Article Text

Abstract
Objective Gestational diabetes mellitus (GDM) is a metabolic disorder of pregnancy that is increasingly prevalent among Chinese women. Few studies have examined whether the migration status of Chinese women contributes to the risks of developing GDM during pregnancy.
Research design and methods In this observational, cross-sectional and hospital-based study, we examined the prevalence of GDM and glycemic levels at oral glucose tolerance test (OGTT) among 491 Australian Chinese migrants (n=491) and native Chinese (n=1000). We defined GDM using the International Association of Diabetes and Pregnancy Study Groups guidelines. We collected data on maternal age, body mass index (BMI) and gestational age (GA) at booking and GA at delivery from medical records. We used multiple logistic and linear regression models to calculate the OR of having GDM and mean differences in glycemic levels in Australian Chinese migrants, relative to native Chinese.
Results Age-at-booking and BMI-at-booking adjusted GDM prevalence was significantly higher in Australian Chinese migrants than native Chinese (19.7% vs 14.6%; p=0.01). After adjusting for age, BMI at booking and GA at booking, fasting glucose levels were significantly lower (β −0.08 mmol/L; 95% CI −0.14 to 0.02), while 2-hour glucose levels were significantly higher (0.22 mmol/L; 0.02 to 0.43) in Australian Chinese immigrants than native Chinese.
Conclusions Migration status may be a marker for abnormal glucose metabolism during pregnancy among Australian Chinese migrants, possibly due to socio-economic disadvantages and lifestyle changes associated with migration.
- migration
- Chinese
- gestational diabetes mellitus
- glycemic profile
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Chinese immigrants have become a large and important part of Western populations.
The process of assimilating into Western lifestyles has increased the risk of developing adverse cardiac-metabolic health, yet little is known of the risk of developing gestational diabetes mellitus (GDM).
What are the new findings?
Compared with native Chinese during pregnancy, Australian Chinese immigrants had:
higher GDM prevalence;
higher postchallenge glucose levels;
lower fasting glucose levels.
Our results suggest that migration status may be a marker for abnormal glucose metabolism during pregnancy among Australian Chinese migrants, possibly due to socioeconomic disadvantages and lifestyle changes associated with migration.
How might these results change the focus of research or clinical practice?
Efforts to improve dietary habits and lifestyle practices of Chinese female migrants might be effective in reducing the risk of developing GDM and other cardiovascular health conditions among Chinese migrants residing in the Western world.
Introduction
Gestational diabetes mellitus (GDM) is defined as hyperglycemia first detected in pregnancy that is less than overt diabetes.1 GDM is associated with adverse maternal and offspring events, including hypertensive disorders in pregnancy, cesarean delivery, postpartum maternal type 2 diabetes (T2D), offspring macrosomia and childhood obesity.1 2 Compared with women of European descent, Chinese women are at higher risk of developing GDM.1 3–5 Identifying women at risk of GDM, especially in the Chinese population, may inform intervention strategies to reduce the rates of GDM.
In addition to traditional risk factors for GDM such as lower socioeconomic status, excessive weight gain and sedentary lifestyle during pregnancy, maternal overweight or obesity, family history of diabetes and history of GDM or macrosomia,1 2 4 emerging evidence has suggested migration to be a potential risk factor for GDM. One study suggested South Asian mothers (ie, Bangladeshis, Sri Lankans, Indians and Pakistanis), who were of lower socioeconomic status (ie, lower maternal education level and health insurance coverage), had higher risks of GDM relative to US-born non-Hispanic whites, all of whom resided in New Jersey.6 Another study reported that in New Zealand, Asian-born women had threefold to fourfold higher risk of GDM compared with women born in New Zealand.7 However, there are no data on the differential prevalence of GDM among Chinese migrants residing in high-income countries.
In the past century, Chinese migrants have become a large part of Western populations.8–12 For example, in Australia, Chinese people represented 8.3% of the overseas-born population in 2016 and are the most common source of Asian migrants.10 Typically, migrants undergo a gradual and continuous process of assimilating into local lifestyles and behaviors (ie, dietary habits, social relations, level of stress, children’s preferences) of the country or region of residence.13 14 This shift in dietary habits (ie, increased consumption of fats/sweets, dairy products, convenience food and a reduction in fruits and vegetables)15 is believed to lead to adverse health outcomes.9 15–19 Asian migrants living in Europe and North America have a greater body mass index (BMI)20 and higher rates of chronic disease including hypertension, T2D, metabolic syndrome, psychological condition or psychiatric disease, cardiovascular disease and even cancer.19 21–23 Females are also more likely to be negatively affected by adverse behavioral changes that stem from migration exposure (ie, increased intake of convenience food, less social support and increased stress and loneliness, unavailability of traditional foods and ingredients, substitution of comfort food in high fat/sugar).18 24 Investigating the prevalence of GDM among Chinese female migrants may inform health promotion and prevention strategies.25
To address these gaps, we examined and compared the prevalence of GDM and gestational glucose levels between Australian Chinese migrants (n=491) and native Chinese (n=1000), from two representative tertiary metropolitan hospitals in Australia (Melbourne) and China (Shanghai).26 We hypothesized that Australian Chinese migrants would be at higher risk of GDM and have higher glucose levels during pregnancy than native Chinese.
Methods
Study population and design
The current investigation is a substudy of the Integrated Platform for Research in Advancing Metabolic Health Outcomes of Women and Children-International (IPRAMHO-International) Collaborative Study. This study is built on the IPRAMHO Asia-Pacific study group, which provides a platform for clinicians from countries in the Asia-Pacific region to share their experience or clinical practices of screening, diagnosing and treating GDM during pregnancy and after delivery.26 27 We obtained delivery electronic records from a total of 6851 singleton pregnancies born in one calendar year in Australia and 1000 singleton pregnancies in China.26 We restricted our analyses to 491 pregnant subjects from Australia who were of Chinese ethnicity and born outside of Australia (including China Mainland, Taiwan and Hong Kong Special Administrative Region (SAR)). We applied simple random sampling method28 29 to select 1000 pregnant subjects from a Chinese cohort (Shanghai birth cohort, n=3692)30 (online supplementary figure 1).
Supplemental material
Exposure, outcomes and co-variates measures
We defined Chinese subjects’ migration status and analyzed it as the exposure in this study. According to their country of birth and permanent residence, we categorized migration status as: (1) Australian Chinese migrants who were born in China Mainland, Taiwan or Hong Kong SAR, but subsequently immigrated to and permanently resided in Australia (n=491); (2) Native Chinese as those who were born and permanently resided in China Mainland (n=1000).
At 24‒28 weeks of gestation, trained staff in both hospitals performed 75 g oral glucose tolerance test (OGTT) and measured fasting, 1-hour and 2-hour glucose levels. Clinicians from both sites diagnosed GDM using the International Association of Diabetes and Pregnancy Study Groups guidelines31 (fasting glucose ≥5.1 mmol/L; and/or 1-hour glucose level ≥10.0 mmol/L; and/or 2-hour glucose level ≥8.5 mmol/L). We further categorized GDM into three additional phenotypes based on individual OGTT readings: (1) fasting glucose impairment alone (fasting glucose ≥5.1 mmol/L and 1-hour glucose level <10.0 mmol/L and 2-hour glucose level <8.5 mmol/L); (2) postchallenge glucose intolerance alone (either 1-hour glucose level ≥10.0 mmol/L or 2-hour glucose level ≥8.5 mmol/L and fasting glucose <5.1 mmol/L); (3) both fasting and postchallenge glucose abnormality (either 1-hour glucose level ≥10.0 mmol/L or 2-hour glucose level ≥8.5 mmol/L and fasting glucose ≥5.1 mmol/L). We analyzed GDM diagnosis, phenotypes and individual OGTT readings as outcomes.
In both hospitals, we obtained data on maternal age, height, weight at first booking (≤13 weeks of gestation), gestational age (GA) at first booking and GA at delivery from medical records. Mercy Hospital for Women additionally collected information on offspring sex and birth weight. We calculated BMI at booking as weight at booking in kilograms divided by the square of height in meters.32
Statistical analysis
We examined distributions on all continuous variables. We compared all maternal characteristics between Australian Chinese immigrants and native Chinese using Student’s t-test or Mann-Whitney U test for continuous variables (based on normality of distribution) and χ2 test for categorical variables.
We calculated crude, as well as age-adjusted and BMI-adjusted prevalence of GDM in both hospitals. We used multiple logistic regression models to calculate the OR of having GDM or glycemic-defined GDM phenotypes, and generalized linear regression models (GLM) to calculate mean difference in OGTT levels in Australian Chinese immigrants relative to native Chinese subjects, respectively. We applied the following models: model 1, unadjusted; model 2, adjusted for age, BMI at booking and GA at booking. We conducted all analyses using STATA (V.14.0, StataCorp, Texas, USA).
Results
Table 1 shows the demographic characteristics of the study participants. Australian Chinese migrants tended to be older (32.7 vs 29.1 years, p<0.001), had earlier GA at delivery (38.9 vs 39.4 weeks, p<0.001) and yet similar BMI at booking (22.4 vs 22.2 kg/m2, p=0.20) compared with native Chinese. Due to the one-child policy in China, all native Chinese were nulliparous while 45.8% of the Australian Chinese migrants were nulliparous. The crude (19.8% vs 14.6%, p=0.01) as well as age-at-booking and BMI-at-booking adjusted GDM prevalence (19.7% vs 14.6%; p=0.01) was significantly higher in Australian Chinese migrants than in native Chinese. Similarly, Australian Chinese migrants had lower fasting glucose levels (4.4 vs 4.5 mmol/L, p=0.02) and yet higher postchallenge glucose levels (1 hour: 7.8 vs 7.6 mmol/L, p=0.02; 2 hours: 6.8 vs 6.4 mmol/L, p<0.001), compared with native Chinese. In addition, Australian Chinese immigrants had slightly more than half of the offspring as boys, and the average weight of infants was 3278.4 g (SD 508.3) at delivery.
Demographics between Australian Chinese migrants and native Chinese
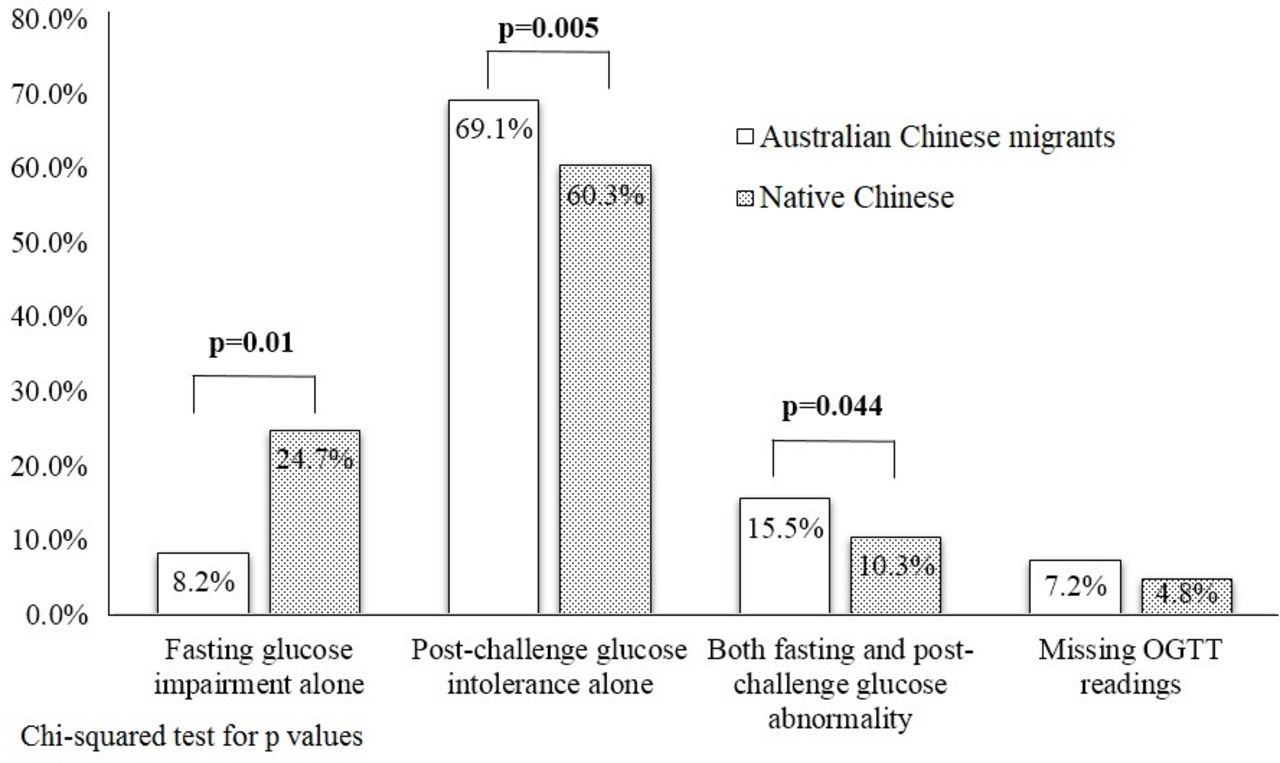
The majority of the GDM cases in both Australian Chinese migrants (67 out of 97, 69.1%) and native Chinese (88 out of 146, 60.3%) were the result of postchallenge glucose intolerance alone. A lower proportion of GDM due to fasting glucose impairment alone was observed in Australian Chinese immigrants than in native Chinese subjects (8.2% vs 24.7%; p=0.01). A higher proportion of GDM due to both fasting and postchallenge glucose abnormality was observed in Australian Chinese immigrants than in native Chinese (15.5% vs 10.3%, p=0.044) (figure 1). Excluding mothers without OGTT readings, the overall distribution of three GDM phenotypes in two hospital showed significant difference (p=0.005).

{kind=link}
The comparison of each gestational diabetes mellitus (GDM) phenotype proportion between Australian Chinese migrants and native Chinese. White column represents Australian China migrants while black dotted column represents native Chinese. Four groups are displayed as ‘fasting glucose impairment alone, postchallenge glucose intolerance alone, both fasting and postchallenge glucose abnormality and missing OGTT readings’. comparisons with ratio and p value between Australian Chinese migrants and native Chinese are shown in each GDM phenotypes except for the missing OGTT readings group. OGTT, oral glucose tolerance test.
In multiple logistic regression analyses, Australian Chinese immigrants had higher odds (OR 1.44, 95% CI 1.09 to 1.91) of GDM complicated pregnancies compared with native Chinese (table 2). In addition, compared with native Chinese, Australian Chinese immigrants had higher odds of GDM due to postchallenge glucose intolerance alone (1.61; 1.15 to 2.24) or both fasting and postchallenge glucose abnormality (2.07; 1.00 to 4.27), but lower odds of having GDM due to fasting glucose impairment alone (0.38; 0.18 to 0.81). After adjusting for maternal age and BMI-at-booking and GA at booking, most of the reported estimates attenuated to null, except for associations with GDM due to fasting glucose impairment alone (0.30; 0.12 to 0.76).
GDM prevalence between Australian Chinese migrants and native Chinese
In unadjusted linear regression analysis, Australian Chinese migrants tended to have lower fasting glucose levels (mean difference: −0.07 mmol/L; 95% CI −0.13 to −0.01) and higher postchallenge glucose levels (1 hour: 0.26 mmol/L; 0.04 to 0.49; 2 hours: 0.35 mmol/L; 0.17 to 0.54) than native Chinese (table 3). After adjusting for confounders, fasting glucose levels remained consistently lower (−0.08 mmol/L; −0.14 to –0.02), while 2-hour glucose levels remained higher (0.22 mmol/L; 0.02 to 0.43) in the Australian Chinese migrants than their counterparts in China.
Comparison of OGTT glucose readings between Australian Chinese migrants and native Chinese
Discussion
Our study from two tertiary hospitals in Australia and China showed that GDM prevalence was higher in Australian Chinese migrants than native Chinese. A substantial majority of GDM cases in both groups were due to postchallenge glucose intolerance alone. Furthermore, Australian Chinese migrants tended to have lower fasting glucose levels, yet higher postchallenge glucose levels than native Chinese. Our results suggest that migration may be a potential marker for abnormal glucose metabolism during pregnancy among Chinese women residing in Australia.
The past few decades have shown a growth in research focusing on Chinese migrants’ health and acculturation in Western world, driven by the increasing number of Chinese migrants globally.8 10–12 Studies in Australia and other Western countries have shown that trends in lifestyle changed among Asians after migration, including increased consumption of take-away foods, decreased intake of fruits and vegetables, elevated degree of social strain and higher intake of red meats and dairy products.16 17 19 33 34 For example, in a review on Chinese migrants in Australia, researchers found substantial alteration or substitution of food items in their diet such as increased usage of fatty meat or cooking oil and soda consumption, instead of green leafy vegetable cooking and Chinese tea drinking.17 Breakfast cereal, bread and potato slowly replaced rice as the main food staple in all meals.17 In addition, potato has become the substitute for sweet potato and yam, and cheese slowly took the place of tofu or bean curd in routine meals.17
As widely reported, sweetened beverages, high fat and protein diet, low fiber diet and lack of physical activity have shown associations with excess adiposity and adverse health outcomes,35 36 since it elevates inflammation in vivo,37–39 and also induces insulin resistance.40 41 In addition, other contextual factors related to migration such as failure to integrate into the new society, feelings of loneliness and exclusion, unemployment and unhealthy lifestyles18 42 43 might worsen the cycle of unhealthy food intake and poor health outcomes. Recent studies have also shown that adverse psychosocial risks such as depression and anxiety could contribute to oxidative stress,44 45 endothelial dysfunction,45 inflammation45 and insulin resistance,46 eventually contributing towards the development of cardiometabolic disease. Migrants from non-English-speaking backgrounds (ie, Mediterranean, South Asian, South-East Asian, African or South Pacific Island) are more likely to develop diabetes or coronary heart disease.17 22 23 34 Unhealthy dietary habits coupled with reduced physical activity and a degree of isolation in social circles have greater negative consequences for female migrants, who are doubly marginalized as being a woman and a foreigner.16 18 24 These findings may explain our observations of a higher prevalence of GDM among the Australian Chinese migrants than the native Chinese, even after adjusting for age, BMI at booking and GA at booking.
We did not observe differences in BMI at booking, yet found differences in glucose levels between Australian Chinese migrants and native Chinese. Even though adiposity is a major contributor for insulin resistance, the pathogenesis of GDM is multifactorial, including insulin secretion insufficiency and insulin resistance.47 We observed that Australian Chinese migrants had lower odds of fasting glucose impairment, yet had higher odds of postchallenge glucose intolerance than native Chinese. As we know, GDM is likely a heterogeneous condition48 and thus, its underlying pathophysiological mechanism varies. Past studies have established that obesity or excessive adiposity could drive the increment in liver fat, hepatic glucose overproduction, reduced insulin action and inadequate beta cell expansion and function,49 50 all of which might lead to elevated fasting glucose in vivo. On the contrary, increased production of inflammatory cytokines (ie, interleukin-6, tumor necrosis factor-α)47 51 and placental hormones (ie, placental lactogen)47 52 could affect the muscles (through reduction in both glucose uptake and insulin receptor substrate 1 protein secretion47 and pancreas (through increased beta cell mass and dysfunction).47 Such phenomena may not necessarily be related to adiposity and could affect postchallenge glucose tolerance and ultimately, elevate postchallenge glucose levels.
The public health importance of our findings is notable. Since the Chinese migrant population is large and growing in Australia, studies that examine the underlying pathophysiology of GDM and subsequent conversion to T2D in female migrants living in high-income countries are needed. This merits further attention from health professionals caring for Chinese migrants, given the known consequences of GDM on both mothers and their offspring.1 2 Moreover, women have the strongest influence on nutrition and health behaviors of all members in the family.18 Efforts to improve dietary habits and lifestyle practices of Chinese female migrants might be effective in reducing the risk of developing pregnancy complications like GDM among these women.
The strength of our study is a relatively large and representative sample of Chinese pregnant women including immigrants in Australia and natives in China Mainland. All medical examinations were done in tertiary hospitals according to standardized protocols. However, there are noteworthy limitations in our study. First, our findings may be biased by residual confounding from data that were unavailable in our study, such as length of residence in Australia, urban or rural residency, physical activity record, household income, maternal education and other sociodemographic characteristics, psychosocial evaluation, GA at GDM diagnosis and fetal sex. In addition, all pregnancies were nulliparous among Shanghai study subjects and thus, parity cannot be considered as a major confounder in our analyses. Second, even though the Han ethnic group is known to be the majority in Chinese societies including China Mainland, Taiwan, Hong Kong SAR and overseas, systematic differences in lifestyles, beliefs and dietary habits and even Chinese ethnicity (ie, Han) among these regions53 may have also biased our study findings.
Conclusion
Our study showed that Australian Chinese migrants were more likely to have GDM, predominantly from postchallenge glucose intolerance alone than fasting glucose impairment alone, than native Chinese subjects. Migration may be a potential marker for abnormal glucose metabolism during pregnancy among Chinese females residing in Australia, possibly due to suboptimal lifestyles (ie, overnutrition and sedentary activity) and socioeconomic disadvantage. Further research using a larger population sample and comprehensive variables (ie, socioeconomic characteristics and length of migration, and birth outcomes) is warranted to explore this relationship in migrants’ health.
References
Footnotes
Contributors L-JL designed the study, performed data analyses, interpreted the results and wrote the whole manuscript. JZ and AS provided the data and edited the manuscript. IA reviewed and edited the manuscript. KHT designed the study, reviewed and edited the manuscript. L-JL is responsible for the integrity of the work as a whole.
Funding This work was supported by Singapore National Medical Research Council (NMRC) KKH Centre Grant (NMRC/CG/C008A/2017_KKH) and NMRC Transition Award (NMRC TA/0027/2014).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The SingHealth Centralised Institutional Review Board and National Health Group’s Domain Specific Review Board approved the study, while Mercy Health Human Research Committee (2018-016) and Ethics Committee of Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine (XHEC-C-2013-001-2) approved the data collection from both study sites.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.