Article Text

Abstract
Objective Vitamin K has proposed beneficial effects on cardiovascular health. We investigated whether serum vitamin K1 was associated with prevalence of microangiopathy and/or macroangiopathy.
Research design and methods Serum vitamin K was quantified in 3239 individuals with and 3808 without diabetes enrolled in Vejle Diabetes Biobank (2007–2010). Each individual was assessed for microangiography and macroangiopathy at enrollment based on registered diagnoses in the Danish National Patient Registry according to the International Classification of Disease 8 (1977–1993) and 10 (since 1994). Using multinomial logistic regression, relative risk ratios (RRRs) were calculated within each group of individuals with and without diabetes. RRRs were estimated for microangiopathic/macroangiopathic status compared with individuals without complications as a function of 1 nmol/L increments in K1. Adjustment for potential confounders was also performed.
Results Vitamin K1 (median) varied 0.86–0.95 nmol/L depending on diabetes, microangiopathic and macroangiopathic status. In individuals with diabetes, the crude RRR for only having microangiopathy was 1.05 (95% CI 0.98 to 1.12) and was found significant when adjusting 1.10 (95% CI 1.01 to 1.19). RRR for having only macroangiopathy was 0.89 (95% CI 0.77 to 1.03) and was again significant when adjusting 0.79 (95% CI 0.66 to 0.96). In individuals without diabetes, adjustments again led to similar estimates that was not significant. The adjusted RRR for having only macroangiopathy was 1.08 (95% CI 0.98 to 1.19).
Conclusions Serum vitamin K1 levels were associated with microangiopathic and macroangiopathic status in individuals with diabetes, but considered of no clinical relevance. The clinical value of other candidate markers for vitamin K status needs to be evaluated in future studies.
- microangiopathy
- macroangiopathy
- vitamins
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Evidence supports beneficial effects of vitamin K on cardiovascular health.
What are the new findings?
Serum vitamin K1 does not serve as a biomarker for microangiopathic and/or macroangiopathic disease status.
How might these results change the focus of research or clinical practice?
Other candidate markers for vitamin K status need to be evaluated in future studies.
Introduction
A growing body of evidence supports beneficial effects of vitamin K on cardiovascular health.1–4 This may be particularly important for certain high-risk groups. As an example, low plasma vitamin K1 has been demonstrated to be associated with an increased risk of cardiovascular diseases (CVDs) in individuals treated for hypertension whereas this association with CVD could not be found in those not treated for hypertension.5 6
The vitamin Ks are a family of very fat-soluble molecules, and vitamin K1 (phylloquinone) is the most abundant form in the Western diet, mainly found in green leafy vegetables and some vegetable oils.6 7 In addition to K1, the vitamin K family also includes vitamin K2. The vitamin K2s are further subdivided, MK-n, with n indicating the number of prenyl units in the side chain. Moreover, there are several vitamin K–dependent proteins, like for example undercarboxylated osteocalcin or undercarboxylated-dephosphorylated-matrix Gla protein that also might serve as biomarker for vitamin K status.
Vitamin K is thought to exert a protective effect on CVD by reducing vascular calcification, through its function as a cofactor in the carboxylation of MGP, an inhibitor of vascular calcification. Carboxylated MGP is capable of chelating calcium and thereby preventing calcium phosphate crystals from forming precipitate on the fibrous elements.7 This formation of crystals is normally enhanced by glycosylation of lipoproteins and increased oxidative stress seen in individuals with diabetes.8 Individuals with diabetes are known to be predisposed to atherosclerosis and to have an increased morbidity and mortality mainly due to CVD.9 Thus, these individuals might be especially susceptible to insufficient vitamin K status in relation to the development of atherosclerosis,1 and identification of individuals with insufficient vitamin K status may be used to identify high-risk groups. It has previously been described how biomarkers of CVD contribute to risk prediction in individuals with diabetes.10 Vitamin K1 is one of the predominant forms of vitamin K in blood and serum concentration of vitamin K1 could potentially serve as an indicator of vitamin K status.11
Results of studies of the association between arterial calcification and serum vitamin K1 have been inconsistent,12 13 and methods of measure vary: some measure vitamin K status using food questionnaires and others measure vitamin K1 concentration directly in the blood, but with too low sensitivity. In addition, no studies have described effects of vitamin K1 on cardiovascular health in individuals with diabetes.
The present study aimed to determine the association between serum vitamin K1 level and the presence of microangiopathic or macroangiopathic diseases in both individuals with and without diabetes, using a newly validated in-house developed highly sensitive liquid chromatography–tandem mass spectrometry (LC-MS/MS) method for measuring serum vitamin K1.14
Research and design methods
Study population and samples
The present study was based on serum samples from individuals with diabetes and age-matched and gender-matched individuals, enrolled in the Vejle Diabetes Biobank (ie, individuals without diabetes were divided into 10-year age intervals and gender matched to the diabetes population, subsequently randomly selected). All participants were Caucasians between 25 and 75 years of age, as of the date per December 31, 2006. A total of 3320 individuals with diabetes (599 with type 1 diabetes and 2721 with type 2 diabetes) and 4255 without diabetes were included in the biobank. Samples were collected during 2007 through 2010. Participants were asked to live and eat as usual 3 days prior to their appointment for entering the biobank and to fast overnight from 22:00 the evening before. Blood sampling took place between 7:15 and 9:30 and serum samples were separated, aliquoted and subsequently stored at –80°C until analysis. Details on the Vejle Diabetes Biobank has previously been described in detail.15 All available samples made up the study population for this study, which in total were 7047 individuals; respectively 3239 individuals with and 3808 without diabetes.
Danish registers
In Denmark, all citizens are assigned a unique 10-digit civil personal register number by which they are registered in the Danish Civil Registration System.16
The Danish National Patient Register contains information on all inpatient and outpatient contacts in Danish hospitals since 1977 and 1995, respectively. The diagnosis information in the register is coded according to the International Classification of Disease (ICD) system 8 (1977–1993) and 10 (since 1994).17 The civil personal register number assigned to all individuals in Denmark were used to link the vitamin K1 results to each participant in the Vejle Biobank.
Definition of microangiopathic and/or macroangiopathic diseases
The existence of microangiopathic and/or macroangiopathic disease when enrolled in the Vejle Diabetes Biobank was based on diagnostic codes (ICD-8 and ICD-10) assigned in the Danish National Patient Register from January 1, 1977 to December 31, 2016. Online supplementary table S1 includes a full list and definitions of microangiopathic and/or macroangiopathic diseases used for this assessment. A pre-defined list from the Diabetes Impact Study of all the codes of diagnoses, treatments and interventions qualifying for the diagnosis of diabetes and related complications was primarily used when making the list in online supplementary table S1.18
Supplemental material
The following categories were used: “No micro- or macroangiopathy”, “Only microangiopathy”, “Only macroangiopathy”, “Micro- & macroangiopathy” and “Unspecific”, respectively (figure 1). Individuals could have one or more registered diagnosis qualifying for the “Micro- & macroangiopathy” group. They could for instances have one microangiopathic and one macroangiopathic diagnosis or a single operational code that qualified as both microangiopathic and macroangiopathic disease, that is, for a type of amputation. Individuals in the “Unspecified group” had one or more diabetes-related diagnosis not specified and therefore impossible to assign any of the other categories.
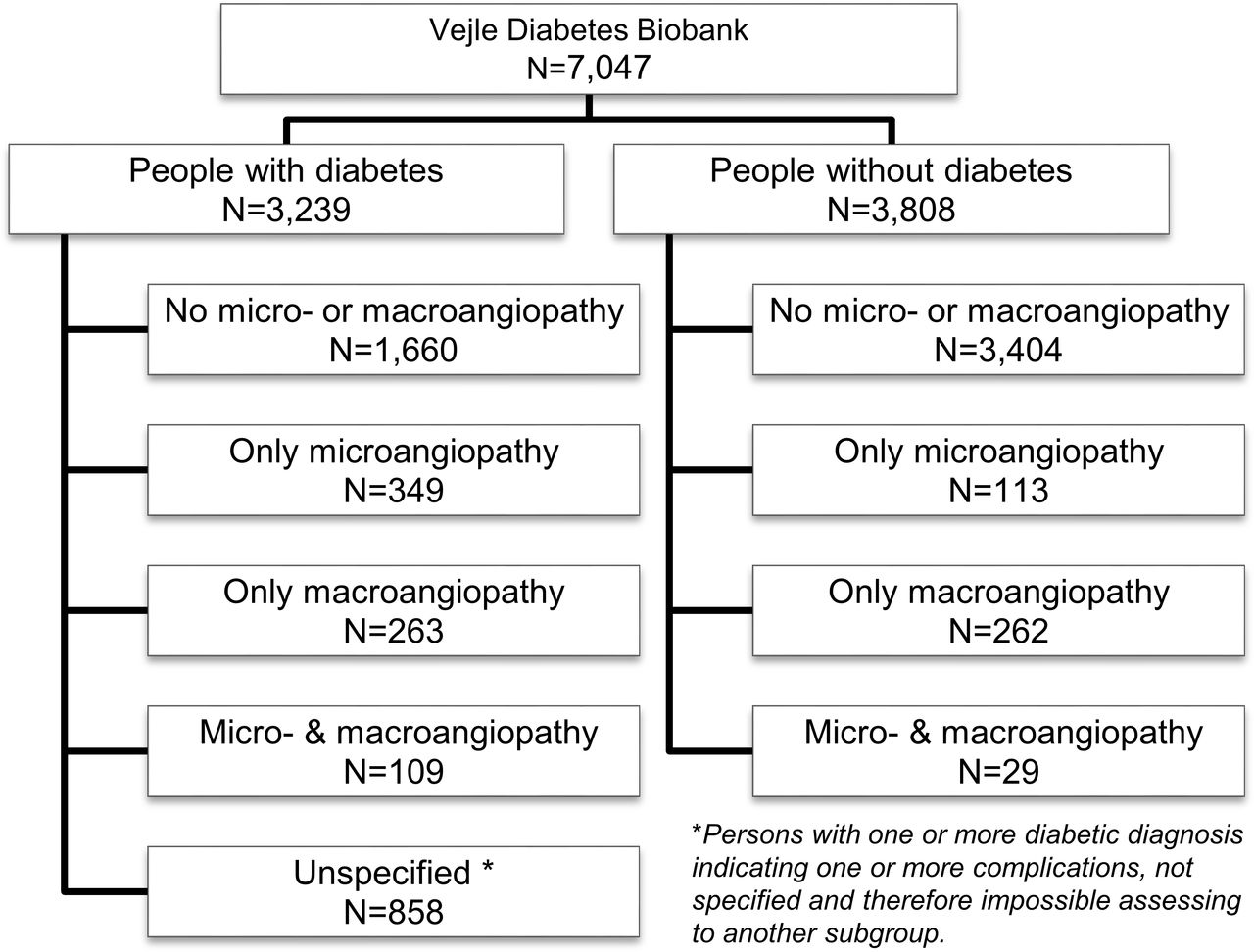
Study population. Subgroups were formed based on the existence of microangiopathic and macroangiopathic diagnoses.
Vitamin K1
An in-house developed, automated and highly sensitive LC-MS/MS method was used for measuring serum vitamin K1. The method has been thoroughly validated and described in detail.14 It has a limit of quantitation of 0.05 nmol/L. The samples were analyzed between June 2018 and February 2019.
Other covariates
Potential confounders were selected a priori for cardiovascular and lifestyle risk factors known from existing literature and clinically plausible criteria.6 19 Included variables were age at enrollment, body mass index, blood pressure (systolic), low-density lipoprotein, triglycerides, HbA1c, estimated glomerular filtration rate, gender (male/female), waist:hip ratio (under cut-off/above; cut-off: ≥0.90 (male); ≥0.85 (female)20), smoking (current, former, never), alcohol consumption (below/above recommended maximum weekly consumption in Denmark (limit for women 14, men 21 units (12 g pure alcohol)), exercise (yes/no, self-reported), lipid-lowering drugs (yes/no), platelet inhibitor treatment (yes/no), vitamin K antagonist treatment (yes/no) and comorbidity (malabsorption: Crohn’s disease (diagnosis DK50), Ulcerative colitis (diagnosis DK51), Intestinal malabsorption (diagnosis DK90) within 10 years before enrollment (yes/no)).
Statistical analysis
We described the study population by anthropometrics, lifestyle factors and previous diagnosis according to microangiopathic and macroangiopathic status stratified by diabetes status. Baseline characteristics were reported by median (25th–75th quartiles) or as number (%) of subjects. We compared disease status by Kruskal-Wallis test. Here, the same categories of the individuals with and without diabetes were compared (eg, no microangiopathy and macroangiopathy vs no microangiopathy and macroangiopathy), as were the “no micro- & macroangiopathy” category to each of the microangiopathy and macroangiopathy categories within the same diabetes status.
We used the serum vitamin K1 as a continuous variable for the following multinomial logistic analyses.
To estimate relative risk ratios (RRRs), we have used multinomial logistic regression which assumes independent observations and linearity for continuous explanatory variables but that does not assume an underlying Gaussian distribution for neither outcome variables nor residuals. RRRs were estimated within the group of individuals with and without diabetes, respectively: RRRs were estimated for microangiopathic/macroangiopathic status with no complications as a function of 1-unit (nmol/L) increments in K1 values. Adjustments were made for potential confounding variables stratified by diabetes status.
We performed sensitivity analyses on the following groups from the cohort (analysis performed on a total of N individuals with/without diabetes, respectively): (1) individuals not in lipid-lowering treatment (N: 929/3110), (2) individuals in lipid-lowering treatment (N: 2193/589), (3) individuals not in vitamin K antagonist treatment (N: 2975/3638) and (4) individuals not in platelet inhibitor treatment (N: 1708/3289). We also performed the analysis on the full cohort (5) adding an adjustment variable for platelet inhibitors (N: 3239/3808) and (6) adjusting for platelet inhibitors and interaction between platelet inhibitors and vitamin K1 (N: 3239/3808).
Statistical tests were two tailed, and the significance level was set at 5%.
All statistical analyses were conducted in Stata/SE V.15.0 for Windows (version 2017; StataCorp LLC, College Station, TX, USA).
Results
Participants
All results are presented for individuals with and without diabetes separately. The baseline characteristics according to microangiopathic/macroangiopathic status for the study populations are presented in table 1.
Baseline characteristics of individuals with and without diabetes
The prevalence of individuals registered with only microangiopathy was almost fourfold higher in the group with diabetes compared with the group without diabetes, in total 349 (11%) and 113 (3%) individuals, respectively. The same did not apply to individuals registered with only macroangiopathy, where similar prevalence of 263 (8%) for individuals with diabetes and 262 (7%) without diabetes was found.
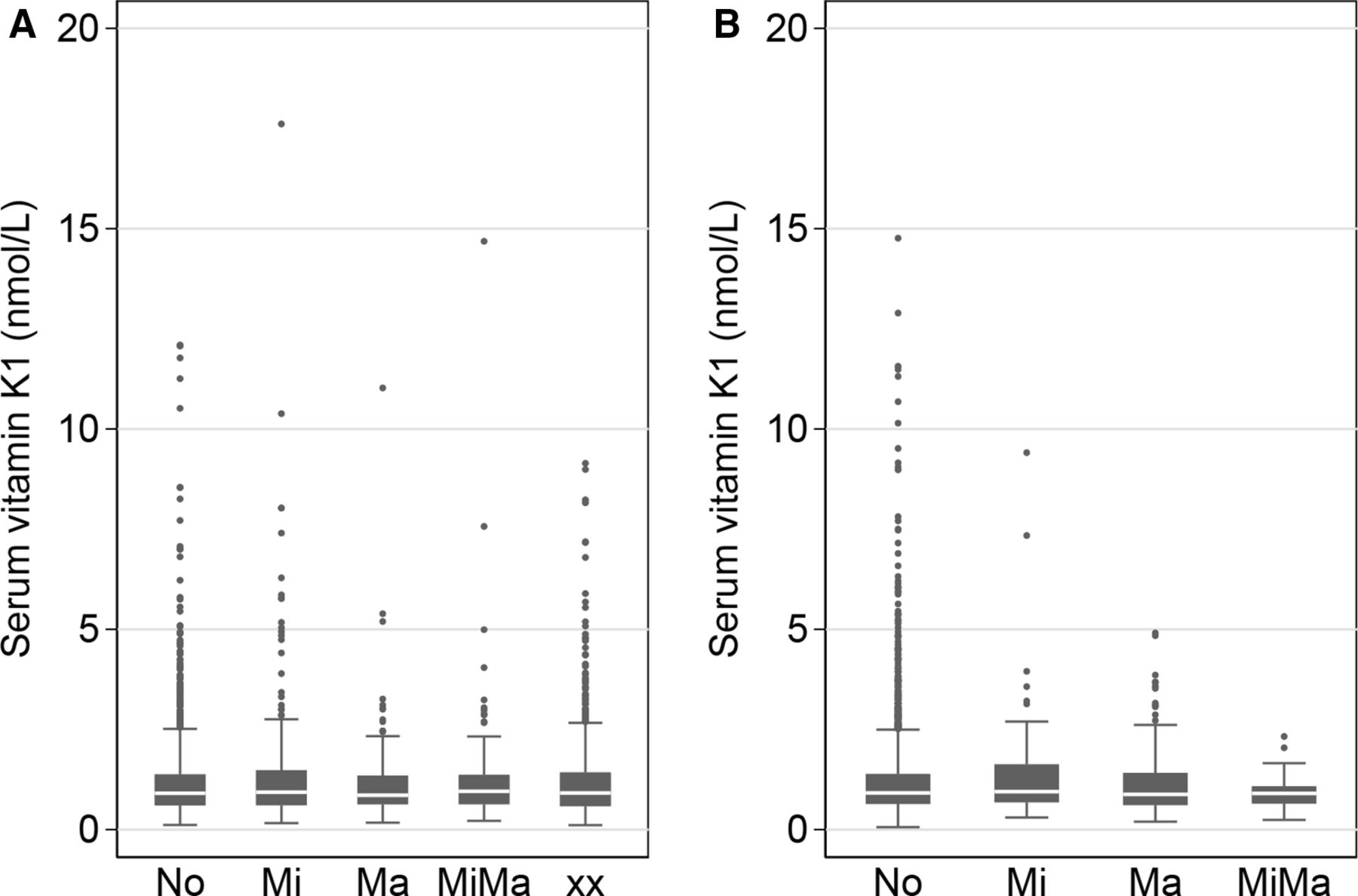
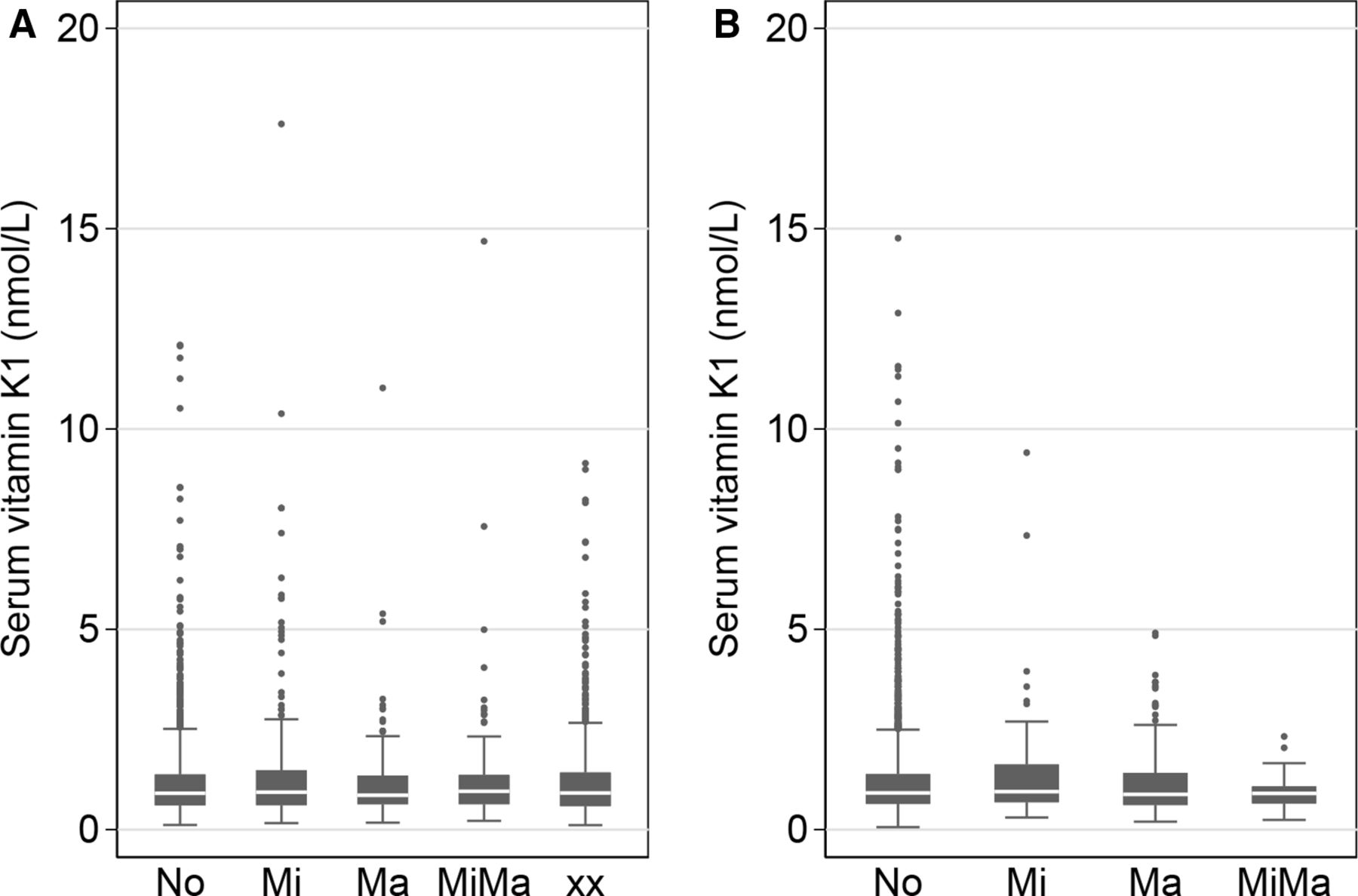
We found similar vitamin K1 levels for both individuals with and without diabetes with median serum vitamin K1 levels varying from 0.86 to 0.95 nmol/L between all the categories (both in respect to diabetes status and microangiopathic and/or macroangiopathic status).
Figure 2 illustrates the median and variation in serum vitamin K1 according to microangiopathic and/or macroangiopathic status. Examination of the difference between the categories showed no significant difference between any of the categories compared.
{kind=link}
{kind=link}
Serum vitamin K1 in relation to diabetes and microangiopathic and macroangiopathic disease status. Serum vitamin K1 depicted graphically for each category for both individuals (A) with and (B) without diabetes. Differences between categories were examined by Kruskal-Wallis test, but none were found statistically different. Two outliers are left out due to very high level. No=no microangiopathy or macroangiopathy, Mi=only microangiopathy, Ma=only macroangiopathy, MiMa=microangiopathy and macroangiopathy, xx=unspecified.
Main association results
In individuals with diabetes, the crude RRR for only microangiopathic status increased 5% (RRR 1.05, 95% CI 0.98 to 1.12) for each increase in serum vitamin K1 (unit nmol/L) (table 2). Crude estimates for the “Micro- & macroangiopathy” and “Unspecified” categories were similar hereto. For the association between serum vitamin K1 and macroangiopathy, we found a RRR of 0.89 (95% CI 0.77 to 1.03).
RRR (95% CI, p value) of serum vitamin K1 status with microangiopathic and macroangiopathic status among individuals with and without diabetes
Mutual adjustments for all categories led to similar estimates, where the only significant estimates were RRR for having only microangiopathy or only macroangiopathy. The RRR for having only macroangiopathy changed the most to 0.79 (95% CI 0.66 to 0.96).
In individuals without diabetes, the crude RRR for only microangiopathic status increased 3% (RRR 1.03; 95% CI 0.96 to 1.11) for each increase in serum vitamin K1 (unit nmol/L) (table 2). Crude estimates for only macroangiopathic status was similar hereto. For the association between serum vitamin K1 and “Micro- & macroangiopathy” category, we found a RRR of 0.63 (95% CI 0.33 to 1.20). Mutual adjustments for all categories led to similar estimates.
The results from the sensitivity analysis are shown in online supplementary tables 2 and 3.
All the sensitivity analyses showed consistent results with the main analysis.
Conclusions
In this cohort of 3239 individuals with diabetes and 3808 without diabetes, we found the median serum vitamin K1 concentration varied from 0.86 to 0.95 nmol/L depending on diabetes status and microangiopathic and/or macroangiopathic status (table 1). For individuals with diabetes, there were indications that the serum vitamin K1 level was associated to microangiopathic and macroangiopathic disease status, though the impact of the vitamin K1 was low and therefore do not indicate that serum vitamin K1 level is useful as a marker of microangiopathic and/or macroangiopathic disease status.
The main strength of the study is that the serum vitamin K1 has been determined with the most sensitive method available at present in a large study population of individuals with and without diabetes, respectively. The Danish National Patient Register is a nationwide register containing information on all hospital contacts in Denmark, and due to the publicly funded healthcare system, it includes all inhabitants thereby minimizing risk of missing information.17 Being able to link these information to the extensive register of Vejle Diabetes Biobank containing rich information on anthropometric and lifestyle is a major strength of this study.
Several limitations need to be addressed. The major limitation of the study is that it still needs to be clarified whether vitamin K1 is the right/best biomarker for vitamin K status. In addition to vitamin K1, the vitamin K family also includes vitamin K2. The vitamin K2s are further subdivided, MK-n, with n indicating the number of prenyl units in the side chain. Thus, a range of different subtypes of vitamin K2, as MK7 and MK4, are also candidates to provide information regarding vitamin K status. Moreover, there are several vitamin K–dependent proteins, like for example undercarboxylated osteocalcin or undercarboxylated-dephosphorylated-matrix Gla protein that also might serve as biomarkers for vitamin K status. An additional limitation might be that we only had a single measurement of serum vitamin K1 and thus any information on day-to-day variation is missing. Serum vitamin K1 is known to be affected by the dietary intake of the vitamin,12 which may therefore change relatively quickly if the diet is altered. The half-life of vitamin K1 has previously been reported to be 1–2 hours, reaching baseline level again 8 hours after intake.21 For this reason, we used fasting blood samples as has been recommended previously.12 Vitamin K1 is mainly found in food that would be considered healthy. Hence, the lack of adjustment for dietary habits is a limitation. A generally healthier dietary lifestyle could be associated with less microangiopathic and/or macroangiopathic disease and not the vitamin K1 itself, even when statistical adjustment of other health factors like exercise and smoking have been made. On the other side, individuals with diabetes and microvascular and/or macrovascular disease could also have made dietary changes eating more vitamin K1 after getting their diagnosis thereby at enrollment in Vejle Diabetes Biobank being higher in vitamin K1 than before their diagnosis. This would be blurring any potential beneficial effect of vitamin K1 on development of calcification. This could be a residual confounder explaining why we generally see no large differences between our crude and adjusted models.
By using the pre-defined list from the Diabetes Impact Study,18 we have not included diagnosis codes used for peripheral arterial disease and hence potentially misclassifying some individuals that should have been assessed with macroangiopathic disease, though the list do include the operational and interventional codes. Moreover, despite the extensive information we have on the study population from The Danish National Patient Register, we may still miss some diagnoses given by general practitioner. This may introduce a bias, but the individuals who are most sick are seen in the hospitals and therefore have diagnoses in the Danish National Patient Register. When we do not see any strong correlations in individuals that are sickest, we do not expect to see anything in the other individuals either.
Ideally, individuals with and without diabetes should have been assessed equally for the presence of microangiopathy and/or macroangiopathy. The practice of using the unspecific complication code in connection with diabetes codes forced us to establish a fifth group exclusively for individuals with diabetes. The extent to which this unbalanced assessment has induced bias is unknown, though when comparing the estimates of the Unspecified category to the others, they seem convincing.
No other studies have investigated the vitamin K1 status by measuring the serum vitamin K1 concentration directly in individuals with diabetes in relation to microangiopathic and/or macroangiopathic disease. By measuring the indirect biomarker dephosphorylated uncarboxylated matrix Gla protein (dp-ucMGP), it has previously been suggested that a poor vitamin K status could be associated with increased CVD risk among patients with type 2 diabetes.1 There can be several explanations for the different results between the studies. First is the discrepancy between study design, with a difference in disease outcome and way of qualifying for disease. Second, the vitamin K status was quantified differently. The vitamin Ks are a family of structurally similar vitamins that may differ physiologically22 23 and if investigating subtypes of vitamin K2, for example, MK7 and MK4, results might have been different. Moreover, as mentioned previously, vitamin K1 has a relatively short half-life21; therefore, the way vitamin K1 has been quantified is important, for example, in relation to fasting prior to blood sampling.
Previous studies using food questionnaires have reported a beneficial role of vitamin K1 in glucose homeostasis24 as well as a reduced risk of development of type 2 diabetes.25 Also, hyperglycemia is a risk factor for microangiopathic and macroangiopathic complications.26 Since we did not find indications of serum vitamin K1 being strongly associated with neither diabetes status nor microangiopathic and/or macroangiopathic disease status, it is irrelevant to investigate further the predictive value of serum vitamin K1 in these contexts. In conclusion, our findings support that vitamin K1 status was associated to microangiopathic and macroangiopathic disease status in individuals with diabetes, although the impact of vitamin K1 was low and considered clinically insignificant. Serum vitamin K1 is not useful as biomarker of microangiopathic and/or macroangiopathic disease status in this cohort study. Still, other markers for vitamin K status might show clinical value as biomarkers for CVD status which needs to be evaluated in future studies.
Acknowledgments
First we would like acknowledge T. Hansen and O. Pedersen from the Novo Nordisk Foundation Center for Basic Metabolic Research, Section of Metabolic Genetics, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark and C. K. Christensen from the Department of Internal Medicine and Endocrinology, Lillebaelt Hospital Hospital, Vejle, Denmark for the design and establishment of Vejle Diabetes Biobank, which we benefited from in this study. In addition, we would like to thank people from our laboratory at Lillebaelt Hospital, Vejle, Denmark; biomedical laboratory technician M. S. Alameddine for great support, pharmacist M. Bergmann and biomedical laboratory technicians S. Egsgaard and P. N. Rank Gottlieb for assistance during the quantitation of vitamin K1 in the biobank samples. Finally, we would like to thank biostatistician S. Möller from OPEN—Open Patient data Explorative Network, Odense, Denmark for statistical support.
References
Footnotes
Contributors All contributors meet the criteria for authorship and are listed in the manuscript. IBA, CLB, AG, MB and JSM conceived and designed the study. Vitamin K1 analysis was carried out by IBA, HN and AS. Data management was done by MS and IBA. Statistical analysis, interpretation and first draft of the manuscript were prepared by IBA. IBA, CLB, MB, AG, IB and JSM revised the manuscript for intellectual content and all authors approved the manuscript for submission. JSM is the guarantor of the study.
Funding This work was supported by Department of Regional Health Research, The Faculty of Health Science, The University of Southern Denmark (SDU), Denmark and Region of Southern Denmark who each granted a 1-year PhD scholarship. The last year of PhD salary was funded by KEJ Fond, Copenhagen, Denmark.
Disclaimer The research did not receive any specific grant from funding agencies in the commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Danish Data Protection Agency (J. no. 2006-53-1385, J. no. 16/13707, J. no 16/28063) and ethical approved by The National Committee on Health Research Ethics and The Regional Committees on Health Research Ethics for Southern Denmark in Denmark (J. no. 2008-58-0035; additional protocol for this project: project-ID S-20080097, authorization no. 44010). All blood samples and data were handled anonymously.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.