Article Text

Abstract
Introduction We examined whether adults living in highly walkable areas are less likely to develop pre-diabetes and if so, whether this association is consistent according to immigration status and ethnicity.
Research design and methods Population-level health, immigration, and administrative databases were used to identify adults aged 20–64 (n=1 128 181) who had normoglycemia between January 2011 and December 2011 and lived in one of 15 cities in Southern Ontario, Canada. Individuals were assigned to one of ten deciles (D) of neighborhood walkability (from lowest (D1) to highest (D10)) and followed until December 2013 for the development of pre-diabetes.
Results Overall, 220 225 individuals in our sample developed pre-diabetes during a median follow-up of 8.4 years. Pre-diabetes incidence was 20% higher among immigrants living in the least (D1) (adjusted HR 1.20, 95% CI 1.15 to 1.25, p<0.0001) versus most (D10, referent) walkable neighborhoods after accounting for age, sex, and area income. Findings were similar among long-term residents and across sexes. However, susceptibility to walkability varied by ethnicity where D1 versus D10 adjusted HRs ranged from 1.17 (95% CI 1.02 to 1.35, p=0.03) among West Asian and Arab immigrants to 1.32 (95% CI 1.19 to 1.47, p<0.0001) in Southeast Asians. Ethnic variation in pre-diabetes incidence was more marked in low walkability settings. Relative to Western Europeans, the adjusted HR for pre-diabetes incidence was 2.11 (95% CI 1.81 to 2.46, p<0.0001) and 1.50 (95% CI 1.27 to 1.77, p<0.0001) among Sub-Saharan African and the Carribean and Latin American immigrants, respectively, living in the least walkable (D1) neighborhoods, but only 1.24 (95% CI 1.08 to 1.42, p=0.002) and 1.00 (95% CI 0.87 to 1.15, p=0.99) for these same groups living in the most walkable (D10) neighborhoods.
Conclusions Pre-diabetes incidence was reduced in highly walkable areas for most groups living in Southern Ontario cities. These findings suggest a potential role for walkable urban design in diabetes prevention.
- epidemiology
- ethnic differences
- pre-diabetes
- environmental factors
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Growing evidence has shown that adults living in neighborhoods that are highly walkable achieve higher mean step counts per day and are more likely to meet recommended levels of physical activity than residents in less walkable areas.
However, because of residential self-selection, it is unclear if individuals living in more walkable neighborhoods are healthier to begin with, resulting in biased estimates of the potential benefits of walkability. Prior studies have not examined the consistency of these associations across higher and lower risk populations.
What are the new findings?
Living in a walkable neighborhood may reduce the burden of diabetes in certain populations by preventing earliest stages of diabetes development.
Residents living in the least walkable neighborhoods had a 15%–20% higher incidence of pre-diabetes than those living in highly walkable areas. However, this association varied substantially, in both magnitude and direction, depending on the ethnicity of the population.
Living in the least walkability neighborhood was associated with a 17% to 32% higher incidence of pre-diabetes areas among immigrants from West Asia and Arab, Latin Americans, Sub-Saharan African and the Caribbean, and Southeast Asian populations, relative to those living in high walkability.
Significance of this study
How might these results change the focus of research or clinical practice?
Findings from this study suggest that urban designs that are more conducive for walking may be beneficial in slowing the progression from early to later stages of diabetes development.
However, a one-size-fits-all solution is unlikely to be sufficient when considering interventions to reach all populations.
Thus, further research should strive to understand the contextual factors contributing to diabetes development in high-risk populations.
What environmental or neighborhood factors offset the effects of walkability on pre-diabetes incidence among high-risk populations?
What other social, cultural, and environmental factors may help to explain the differences in the propensity for different ethnic populations to walk or not walk within residential areas?
Would policies and interventions focused on increasing neighborhood walkability in fact translate into fewer cases of pre-diabetes or diabetes?
Introduction
The current wave of type 2 diabetes is a global public health concern. Rapid rises in obesity in many areas of the world combined with an aging population have contributed to an increase in the prevalence of type 2 diabetes.1 2 These changes have been particularly marked in low-income and middle-income countries where rapid urbanization and economic development have led to widespread changes in physical activity and diet.3 These trends create a challenge for health systems worldwide and carry substantial economic implications. Projections suggest that diabetes will cost USD $1.7 trillion to world economies between 2011 and 2030 through losses in GDP.4 Policies to address factors within the environment that perpetuate sedentary behaviors and unhealthy eating may help offset the burden and costs associated with diabetes.
Diabetes prevention trials have shown that intensive lifestyle interventions consisting of dietary changes and physical activity were highly effective in reducing the likelihood of transitioning from pre-diabetes to type 2 diabetes.5 These interventions generally involved one-on-one counseling by a team of experts and thus, were associated with considerable costs and resources.6 There are growing concerns regarding the feasibility of broadly incorporating such interventions in real-world clinical settings. In light of this, many governments are searching for effective policies to promote physical activity and healthy eating in the general population.
A growing body of evidence suggests that residents living in older, more compact neighborhoods engage in more physical activity than those living in sprawling, car-dependent areas.7 8 In the International Physical activity and Environment Network study, conducted in 14 cities across Europe and the USA, residents living in activity-friendly neighborhoods were more likely to meet the recommended number of minutes of moderate to vigorous physical activity.7 Countries where a larger proportion of the population walk have a lower prevalence of obesity.8 Moreover, highly walkable neighborhoods have been associated with lower rates of diabetes and other metabolic diseases, presumably through beneficial effects on obesity, weight gain, and insulin resistance.9–14
Pre-diabetes, characterized by mild elevations in glycemia, represents a phase in the course of type 2 diabetes development where prevention strategies targeting physical activity and diet may be most impactful. It is unknown whether neighborhood environments that support walking can ameliorate these early glucose abnormalities. Also, prior studies have not examined the consistency of these associations across higher and lower risk populations. The primary objective of this study was to examine whether neighborhood walkability is a risk factor for pre-diabetes development in general, and among ethnic groups with varying levels of risk for type 2 diabetes. Further, we sought to examine whether neighborhood walkability modifies the effects of ethnicity on pre-diabetes incidence.We hypothesized that highly walkable neighborhoods would be associated with a reduced incidence of pre-diabetes relative to less walkable areas and that differences between ethnic groups would vary more in low walkability settings than highly walkable ones.
Methods
Study design
We used population-level data to study the association between neighborhood walkability and pre-diabetes incidence among residents of Southern Ontario, Canada, and to assess the consistency of its effects in higher and lower risk populations defined by their immigration status and ethnicity. Federal immigration records were linked to administrative healthcare datasets to ascertain information about immigration status. All datasets were linked and analyzed at ICES, a research institute affiliated with the University of Toronto, using unique encoded identifiers based on encrypted versions of each individual’s health card number to retain anonymity. The study focused on residents living in one of 15 municipalities in Southern Ontario (the Greater Toronto–Hamilton Area, London, and Ottawa) during the period from January 1, 2002 to December 31, 2011.
Study population
Adults aged 20–64 with normal glucose values were identified using a commercial laboratory database, Dynacare Medical Laboratories (DML) and followed until December 31, 2013 for the development of pre-diabetes. Individuals entered the cohort on the date of their first glucose test performed during the eligibility period. Normoglycemia was defined as a fasting plasma glucose value less than 6.1 mmol/L, a glucose value of less than 7.8 mmol/L 2 hours after a 75 g oral glucose tolerance test (OGTT), or a glycosylated hemoglobin (HbA1c) of <6.0% as per the case definition adopted by WHO and Diabetes Canada.15 Those with values <6.1 mmol/L on a non-fasting, or random glucose test were also included in our cohort in the absence of any exclusion criteria. Individuals with a prior diagnosis of type 2 diabetes, identified using the Ontario Diabetes Database (ODD), were excluded from our cohort. The ODD uses a validated algorithm based on physicians’ services claims and hospitalization records to identify new cases of diabetes, with a sensitivity of 84.2% and specificity of 99.2%.16 Because previous studies have shown clear associations between area walkability and diabetes incidence among younger but not older adults and the etiology of pre-diabetes development may differ between these populations, we restricted our cohort to adults 20–64 years of age.9–12
Records were linked to the Ontario Registered Persons Database (RPDB) to gather demographic and vital statistics information on all individuals in the cohort and to ascertain their eligibility to receive coverage under the province’s universal healthcare plan.
Main exposures
The primary exposure in this study was neighborhood walkability at baseline, which was assigned to individuals using a validated walkability index based on their postal code of residence. Briefly, the walkability index was created for small neighborhood units (dissemination areas) in Southern Ontario cities and validated against transportation data collected from 128 420 households living in the same communities. Dissemination areas (DAs), as defined by Statistics Canada, include one or more adjacent city blocks and a population of ~400–700 people. The walkability index was derived based on four variables: population density and residential density (2006 Canada Census), street connectivity (DMTI Spatial Inc., 2009), and the availability of retail outlets, services, and schools within walking distance of people’s homes using an 800 m geographic boundary around the center of each residential area (DMTI Spatial Inc., 2009; Ontario’s Ministry of Education, 2009).9–12 Standardized scores for each of the four components were weighted equally, resulting in a single score ranging from 0 to 100.11 In previous research, the walkability index was validated and neighborhoods with higher walkability scores had higher rates of walking and cycling and lower rates of car use, overweight and obesity, and diabetes incidence. Deciles of the walkability index were generated by ordering DAs according to increasing walkability and allocating an equal number to each decile, from least (decile (D1)) to most (decile (D10)) walkable.
Second, the Immigration, Refugees and Citizenship Canada Permanent Resident (IRCC-PR) database includes records for individuals who immigrated since 1985 and includes a variety of sociodemographic indicators on immigrants prior to their arrival to Canada. Therefore, individuals who were in the IRCC-PR were classified as immigrants; otherwise, all others were classified as long-term residents. For immigrants only, ethnicity was derived based on a validated algorithm using country of birth, mother tongue, and surname (online supplementary table 1).17 The distinct ethnic groups in which pre-diabetes development was examined included South Asian, East Asian, West Asian and Arab, Sub-Saharan African and Caribbean, Latin American, Southeast Asian, Eastern European, and Western European. On arrival to ICES, records from the IRCC-PR are probabilistically linked to the RPDB (linkage rate of 86.4%) using a encoded identifier which allows them to be linked to other datasets, as described previously.18
Supplemental material
Outcome measures
Individuals were followed for a minimum of 2 years until December 31, 2013 for the development of pre-diabetes. Pre-diabetes was defined as per criteria used by WHO and Diabetes Canada, which includes one or more of the following test results: any fasting glucose (impaired fasting glucose (IFG)) value in the range of 6.1 to 6.9 mmol/L, a glucose value of 7.8 to 11.0 mmol/L 2 hours after a 75 g OGTT (impaired glucose tolerance (IGT)), or HbA1c of 6.0%–6.4%, inclusive.15
Secondary outcomes included pre-diabetes defined using the American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD) to ascertain pre-diabetes incidence based on IFG (5.7 to 6.9 mmol/L) and HbA1c (5.7%–6.4% (39 to 46 mmol/mol)) or the presence of IGT as defined previously.
Other covariates
The IRCC-PR database was used to gather additional baseline information at the time of immigration to Canada on all members of our cohort, including education level at arrival, English or French language proficiency, marital status, immigration visa category, country of birth, and mother tongue. Baseline metabolic risk was assessed using information on hypertension and dyslipidemia. A previous diagnosis of hypertension was assessed using a validated algorithm, which included any hospital admission record or two physician services claims within 2 years listing a diagnosis of hypertension (specificity 95%, sensitivity 72%).19 Lipid levels (high-density lipoprotein (HDL)-cholesterol, low-density lipoprotein (LDL)-cholesterol, total cholesterol, and triglycerides) prior to index were obtained from the DML database. The 2006 Canadian census and residential postal codes were used to derive relative area-level income quintiles, adjusting for household and community size.9–12
Statistical analyses
Cox proportional-hazards models were used to assess whether neighborhood walkability was a risk factor for pre-diabetes incidence in our overall cohort. We divided our population into two groups (lowest and highest walkability decile) based on their neighborhood walkability scores, with high walkability neighborhoods (D10) serving as the referent. Unadjusted and adjusted models (including age, sex, area income, and walkability) were generated, censoring for death or loss of healthcare eligibility.
In addition, we compared the effects of walkability on pre-diabetes incidence by immigration status and among immigrants to Canada, we examined its effect within each ethnic group. To do so, our Cox models were generated by ethnic group and adjusted for all the baseline covariates listed above (ie, age, sex, area income, and walkability) as well as education, immigration visa category, marital status, and duration in Canada. In each model, high walkability (D10) served as the referent category. We also examined the extent to which neighborhood walkability modified the effects of ethnicity on pre-diabetes incidence among immigrants. To do so, we ran separate, fully adjusted Cox models in this population for the highest and lowest deciles of walkability. As a sensitivity analysis, we re-ran our models using ADA/EASD thresholds for pre-diabetes instead.
All analyses were conducted using an alpha level of 0.05 and by using SAS V.9.4.
Results
Overall, our study population consisted of 267 529 and 860 652 immigrants and long-term residents, respectively. Baseline characteristics of the study population according to most and least neighborhood walkability and by ethnicity are shown in tables 1 and 2, and online supplementary table 2, respectively. A greater proportion of the most walkable neighborhoods were low income (table 1). Across all ethnic groups, a significant proportion of immigrants had high school education or less and more than half reported English proficiency at the time of application for immigration (table 2). The largest proportion of immigrants in our sample were from South Asia and East Asia. A relatively higher proportion of immigrants lived in less walkable neighborhoods, particularly those of South Asian, West Asian and Arab, and Eastern Europeans compared with other ethnic groups. There were few differences in the prevalence of underlying metabolic abnormalities at baseline (ie, previous hypertension, low HDL, high triglycerides, and total cholesterol) between people living in least and most neighborhood walkability decile, and across different ethnic groups (tables 1 and 2 and online supplementary table 2).
Baseline characteristics of study population living in neighborhoods within the lowest and highest decile of walkability (n=1,128,181)
Baseline characteristics of immigrants living in neighborhoods within the lowest and highest decile of walkability (n=267 529)
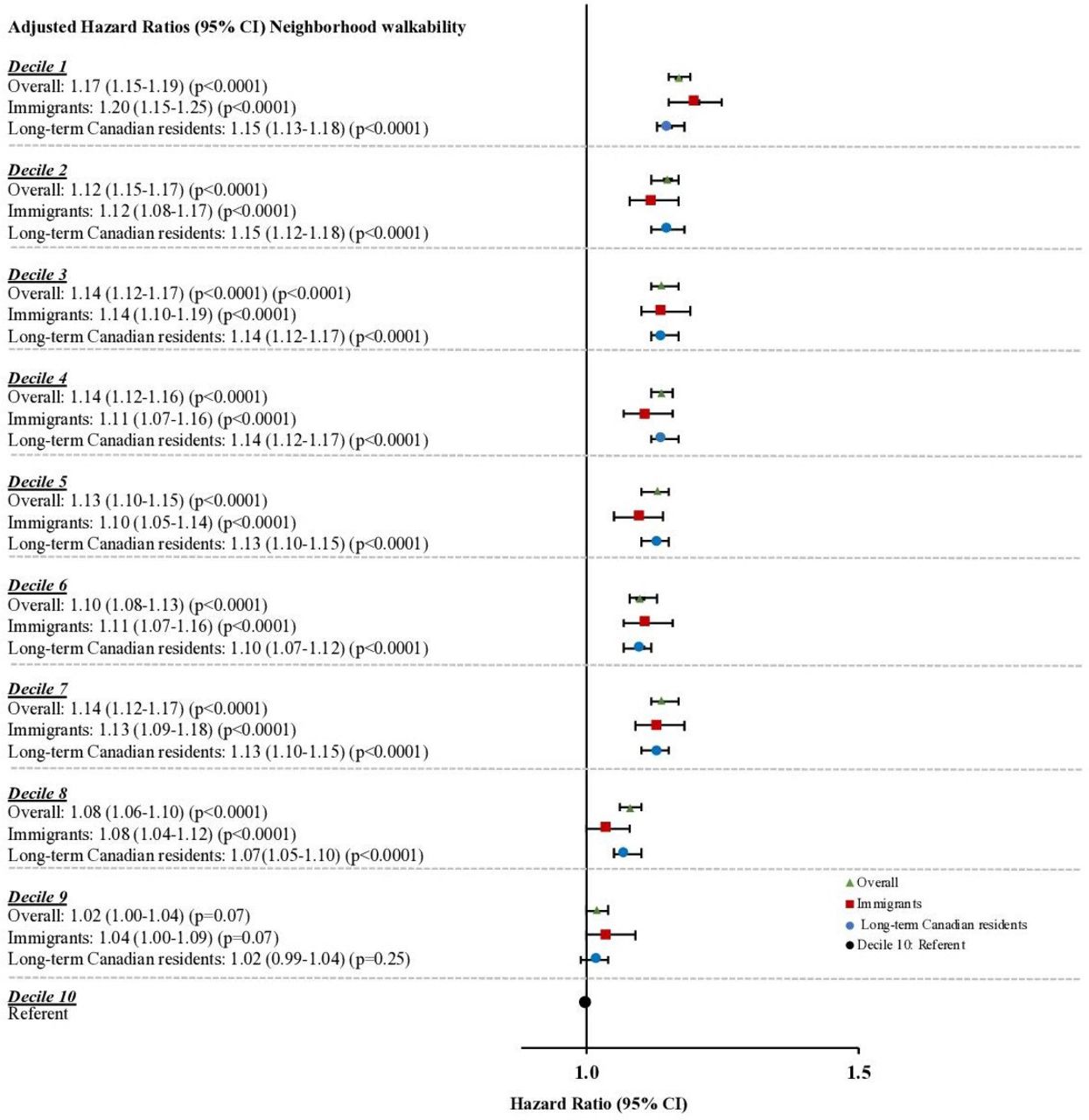
Over a median follow-up of 8.4 years, 50 971 immigrants developed pre-diabetes, of whom 5641 lived in neighborhoods in the lowest walkability decile (crude incidence rate of 3.48 per 100 person-years), and 4407 lived in neighborhoods in the most walkable decile (crude incidence rate of 3.30 per 100 person-years). Living in the least (D1) versus most (D10) walkable neighborhood was associated with a significantly increased risk of developing pre-diabetes overall (adjusted HR 1.17, 95% CI 1.15 to 1.19), as well as among immigrants (adjusted HR 1.20, 95% CI 1.15 to 1.25) and long-term residents (adjusted HR 1.15, 95% CI 1.13 to 1.18) (figure 1). Furthermore, there was a significant interaction between area walkability and ethnicity (p<0.0001 for the interaction), suggesting that low walkability was an important risk factor for some but not all ethnic groups (figure 2). For example, living in the least walkability neighborhood was associated with a 17% to 32% higher incidence of pre-diabetes relative to those living in high walkability areas among immigrants from West Asia and Arab, Latin Americans, Sub-Saharan African and the Caribbean, and Southeast Asian populations. However, low walkability had a neutral (South Asians and East Asians) or reverse association (Western Europeans) among other groups.

Risk of developing pre-diabetes according to decile of neighborhood walkability (n=1 128 181). *Adjusted for age, sex, and area income. Referent for Overall population, Immigrants, and Long-term Canadian residents is indicated by single symbol (black circle). Separate models were run for each subpopulation. Study population: adults aged 20–64. Study area: Greater Toronto Area, Hamilton, Ottawa, London. Data sources: Dynacare Medical Laboratories, Immigration, Refugees and Citizenship Canada Permanent Resident, 2006 Canadian census, Registered Persons Database, Ontario Diabetes Database. Pre-diabetes was ascertained using glucose thresholds according to WHO and Diabetes Canada: (1) fasting glucose 6.1 to 6.9 mmol/L, (2) 2-hour glucose 7.8 to 11.0 mmol/L on 75 g OGTT, (3) HbA1c 6.0% to 6.4%. HbA1c, glycosylated hemoglobin; OGTT, oral glucose tolerance test.
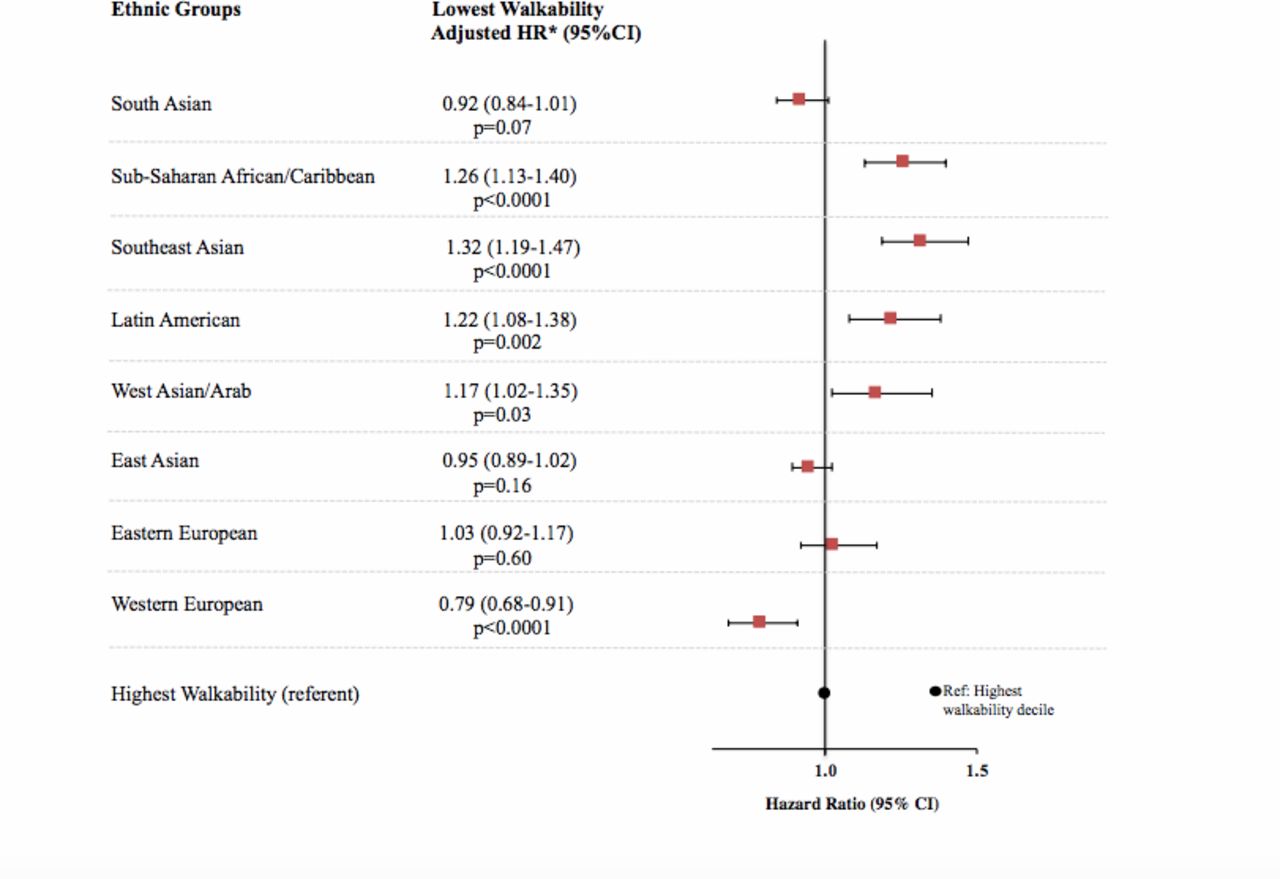
Pre-diabetes incidence among immigrants living in least walkable relative to most walkable neighborhoods, by ethnicity. *Adjusted for age, sex, area income, ethnicity, education, marital status, immigration visa category, duration. Lowest walkability refers to decile 1 and highest walkability, decile 10, is the referent. Interactions between the lowest walkability decile (D1) and Sub-Saharan African/Caribbean, Southeast Asians, and Western Europeans were significant at p<0.0001, interactions between D1 and Latin Americans and West Asian/Arabs were significant at p<0.05. Study population: adults aged 20–64. Study area: Greater Toronto Area, Hamilton, Ottawa, London. Data sources: Dynacare Medical Laboratories, Immigration, Refugees and Citizenship Canada Permanent Resident, 2006 Canadian census, Registered Persons Database, Ontario Diabetes Database. Pre-diabetes was ascertained using glucose thresholds according to WHO and Diabetes Canada: (1) fasting glucose 6.1 to 6.9 mmol/L, (2) 2-hour glucose 7.8 to 11.0 mmol/L on 75 g OGTT, (3) HbA1c 6.0% to 6.4%. HbA1c, glycosylated hemoglobin; OGTT, oral glucose tolerance test.
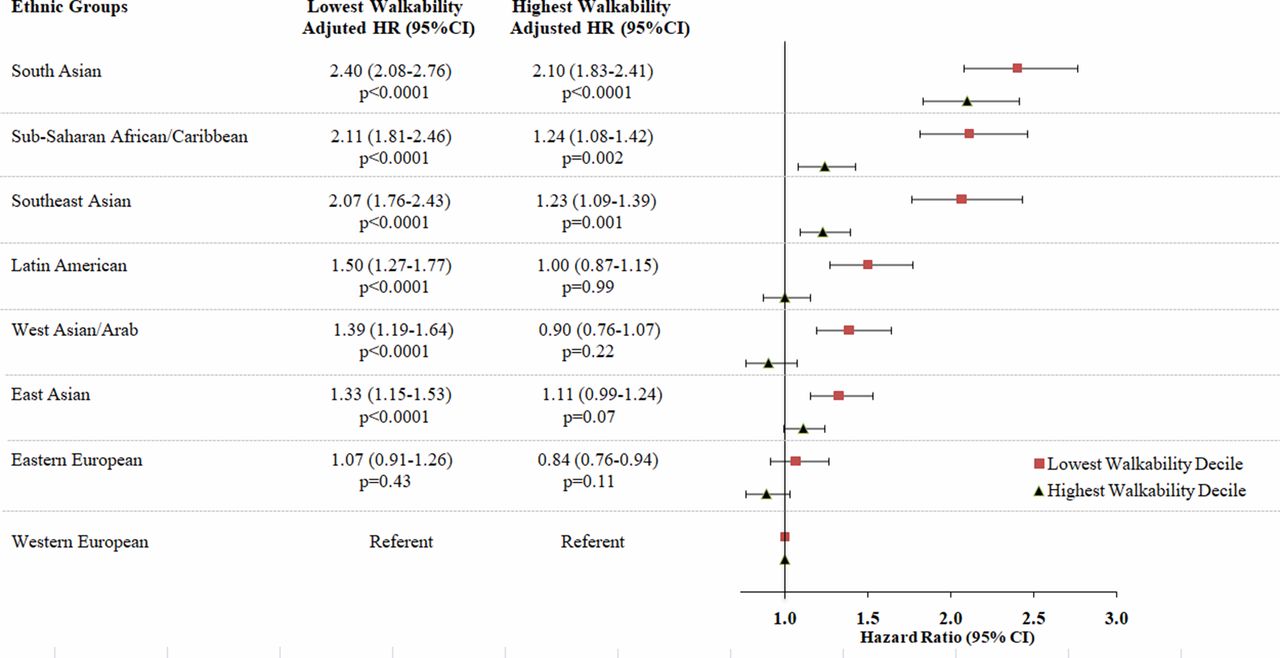
Overall, ethnicity was an important predictor of pre-diabetes incidence with many non-European immigrant groups having a higher risk of developing pre-diabetes than immigrants of European descent (figure 3). However, ethnic disparities were more marked in the least walkability neighborhoods and substantially diminished in the most walkability areas, depending on the population. For example, among immigrants living in low walkability areas, South Asians (HR 2.40, 95% CI 2.08 to 2.76) and Sub-Saharan African and Caribbeans (HR 2.11, 95% CI 1.81 to 2.46) had twice the incidence of pre-diabetes relative to Western Europeans after adjusting for sociodemographic and immigration factors (figure 3). These same groups had only a 10% (HR 2.10, 95% CI 1.83 to 2.41) and 24% higher (HR 1.24, 95% CI 1.08 to 1.42) incidence relative to Western Europeans in high walkability areas, respectively. West Asians and Arabs, Latin Americans, and East Asians had a 33%–50% higher risk of developing pre-diabetes relative to Western Europeans in low walkability areas but nearly identical incidence rates to this group in more walkable neighborhoods. Although in the least walkability areas, South Asian populations had the highest incidence of pre-diabetes at more than twice the incidence of Western Europeans, the association with neighborhood walkability changed the least when comparing the most to least walkable deciles. Lastly, our analyses based on the ADA/EASD cut-offs for pre-diabetes yielded similar results, as shown in online supplementary tables 3–5.
{kind=link}
{kind=link}
{kind=link}
Likelihood of developing pre-diabetes among non-Western European immigrants relative to Western Europeans in the least and most walkable neighborhoods. Study population: adults aged 20–64. *Adjusted for age, sex, area income, ethnicity, education, marital status, immigration visa category, duration. Study area: Greater Toronto Area, Hamilton, Ottawa, London. Lowest walkability refers to decile 1 and highest walkability refers to decile 10. Data sources: Dynacare Medical Laboratories, Immigration, Refugees and Citizenship Canada Permanent Resident, 2006 Canadian census, Registered Persons Database, Ontario Diabetes Database. Pre-diabetes was ascertained using glucose thresholds according to WHO and Diabetes Canada: (1) fasting glucose 6.1 to 6.9 mmol/L, (2) 2-hour glucose 7.8 to 11.0 mmol/L on 75 g OGTT, (3) HbA1c 6.0% to 6.4%. HbA1c, glycosylated hemoglobin; OGTT, oral glucose tolerance test.
Discussion
In this study, residents living in highly walkable neighborhoods had a lower likelihood of developing pre-diabetes than those living in less walkable areas. Individuals of non-European descent developed pre-diabetes at a more accelerated rate than Western Europeans, with some ethnic groups including South Asians and Sub-Saharan Africans and Caribbeans demonstrating a twofold increase in pre-diabetes incidence. However, this disparity was primarily observed among those living in low walkability areas–and was markedly diminished among those living in high walkability areas. These findings support the notion that neighborhood designs that encourage walking and other physical activities could potentially help to reduce the burden of diabetes in certain populations by preventing earliest stages of diabetes development.
Growing evidence has shown that people living in more walkable neighborhoods have higher overall levels of physical activity and as a result are more likely to meet recommended guidelines for the number of minutes of moderate to vigorous physical activity per week.7 These associations may contribute to the reduced prevalence of obesity and lower incidence of diabetes observed among those living in high walkability neighborhoods.8–14 Findings from our study revealed that the benefits of walkability may extend to the earliest stages of type 2 diabetes development—prior to even the mildest elevation in glucose. Concordant with our findings, a small, randomized controlled trial from the UK showed that a strategy that promoted physical activity through walking was effective in improving glucose tolerance and fasting glucose levels.20 Findings from the Multiethnic Study of Atherosclerosis cohort in the USA found that residents who reported greater access to physical activity resources and healthy foods were less likely to develop insulin resistance and type 2 diabetes.21 Thus, neighborhood designs that support residents in making positive behavioral changes, including the ability to walk or perform other physical activities on a regular basis, may help to reduce the community-level burden of pre-diabetes or type 2 diabetes.
One of the most important features of walkable neighborhoods is that they provide opportunities to engage in various forms of physical activity.22 In recent decades, urban planning practices have shifted toward sprawling urban developments with separation of lands for residential and commercial purposes.9 Such designs may limit opportunities for walking or cycling as a means of transportation or to conduct errands, as opposed to neighborhoods built prior to World War II that are more compact and offer greater access to retail destinations within walking distance of residents’ homes.9 As a result, increasing reliance on vehicles for transportation is thought to have contributed to reduced levels of physical activity and more time spent on other sedentary forms of transportation.10 In our study, the majority of immigrants lived in sprawling, car-dependent neighborhoods which offer fewer opportunities for physical activity, thereby contributing in theory to an increased risk of pre-diabetes development.
In this study, the associations between walkability and pre-diabetes incidence varied across ethnic groups for reasons that were unclear. This may be due to differences in the propensity for different ethnic populations to walk within residential areas, which may vary depending on cultural attitudes toward walking and/or a preference toward other physical activities. Studies from the USA, UK, and Canada have shown that non-whites and South Asians in particular were less physically active compared with people of other ethnicities.23–25 In addition, the type of physical activity varies by ethnicity; for example, some ethnic groups participate in recreational activities, while others prefer organized exercise programs or home-based exercises.26 Hence, neighborhood-level walkability measures may not be an ideal proxy for overall physical activity behaviors in certain ethnic groups. Furthermore, other neighborhood factors such as perceptions of safety (eg, levels of crime, sidewalk repairs, and lighting), seasonality, access to healthy versus unhealthy food options, social cohesion, and enhanced social support in ethnic enclaves may also influence the extent to which people walk within their neighborhood, along with other risk factors for diabetes.27–29 Hence, neighborhoods that support healthy living may be necessary, but perhaps not sufficient to enable all residents to be healthy and active.
This study has several limitations. First, administrative and immigration databases were used to classify individuals into appropriate ethnic origins, and due to heterogeneity in ethnic identities, some misclassification may have occurred. Second, self-selection may lead to confounding if residents who choose to live in high versus low walkability neighborhoods based on non–health-related factors (ie, proximity to work or school, affordability, etc) or prefer to do so are inherently healthier. However, studies that have attempted to address self-selection bias have found significant associations between walkability, physical activity, and diabetes risk.30 Furthermore, we assumed that people remained in the same neighborhood during the follow-up period due to missing data on changes in address. Third, our study also lacked information on behavioral data such as body mass index, physical activity level, or diet. Other Canadian studies suggest that overweight and obesity rates remained lower over time in highly walkable areas, and those living in highly walkable areas or moving from areas of low to high walkability gain less weight over time.11–13 However, the baseline metabolic profile of our study population by immigration status and ethnicity were comparable for those living in the least and most neighborhood walkability decile. Fourth, the long-term resident group may have included individuals who arrived to Canada prior to 1985, leading to some degree of misclassification. Also, because the IRCC-PR data include sociodemographic information on immigrants only, ethnicity could not be derived for long-term residents. Fifth, we did not account for differences in the retail food environment across neighborhoods which may have offset potential benefits of highly walkable neighborhoods.27 Sixth, in this study we did not examine the impact of air pollution concentrations as a contributing risk factor for pre-diabetes development. However, other studies have shown that concentrations of traffic-related air pollutants, such as nitric oxide, may be higher in some highly walkable areas due to idling of cars—a factor that might offset the benefits of high walkability on diabetes risk.31 32 Lastly, although we did not examine healthcare utilization via primary care visits, prior research suggests that under Ontario’s universal healthcare plan, screening rates for diabetes are high among immigrant populations.33
Pre-diabetes is a critical window for diabetes prevention and a risk factor for other chronic diseases including cardiovascular disease and certain cancers.34 Our study was the first to examine the effect of walkability on early markers of dysglycemia in populations at high risk of developing diabetes and to investigate the extent to which the susceptibility to walkability varied across ethnic groups. Our findings suggest that urban environments that support physical activity may help to reduce the development of pre-diabetes. However, while these findings may appear intuitive, randomized trials in this field are not feasible; thus, it is not known whether policies that increase neighborhood walkability would in fact translate into fewer cases of diabetes. The growing enthusiasm among city planners to adopt healthy urban designs provides an opportunity for researchers to study the effects of such natural experiments on diabetes and related diseases. From our research, built environment interventions alone are unlikely to be effective in all populations. This is because a one-size-fits-all solution is unlikely to be sufficient when considering interventions to reach all populations. Further research is needed to understand the causes for the ethnic disparities we observed, including the factors influencing whether people walk in their neighborhoods. Our findings also suggest that the effects of ethnicity differ depending on the context in which people live. Therefore, future research should strive to understand the contextual factors contributing to diabetes risk in high-risk populations to inform built environment policies and more targeted interventions to promote healthier lifestyles in high-risk populations. Urban design interventions could adopt more equitable strategies for building neighborhoods that are livable, walkable, and sustainable which target populations at greatest risk for chronic diseases. Achieving this aim requires collaborations across multiple sectors and levels of government and a greater understanding of the barriers and promotors influencing the adoption of healthy behaviors in high-risk communities.35
Acknowledgments
The authors would like to acknowledge Dr. Mohammad-Reza Rezai for his support ingaining access ICES datasets. As part of the the CArdiovascular HEalth in Ambulatorycare Research Team (CANHEART) database, we also thank Dynacare MedicalLaboratories for providing access to the laboratory data used in the study.
References
Footnotes
Contributors This study was conceptualized and written by GSF and GLB, and RM, AC, and ASB helped in design and review of the manuscript.
Funding Funding for this study was provided by the Canadian Institute for Health Research (CIHR). This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Parts of this material are based on data and information compiled and provided by MOHLTC, Canadian Institute for Health Information and Immigration, Refugees, and Citizenship Canada. GLB is supported by a Clinician Scientist Merit Award from the University of Toronto and received a Heart and Stroke Foundation of Ontario Mid-Career Investigator Award during the tenure of this study. GSF is funded by the CIHR Health Systems Impact Post-Doctoral Fellowship.
Disclaimer None of the funding or sponsoring agencies were involved in the study conception or design, the interpretation of findings, or decision to publish the data. ASB contributed to this article in her personal capacity. The views expressed are her own and do not necessarily represent the views of the Agency for Healthcare Research and Quality or the United States Government. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study received ethics approval from the University of Toronto (Protocol Reference No. 33538) and Institutional Review Board at Sunnybrook Health Sciences Centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data presented in this study are housed at ICES and are not publicly available due to privacy agreements.