Article Text

Abstract
Objective Most patients with type 2 diabetes mellitus (T2DM) also have hypertension and hyperlipidemia. Consequently, they are taking medications for all three conditions concurrently and the effect of one drug could be confounded with that of another. This study aimed to determine the independent effects of 15 commonly prescribed medications for three conditions on the risk of all-cause mortality among elderly patients with T2DM.
Research design and methods A cohort of 360 437 elderly patients with T2DM from 2007 to 2016 US Medicare data was traced along with cumulative uses of 8 diabetes, 6 hypertension and 1 hyperlipidemia drugs. The relative risk of all-cause mortality for each study drug was estimated using an extended Cox regression analysis adjusting for the concurrent use of other study drugs.
Results Compared with the no use of each study medication, mortality risk declined with use of 3 diabetes drugs, sodium-glucose cotransporter-2 inhibitors (HR=0.73; 95% CI 0.64 to 0.84), glucagon-like peptide-1 receptor agonists (HR=0.75; 95% CI 0.70 to 0.80) and dipeptidyl peptidase-4 inhibitors (HR=0.94; 95% CI 0.91 to 0.98), the use of 3 blood pressure medications, diuretics (HR=0.89; 95% CI 0.87 to 0.92), angiotensin receptor blockers (HR=0.86; 95% CI 0.84 to 0.89), ACE inhibitors (HR=0.98; 95% CI 0.95 to 1.01) as well as statins (HR=0.83; 95% CI 0.80 to 0.85). It increased moderately with insulin (HR=1.55; 95% CI 1.51 to 1.59), sulfonylureas (HR=1.16; 95% CI 1.13 to 1.20), a small inconsistent amount with metformin (HR=1.05), beta-blockers (HR=1.07), dihydropyridine calcium-channel blockers (HR=0.99) and non-dihydropyridine calcium-channel blockers (HR=1.05). The use of thiazolidinedione had no effect.
Conclusion Among older patients with diabetes, mortality risk decreased importantly with three new diabetes drugs, 3 blood pressure drugs and statins. It increased moderately with sulfonylurea and insulin. Studies of aggressive use of new T2DM drugs instead of sulfonylureas and insulin are needed. Our statin results empirically validate two national guidelines for using statins in older patients with diabetes. However, 23% of study patients never took a statin, suggesting missed opportunities for prevention.
- cardiovascular drugs
- drug effects
- drug epidemiology
- antidiabetic drugs
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
A majority of patients with type 2 diabetes (T2DM) take metformin, statins and one or more blood pressure medicines.
The studies of the effect of each of these classes on survival exist but are not adjusted for the concurrent use of other drugs.
What are the new findings?
Of T2DM medications, sodium-glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) agonists, were associated with large (by as much as −59%) reductions in mortality risk, but were used by few patients (6% of patients with T2DM in 2017) while insulin and DPP-4 inhibitors which had greater out-of-pocket costs were used by 27.9% and 17.5% of patients with T2DM, respectively.
Among blood pressure medications, diuretics and angiotensin receptor blockers (ARBs) were associated with the largest reductions in mortality risk (up to −29%); so ARBs might be a better choice than ACE inhibitors for elderly patients with T2DM. Statins exhibited the greatest and most consistent mortality risk reduction (as much as −49%). Twenty-three percent of our study population were never prescribed a statin-suggesting a missed opportunity for prevention.
Significance of this study
How might these results change the focus of research or clinical practice?
For management of diabetes in older patients, clinicians might use GLP-1 agonists and SLGT-2 inhibitors more often and sulfonylureas and insulin less often.
For blood pressure control, clinicians might increase their use of diuretics and ARBs.
For hyperlipidemia, they might be more attentive to statin guidelines among the 23% of older patients with diabetes who have never taken them.
More research is needed to determine if less use of insulin and more use of the newer diabetes agents reduces mortality.
Introduction
In 2011, most Medicare enrollees who suffer from type 2 diabetes (T2DM) also suffer from hypertension (91%) and hyperlipidemia (83%).1 Consequently, they may be treated with multiple drugs for these three conditions concurrently. Studies that asses the effect of one or a few of such drugs on survival are available. Studies of effects of such drugs taken concurrently as occurs in real-life practice are needed.
Within its Virtual Research Data Center (VRDC), the US Centers for Medicare and Medicaid Services (CMS) has accumulated 10 years of de-identified enrollee claims records (including visit diagnoses, procedures) vital status and medications dispensed.2 Because diabetes affects 28% of US Medicare beneficiaries, VRDC carries a trove of medication information about patients with diabetes including the prescription date, duration of supply and out-of-pocket costs. We used the VRDC data of senior (aged 65 years or more) patients with diabetes in an extended Cox regression analysis to assess the effect on survival of each of eight classes of T2DM medication, six classes of blood pressure (BP) medications and statins. Here, we report the results of that analysis.
Method
Study population and outcome
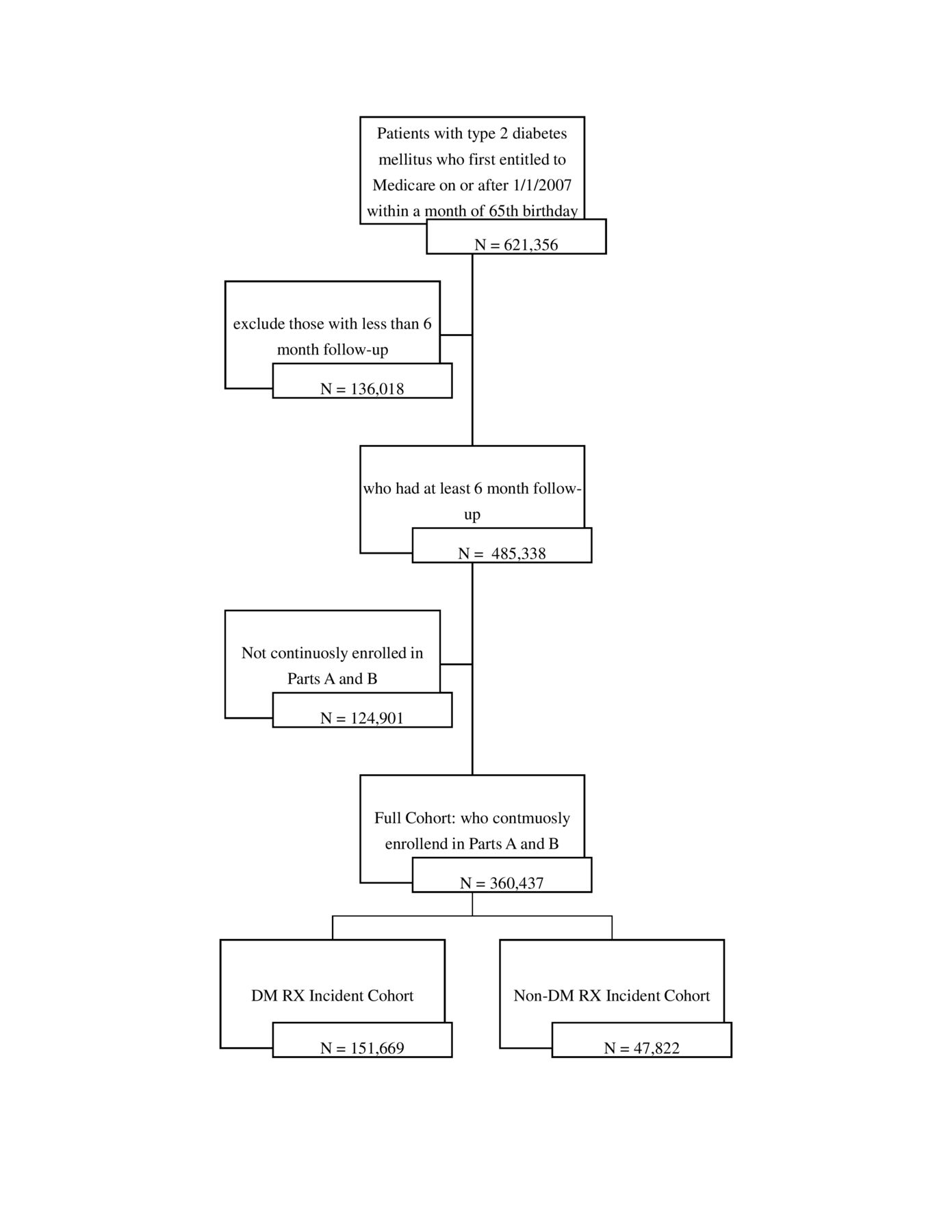
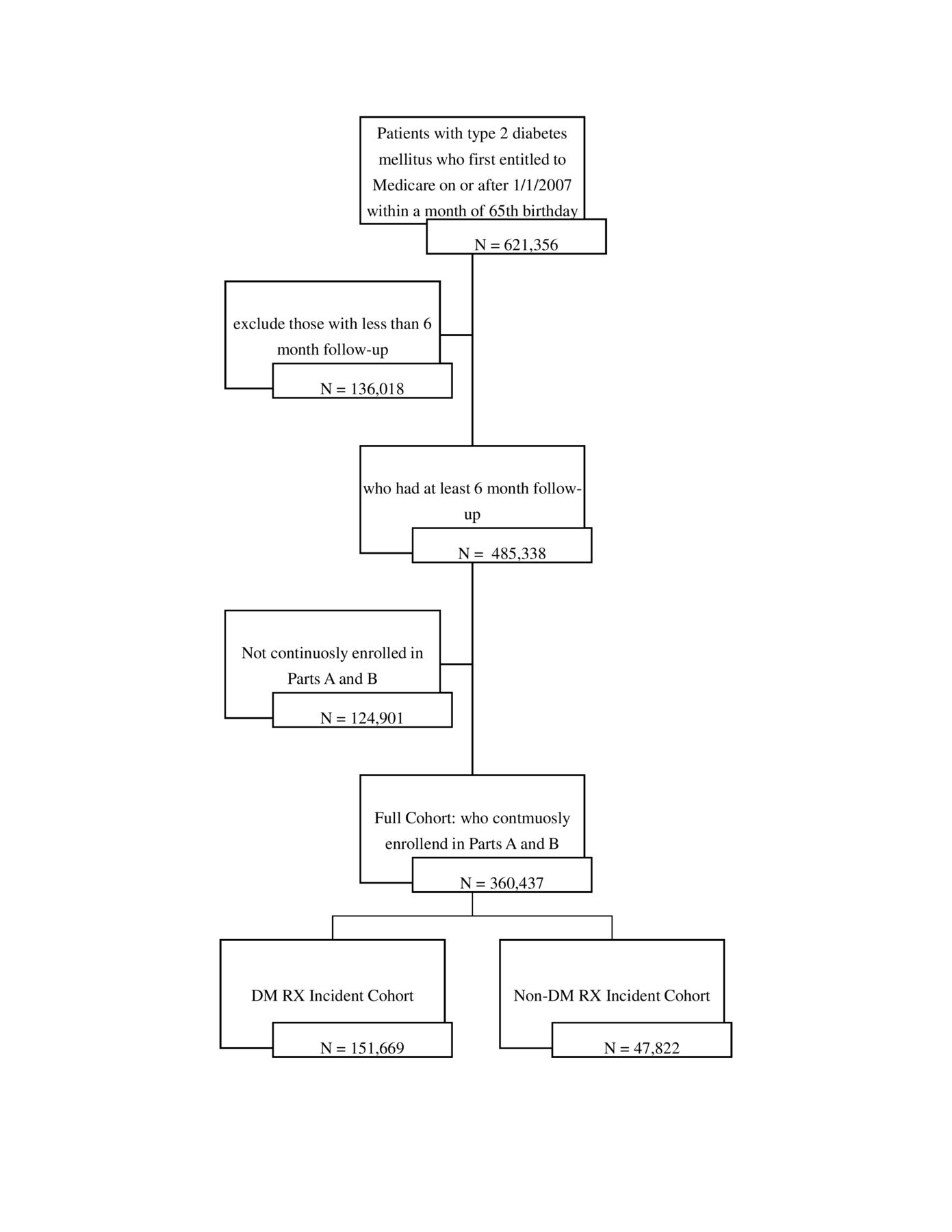
Our initial T2DM cohort came from the 20% random sample of the US Medicare beneficiaries first enrolled in the Medicare on or after 2007 (the first full year of prescription drug coverage (part D) claims availability) and within 1 month of age 65 (779–781 months). We identified the patients with T2DM based on International Classification of Diseases (ICD)-9/ICD-10 codes (250.x0, 250.x2, E11) and included patients with an encounter diagnosis of T2DM after their entry into Medicare. Patients became eligible for the study at the time of their Medicare entitlement/enrollment, but prescription information did not become available until their part D enrollment, which could occur at the time of Medicare entitlement or later. We followed them from their entry to the Part D (while accounting for left truncation3) until their death, switch to a capitated plan, disenrollment from Medicare or 31 December 2016, whichever came first. We excluded patients with <6 months follow-up and those not continuously enrolled in hospital insurances (part A) and medical insurances (part B) to assure we had full access to outpatient and inpatient claims data. To avoid survivor bias from the prevalent drug users, we also analyzed two incident cohorts as described in ‘Statistical analysis’ section. The data were exempted from human subject review by the Office of Human Research Protection at the National Institutes of Health and by the CMS’s Privacy Board.
Descriptive statistics
During the 10 years of observation, secular trends occurred in the use of the study medications. We report the trend and patient’s demographics, socioeconomic status, the prevalence of 43 chronic conditions, the usage, full cost and out-of-pocket costs of each study drug class as well as crude rate of death. We also report the user persistence4 in their use of medications for each drug class.
Statistical analysis
For our primary analysis, we employed an extended Cox regression to explore the independent effect of each study drug on all-cause mortality.5 We adjusted HRs for patient’s characteristics and for concurrent use of any study drug. Patient characteristics included gender, race, degree of low-income subsidy (LIS) (as a surrogate for income), rural residence indicator, calendar year of T2DM diagnosis (to adjust for secular trends) and 43 Medicare chronic conditions6 with >1% prevalence, as an adjustment for overall medical burden. We separated individuals into three groups based on their degree of LIS: 1) dual Medicare/Medicaid eligible whose income is at or below 135% Federal Poverty Line (FPL), 2) non-dual LIS whose income is in 135%–150% FPL and 3) non-dual non-LIS whose income is >150% FPL.7
We considered the effects of 15 different drugs, used to treat T2DM, hypertension and hyperlipidemia, in one analysis because the effect of one drug could be confounded with that of the others. From part D claims, we obtained usage information about eight diabetes drug classes including: metformin, insulin, sulfonylureas, thiazolidinedione (TZD) also called glitazones, glucagon-like peptide-1 receptor agonists (GLP-1a), dipeptidyl peptidase-4 inhibitors (DPP-4i) also called gliptins and sodium-glucose cotransporter-2 inhibitors (SGLT-2i). We grouped five rarely prescribed diabetes drugs (acarbose, miglitol, nateglinide, repaglinide and pramlintide) into one small class. We also included usage information about statins and six of the most common classes of BP medication: thiazide-like diuretics, beta-blockers (BBs), dihydropyridine calcium-channel blockers (DHP CCBs), non-DHP CCBs, ACE inhibitors (ACEIs) and angiotensin receptor blockers (ARBs).
In the diuretic class, we included only thiazides and thiazide-like diuretics (eg, chlorthalidone, indapamide), because they are the ones recommended for BP control. We included BBs as one class, although some subtypes of this classes have indications beyond BP control that might select for sicker patients and included DHP CCBs and non-DHP CCBs as separate class because of their different indications. We assumed patients were using the drug from each prescription dispensing date to the end of supply date. Within drug class, we ignored difference by generic name, and grouped patients by cumulative days of exposure (none, ≤6 months and >6 months) to reduce the risk of non-differential misclassification associated with too simple (yes/no) drug exposure measure.8 In order to minimize the immortal time bias, all drugs and covariates were treated as time-dependent covariates in the Cox regression.9 Only gender, race, and rural residency were time-fixed covariates.
We conducted a series of sensitivity analyses to see if the results held under different conditions. (1) In order to mitigate selection bias toward use of any study drug, we implemented an inverse propensity score weight (IPSW) approach where the propensity score (PS) was the likelihood of receiving any study medication conditional on patient’s characteristics at/before the first T2DM diagnosis.10 (2) To control for survivor bias as can occur in a prevalent cohort,11 we separately analyzed incident cohorts of diabetes and BP/statin drugs by respectively washing out patients who were prescribed study drugs in their first year after part D, while ignoring the data during the same time window of patients not taking study drugs.
Total drug cost and patient out-of-pocket cost
In order to obtain patient total, and out-of-pocket cost per prescription, we used 2017 prescription drug event (PDE) data which only became available after primary analyses were completed. We only included drug costs for non-dual no LIS patients while excluding costs for dual or non-dual LIS patients who have a low income and have a more generous prescription drug benefit beyond the standard part D benefit. Including dual or non-dual LIS patients would distort out-of-pocket costs. The total drug cost is the sum of the ingredient cost, dispensing fee and sale tax and patient out-of-pocket cost includes copayment, coinsurance, deductible or other patient expenditures for the drug. We first divided costs by days of supply and calculated median daily costs per prescription. Then, we multiplied the daily median costs by 365 to obtain a median 1 year cost per prescription in a given class. We also obtained independent prevalence of usage data for patients with T2DM aged ≥65 years, for years of 2017 and 2018 for GLP-1a and SGLT-2i from IBM’s Explorys (courtesy of Cecily Lynch, MD, Accenture).
Results
Secular trends and study population
Between 2007 and 2016 (online supplementary figure 1), the proportion of patients taking five diabetes drugs increased: metformin from 68.2% to 76.5%; insulin from 21.4% to 27.6%; DPP-4i (introduced in 2006) from 4.9% to 17.5%; GLP-1a (introduced in 2005) from 2.8% to 5.8% and SGLT-2i, which was introduced in 2013, from 0.0% to 5.1%. During this same time period, the proportion on sulfonylurea users shrank from 47.1% to 34.9% and that of TZDs plummeted from 29.5% to 7.2% in response to the report of rosiglitazone’s excess, myocardial infarction rate and cardiovascular mortality.12 Based on the commercial database, GLP-1a usage prevalence among older patients with T2DM increased from 5.4% to 6.5% and SGLT-2i from 3.6% to 4.1% between 2017 and 2018.
Supplemental material
Our study patients took drugs from different classes at the same time and in many different combinations reflecting real-world prescribing patterns. Eighty six per cent of our study subjects took two study drug classes simultaneously. The proportion taking three, four or five different classes, simultaneously were 76%, 59% and 38%, respectively, and in all cases, the mean duration of overlapping usage was more than >1 year (data not shown).
From our 20% random sample of part D enrollees, 360 437 (58.0%) patients with T2DM satisfied all of our selection criteria (see cohort diagram figure 1). Starting with part D enrollment, median (IQR) 0 (0–181) days from Medicare entitlement, we followed subjects for a median of 4 years (total 1 587 857 patient years) ranging from 9.3 years of follow-up for the 2007 ‘class’ of enrollees to 1.7 years for the 2015 ‘class’. Follow-up ended when they died (8.0%), switched to a capitated plan (14.1%), dis-enrolled from Medicare (<1%) or reached the end of our study 31 December 2016 (77.9%). The proportions of female, non-Hispanic white and rural resident were 54.0%, 74.8% and 22.4%, respectively. About a quarter of patients received federal/state subsidies: dual 22.3% or non-dual LIS 3.0%. Among the 43 chronic conditions included as covariates, hypertension (91.4%), hyperlipidemia (89.1%) were almost ubiquitous. After these two, cataract (48.7%), anemia (48.7%), rheumatoid arthritis/osteoporosis (48.0%), ischemic heart disease (44.6%), chronic kidney disease (40.7%) and obesity (35.6%) were most common (table 1).
Outcome, medication use and patient characteristics
{kind=link}
Consort diagram. DM, diabetes medications.
Regarding diabetes drugs, the usage rate and median duration of exposure varied from a high of 59.4%, 709 days for metformin to a low of 3.8% and 210 days for SGLT-2i. For BP/statin drugs it ranged from 88.5% and 1098 days for all BP drugs taken together, from 76.6% and 875 days for statins to a low of 33.1% and 686 days for DHP CCBs and 8.6% and 614 days for non-DHP CCBs (table 1).
Primary analyses
Table 2 presents HRs for all covariates in our Cox regression. Being a female, non-white and dual-eligible were associated with lower mortality risk than their comparators shown in table 2 (reference). Being dual-eligible (vs non-dual non-LIS) exhibited better survival perhaps due to the better access to care given their more complete coverage status, despite their lower economic status. Being non-dual LIS and living in rural area had the greatest effects, exhibiting higher mortality risk than their counterparts. As would be expected, heart, kidney, lung diseases, cancers and some mental disorders were associated with higher mortality risk. In the analysis adjusted for economic status, African-American had an HR <1 compared with whites. However, in a separate analysis without the adjustment for economic status, the beneficial effect disappeared, and the mortality risk increased, suggesting that the mortality risk of African-American may be due to economic factors rather than race per se.
HRs of all-cause mortality for each covariate
Diabetes medications
Table 3 column (A) presents marginal adjusted HRs of all-cause mortality for all 15 drugs in our full cohort analysis. Two of the eight diabetes drug classes were associated with impressive reductions in mortality risk: SGLT-2i, by −27% (HR=0.73; 95% CI 0.64 to 0.84) and GLP-1a, by −25% (HR=0.75; 95% CI 0.70 to 0.80) when compared with no use of the drug in question. The risk with use of DPP-4i also declined, but by only, −6% (HR=0.94; 95% CI 0.91 to 0.98). In contrast, insulin, sulfonylureas and metformin were associated with +55% (HR=1.55), +16% (HR=1.16), +5% (HR=1.05) increased mortality risk, respectively. With >6 months of use, the mortality risk of GLP-1a, and DDP-4i in the full cohort analysis declined further reaching −32%, and −11%, respectively. The risk with the remaining diabetes drugs did not change importantly with >6 months of use. (table 4 columns (A), (B) and (C)).
Marginal HRs of all-cause mortality for each drug
HRs of all-cause mortality for each drug by duration of drug exposure
In our analysis with IPSW (table 3 column (B)), SGLT-2i, GLP-1a and DPP-4i continued to exhibit decreased mortality risk and in this analysis, metformin exhibited a significant (−8%) risk reduction. With IPSW, the mortality risk for insulin and sulfonylurea persisted but at a lower level, +40% and +6%, respectively. Neither TZDs, almost all (95%) of which was pioglitazone, nor the small mixed class of ‘other diabetes medications’, showed any significant effect on mortality risk in almost all analyses.
With a 1-year washout to obtain an incident cohort of diabetes drug users, the sample size of diabetes drugs shrank to less than half of the full cohort. Mortality risks were similar to, or lower than, those in the full cohort analysis. The increased risks of insulin (+35%) and sulfonylureas (+16%) persisted. However, the risks for metformin (−9%) and DPP-4i (−13%) improved importantly, and those for GLP-1a (−34%) and SGLT-2i (−59%) improved greatly compared with the full cohort analyses (table 3 column (C)).
BP/Statin medications
In our full primary analysis (table 3 column (A)), the effect of any BP drugs use, exhibited a small, −3% (HR=0.97; 95% CI 0.96 to 0.98) reduction in risk. Among the BP medications, only diuretics (11%) and ARBs (−14%) exhibited significant reductions. However, in our analysis with IPSW (table 3 column (B)), all BP drugs except non-DHP CCBs exhibited decreased risk of mortality, −5% for DHP CCBs, −13% for BB, −16% for ACEI, −17% for diuretics and −23% for ARBs. Non-DHP CCBs exhibited significantly increased risk in both analyses, +5% in the primary analyses and +30% in the analysis with IPSW.
In the primary analysis, with >6 months of use, diuretics and ARBs, both yielded further risk reductions to −14% and −18%, and in with IPWS and >6 months use to, −19% and −25%, respectively. ACEI, which in overall analysis had no significant effect, with >6 months use exhibited a −7% risk reduction in the full cohort analysis and −18% with IPSW (table 4 columns (A) and (B)).
The creation of a 1-year incident/washout cohort for BP/statin drugs reduced the sample size to one-tenth (44,375) of the full cohort. Yet within this incident cohort, BP medication taken as a class, diuretics, ACEI and ARBs exhibited significant risk reductions of −16%, −20% −16% and −29%, respectively. The results for non-DHP CCBs and BBs were not significant in this washout cohort (table 3 column (D)).
Of all study drug classes, statins had the most consistent and always significant effect on mortality risk. In the full cohort analysis, its effect was −17% (HR=0.83; 95% CI 0.80 to 0.85) compared with no use of statin. In the same cohort with >6 months of use, it improved to −23% and with IPSW adjustment the risk reached −35%. In the BP/statin washout incident cohort, risk was −23% (table 3 column (D)). In this same cohort considering the group with >6 months of use (table 4 column (D)), the mortality risk shrank to −49%!
Estimated annual costs for studied drug classes
Online supplementary table 1 presents estimated annual total drug costs and patient’s out-of-pocket costs for the study drug classes. Among diabetes medications, metformin, sulfonylureas and TZD had very low median total drug costs of US$45, US$68 and US$92 per year, respectively. Their corresponding annual out-of-pocket costs were even lower, at US$24, US$31 and US$48, respectively. Such low costs are unlikely to influence treatment decisions. In contrast, the total drug costs of the newer classes of diabetes medications and insulin was very high, with median 1-year total drug costs of US$4358 for DPP-4i, US$4677 for SGLT-2i, US$7462 for GLP-1a and US$4622 for insulin. However, the median Medicare out-of-pocket costs for these classes were only US$500, US$493, US$492 and US$564, respectively, almost one-tenth of the total drug cost. Notably, GLP-1a and SLGT2i which were used by a small (<6%) proportion of patients had median out-of-pocket costs less than that of insulin which was used by almost 30% of study patients.
In general, the BP medications except non-DHP are all at bargains with full drug costs from US$34 to US$88 per year, and out-of-pocket costs of US$20 to US$40 per year, respectively.
Discussion
We assessed the effects of 15 commonly used drug classes on survival among elderly, US Medicare fee-for-service beneficiaries with T2DM. We employed a Cox regression with time-varying covariates to identify the independent effect of each drug while controlling for patient’s characteristics and for concurrent use of any of the other study drugs as is common in real-world practice. Our full cohort of 360 000+ patients, was large enough, and followed long enough, to accommodate our large number of covariates. We also conducted a sensitivity analyses using a propensity score approach to reduce the effect of selection bias toward use of any drug of interest10 and another with a 1-year washout to protect against survivor bias.11 Our study is one of the very few observational studies that assessed concurrent use of multiple drugs to reflect real-world care13 and one of the very largest with a focus on elderly patients with diabetes. We also assessed the prescription costs to find an explanation for the discordance between large survival benefits and the small usage rates of some diabetic drugs.
Among medications for T2DM, insulin exhibited a large, and significant, 55%, increase in mortality. Similar sized increase have previously been observed in association with insulin use.14 15 However, this increase could be explained by selection biases, as insulin is often a last resort choice for patients with difficult to control diabetes. Regardless, formal trials of substituting GLP-1a or SGLT-2i for insulin among patients with T2DM now requiring insulin should be considered for patients with hemoglobin A1c ≤10 to see if these poor outcomes with insulin use could be improved.
Sulfonylureas also exhibited increased mortality risks in our study. Observational studies and a randomized trial have reported the same increased risk of all-cause mortality and cardiovascular mortality.16–18 The proportion of elderly patients with T2DM treated with sulfonylureas decreased by 25% since 2007, which seems an appropriate response to the available data. In the case of metformin, we saw small mortality increases in our primary analyses and moderate decreases in our analysis with IPSW. Our results do not support the speculation that metformin is a medicinal fountain of youth.19 However, it does not provide any reason to quarrel with the treatment guidelines that consistently recommend metformin as the first-line treatment for T2DM.20 It controls glucose levels well, does not induce weight gain and has an excellent safety record.
We observed a decrease in mortality risk with DDP-4i in our primary analyses and a further decrease with >6 months of cumulative usage. Compared with sulfonylureas, it had as strong relative benefit consistent with a previous observational study.21
Pioglitazone does not have the cardiac baggage of rosiglitazone and accounted for almost all (96%) of the TZD use in our study. It exhibited a small decreased mortality risk (−4%) in our analysis with IPWS, concordant with another report.22
In our study, GLP-1a and SGLT-2i were the standouts, exhibiting large and significant decreases in mortality in all analyses adding to existing evidence of their beneficial effects on all-cause mortality.23 24 Given the important improvements in mortality that we and others have observed, the small proportion of patients prescribed these two drugs (around 6% each) based on Medicare data and even less based in commercial medical records database. The low usage rate may be due to concerns about rare reports of the atypical fracture and amputations risk with SGLT-2i25 26 and pancreatitis, pancreatic cancer and thyroid cancer with GLP-1a27 but the evidence that these drugs cause such adverse effect is mixed and/or weak.28 Moreover, the 2019 American Diabetes Association guideline suggests use of one of these two drug classes for non-catabolic patients with T2DM, when metformin alone is not enough, and it does not call out the above-mentioned side effects. However, their recommendations for elderly patients with diabetes are not as strong.20 29 Physician and patient awareness of the fiercely high cash price, that is, a median total drug cost of US$7500 per year for GLP-1a, might explain the low usage. However, the median annual out-of-pocket costs to Medicare patients for either of these two drugs is not high. They cost about US$500 per year which is less than the comparable cost of insulin, and insulin is used in a much larger, 21% of our study population. Physicians may not appreciate how ‘low’ the out-of-pocket costs for these drugs can be for Medicare patients.
Regarding BP medications, thiazide-type diuretics, ARBs and ACEIs exhibited important decreases in mortality risk that improved further with >6 months of use in our primary analysis. The results were similar in our analysis with IPSW and incident cohort analysis. Together, these results accord with national recommendation to use diuretics as the first-line drug for BP treatment30 31 and with reports of beneficial effects of ARBs32 and ACEIs33 among patients with T2DM. Current opinion varies regarding whether ARBs or ACEIs are better for BP treatment in general. Our data hint that ARBs are the better choice for elderly patients with T2DM.
In contrast to diabetes drugs, the BP medications are all bargains, with median total drug cost and out-of-pocket costs below US$76 and US$36/year, respectively in 2017. The annual total drug cost and out-of-pocket cost for non-DHP CCBs were somewhat larger, at US$205 and US$94, respectively.
Our results showed risk reduction for DHP CCBs and risk increases with non-DHP CCBs, probably due to diagnostic bias.34 Both non-DHP and BBs can be prescribed for indications beyond BP control such as arrhythmia, angina, heart failure/attack, which might account for their greater mortality risk.
We saw the largest (between −17% and −39%), and most consistent, reduction in all-cause mortality among patient taking statins. These mortality reductions concord with results of a large meta-analysis showing that statins yielded important survival benefits.35 More recent studies reported similar benefits in an older and non-diabetic population36 37 suggesting that statin’s benefits may apply more broadly. Two respected guidelines advise statin treatment for patients with risk factor of diabetes and age between 40 and 75 years,38 39 and our mortality data indicate that their advice reduces mortality risk at a bargain cost (median out-of-pocket cost of US$40 per year). However, >20% of patients for whom the guidelines recommend the use of statins were never prescribed one. There is room for better statin guidelines adherence.
Our findings are subject to a number of limitations. Most importantly, VRDC database contains no test or measurement results, so we could not adjust for BP measurements, glucose values or other important measurements. Furthermore, our analyses might be exposed to various selection and indication biases toward the use of study drug(s), unadjusted confounders and the other weaknesses common to observational studies. We considered 15 different medications taken in the combinations that occur in real-life practice. Practical and well-vetted methods for developing propensity scores with such large numbers of treatments are lacking; so we implemented an ad hoc approach defining the score as the likelihood of taking any of the study drugs, although with large sample sizes PS may not be necessary.40
In summary, metformin did not exhibit stand-out improvements in mortality risk. SGLT-2i and GLP-1a, and diuretics, ARBs, ACEIs and statins (especially) did exhibit strong and consistent reductions in all-cause mortality risk. The reasons for the slow uptake of two diabetes GLP-1a and SGLT-2i are not clear. Providers may need to be educated about the out-of-pocket costs for these drugs which are similar to insulin and DDP-4 which are used much more widely. Studies are needed to determine whether the use of either of these two drugs as replacements for insulin and sulfonylureas as second-line treatments after metformin will provide equivalent glucose control and better outcomes.
Acknowledgments
The authors would like to thank Dr Cecily Lynch, MD—Accenture for providing estimate of GLP-1 and SGLT-2 usage prevalence for 2017 and 2018 from IBM’s Explorys.
References
Footnotes
Contributors Both authors contributed to the study conception, design, analysis and interpretation, critical review of study content, manuscript drafting, approval of the final manuscript.
Funding This study is supported by the Intramural Research Program of the National Library of Medicine, National Institutes of Health.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The data were exempted from human subject review by the Office of Human Research Protection at the National Institutes of Health and by the CMS’s Privacy Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Data belong to the US Centers for Medicare and Medicaid Services (CMS) and can be accessed only through its Virtual Research Data Center (VRDC). Original data are not available. Data from statistical analyses are available on reasonable requests.