Article Text

Abstract
Objective Type 2 diabetes care management (DCM) is challenging. Few studies report meaningful improvements in clinical care settings, warranting DCM redesign. We developed a Boot Camp to provide timely, patient-centered, technology-enabled DCM. Impact on hemoglobin A1c (HbA1c), emergency department (ED) visits and hospitalizations among adults with uncontrolled type 2 diabetes were examined.
Research design and methods The intervention was designed using the Practical Robust Implementation and Sustainability Model to embed elements of the chronic care model. Adults with HbA1c>9% (75 mmol/mol) enrolled between November 2014 and November 2017 received diabetes education and medication management by diabetes educators and nurse practitioners via initial clinic and subsequent weekly virtual visits, facilitated by near-real-time blood glucose transmission for 90 days. HbA1c and risk for ED visits and hospitalizations at 90 days, and potential savings from reducing avoidable medical utilizations were examined. Boot Camp completers were compared with concurrent, propensity-matched chart controls receiving usual DCM in primary care practices.
Results A cohort of 366 Boot Camp participants plus 366 controls was analyzed. Participants were 79% African-American, 63% female and 59% Medicare-insured or Medicaid-insured and mean age 56 years. Baseline mean HbA1c for cases and controls was 11.2% (99 mmol/mol) and 11.3% (100 mmol/mol), respectively. At 90 days, HbA1c was 8.1% (65 mmol/mol) and 9.9% (85 mmol/mol), p<0.001, respectively. Risk for 90-day all-cause hospitalizations decreased 77% for participants and increased 58% for controls, p=0.036. Mean potential for monetization of US$3086 annually per participant for averted hospitalizations were calculated.
Conclusions Redesigning diabetes care management using a pragmatic technology-enabled approach supported translation of evidence-based best practices across a mixed-payer regional healthcare system. Diabetes educators successfully participated in medication initiation and titration. Improvement in glycemic control, reduction in hospitalizations and potential for monetization was demonstrated in a high-risk cohort of adults with uncontrolled type 2 diabetes.
Trial registration number NCT02925312.
- delivery of care
- education and behavioral interventions
- treatment algorithms
- outcome research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Strategies are needed to translate evidence-based diabetes medication management and self-care management education and support practices into optimized diabetes care management and outcomes among adults with uncontrolled type 2 diabetes.
What are the new findings?
This pragmatic technology-enabled Boot Camp intervention demonstrated improvement, among predominantly African-American participants, in glycemic control and reduction in hospitalizations when compared with concurrent propensity-matched chart control patients receiving usual primary care for diabetes.
To support translation of evidence from randomized controlled trials to effective clinical diabetes care management, this research deployed chronic care and implementation science models to implement a pragmatic Boot Camp for uncontrolled type 2 diabetes in alignment with organization, provider and patient factors in a regional mixed-payer health system.
How might these results change the focus of research or clinical practice?
In collaboration with primary care, a focused, intensive diabetes care management strategy delivered by diabetes educators and using near real-time blood glucose monitoring to inform virtual visits can potentially promote access for high-risk adults with diabetes to self-care education and safe and effective titration of the diabetes medication regimen.
Introduction
Uncontrolled type 2 diabetes burdens patients, providers and healthcare systems.1 Glycemic control reduces type 2 diabetes complications.2–7 National guidelines provide evidence-based recommendations, including from randomized controlled trials (RCTs), for diabetes care management (DCM), which incorporate treatment with antihyperglycemic medications.8 9 Diabetes self-management education and support (DSMES) improves outcomes,10–13 but only 5% of Medicare beneficiaries with diabetes and <7% of persons with private insurance receive DSMES within the first year of diagnosis.14 15 Overall, glycemic control remains challenging, with 15.6% of US adults with type 2 diabetes having a hemoglobin A1c (HbA1c) >9% (75 mmol/mol).16
Most type 2 DCM is delivered in primary care settings,17 with referrals for DSMES and endocrine consultation as needed. Numerous patient, provider and system variables affect DCM and may contribute to suboptimal outcomes,18 including clinical inertia in advancing antihyperglycemic medications19 and insufficient DSMES.10 14 15 Research has also shown this care should be individualized.18 Redesigned approaches are needed to overcome barriers to DCM and to support primary care providers (PCPs) and persons living with diabetes in improving glycemic control and diabetes outcomes.
In response to this need, and building on our previous research,20 21 we designed and implemented a pragmatic evidence-based DCM intervention—the Diabetes Boot Camp—for patients being managed in primary care settings. We define the Diabetes Boot Camp as a focused and intensive intervention that provides patient-centered diabetes clinical management and education in knowledge and skills for self-care. The Boot Camp leverages technology and an extended care team to support optimizing glycemic control for uncontrolled type 2 diabetes. Here, we describe the development and implementation of the Diabetes Boot Camp and its impact on primary glycemic (HbA1c reduction) and secondary effectiveness outcomes.
Research design and methods
We conducted a pragmatic, prospective cohort study to examine the impact of the Diabetes Boot Camp in a US regional mixed-payer distributed care delivery health system with 10 hospitals and 250 ambulatory care access points in the Northeastern USA. We employed a pragmatic rather than an explanatory experimental approach to evaluate the implementation effectiveness of the Boot Camp intervention because this approach more accurately reflects real-world practice.
Participants
Adults with suboptimally controlled type 2 diabetes receiving care in 35 ambulatory practice sites in Maryland and the District of Columbia were invited to participate in the Boot Camp. Participants were aged >21 years with type 2 diabetes and HbA1c>9% (75 mmol/mol) and one or more visits to a system provider in the year prior to study entry. Exclusion criteria included documented history of diabetic ketoacidosis, advanced comorbidities predisposing to emergency department (ED) visits and hospitalizations unrelated to glycemic control (eg, severe active mental illness or advanced congestive heart failure), end-stage renal disease on dialysis, non-English language speaker or not willing, ready and/or able to engage in improving self-care behaviors and glycemic control.
Concurrent chart controls not exposed to the Boot Camp intervention were matched 1:1 to completers exposed to the intervention using propensity score matching for age, sex, race/ethnicity, insurance group, baseline HbA1c and study entry date. Prevalence rates of exclusion criteria by group were also determined. Data extraction for controls was approved under Health Insurance Portability and Accountability Act (HIPAA) waiver and waiver of informed consent. Controls received usual diabetes care through their PCPs which is aligned with the American Diabetes Association Standards of Medical Care and includes recommendations for quarterly office visits, medication management, referrals for DSMES and endocrine consultation as needed and laboratory HbA1c checks. The flow of participants is shown in figure 1.
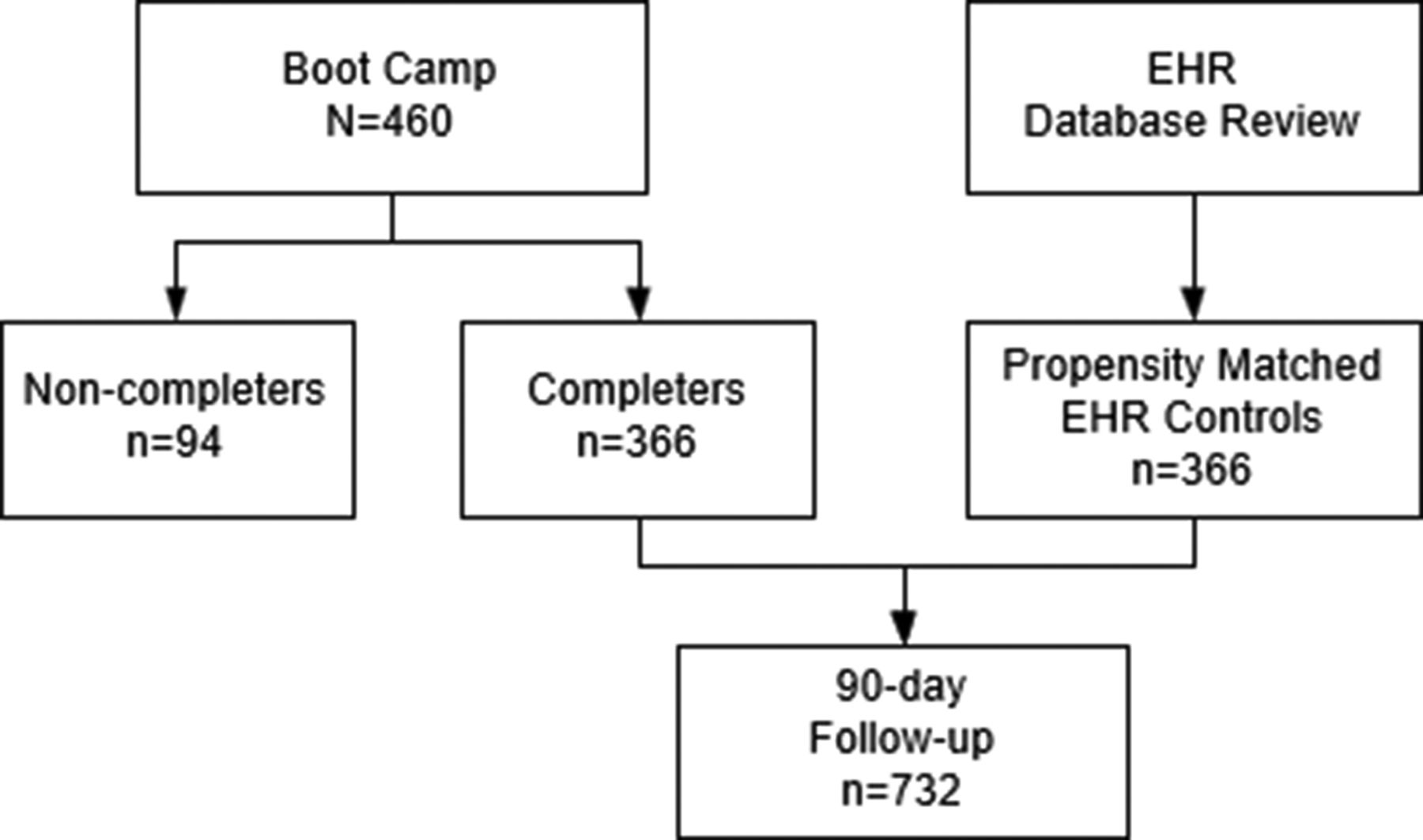
Boot Camp study flow chart. EHR, electronic health record.
Intervention design process
The Diabetes Boot Camp was developed in response to a need identified by system leadership to test alternative strategies to current DCM approaches. More than a quarter of all the target health system’s patients have diabetes, presenting a growing care burden. The Practical Robust Implementation and Sustainability Model (PRISM) was used to guide Boot Camp design.22–24 The development team included experts in DCM, primary care, health systems delivery science, implementation science and human factors engineering, as well as patients.
Diabetes Boot Camp description
The Boot Camp uses a team-based approach to offer DCM to high-risk patients with high-cost type 2 diabetes. It promotes DSMES and timely, technology-enabled antihyperglycemic medication management by certified diabetes educators (CDEs), in an expansion of their usual role and under the supervision of physicians and nurse practitioners (NPs). The extended care team includes internists, endocrinologists, CDEs, NPs, medical assistants and community health workers. Endocrinologists conceived the programme, designed all aspects of the intervention in consultation with system PCPs, diabetes educators and patients, developed the diabetes medication management algorithm, participate in educator training and provide ongoing mentoring for Boot Camp provider educators and NPs. They also consult as needed with the Boot Camp CDEs for all aspects of programme deployment including glycemic management support for individual participants.
Algorithm-guided medication management was delivered by CDEs, who were nurses, dietitians or pharmacists. System endocrinologists and CDEs developed a medication algorithm decision support tool (figure 2) based on national guidelines and an evidence-based algorithm for insulin titration.25–28 The algorithm guides adjustments based on current blood glucose (BG) values and current medications. CDEs were trained via a full-day education programme and subsequent coaching with an experienced CDE. Study diabetes-centric physicians and NPs were available as needed to provide advice to the CDEs. Embedded hard-stops in the algorithm (eg, persistent marked hyperglycemia and/or hypoglycemia) required consultation with a diabetes specialist. A study clinician reviewed and signed all medication orders daily. DSMES was initiated during the onsite, one-on-one visits with the CDE then continued by the NPs during the weekly virtual visits. The education was adapted from the American Association of Diabetes Educators.29 It covered healthy eating; glycemic targets and glucose monitoring; taking medications as prescribed; hyperglycemia and hypoglycemia recognition, treatment and prevention; knowing when to seek medical help; lifestyle and other topics identified by the participant or the provider. DSMES and medication management was facilitated by an FDA-cleared cellular-enabled BG monitoring system (BioTel BGM, previously Telcare, Concord, Massachusetts, USA), which accrues no data charges and was provided to participants with sufficient test strips to do at least two fingerstick BG checks daily. The BG measurements were auto-transmitted to a provider dashboard in near-real-time without a need for additional steps by the participant and were reviewed daily by CDEs for hypoglycemic and hyperglycemic events and weekly for participant progress.

{kind=link}
{kind=link}
MedStar Diabetes Institute type 2 diabetes Boot Camp medication management. Algorithm and guidelines.
The participant’s Boot Camp experience
A one-click Boot Camp order in the electronic health record (EHR) allowed the PCP to refer the participant for medication management, DSMES and laboratory HbA1c testing at baseline and 90 days. Participants attended two in-person meetings with a CDE within a 2-week period. These visits were held at one of five site hubs. At the first in-person visit, participants completed the ‘KNOW Diabetes’ knowledge test30 using a tablet computer then were auto-directed to short educational videos that corresponded to their knowledge deficits. DSMES content was also provided in print. Participants were provided with the BGM and taught how to use it. CDEs adjusted medications using the algorithm when needed. If a new drug was indicated, a shared decision-making process that outlined the potential risks and benefits of two medication choices was used. At the second in-person visit, CDEs discussed recent BG values, continued medication adjustment and provided DSMES. The team also addressed other needs, including psychosocial support, access to medications, and referrals to community resources.
Site visits were followed by 10 weeks of virtual visits by telephone, text and/or email. The CDEs contacted participants at minimum weekly to discuss progress, adjust diabetes medications, continue DSMES and coach towards lifestyle goals using motivational interviewing strategies. Participants were also contacted when high or low BG alerts were generated. A final in-person or virtual visit occurred at 90 days at which time patients were referred back to their system provider via an EMR flag for usual ongoing diabetes care management. Documentation of the patient’s progress during the Boot Camp including the final diabetes medication regimen, current HbA1c if available and any pertinent recommendations for additional diabetes-related care, such as referrals to podiatry or ophthalmology if needed, were provided.
The usual care experience
Controls received usual diabetes care delivered by system PCPs, per evidence-based national guidelines for type 2 diabetes care management based on the ADA Standards of Medical Care in Diabetes. They were not exposed to the Boot Camp intervention. Visits typically were quarterly, and the providers managed diabetes medications and referred to endocrinology and/or for DSMES as needed. Data were examined for a 90-day period for each control case.
Outcome measures
Effectiveness outcomes were compared among participants and controls. The primary outcome was change in HbA1c between baseline and 90 days. Secondary outcomes included risk for all-cause ED visits and hospitalizations and costs for hospitalizations. Hypoglycemia events (stratified as BG <70 mg/dL (3.9 mmol/L), BG <54 mg/dL (3.0 mmol/L) and BG <40 mg/dL (2.2 mmol/L)) were extracted from the BioTel system.
Statistical analysis
The study was powered to detect a difference of 0.5 in the change in HbA1c with SD=2 with 80% power at alpha=0.05 with a sample size of 128 in each group (paired t-test). The study reaches 100% power to detect this observed difference (1. 6, SD=2.25, post hoc) with an alpha level of 0.01. Data were summarized using means and SD for continuous variables and frequencies and percentages for categorical variables. Differences in patient characteristics and the unadjusted differences in the outcome measures between the intervention and control groups were tested using linear mixed models, McNemar tests and conditional logistic models due to matching (tables 1 and 2). The significance of the comparison between the groups of their respective within-group risk change from preintervention to postintervention was determined by longitudinal Poisson models that include time and group interactions. Multivariable Poisson regression models adjusted for preintervention utilization, baseline HbA1c, age and sex were used to estimate postintervention 30-day and 90-day hospital admission and ED visit risk for participants compared with controls (table 2). The average decrease in HbA1c among men compared with women was examined using a mixed model that included an interaction with sex and group.
Glycemic outcomes
Patient counts for hospitalizations and ED visits for 30 and 90 days and within-group/between-group IRR based on Poisson regression models
Preintervention differences between the groups in utilization outcomes were computed and tested using unadjusted Poisson regression models. Analyses were conducted in R V.3.1.0 (R Core, Vienna, Austria)31 and Stata V.14 (StataCorp, College Station, Texas, USA).32
We also conducted an analysis to examine potential for monetization of the intervention benefits from reduced inpatient services to the health system. Based on the expected times of hospitalization per patient in 90 days for both the intervention group and comparison group, estimated by the Poisson regression model, we projected the annual difference in usage of inpatient services between a patient with and without the intervention. The projected change in usage was then multiplied by the expense per diabetes-associated hospitalization, which was calculated from the actual claims data of the health system’s employee health plan in year 2017 to be US$25 162.95 per hospitalization.
Results
Patient population
Of the 460 participants enrolled, 366 who completed the 90-day intervention had both pre-HbA1c and post-HbA1c tests that could be compared. The completers were compared with 366 matched controls, resulting in a 732-person study cohort. The Boot Camp cohort had a mean age of 56 years (SD=12), was predominantly African-American (79%), female (63%), insured by Medicare and/or Medicaid (59%) and with 36% having private insurance. Baseline demographics did not differ between participants and controls and the incidence of exclusion criteria was low and not different in cases versus controls (table 3). Non-completers (n=94, 20%) were slightly younger at 51 (SD=11.8) years than completers at 56 (SD=10.6) years, p<0.001 and were 80% African-American compared with 85% for completers, p=0.0046, but did not differ by sex, insurance payer or baseline HgA1c compared with completers.
Demographics and characteristics
Process results
The Boot Camp was implemented in stepwise fashion by site over the study period. The core Boot Camp team started with a total of 1.0 FTE CDE Programme Managers, subsequently expanded to 2.0 FTE who administer the programme, train and mentor the system educators. The Boot Camp was initiated at one of nine system hospital campuses in the ambulatory clinic setting and then spread progressively to a total of five sites by the end of the study period. In-person visits were integrated into 10 existing system diabetes educators’ visit schedules. Patients were seen for in-person visits in existing diabetes education programme ambulatory clinics throughout the system in locations ranging from within a diabetes and endocrine center to community/wellness centers to embedded in internal medicine clinics.
The virtual clinic was staffed initially by one 0.6 FTE NP, CDE which was subsequently increased to a total of 2.2 FTE. The number of patients per provider is highly variable depending on the volume of referrals for each participating system site and the availability of each CDE to schedule patients for in-person visits. Virtual clinic providers—NPs have the capability of managing a total of 250 patients per year with 2.2 FTEs.
All Boot Camp participants completed the KNOW Diabetes Survey, which took 10 min to complete on average, and viewed all videos assigned during the site visits. Time viewing videos averaged 15 min depending on how many test questions had been answered incorrectly. Time to set each participant up with the BGM was 20 min or less. On average, participants had two in-person visits and 10 follow-up contacts with the virtual clinic. The 366 participants received the full Boot Camp curriculum. A total of eight CDEs delivered the programme system-wide which was usually integrated into usual workflow. Virtual clinic NPs followed about 50 participants at a time.
Effectiveness—glycemic control
The mean HbA1c for participants and controls, respectively, were 11.2% (99 mmol/mol) and 11.3% (100 mmol/mol) at baseline (p=0.14) and 8.1% (65 mmol/mol) and 9.9% (85 mmol/mol) at study end (p<0.001) (table 3). The participants’ HbA1c reduction of −3.1 units was significantly greater than the −1.4-unit reduction for controls by 1.6 (p<0.001). The change in HbA1c from baseline to postintervention was estimated to be 1.7 units larger for participants when analyzed with a linear mixed model adjusted for age, sex and baseline HbA1c (95% CI −1.9 to −1.4, p<0.001, not shown in table 2). The average decrease in HbA1c was greater by −0.52% among men compared with women (p=0.001) and did not significantly differ by study group. Additionally, a significantly higher percentage of patients in the intervention group achieved an HbA1c lower than 8% and lower than 7% as compared with the control group (table 1).
A total of 48 111 fingerstick BG measures were entered into the BioTel BGM system. Of these, 579 values were <70 mg/dL (1.2%), 133 were <54 mg/dL (0.28%) and 89 were <40 mg/dL (0.18%). No serious adverse events occurred that required assistance to treat due to hypoglycemia. Patients checked a mean of 1.5 fingerstick BGs daily. Time of day tested was varied to provide actionable BG data to facilitate medication adjustments and lifestyle management recommendations. Home BG test frequency and results were not available for the controls.
Health services utilization
Frequencies for acute care utilization (ED visits and hospitalizations) and incidence risk ratios (IRR) for readmission and ED visits at 30 and 90 days for the participants and controls are presented in table 2. At baseline, participants had significantly higher utilization levels than controls, which corresponded to significantly greater hospitalization risk in the prior 30-day window (IRR=2.7; 95% CI 1.03 to 7.13; p=0.04) and prior 90-day window (IRR=3.3; 95% CI 1.44 to 7.34; p=0.005). There were no significant differences in ED visit risks between the groups prior to baseline.
In the pre/post comparison for hospitalization risk by group, unadjusted models showed that, at 30 days, participants exhibited a 79% reduction in risk of hospitalization (IRR=0.21, 95% CI 0.07 to 0.60; p=0.003), while controls showed a non-significant increase (IRR=1.14, 95% CI 0.47 to 2.75; p=0.77), which resulted in a significant difference in the risk change between the groups (p=0.02). For the 90-day pre/post comparison, participants exhibited a 77% reduction in hospital admission risk (IRR=0.23, 95% CI 0.11 to 0.50, p<0.001) while controls exhibited a 58% non-significant increase in risk (IRR=1.58, 95% CI 0.750 to 3.33; p=0.23). The difference between the groups in risk change was highly significant (p<0.001). The difference in the decrease in the risk of all utilization (51% for participants and 20% for controls) was also significant suggesting that overall there was a bigger improvement in utilization for participants. All other differences in changes in utilization were not significant between the groups. The differences in the hospitalization risk in the postintervention period showed that the risk for admission remained significantly lower for participants at 90 days postintervention (IRR=0.44, 95% CI 0.20 to 0.95; p=0.04).
Potential financial impact attributed to averted hospitalizations
Poisson regression models of hospitalizations revealed that Boot Camp participants experienced a mean 0.1227 fewer hospitalizations per participant per year when compared with usual care controls. Based on the mean cost estimate of US$25 163 per hospitalization for a patient with diabetes, a participant in the Boot Camp is projected to potentially save the system US$3086 (in 2017 USD) annually in averted hospitalization costs in an at-risk reimbursement model.
Boot Camp adaptations
Adaptations were undertaken to better support care processes over the 3+ year study. Participants during the first 16 months provided informed consent. In July 2016, the study received a Quality Improvement designation by the IRB, so informed consent for research was no longer required.
Resources available to the Boot Camp, including space and staffing, varied by site. This made flexibility in site-specific implementation key. The intervention was first offered at three then five sites based on where system CDEs were located. Participants were initially recruited from lists generated by the study team using the EHR. Subsequently, participants were referred by their providers via a one-click order in their EHR workflow. To allow CDEs to focus on medication management and DSMES, community health workers and medical assistants were added to the team to register the BGM and instruct in its use; establish a strip supply; administer the videos; and obtain authorization for medications.
Conclusions
Compared with usual care, this 90-day patient-centered, technology-enabled DCM Boot Camp safely and significantly improved glycemic control in adults with uncontrolled type two diabetes. Reduced risk for all-cause hospitalizations and potential for monetization due to averted hospitalizations were also demonstrated.
This evidence-based Diabetes Boot Camp translated results from the DSMES literature,10 diabetes pharmacotherapy trials and national guidelines for DCM9 25–28 into real-world settings to successfully support PCPs and their patients within a regional healthcare system.9 10 18 This translation was accomplished through incorporation of multiple elements of the CCM to enhance care delivery and consideration of the PRISM domains to assure intervention alignment with organization, provider and patient factors.22 23 The intervention was well received by patients, referring providers and CDEs.
The Boot Camp enrolled high-risk (as confirmed by acute care utilization data for the 90 days prior to baseline), majority African-American participants, insured by mixed payers, and with a mean HbA1c of 11.2% (99 mmol/mol). The intervention achieved significantly improved glycemic control compared with propensity-matched controls. The observed 3.1% units (10 mmol/mol) HbA1c reduction for participants at 90 days was almost double that seen in controls and was both statistically and clinically significant. HbA1c also improved among controls, although to a lesser degree, which suggests that their providers appropriately took some action for a high HbA1c. The −1.6% absolute greater reduction in HbA1c between cases and controls is a greater improvement than is reported in most DCM interventions in the literature where mean changes in HbA1c range between −0.22% and −0.34% and absolute change ranges from no significant change to −1.5%.23 33–35 From a pragmatic perspective, the post-intervention mean HbA1c of 8.1% (65 mmol/mol) corresponds to an estimated average glucose of 186 mg/dL (10.3 mmol/L), which is close to the American Diabetes Association-recommended peak postprandial BG of <180 mg/dL (10 mmol/L).36 This degree of glycemic improvement has the potential to produce clinically meaningful change from the patient perspective, including less symptomatic hyperglycemia and improved cognitive function and mood.37
Reports from the Ochsner Clinic describe a small retrospective cohort study of a boot camp which delivered a 2-hour DCM intervention. Participants met consecutively with a physician or NP who developed a care plan, a pharmacist who evaluated medications and financial constraints, a nurse/health coach who reviewed the DCM plan and a dietitian who addressed individual nutrition needs. A diabetes care plan that explained diabetes status and important follow-up items, education handouts and a follow-up PCP appointment was provided. At 3–6 months postparticipation, HbA1c was decreased by 1.25% vs 0.11% compared with controls (p<0.001).38 At 3.2 (SD +0.54) years follow-up, sustained benefit on glycemic outcomes was demonstrated. Using comparison-over-time analysis, their boot camp group (n=69) showed a mean decrease in HbA1c from 8.57% (SD ±2.32%) to 7.76% (SD ±1.85%) compared with an increase from 7.92% (SD ±1.58%) to 8.22% (SD ±1.82%) in the controls (n=107, p<0.001).39 These data are consistent with our findings that a boot camp approach can improve glycemic control.
Our Boot Camp achieved improvements in a predominantly African-American population. This group bears an increased prevalence and disproportionate burden from diabetes and its complications.40 These disparities may be attributed to differences in quality of DSMES and medical care and other factors, including cultural beliefs about medical care, low health literacy and inequalities in health services access. A systematic review of interventions aimed at improving the diabetes care quality in African-Americans showed that interventions (mainly culturally adapted DSMES) reduced HbA1c by 0.8%.41 Future examination of the factors which supported Boot Camp success in our majority African-American cohort would be of interest.
The combined data for glycemic control suggests that the algorithm was applied both safely and effectively by trained and mentored CDEs. The Boot Camp significantly reduced risk for hospitalizations at 90 days compared with usual care. A preliminary monetization analysis calculated potential savings of approximately US$3100/participant, amortized over the study cohort. The implications of the potential savings are quite different when one considers fee-for-service compared with value-based care models. Both models need to be examined in a mixed-payer care system.
There were limitations to our study. The Boot Camp focused on participants with markedly uncontrolled type two diabetes to develop an approach to DCM for high-risk, high-cost patients. By design, this real-world study was not an RCT. We chose a pragmatic study design, with relatively broad inclusion criteria and few exclusion criteria, over the traditional explanatory study design because we wanted to see if the intervention was effective in real-world situations under the usual patient care conditions. Based on our own prior research findings12 and knowing that RCTs have shown repeatedly that an enhanced DCM strategy delivered by a dedicated team will improve outcomes, the study team and health system PCPs agreed that randomization was not desirable. We chose instead to design and evaluate an evidence-based DCM model using established implementation science strategies and standardization for delivery by CDEs and NPs.
Participants had higher utilization rates for acute care encounters pre-Boot Camp than controls which may have drawn the sicker patients to their providers’ attention and resulted in referral to the intervention. We did not conduct temporal analysis, such as seasonal trends. This was a 90-day, short-term study. We are currently examining sustainability of improved glycemic control and need for long-term support. Further work will be needed to refine implementation models for generalizability across ambulatory settings.
We hypothesize that the positive Boot Camp outcomes resulted from a synergistic impact of multiple factors. Successful patient engagement was accomplished via highly individualized support, real-time transmission of BGs and timely adjustment of diabetes medications in collaboration with the participants. Diabetes Educators were enabled to move beyond their traditional role of delivering DSMES into a non-traditional and emerging role. The CDEs participated in diabetes medication management, including the addition of new drugs to the antihyperglycemic regimen and making medication adjustments using the evidence-based medication algorithm. There are reports of diabetes educators recommending and/or adjusting medications using established protocols in the literature.42 43 In a recently reported RCT, registered dietitian nutritionists used a treatment protocol to initiate and titrate therapies for BG, hypertension and lipids in conjunction with medical nutrition therapy via telemedicine visits among adults (n=118) with type two diabetes.44 A modest but significantly greater improvement in the number of diabetes care measures met and in medication use was found in the intervention group. To our knowledge, this practice has not gained widespread traction to date and is not included in the traditional services that most diabetes educators deliver.
Additional success factors included: alignment with the CCM and PRISM; health system leadership and funding; site provider champion support; collaborative work with primary care practices; consistency with provider workflow; intensive DSMES and the personal connections established between the participants and care team through frequent interactions. In addition, real-time transmission of BG measurements was found to be transformational for care both by patients and CDEs. Finally, from the often-challenging perspective of obtaining funding to implement DCM initiatives, it is of practical interest to note that based on outcomes generated by this research, including monetization potential, health system leadership allocated financial support for further programme spread.
Challenges to implementation were encountered. Marked heterogeneity in resources, including staffing and space, existed across the sites, and necessitated flexibility in implementation. Reimbursement for site DSMES visits was possible, but we were not able to bill for the virtual visits. It will be necessary to further address reimbursement including exploration of now available billing codes for telemedicine visits moving forward.
In summary, by addressing common system, provider and patient barriers to DCM, our redesign of DCM with a technology-enabled, high-touch Boot Camp approach provides evidence to suggest that this approach can successfully meet real-world challenges.
Acknowledgments
The authors would like to thank Adline Ghazi, MD and Susan Clark, BSN, RN, CDE, MedStar Good Samaritan Hospital; Lynne Brecker, RN, CDE and Pamela Schroeder, PhD, MD, MedStar Union Memorial Hospital; Kristin Bartel, PharmD, CDE; Claudia Morrison, RD, CDE, MedStar Washington Hospital Center; Linda Rozzelle, RD, CDE and Jennifer Sapolsky, RN, CDE, MedStar Georgetown University Hospital and Debra Thayer, NP, CDE, Patricia Montesinos, NP, CDE and Maranda Parkin-Jackson, NP, PhD, MedStar Diabetes Institute, who participated in delivering the programme. The authors would like to thank Teresa Davidson, PhD, who provided editorial assistance with the manuscript.
References
Footnotes
Contributors MFM, CMN, GAY and SRE are responsible for the conception and design of the study. MFM, SJF, C-CH, MM, ARM, CMN, PAS and GAY acquired, analysed and interpreted the data. MFM, MM, C-CH, CMN, GAY and SRE drafted the manuscript. MFM, KMB, MM, ARM, CMN, PAS, KS and GAY participated in critical revision of the manuscript for important intellectual content. MFM, MM, CMN and GAY supervised the study. MFM had full access to all study data and final responsibility for the decision to submit for publication.
Funding MedStar Health provided funding and participated in the conception and design of the study and in review of the manuscript but did not participate in the decision to submit the manuscript for publication. The District of Columbia Department of Health and the American Diabetes Association each provided funding for initial pilot studies that generated preliminary data for this work. BioTel (Telcare) provided starter blood glucose monitoring system kits to enrolled patients and trained study staff but did not participate in the design and conduct of the study or the writing and submission of the manuscript.
Disclaimer The content of this manuscript is solely the responsibility of the authors.
Competing interests MFM received funding on behalf of MedStar Health Research Institute during the study period from Eli Lilly for the REWIND Study, from the Patient-Centered Outcomes Research Institute (NCT-02093234), from the National Institutes of Health (NIH DK-109503) and from Mytonomy. She served as a speaker for the American Diabetes Association and for PRIMED. KMB has no interests to declare. SJF received funding on behalf of MedStar Health Research Institute during the study period from the National Institutes of Health. CMN received funding on behalf of MedStar Health Research Institute during the study period from Eli Lilly for the REWIND Study and from the Patient-Centered Outcomes Research Institute. KS received funding from the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1-TR001409, the Agency for Healthcare Research and Quality and the National Institutes of Health (NIH DK-109503). GAY was a speaker for the American Diabetes Association during the study period. No other potential conflicts of interest relevant to this article were reported. C-CH, MM, ARM, PAS and SRE have no interests to declare.
Patient consent for publication Not required.
Ethics approval The study was reviewed and approved by the MedStar Health Research Institute’s Institutional Review Board (IRB) and was conducted from November 2014 to February 2018.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.