus.22 We currently have over 100 000 emergency admissions a year, of which 20.89% have diabetes.23
About 10% of people with diabetes have type 1 diabetes.24 A proportion of this population (45.9% in 2015) were admitted to a hospital with DKA. More alarmingly, there is an unchanging incidence (about 4%) of patients with type 1 diabetes inpatients that developed DKA during their hospital stay.24 This underlines the need to identify key drivers to enhance DKA management.
Measurement, design and strategy
This study was conducted at the Queen Elizabeth Hospital Birmingham, part of the University Hospitals Birmingham National Health Service (NHS) Foundation Trust. As one of the busiest NHS organizations, it saw more than 135 000 inpatient episodes and over 115 000 emergency department attendances (~315 patients, daily) over the course of 2016/2017.25
All patients diagnosed with DKA as per national guidelines from April 2014 to September 2018 were included in this study. Those patients managed in intensive care unit were excluded to avoid bias resulting from personalized and one-to-one care. Results showing improvement in DKA duration up to September 2016 following certain interventions have been previously reported.8 9 We have further divided the entire study into six distinctive time periods (figure 1). The study was based on the ‘theory of change’ concept that suggests the changes of primary drivers determine the main outcome.26–29 A set of secondary drivers were implemented to achieve improvements in these primary drivers and thus the main outcome. Therefore, the measurement of the primary drivers in their own entity is an overall measurement of the principal outcome.

Six distinctive time periods of the study.
Results from the initial retrospective audit from April 2014 to September 2014 were presented to frontline staff involved primarily in the initiation of DKA management (emergency, acute and diabetes teams). From the ensuing discussion, the main outcome of a reduction in DKA duration by 50% within the first 12 hours of the diagnosis of DKA was established. The process of choosing primary and secondary drivers is graphically described in figure 2. As previously described,9 the primary outcome was tested by five main interventions (secondary drivers) through the plan–do–study–act (PDSA) method:
Development of a real-time live audit tool:. This intervention led to the generation of a real-time audit tool that shortens the delay between data collection and propagation of the analyzed results. We used the existing Prescribing Information and Communications System (PICS) to capture observations, prescribing and referral requests. This system has enabled the timely monitoring of glucose and ketone measurements, prescription of fluids and insulin, and specialist referrals.
An automatic referral system to the specialist team: The prescription of a fixed rate intravenous insulin infusion (FRIII) on PICS triggers an automated referral to the diabetes team.
Electronic monitoring of blood gas measurements:. Before this intervention, point-of-care blood gas analyzer results were not part of our electronic observation system. Since the incorporation of these results onto PICS, it has allowed for electronic and remote monitoring of pH, blood glucose and ketone measurements accurately.
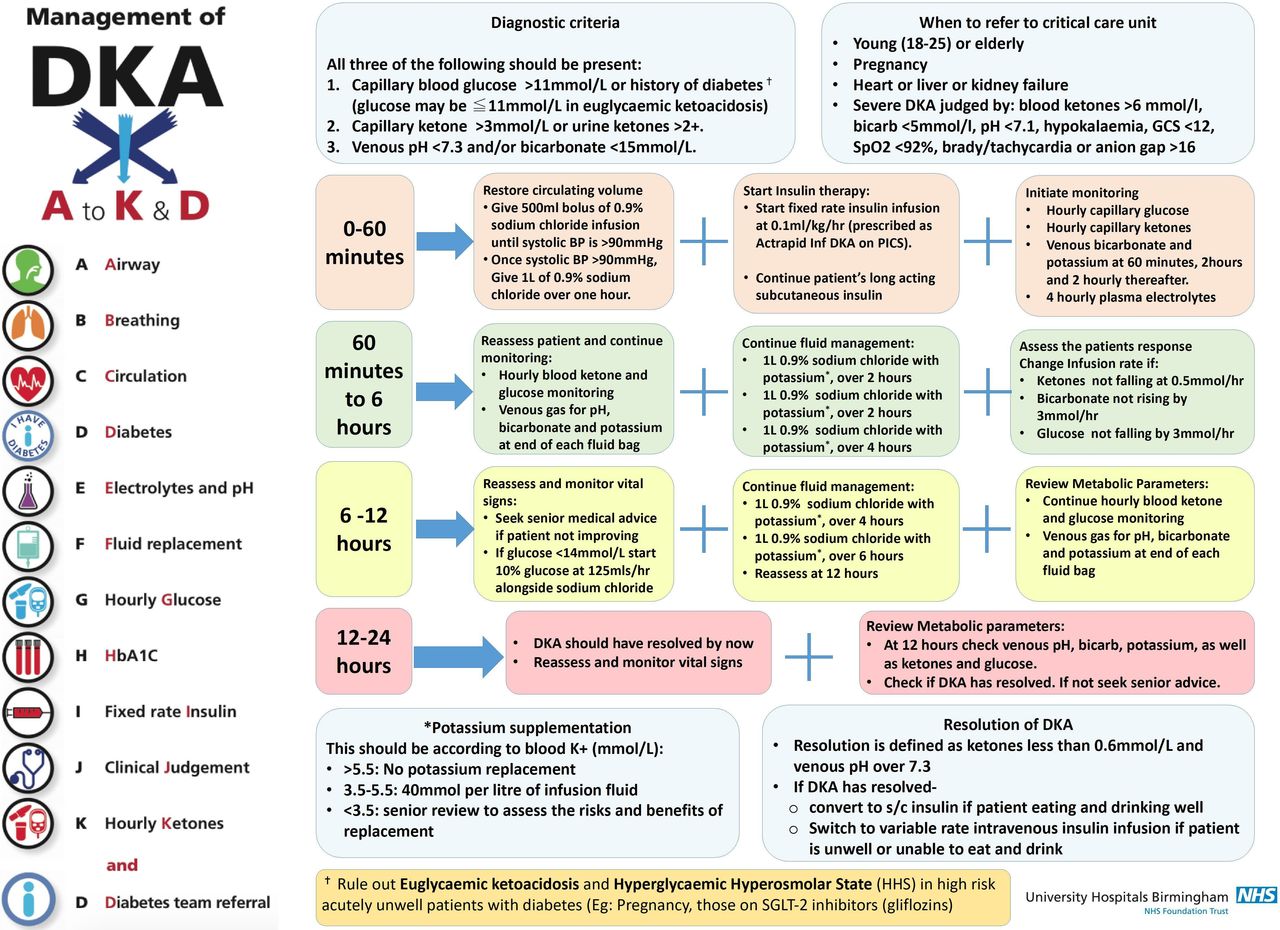
Education and redesigning of local (trust) guidelines. A simplified ‘A to K & D’ DKA trust guideline was designed and made accessible through the intranet and as posters in the emergency and acute medicine floors.
Monthly feedback: Monthly audits of the primary drivers were presented to the frontline teams.

Several factors underlie the primary drivers that overall influenced the main outcome of DKA duration. The lower half of the figure describes the timeline of various interventions (secondary drivers) during the QIP. DKA, diabetic ketoacidosis. ED, emergency department; CDU, clinical decision unit; QIP, quality improvement project.
Interlink between the primary and secondary drivers with the main outcome of DKA duration is represented in figure 3. The newly improved one-page DKA protocol with mnemonic introduced as part of this study is represented in figure 4. The performance of the key drivers that influence DKA duration (appropriateness of FRIII, fluid prescription, glucose monitoring, ketone monitoring and referral to specialists) were presented to our liaison consultants in the frontline team who then cascaded the results to the rest of their team. The frontline team in our hospital consists of members of the emergency medical team and the acute medical team. In our DKA pathway, patients would be first assessed in the emergency department where the diagnosis of DKA would be confirmed and treatment initiated. Once stabilized, the patient would subsequently be transferred to our acute medical unit where they would be managed until DKA resolution. One of the authors regularly met the liaison consultants in person during this process to ensure a two-way communication so that factors that influenced that month’s results could be learnt and required interventions were initiated in the following months to improve the performance of key drivers. Such feedback continued until September 2016. We then studied the effect of not having the monthly feedback to the frontline teams from October 2016 to March 2018.

Five (numbered) primary and secondary (yellow) divers. (1) Fluid replacement is the most vital initial management step. Guidelines recommend at least 4 L of fluid replacement within the first 12 hours (1000 mL in the first hour, 2000 mL over the next 4 hours and 8 hours, respectively). (2) Fixed rate intravenous insulin infusion (FRIII) will switch lipolysis off, thereby disinitiating the metabolic acidosis induced by DKA. It is recommended that 0.1 units/kg body weight of FRIII be used. (3) Initiation of FRIII will cause the glucose to fall sharply, and as such, hourly glucose measurement is mandatory. Further glucose infusions may be required in the latter stages of DKA management to avoid hypoglycemia until ketogenesis is switched off. (4) The recommendation is for hourly ketone measurement and aiming for insulin titration to reduce blood ketones by 0.5 mmol/L/hour. (5) Patients with DKA should be referred to the specialist diabetic team on admission or early specialist input. Secondary interventions in our QIP included: (A) the development of a real-time audit tool; (B) automatic referral system; (C) electronic blood gas monitoring; (D) monthly feedback; and (E) education and redesigning of local guidelines. DKA, diabetic ketoacidosis.

The revised one-page DKA protocol with easy to remember mnemonic introduced as part of the intervention in the QIP. DKA, diabetic ketoacidosis.
Results
A total of 432 DKA episodes were included in the study. table 1 describes the baseline characteristics of the study population throughout each year of the study with the breakdown of DKA admissions contributing to the study. There were a significantly lower number of DKA admissions in the follow-up period despite no change in the eligibility criteria of enrolling DKA admissions to the study. figure 5 reports our primary outcome measure that was the duration of time patients were in DKA. When continuous feedback was in place, there was a significant reduction in the duration of DKA postintervention (p<0.001). However, in the absence of regular feedback from September 2016 onward, the duration of DKA showed an upward trend. Yet, the median DKA duration in the post follow-up period remained significantly lower compared with the preintervention period. Further details of the median values of change are described in table 1.
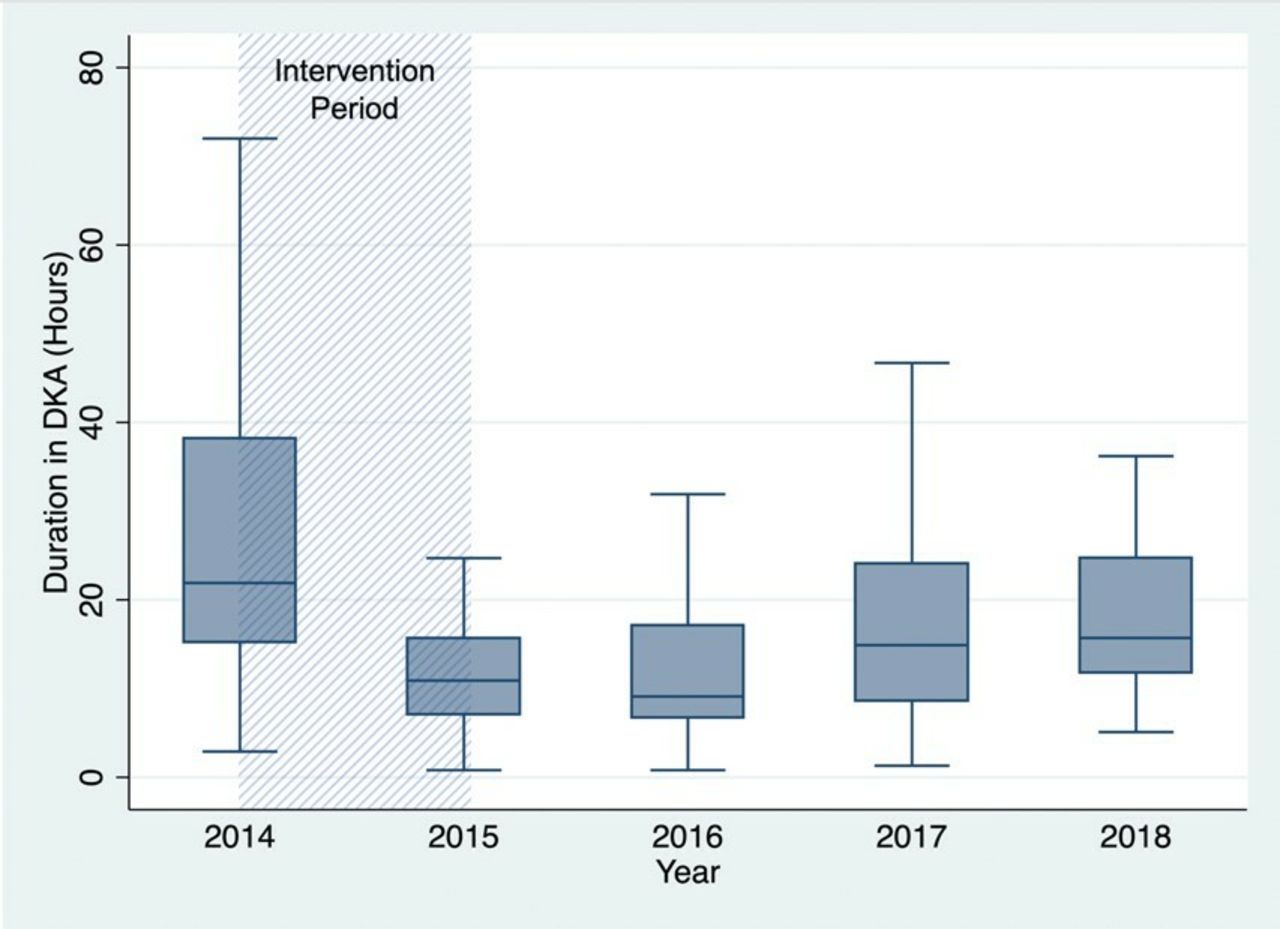
Duration of DKA per year. DKA, diabetic ketoacidosis.
Changes to various parameters during our quality improvement program
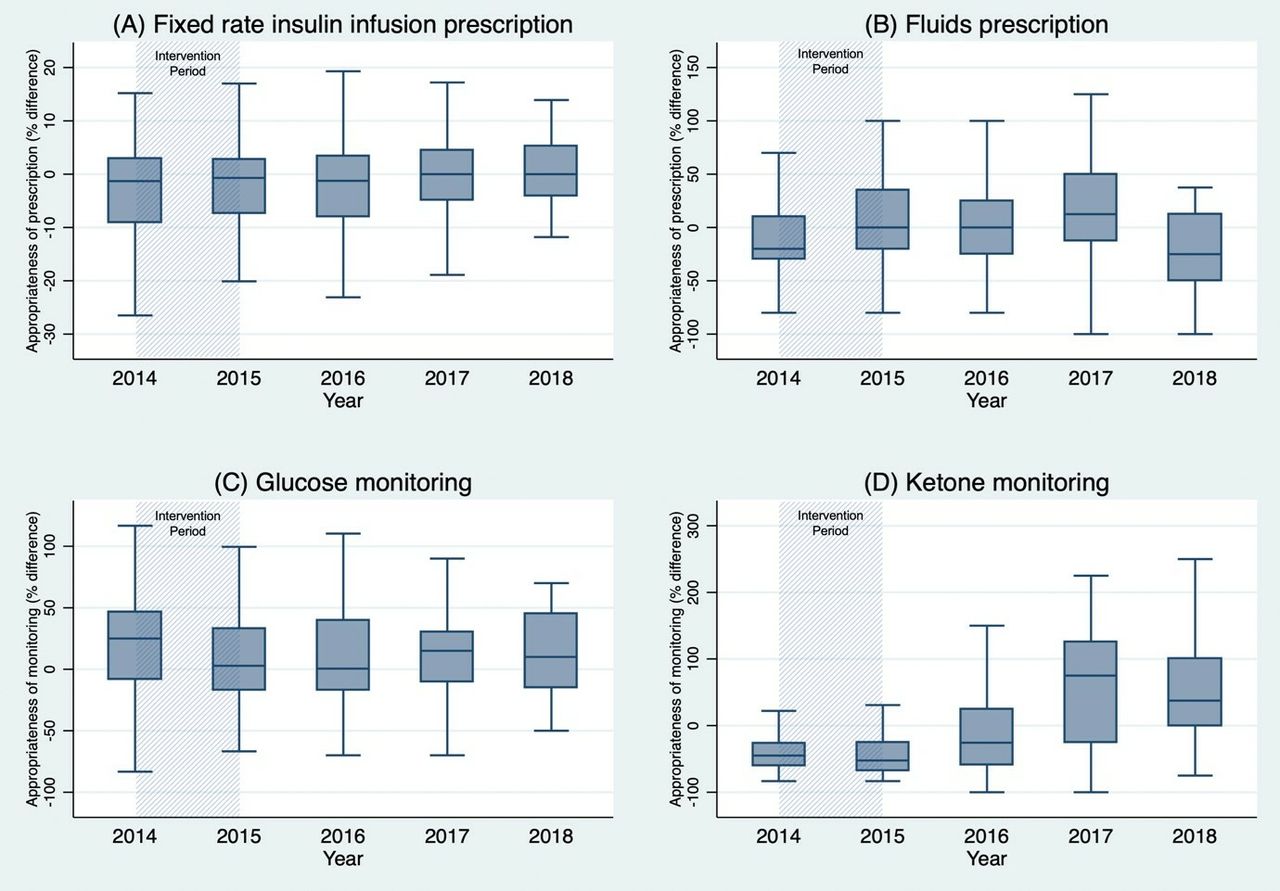
Appropriateness of FRIII, fluid prescription, glucose monitoring and ketone monitoring is described in figure 6. Following our interventions, we successfully reduced the dispersion values for FRIII—up to 92% of the values were within 20% of the guideline value. The effect persisted in the post follow-up periods; the values became less dispersed and showed a continually improving prescribing practice. The proportion of patients receiving recommended fluids improved in the period of regular feedback. However, this became more variable during the post follow-up period. While the dispersion of glucose measurement frequency improved with regular feedback, the trend towards increased monitoring was noted after feedback was stopped. A significant increase in ketone monitoring was noted in the latter periods of the study. Although there was more appropriate ketone testing following our interventions, the trend diverted toward the opposite axis indicating an unnecessary use of resources.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Appropriateness of fixed rate intravenous insulin infusion prescription, fluid prescription, glucose monitoring and ketone monitoring. It represents the dispersion of each measure from the baseline recommendation. For example, the standard recommendation for FRIII rate for a patient weighing 60 kg is 6 units/hour (0.1 unit × weight of the patient). A prescription of 6 units/hour would register at ‘0’ on the y-axis, whereas a prescription of 3 and 9 units for the same patient would register at −50% and 50%, respectively.
Lessons and limitations
In this study, we demonstrate a significant and sustained reduction in DKA attributable to the ‘theory of change’ model of quality improvement. Furthermore, the absence of regular performance feedback (secondary drivers) in the post follow-up period was associated with a greater degree of deviation from treatment guidelines and longer DKA duration. Although we cannot conclude with certainty that the lack of feedback was the sole reason for worsening DKA duration, we observed a strong relationship between regular feedback and DKA duration. Conversely, we also recognized that withdrawal of the regular feedback mechanism, even if not strictly causal, has resulted in an increase in DKA duration.
Improvements need to continue to ensure the best quality of care and patient safety within the NHS. While simple audits have been useful in assessing adherence to guidelines,30 they have their limitations. A recent review of assessing the impact of healthcare interventions using routine data by Clarke et al31 outlines these points. We demonstrate the utility of the PDSA model to improve clinical care in DKA management. We have gone further and demonstrated that key to the sustainability of improved outcomes relies on regular feedback. Ideally, we would have collected data using more prospective methodology. However, lack of resources restricted the span of our data collection. Nevertheless, the deterioration in DKA duration with concomitant lack of feedback mechanism is noticeable and statistically significant.
Duration of DKA is multifactorial and relates to the underlying cause of DKA, timely diagnosis, quick and appropriate treatment and monitoring. This is in turn dependent on the knowledge of nursing and medical staff and approach of the diabetes specialist team. We initially tried to measure the baseline knowledge, attitude and practices for DKA among frontline staff in the emergency department and acute medical unit. However, we found it challenging to update the constantly changing junior doctors in training rotations. Furthermore, we also noted a higher turnover of nursing and allied medical health staff in these departments compared with the rest of the hospital. Following this, we established a liaison consultant in these departments through whom we disseminated the results of performance indicators for DKA and suggested necessary improvements that were to be delivered at the department level. We aim to capture such interventions in our future updated study.
While the DKA duration is important, complications such as hypokalemia and hypoglycemia resulting from the management of DKA could be life threatening.32–35 The initial hyperglycemia and metabolic acidosis result in a relatively higher serum osmolarity, which then induces osmotic diuresis and renal electrolyte loss, potassium being the most significant. Vomiting, a commonly associated symptom in DKA, results in further potassium loss.36 With treatment initiation and insulin infusion, there is a shift of potassium from serum into cells further exaggerating the hypokalemia. Several cases of profound hypokalemia leading to cardiac dysrhythmias have been reported in the past.37–39 Hypoglycemia is the most frequent complication with DKA treatment arising secondary to the discrepancy between the availability of glucose to insulin that that needs to switch off lipolysis.32 Lately, there is an increased frequency of euglycemic ketoacidosis associated with sodium-glucose cotransporter-2 (SGLT2) inhibitors. Such patients with SGLT2 inhibitor associated euglycaemic ketoacidosis are more susceptible to hypoglycemia with DKA treatment further to a complex drug-associated mechanism.40 However, there is limited literature studying the prevalence and associated risk factors of hypoglycemia resulting from DKA treatment.
Regrettably, we did not measure these complications in this study. Therefore, we cannot ascertain if our intervention made any difference to these complication rates. Moreover, we were not able to assess if a shorter duration of DKA influences readmission rates. We are currently in the process of updating our DKA monitoring system to include monitoring for hypokalemia and hypoglycemia alongside the time of administration of basal insulin during each episode. Frequencies of recurrent DKA admission and its causal factors have been proposed as further parameters that warrant monitoring. We excluded patients who were managed in intensive care as the benefit of continuous monitoring and one-to-one nursing could impact patients’ management. Further research is needed to study the specifics (impact of timing, dose and administration of long-acting insulin) on DKA duration and the global management of DKA.
Conclusion
In this study, we demonstrated that regular audit and feedback is required to sustain improvements in DKA management. We hope to implement further audit cycles into our service development to continue data collection and reduce DKA duration. Further studies are needed to assess the reproducibility and validity of these findings in larger and diverse settings.
Acknowledgments
We thank the University of Birmingham for their support towards publishing this article. We also thank the staff and patients of the Queen Elizabeth Hospital Birmingham for their contributions during the study. Finally, we thank the helath informatics team for helping with data collection for the study.
References
Footnotes
Contributors PK conceptualized the study, collected and analyzed the data. JSC, BC, ADB and NJ collected and analysed the data. SJ analyzed the data and wrote the first draft. SG and PN supervised the overall project. All authors provided inputs toward writing up the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.