Article Text

Abstract
Objective To evaluate overall prevalence and trends of use of any supplements, multivitamins/multiminerals (MVMM), individual vitamins, minerals, and non-vitamin, non-mineral (NVNM) supplements among adults with diabetes in the USA.
Research design and methods We used a nationally representative sample from the National Health and Nutrition Examination Survey collected between 1999 and 2014. Information on supplement use in the preceding 30 days was collected during interview over 8 continuous 2-year waves. To account for the complex sampling design, weighted analyses were conducted among 6688 US adults with diabetes aged 20–85 years and also stratified by age, sex, race/ethnicity, education, comorbidity status, and diabetes duration.
Results Overall, the prevalence of any supplement use (52%–58%; P for trend=0.08) and that of any mineral use (47%–51%; P for trend=0.23) seemed stable over the years studied. Reported use of MVMM slightly decreased from 36% to 32% (P for trend=0.006). Use of any vitamin products significantly increased from 47% to 52% (P for trend=0.03). Use of some individual supplements, especially vitamin D, choline, lycopene, and fish oil supplements, significantly increased, while some vitamins, minerals and NVNM supplements decreased over the years. In addition, the trend of any supplement use varied by age, sex, race/ethnicity, or education, but not by diabetes duration or diabetic comorbidities.
Conclusions Among US patients with diabetes, use of any dietary supplements or any minerals remained stable, while MVMM use slightly decreased and use of any vitamins increased. Additionally, use of several individual supplements varied significantly over the 16-year period studied.
- dietary supplement
- diabetes
- the National Health and Nutrition Examination Survey (NHANES)
- multi-vitamins/multi-minerals (MVMM)
- non-vitamin, non-mineral (NVNM)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- dietary supplement
- diabetes
- the National Health and Nutrition Examination Survey (NHANES)
- multi-vitamins/multi-minerals (MVMM)
- non-vitamin, non-mineral (NVNM)
Significance of this study
What is already known about this subject?
Most of the previous nationwide surveys of dietary supplements have been conducted in the general population or healthy population.
It remains unclear whether trends or patterns of taking dietary supplements would vary among US patients with diabetes.
What are the new findings?
Use of any dietary supplements or any minerals remained stable, while use of multivitamins/multiminerals slightly decreased among US patients with diabetes over the past 16 years between 1999 and 2014.
The trend of any supplement use seemed to vary by age, sex, race/ethnicity, or educational levels.
How might these results change the focus of research or clinical practice?
Our national survey data provide important information for future dietary/nutritional recommendations and/or guidelines for US adults with diabetes.
Introduction
Dietary supplements are often taken by adults in USA to maintain or promote health. Approximately 50% of US adults routinely take dietary supplements and spend billions of dollars annually.1 National surveys have reported that dietary supplement use among US adults remained stable through 1999 to 2012 with an obvious increase between the 1980s and the mid-2000s.1 Older US adults also showed a higher prevalence of dietary supplement use in 2011–2014.2 Meanwhile, a growing body of evidence suggests that increased intake of some dietary supplements, such as omega-3 fatty acids, vitamin D, and lycopene, might be associated with reduced risk of cancer and cardiovascular disease,3 4 which might have motivated the use of supplements.
Due to their relative safety and low cost, dietary supplements such as multivitamins are advocated as an attractive option for preventing chronic diseases, such as cancer, cardiovascular disease, and type 2 diabetes. Type 2 diabetes has been called ‘the epidemic of the 21st century’, given its rising prevalence and increasing healthcare burden in USA and worldwide.5 In particular, complications from diabetes seriously influence the quality of life for patients with diabetes.6 Evidence from basic research has suggested that adequate intake of antioxidant vitamins or minerals may protect against the development of type 2 diabetes via reduction of oxidative stress and its associated metabolic abnormalities, including insulin resistance, pancreatic β-cell insulin secretion, systemic inflammation, endothelial dysfunction, hypertension, and dyslipidemia.7 8 Observational studies have shown that high consumption of some specific nutrients, vitamins, or minerals was associated with decreased incidence of diabetes.9–11 For instance, several systematic reviews and meta-analyses supported a link between adequate vitamin D levels and low risk of type 2 diabetes.12 13 Several lines of experimental evidence supported the potential favorable effects of vitamin D supplementation on glucose and insulin homeostasis as well as other metabolic abnormalities in patients with diabetes.14 Among the non-vitamin, non-mineral (NVNM) supplements, omega-3 fatty acid may decrease C reactive protein concentrations and improve dyslipidemia in patients with diabetes, thereby delaying the development and progression of diabetic complications.15 However, given the lack of conclusive evidence from randomized controlled trials, much controversy exists over the potential yet unproven benefits or risks of any dietary supplement use regarding the development and progression of type 2 diabetes.
Most previous nationwide surveys were conducted in the general population or healthy populations and clearly show the patterns and trends of nutritional supplement use among US adults;1 16 17 however, it is unclear whether such trends or patterns differ among US patients with diabetes. Based on the nationally representative sample of US adults from the National Health and Nutrition Examination Survey (NHANES) with eight continuous 2-year surveys from 1999 to 2014, our study aimed to investigate serial trends in supplement use among US patients with diabetes, including the use of any supplement product and multivitamins/multiminerals, as well as individual vitamins, minerals, and NVNM supplements.
Research design and methods
Study design and data collection
The NHANES is a series of cross-sectional, stratified, multistage surveys representative of the non-institutionalized population in USA. NHANES has assessed the health and nutritional status of both adults and children for several decades. The current NHANES has continuously collected data in 2-year waves since 1999. Survey data were collected both through an in-home interview and a visit to a mobile examination center with direct standardized physical examinations. A standardized questionnaire was given to participants to collect demographic information, such as age, sex, race/ethnicity, and education level. All participants provided written informed consent.
We used NHANES data from 1999 to 2014 to estimate the prevalence and trends in dietary supplement use among US patients with diabetes. The sample size of each survey ranged from 577 to 1089. After we excluded women who were pregnant (because pregnancy affects glucose measurements) (n=1280), participants younger than 20 years old (n=38 140), participants who failed to go to the mobile exam center (n=2134), and subjects without diabetes (n=33 905), there were 6688 patients with diabetes in the analyses.
Definitions of diabetes
During the interview, participants were asked if they have ever been diagnosed with diabetes by a ‘doctor or a health professional’. If the answer was ‘yes’,we defined it as a self-reported previous diagnosis of diabetes. In this study, diabetes is defined if any of the following conditions are met: (1) Previous diagnosis of diabetes. (2) A hemoglobin A1c level of 6.5% (48 mmol/mol) or greater. (3) Fasting plasma glucose level of 126 mg/dL or higher. (4) Any plasma glucose (PG) level of 200 mg/dL or higher. (5) Two-hour PG level of 200 mg/dL. (6) Use of insulin.
Dietary supplement use
During the interview, participants were asked if they had taken any dietary supplements in the last 30 days. The prevalence of supplement use was defined based on this self-reported use in each NHANES wave. Multivitamins/multiminerals (MVMM) was defined as ≥10 vitamins and/or minerals.
Statistical analyses
NHANES is a very complex stratified multistage cross-sectional survey. It oversamples many groups, such as children aged 2 months to 5 years, people older than 60 years, Mexican Americans, and non-Hispanic blacks. All analyses used sample weights and took into account the complex survey design. Categorical variables were presented as weighted percentages and corresponding weighted 95% CIs. Survey-weighted logistic regression was used to calculate p value for linear trend across waves. The linear trend was considered statistically significant at 0.05 based on the two-sided Wald test. Ratios and differences for the comparison of the prevalence of supplement use in 2013–2014 vs 1999–2000 were calculated. A statistically significant decrease corresponded to a ratio <1 (or a difference <0) and p for linear trend <0.05; a significant increase represented a ratio >1 (or a difference >0) and p for linear trend <0.05; and a stable trend represented a p for linear trend ≥0.05.
Overall prevalence of dietary supplements (any supplement, any vitamin, any mineral, MVMM, individual vitamins and minerals as well as NVNM) for each wave of NHANES was also presented. Prevalence for NVNM supplements was not presented due to NHANES analytic guidelines on large relative standard errors (>30%).
We also performed subgroup analyses stratified by age (20–39 years, 40–64 years, and ≥65 years), sex, race/ethnicity (non-Hispanic white, non-Hispanic black, and Mexican American), education level (less than high school, high school and some college, and college or higher), status of comorbidities (yes if patients with diabetes had cardiovascular disease, chronic kidney disease or nephropathy, retinopathy, neuropathy, or cancer), and diabetes duration (<10 years and ≥10 years). All analyses were conducted using SAS, V.9.4 (SAS Institute).
Results
Over the eight continuous 2-year surveys, 6688 patients with diabetes aged over 20 years were identified: 3382 men and 3306 women. Table 1 presents basic population characteristics by use of any dietary supplement among US adults with diabetes. In 1999–2014, 54% of patients with diabetes took any dietary supplements (95% CI 52% to 55%). Approximately 30% of patients aged 20–39 years, 51% of those aged 40–64 years, and 62% of those aged over 65 years took dietary supplements. Female patients were more likely to use dietary supplements than male (57% vs 50%). The highest prevalence of dietary supplement use was among non-Hispanic whites (59%), followed by non-Hispanic blacks (44%), and Mexican Americans (39%). As expected, higher prevalence of supplement use was associated with higher education levels or longer diabetes duration. Additionally, diabetes-related comorbidity status was associated with supplement use (all proportions ≥55%); the highest prevalence of supplement use was 65% among patients with diabetes with cancer, followed by 58% for chronic kidney disease, 56% for cardiovascular disease, and 55% for chronic obstructive pulmonary disease.
Population characteristics of US adults aged 20 years or older with diabetes using any dietary supplements between 1999 and 2014
The prevalence and trends in the use of any supplement, MVMM, any vitamin, and any mineral from 1999 to 2014 are presented in table 2. The use of any dietary supplement seemed to increase from 52% in 1999–2000 to 58% in 2013–2014 but without statistical significance (P for trend=0.08). After excluding MVMM, the increasing trend in any supplement use became statistically significant, rising from 17% to 26% (P for trend <0.0001; difference: 9.7%; 95% CI 3.8% to 16%). MVMM use slightly but statistically significantly decreased from 36% (95% CI 28% to 43%) in 1999–2000 to 32% (95% CI 28% to 36%) in 2013–2014 (P for trend=0.006; difference: −3.6%; 95% CI −12% to 4.4%). Use of any vitamin supplement slightly but significantly increased from 47% to 52% (P for trend=0.03; difference: 5.8%; 95% CI 1.8% to 14%), and the increasing trend remained statistically significant after excluding MVMM (P for trend <0.0001; difference: 9.5%; 95% CI 4.6% to 14%). Use of any mineral seemed relatively stable with a prevalence of 47% in 1999–2000 and 51% in 2013–2014 (P for trend=0.23; difference: 3.7%; 95% CI −3.6% to 11%), and the overall trend remained stable after excluding MVMM (P for trend=0.15) whereas its prevalence of 19% in 2013–2014 was significantly higher than its 13% in 1999–2000 (difference: 5.8%; 95% CI 0.2% to 12%).
Prevalence and trends in the use of any supplement, MVMM, any vitamin, and any mineral supplement among US adults aged 20 years or older with diabetes from 1999 to 2014* †
The prevalence and trends in use of individual vitamins, minerals, and common MVMM components are shown in table 3. Among the individual vitamins considered, the prevalence of vitamin D use notably increased from 34% to 43% between 1999 and 2014 (p for trend=0.001; difference: 9.2%; 95% CI 2.0% to 16%). Use of lycopene supplements among men substantially increased from 2.4% in 1999–2000 to 21% in 2003–2004 and then gradually rose to 27% in 2013–2014 (p for trend <0.0001; difference: 24%; 95% CI 18% to 30%). Of note, the overall prevalence of choline was relatively low (≤4.5%) across the years, with an increase from 2.8% in 1999–2000 to 4.5% in 2013–2014 (p for trend=0.04). The prevalence of vitamin A use among patients with diabetes increased from 32% to 38% from 1999 to 2006, then dropped back in 2007 and remained stable at 32% between 2007 and 2014, which resulted in an overall decreased use (p for trend=0.02; difference: −0.2%; 95% CI −7.9% to 7.6%). Meanwhile, use of B vitamins (except B12) and vitamin E tended to decrease over time with statistical significance. After excluding MVMM and vitamin D, any vitamin use appeared stable over the years (difference: 0.5%; 95% CI −4.7% to 3.7%).
Prevalence and trends in the use of individual vitamins, minerals, and common MVMM components among US adults aged 20 years or older with diabetes from 1999 to 2014* †
Of the mineral supplements taken by patients with diabetes, calcium was the most common over the years, accompanied by magnesium, copper, chromium, selenium, manganese, and zinc (whose prevalence all being 24% or above). About 45% of patients with diabetes used calcium supplements in 2013–2014, although the trends of calcium use were similar between 1999–2000 and 2013–2014 (p for trend=0.18; difference: 2.7%; 95% CI −4.2% to 9.6%). Additionally, use of chromium, copper, manganese, and selenium did not significantly change, while use of boron, iodine, iron, magnesium, molybdenum, phosphorus, potassium, vanadium, and zinc decreased.
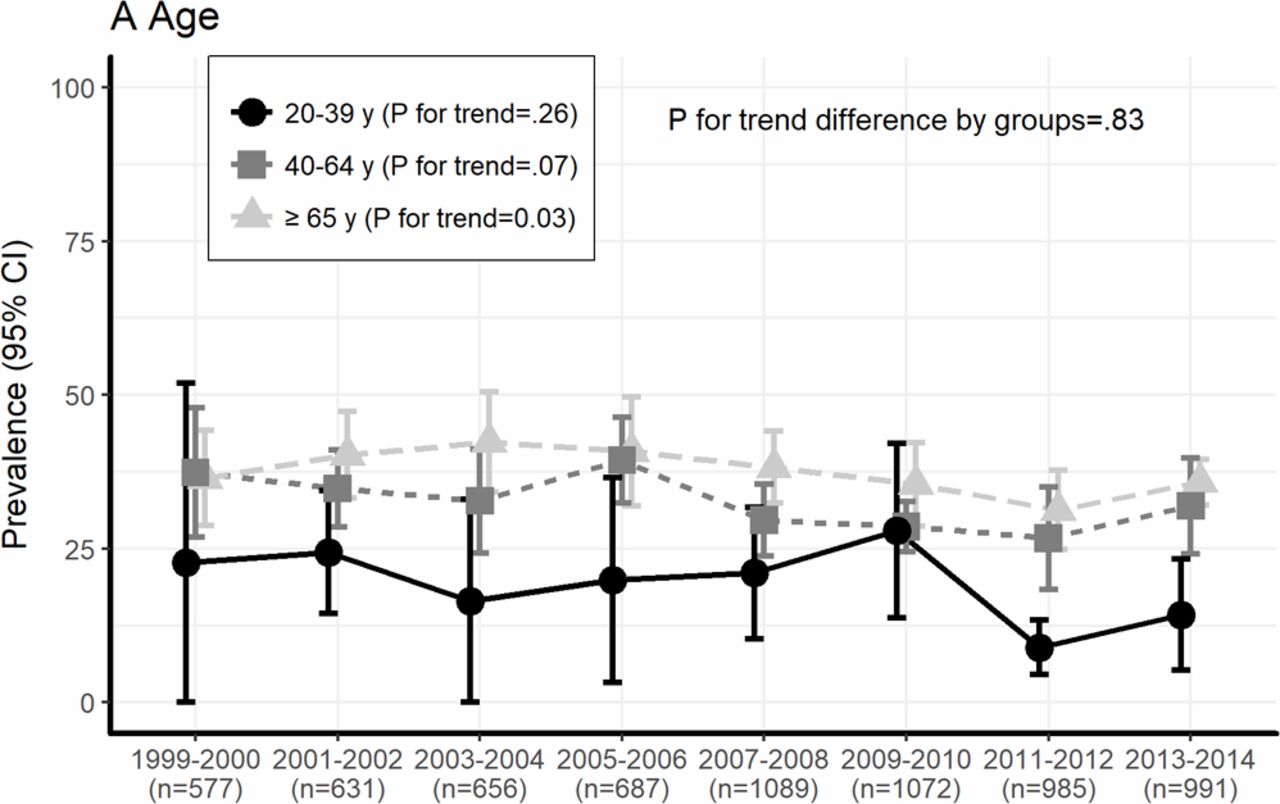
The trends in any supplement use stratified by age, sex, race, education level, comorbidity status, and diabetes duration are shown in figure 1. Prevalence of any supplement use tended to be higher in older patients aged ≥65 years (figure 1A) and in women (figure 1B). The overall prevalence of any supplement use was much higher in patients with higher education (figure 1D). Mexican Americans had the lowest prevalence of any supplement use, and non-Hispanic whites had the highest prevalence (figure 1C). The prevalence in non-Hispanic blacks was as low as that in Mexican Americans between 1999 and 2003, but dramatically increased after 2005–2006 and then became similar to that in non-Hispanic whites between 2009 and 2014 (figure 1C). Trends in any supplement use appeared similar across subgroups stratified by comorbidities (figure 1E) or diabetes duration (figure 1F) from 1999 to 2014.

Trends in any supplement use stratified by age, sex, race, education level, comorbidity status, and diabetes duration in US adults with diabetes aged over 20 years in the National Health and Nutrition Examination Survey (NHANES) 1999–2014.
The use of MVMM showed a decreasing trend among patients aged 20–39 years, especially from 2009–2010 to 2011–2012, while no significant change was observed among those aged 40–64 years or older (figure 2A). Use of MVMM decreased significantly among women, while the use of MVMN remained stable for men (figure 2B). Patients with higher education (≥high school) were more likely to take MVMM compared with those with lower education (<high school) (figure 2D). Use of MVMM decreased significantly since 2005–2006 among non-Hispanic whites and increased among non-Hispanic blacks since 2007–2008, but remained stable among Mexican Americans since 2007–2008 (figure 2C). MVMM use was similar among patients with different comorbidity status or diabetes duration (figure 2E and F).

{kind=link}
{kind=link}
Trends in multivitamins/multiminerals use stratified by age, sex, race, education level, comorbidity status, and diabetes duration in US adults with diabetes aged over 20 years in the National Health and Nutrition Examination Survey (NHANES) 1999–2014.
Use of several NVNM supplements increased over the years of 1999–2014 (online supplementary table S1). Except for fish oil and omega-3 supplements, use of NVNM supplements had very low overall prevalence (≤5%) in general over the years. The use of any omega-3 fatty acid-containing supplements increased almost 18-fold from 0.7% in 1999–2000 to 12.8% in 2013–2014 (p for trend <0.0001; difference: 12.5%; 95% CI 8.6% to 16.4%). Fish oil/eicosapentaenoic acid (EPA)/docosahexaenoic acid (DHA)/docosapentaenoic acid (DPA) supplements were the most commonly used NVNM in 2013–2014, with an average 10-fold increase (difference: 13.4%; 95% CI 8.9% to 17.9%) from 1999 to 2000. Use of omega-6 and omega-9 fatty acid supplements, amino acids, methylsulfonyl-methane, and probiotics use appeared to increase. In addition, use of bilberry, garlic, ginkgo biloba, ginseng, grape seed, para-aminobenzolic acid, quercetin, and soy significantly declined over the years while all others did not significantly change.
Supplemental material
Conclusions
Our study based on the serial NHANES from 1999–2000 to 2013–2014 specifically investigated prevalence and trends in dietary supplement use among US adults with diabetes. Overall, approximately 54% of US adults with diabetes took any dietary supplement between 1999 and 2014. Use of MVMM slightly decreased from 36% in 1999–2000 to 32% in 2013–2014. Use of any vitamin product significantly increased, especially after excluding MVMM, while use of any minerals remained stable over the 16 years studied. Use of some individual supplements, especially vitamin D, lycopene (among men), choline, and fish oil significantly increased while some vitamins, minerals and NVNM supplements decreased over the years. In addition, trends in the use of any supplement or MVMM seemed to vary by age, sex, race/ethnicity, or educational level, but not by diabetes duration or diabetic comorbidities.
The overall prevalence and trends in use of any dietary supplement were similarly stable in both of the US general and diabetic populations. The results from earlier studies among US generally healthy adults showed an increased trend of any supplement use between the 1980s and early 2000s.18 19 A recent survey reported that use of any supplement among US adults from 1999 to 2012 was stable (52%),1 which is almost the same as our finding of overall prevalence of 53% of any dietary supplements among patients with diabetes in 2011–2012. We further explored 2013–2014 data and found a slight increase from 52% in 1999–2000 to 58% in 2013–2014 among US patients with diabetes. The trends in any supplement use varied by age, sex, race, or education level. Any supplement use tended to be higher in older patients (aged ≥65 years), women, patients with higher education, and non-Hispanic whites. The prevalence of any supplement use was becoming similar between non-Hispanic whites and non-Hispanic blacks between 2009 and 2014. Higher socioeconomic status might at least partially explain these race-specific patterns.
The stability of any supplement use might reflect the net balance of the decreased use of MVMM and the increased use of any vitamins. Between 1999 and 2014, the use of MVMM containing ≥10 vitamins and/or minerals slightly decreased from 36% to 32%. The trend in MVMM use varied by age, sex, race/ethnicity, and education, with the highest prevalence of MVMM use among older adults and the lowest prevalence among young adults. The decreasing trend in MVMM use was more apparent among women. Furthermore, use of MVMM seemed to decrease among non-Hispanic whites and those with high school or some college education. Several studies have suggested that the decrease in the use of MVMM was caused by media reports on the unproven health effects of MVMM supplements. Meanwhile, many evidence-based recommendations released by professional organizations did not strongly support the beneficial role of MVMM supplementation in the prevention of chronic diseases.20–22 Further, taking too many supplements might be harmful for human health.23 Additionally, the beneficial effects of MVMM or antioxidant supplements on preventing diabetes or diabetic complication have not been demonstrated by reliable trial data.
Although some experts do not support the role of dietary supplements in preventing and treating diseases,24 suggestive beneficial effects of several antioxidant vitamins have been shown in some clinical trials25 26 and might account for the increased trend of vitamin supplement use among patients with diabetes. Contrary to the decreased use in MVMM over years, use of any vitamin products slightly increased from 47% in 1999–2000 to 52% in 2013–2014. After excluding the use of MVMM, the increase in the prevalence of vitamin product use almost doubled from 11% in 1999–2000 to 20% in 2013–2014. This observation was consistent with the report among generally healthy US adults that the increase in use of any vitamin products1 was due to an increased use in individual or combined vitamins.
In particular, it was worthwhile to note that vitamin D use significantly increased from 34% in 1999–2000 to 43% in 2013–2014.27 Emerging evidence based on systematic review and meta-analysis indicated that vitamin D may be beneficial to patients with diabetes due to its favorable effects on insulin action and secretion as well as other metabolic outcomes.13 28–30 However, recent reports from large-scale randomized controlled trials of the effects of vitamin D supplementation on cardiovascular disease, cancer, and type 2 diabetes have been disappointing.31 32 Solid evidence of the beneficial effects of vitamin D on type 2 diabetes from other well-designed and conducted randomized controlled trials would be expected to have a profound impact on future trends in vitamin D or any vitamin use among healthy individuals or patients with diabetes for health promotion.
The prevalence of lycopene supplements was 24% among male patients with diabetes in 2007–2008, which was similar to 22% in the US healthy male adults in the same time period.1 We also observed significantly increased use of lycopene supplements among male patients with diabetes from 2.4% in 1999 to 27% in 2014, which may have contributed to increased use of any vitamin use among patients. Since it was first reported in 2002 that consumption of lycopene-rich tomato products was associated with reduced risk of prostate cancer,3 use of lycopene supplements became popular among male adults. Lycopene, a plant nutrient with antioxidant properties, might also drive the increased use of lycopene among patients with diabetes.
Despite decreasing trends in almost all B vitamins and MVMM, there was an increasing trend in choline use, especially after 1999 (from 2.8% in 1999–2000 to 4.5% in 2013–2014). Choline is a naturally occurring nutrient present in some foods and available in dietary supplements containing only choline, in combination with B-complex vitamins, and in some MVMM products.33 Previous studies have linked choline status with cardiometabolic disorders, such as hypertension, dyslipidemia, and hyperhomocysteinemia, because dietary choline and other ingredients can be converted to gut microbiota-derived metabolites that have been linked to multiple cardiometabolic outcomes.34 There is currently not enough evidence to support using choline-containing supplements to either prevent or treat diabetes.
The trend of any mineral use remained stable, with 47% of reporting use in 1999–2000 and 51% in 2013–2014, and the trend persisted when limited to non-MVMM supplements, indicating that the use of MVMM did not affect the use of individual minerals. However, there was an upward trend in the prevalence of mineral use between 1999 and 2006 and a downward trend after 2006. Meanwhile, of all surveyed individual minerals, calcium was the most commonly used, with 45% of reporting use among patients with diabetes in 2013–2014. Calcium is critically important for bone health but its effects on cardiometabolic disease have not been demonstrated by large randomized trials. Lately, there is evidence that optimal magnesium-calcium ratio is more important for health. Combined magnesium/calcium supplements have become available; however, there is lack of detailed information on these supplements in NHANES. We observed a decreased change in the prevalence of the use of individual magnesium supplements over the years.
Among NVNM, use of omega-3 fatty acid-containing supplements also increased, accompanied by an increase in fish oil supplements. A growing body of research showing robust reductions in triglycerides and potential beneficial effects on other cardiometabolic traits might have contributed to the increased use of omega-3 fatty acid-containing supplements,4 35–39 although there remains controversy over their long-term beneficial effects in prevention of diabetic complications. Recent systematic reviews and meta-analyses did not support recommendations that patients with diabetes take fish oil supplements. However, whether such updated reviews or ongoing large randomized trials would affect the use of omega-3 fatty acid-containing supplements needs further investigation.
Our study had some strengths. First, we used data from NHANES, a nationally representative sample of US adults. Trends of supplement use were assessed over a 16-year span based on eight continuous 2-year waves of surveys. Second, our study focused on patients with diabetes rather than the general population. Third, information on whether dietary supplements had been taken over the prior 30 days was collected through in-home interviews and verified by seeing the dietary supplement bottles/labels, which has high credibility and could reduce recall bias and improve self-reported data quality. Finally, the large sample sizes allowed us to reliably assess whether the prevalence and trends of supplement use were modified by prespecified factors such as age, sex, race/ethnicity, education, comorbidity status, and diabetes duration.
However, our study also has several limitations. First, although the study consisted of eight cross-sectional surveys, the sample size of each survey was relatively small, and the largest sample size was only 1089 patients, which might have produced sampling error. In particular, large variance may explain the disparate prevalence estimates for the majority of individual supplements with low prevalence (<10%). Second, the study provided information on generic information of dietary supplement use, instead of accurate information on the specific brands or daily intake across eight continuous 2-year waves for all supplements considered in the research. Third, dietary assessment in NHANES investigated if the participants used supplements only in the past 30 days and thus may not accurately reflect long-term dietary supplement use, which might lead to imprecise estimates of annual seasonal changes in the use of supplements. Finally, there is lack of power to examine the prevalence or trend of specific supplements that were less frequently consumed by patients with diabetes.
In conclusion, our study found that among patients with diabetes in USA, use of any dietary supplements or any minerals remained stable, use of MVMM slightly decreased, and use of any vitamins and several individual supplements, such as vitamin D and lycopene, increased between 1999 and 2014. To date, there are no concrete dietary recommendations on the use of vitamin and/or mineral supplements for patients with diabetes due to lack of reliable and robust evidence on the long-term benefits/risks of taking supplements of antioxidant vitamins. All the data from large randomized trials including multivitamin use, vitamin D, and fish oils for primary or secondary prevention of type 2 diabetes have not been published yet and will be very important and informative for future dietary recommendations affecting the trends and patterns of dietary supplement use among patients with diabetes.
References
Footnotes
Presented at Parts of this work were presented in abstract form at EPI|LIFESTYLE 2018 Scientific Sessions, New Orleans, LA, 20–23 March 2018 and ASN Nutrition 2018, Boston, MA, 8–11 June 2018.
Contributors JL and YS researched data. JL, XL and YS wrote the manuscript. JL and XL reviewed/edited the manuscript. WG-M and YS contributed to the discussion and reviewed/edited the manuscript.
Funding This study was supported by the Indiana University Health-Indiana University School of Medicine Strategic Research Initiative Grant (Ms. Jing Li and Dr. Yiqing Song).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All procedures in surveys were approved by the National Center for Health Statistics (NCHS) Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The study’s authors commit to full transparency in this work. To the extent allowed by their institutions’ policies, they will be willing to provide applicable study data, if needed.