Article Text

Abstract
Objective We sought to compare the association of categorized ankle–brachial index (ABI) with mortality and complications of diabetes in persons with no symptoms of peripheral arterial disease (PAD) and in primary cardiovascular disease prevention.
Research design and methods This is a retrospective cohort study of persons with type 2 diabetes aged 35–85 years, from 2006 to 2011. Data were obtained from the Sistema d'Informació per al Desenvolupament de la Investigació en Atenció Primària (SIDIAPQ). Participants had an ABI measurement that was classified into six categories. For each category of ABI, we assessed the incidence of mortality; macrovascular complications of diabetes: acute myocardial infarction (AMI), ischemic stroke, and a composite of these two; and microvascular complications of this metabolic condition: nephropathy, retinopathy, and neuropathy. We also estimated the HRs for these outcomes by ABI category using Cox proportional hazards models.
Results Data from 34 689 persons with type 2 diabetes were included. The mean age was 66.2; 51.5% were men; and the median follow-up was 6.0 years. The outcome with the highest incidence was nephropathy, with 24.4 cases per 1000 person-years in the reference category of 1.1≤ABI≤1.3. The incidences in this category for mortality and AMI were 15.4 and 4.1, respectively. In the Cox models, low ABI was associated with increased risk and was significant from ABI lower than 0.9; below this level, the risk kept increasing steeply. High ABI (over 1.3) was also associated with significant increased risk for most outcomes.
Conclusions The studied categories of ABI were associated with different risks of type 2 diabetes complications in persons asymptomatic for PAD, who were in primary cardiovascular prevention. These findings could be useful to optimize preventive interventions according to the ABI category in this population.
- peripheral arterial disease
- vascular complications
- electronic patient records
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
The diabetic condition has been associated with microvascular complications and with increased cardiovascular risk. The latter has been related to the presence of peripheral arterial disease, indicated by low ankle–brachial index (ABI), a non-invasive, inexpensive test that is recommended to screen persons with diabetes. In these persons, the ABI has also been associated with increased risk when its values are high.
What are the new findings?
Our study allows comparison of various categories of ABI, including low and high values, regarding the incidence of mortality, macrovascular, and microvascular complications in persons with diabetes. We found the risk of these outcomes was similar or lower in persons with high ABI compared with those in the category immediately under the pathological threshold of 0.7≤ABI<0.9, and the risk increased notably as the ABI decreased.
How might these results change the focus of research or clinical practice?
The ABI has not been sufficiently used in persons with diabetes mellitus. These findings emphasize the usefulness of the ABI to screen persons with diabetes, specifying their risk of mortality, and of macrovascular and microvascular complications. The binary division of persons between low ABI or not-low ABI may be insufficient to identify persons at different risks of future events. A more detailed classification could personalize the intensity of preventive recommendations and treatments according to different risk categories.
INTRODUCTION
Diabetes is a disorder of the glucose metabolism that affects the macrovascular and microvascular systems, and thus, prevention of its associated complications is essential. The association of glycemia with microvascular damage is more established than the relation with macrovascular disease,1 2 but the latter has also been evidenced.3 Moreover, the increased cardiovascular risk in persons with diabetes is especially pronounced in persons with poor metabolic control,4 5 longer duration of diabetes,6 or low ankle–brachial index (ABI).7 The ABI is considered a risk modifier to refine risk stratification,8–10 especially in women,11 and also in persons with diabetes.10
The ABI is a measurement of the arterial health status of the lower extremities relative to the upper extremities. When performed by trained health professionals, it is an inexpensive first test to evaluate the presence of asymptomatic peripheral arterial disease (PAD), indicated by ABI values of <0.9. Most persons with PAD are asymptomatic, which is particularly concerning because their associated cardiovascular risk is as high as in symptomatic cases.12 Thus, this is a silent condition associated not only with leg symptom deterioration but also with risk in other arterial territories.13
In persons with diabetes, low ABI has been associated with mortality and cardiovascular outcomes, but its relation with other complications has had limited attention. Additionally, some studies have examined the risk of both high and low ABI values, but the association of the degree of arterial impairment (obstruction or pathological constriction) with complications has been hardly addressed,14 especially regarding microvascular complications. Even more, previous reports in persons with asymptomatic PAD included patients with previous cardiovascular events,15 16 but primary prevention is of particular importance in persons with diabetes, because the occurrence of a first cardiovascular event is associated with increased morbidity and mortality in these persons, compared with the population without diabetes.10 Accordingly, we sought to evaluate the association of categorized ABI with mortality, cardiovascular outcomes, and microvascular complications in patients with diabetes in primary cardiovascular prevention.
RESEARCH DESIGN AND METHODS
Data source
We analysed a subset of records from the System for the Development of Research in Primary Care (SIDIAP) database, which gathers anonymized longitudinal information of persons from the primary care services in a structured way so it can be reliably used for research. The information includes demographic data, clinical diagnoses coded using the International Classification of Diseases, 10th Revision (ICD-10), referral and hospital discharge information coded using International Classification of Diseases, Ninth Revision (ICD-9), laboratory tests, and medications (drug prescriptions and drug invoicing at any community pharmacy). SIDIAP covers 80% of the Catalan population, comprising 274 primary care practices and 1365 general practitioners (GPs) and nurses throughout Catalonia, managed by the Catalan Institute of Health. A subset of this database is restricted to information from GPs and nurses who met predefined quality standards in recording and composes SIDIAPQ, the database we have used for this study. SIDIAPQ includes information on nearly 2 million patients and 20 million person-years for the period 2005–2015. The quality and representativeness of these data regarding geographical, age, and sex distributions have been documented,17 particularly for cardiovascular risk factors and cardiovascular diseases,18 and have been applied to previous epidemiological reports.19–21
Study design and participants
We carried out a retrospective cohort study including persons with ABI aged 35–85 at the time of study entry who suffered from type 2 diabetes mellitus. Diabetes was defined using either the diagnosis of diabetes (codes from E11 and E14 categories and the corresponding subdivisions in the ICD-10, and 250 and subdivisions in the ICD-9) or the treatment with drugs used in diabetes (a10 code in the Anatomical Therapeutic Chemical Classification System). Exclusion criteria applied to persons with type 1 diabetes; individuals with ABI equal or higher than 3; persons with symptomatic PAD, defined as follows: (1) any symptom of intermittent claudication in the attending physician’s notes, detected by thorough review of the uncoded information in SIDIAPQ; (2) an ABI of <0.4, even in the absence of any suggestive symptom; (3) an invoicing of any drug related to intermittent claudication (cilostazol, pentoxifylline, buflomedil, or naftidrofuryl); and persons with previous cardiovascular disease, which included acute myocardial infarction (AMI), angina, stroke, and transient ischemic attack. These persons with previous macrovascular disease were excluded because they would be in secondary prevention of cardiovascular disease, and we aimed to assess the incidence of mortality and complications of diabetes mellitus in a population in primary prevention.
The recruitment period ran from January 2006 through December 2011. Study entry was defined by the first ABI measurement, and the follow-up extended until the first date of the occurrence of an outcome, transference out of the SIDIAPQ, or end of study period, in December 2015.
Exposure, outcomes, and covariates
ABI was measured following the standardized protocol from the primary care services.22 This protocol explains that the systolic blood pressure (SBP) has to be measured in each ankle right above the malleoli and in each arm using Doppler probes. Two measurements are obtained in each ankle, one from the the dorsalis pedis and another one from the posterior tibial artery. The two higher values are divided by the higher of the brachial SBPs, and the lower of these defines the ABI.23 ABI levels defined exposure, categorized as follows: 0.4≤ABI<0.5, 0.5≤ABI<0.7, 0.7≤ABI<0.9, 0.9≤ABI<1.1, 1.1≤ABI<1.3, and 1.3≤ABI. We presented the ABI values in categories because previous reports showed a J shape in the relation of ABI with mortality8 24 and hypothesized that a similar distribution might occur with other outcomes.25 Instead of the subdivisions of the ABI values by ranges of 0.1, we merged some categories to ensure enough number of participants in each group. However, we used more categories than in other studies26 to observe potential differences within the low ABI values.
We studied the following outcomes: mortality, macrovascular complications of diabetes, and microvascular complications. Macrovascular complications of diabetes were defined by the incidence of AMI, ischemic stroke, and major cardiovascular event (MCE), which was a composite of these two; microvascular complications were defined by incident nephropathy, retinopathy, or neuropathy. Participants who had suffered a microvascular event previous to baseline were excluded when examining that particular outcome during follow-up.
We used the following covariates to describe the population and to adjust the potential association of the ABI categories with mortality and complications of diabetes27 28: age, sex, smoking habit, body mass index (BMI) calculated as weight divided by squared height, SBP, diastolic blood pressure (DBP), pulse pressure, total serum cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, glycated hemoglobin (HbA1c), glucose, diabetes duration, comorbidities (hypertension, atrial fibrillation, heart failure, chronic obstructive pulmonary disease, and malignant neoplasms), and medications (antidiabetic therapy, diuretics, beta-blocking agents, calcium channel blockers, agents acting on the renin–angiotensin system, other lipid modifying agents, and aspirin). Continuous variables were considered up to 1 year previous to study entry, and categorical variables were present if they were recorded in the database previous to study entry. Each outcome and covariates were defined using the corresponding ICD-10 codes from the primary care settings, and/or the ICD-9 codes from referrals and hospital discharges. All covariates and diagnoses are routinely collected following the protocols to standardize data recording.29
Statistical analysis
Continuous variables were presented as mean (SD) or as median (first and third quartiles), and categorical variables as counts (percentages). We used multiple imputation by chained equations to impute the missing values of BMI, SBP and DBP, pulse pressure, total cholesterol, LDL cholesterol and HDL cholesterol, triglycerides, HbA1c, and glucose because excluding participants with missing values may incur a selection bias.30 We used the fraction of missing information to estimate the number of necessary imputations at 10, with 50 iterations per imputation.31 Given the characteristics of the study population, the missing-at-random assumption was plausible.
We estimated the raw new incidence of diabetes mellitus complications in each category of ABI using Poisson models. Cox proportional hazards models were used to estimate adjusted HRs between categories of ABI. The proportionality of hazards assumption was examined.32 The candidate variables for adjustment were based on the literature, and a backward–forward selection method based on Bayesian Information Criterion was used to build the final model.
All analysis were carried out using R-software33 V.3.5.1 (R Foundation for Statistical Computing, Vienna, Austria); the MICE V.2.15 package was used for multiple imputation.34 The datasets generated during and/or analyzed during the current study are not publicly available due to legal reasons related to data privacy protection. No applicable resources were generated or analyzed during the current study.
RESULTS
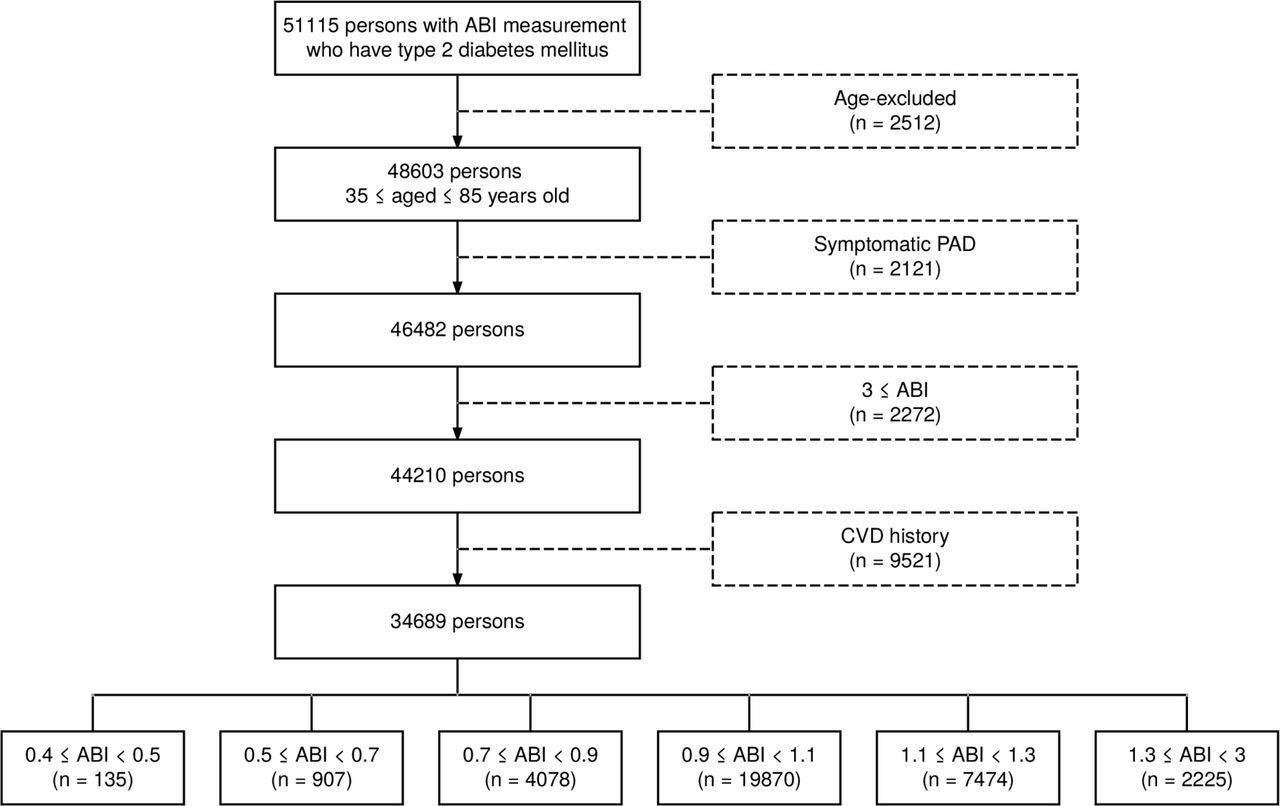
From an initial population with type 2 diabetes and an ABI measurement at the recruitment period of 51 115 persons, 48 603 were aged between 35 and 85 years old; after the exclusion criteria were applied, data regarding 34 689 persons remained for analysis (figure 1). The median (first–third quartile) follow-up was 6.0 (95% CI 4.8–7.5) years, and 532 (1.5%) participants were lost to follow-up, due to transfer out of the SIDIAPQ database. The maximum percentage of missing values was 27.3% for LDL cholesterol (online supplementary table S1). A detailed count of the missing values for each variable is shown in online supplementary table S1, along with the baseline characteristics of the overall population, comparing the imputed and the complete-cases dataset.
Supplemental material

Study flowchart. ABI, ankle–brachial index; CVD, cardiovascular disease; PAD, peripheral arterial disease.
The mean age of the study population was 66.2 (SD 10.5) years old; 17 880 (51.5%) were men (online supplementary table S1); 5120 (14.7%) had ABI values lower than 0.9; 2225 (6.4%) had ABI values of ≥1.3 (table 1). The mean age, pulse pressure, diabetes duration, and the percentage of comorbidities and treatments considered tended to increase as the ABI decreased and in the group with high ABI (≥1.3) (table 1).
Baseline characteristics of the study population
A general trend was observed in the incidences by ABI of all outcomes: they followed a J-shaped curve with the lowest rates in patients with normal ABI (1.1≤ABI<1.3) (table 2). Regarding macrovascular complications, the incidence of ischemic stroke doubled that of AMI; it was 7.7 (95% CI 7.0 to 8.6) and 4.1 (95% CI 3.6 to 4.7) per 1000 person-years, respectively, in the group with normal ABI (1.1≤ABI<1.3). As for the microvascular complications, neuropathy presented the lowest incidence of 3.4 (95% CI 2.9 to 4.0) per 1000 person-years in the category with normal ABI; slightly higher was the incidence of retinopathy, and nephropathy had a markedly higher incidence: 24.4 (95% CI 22.9 to 25.9) per 1000 person-years in the above-mentioned category. In fact, the incidence of nephropathy was the highest of all outcomes, even higher than all-cause mortality, in all the ABI categories.
Events and incidence rate* (95% CI) for diabetes mellitus complications and mortality by ABI categories
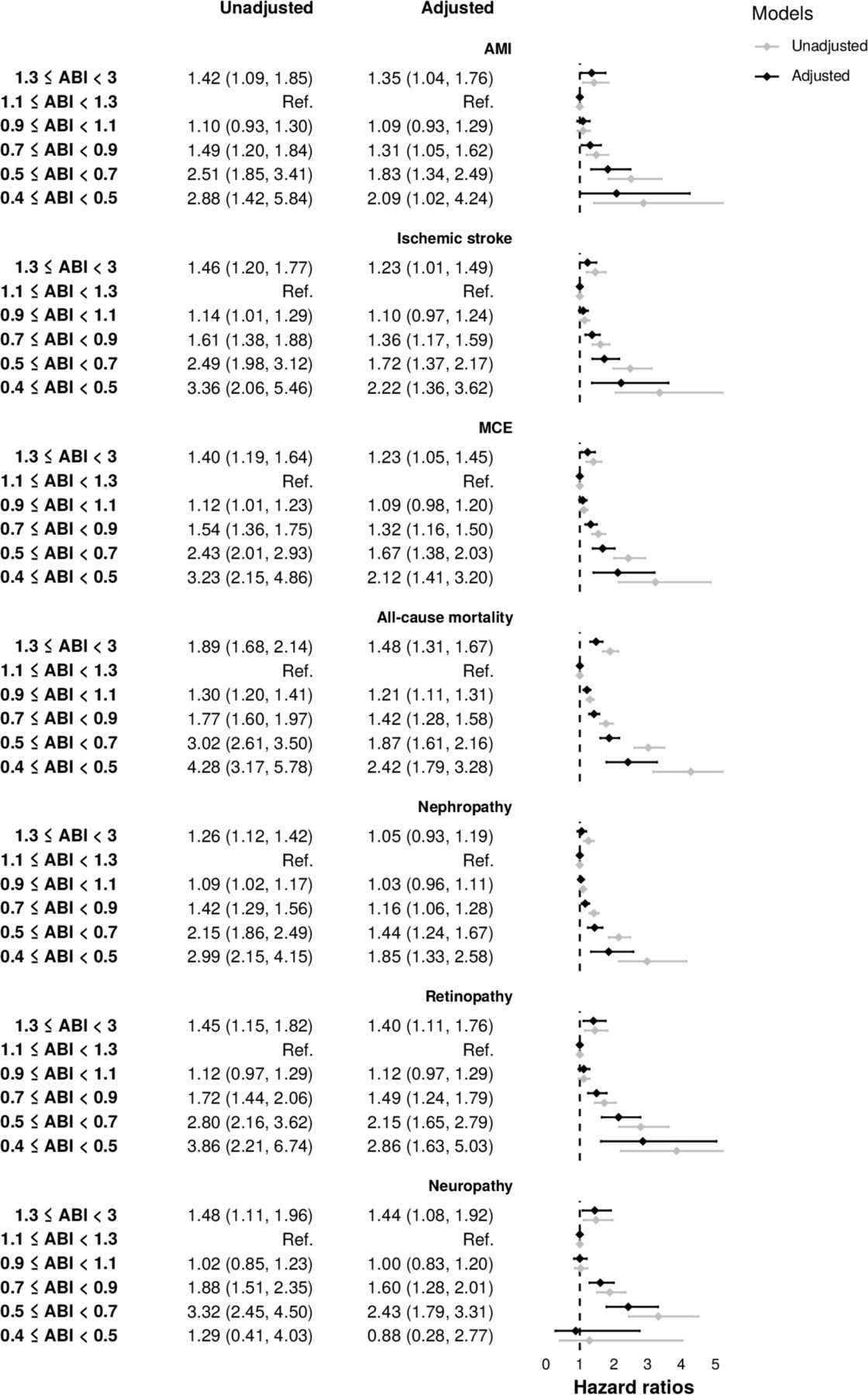
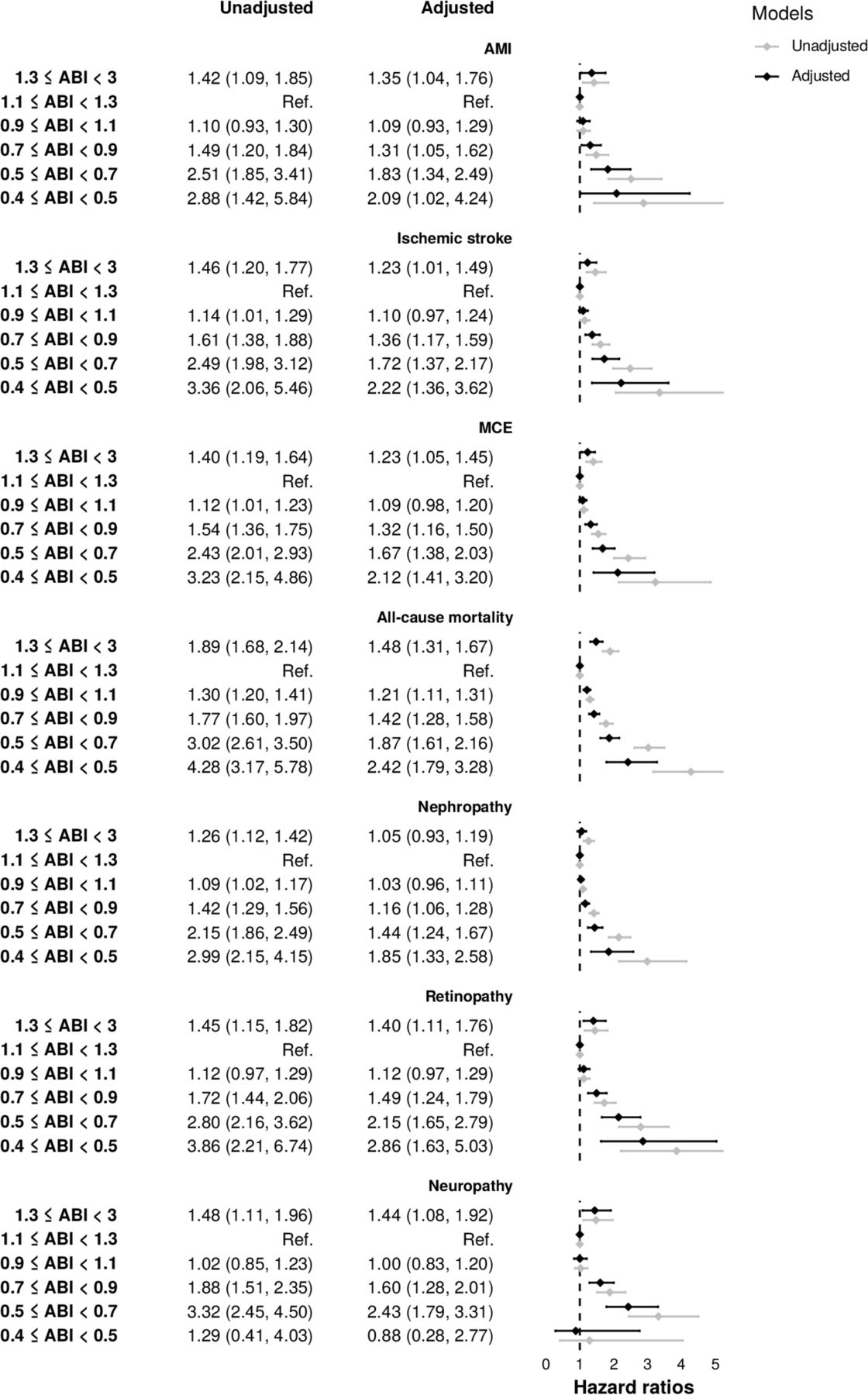
A general J-shaped trend for all the studied outcomes was also observed regarding the HRs of the ABI categories (figure 2). The reference category was the group with 1.1≤ABI<1.3. The group with high ABI (≥1.3) was significantly associated with most outcomes and presented similar or lower HRs than the group with 0.7≤ABI<0.9, depending on the outcome, whereas the groups with ABI<0.7 had a significant and marked increment in the HRs that kept increasing steeply with the decrease of ABI.
{kind=link}
{kind=link}
HRs for each outcome by ankle–brachial index categories. ABI, ankle–brachial index; AMI, acute myocardial infarction; MCE, major cardiovascular event; Ref., reference.
By outcome, the significance of the HRs for macrovascular complications of diabetes was similar in most ABI categories. Mortality was the only outcome with which the category of 0.9≤ABI<1.1 presented a significant association. Regarding microvascular complications, two exceptions showed lack of significance, for the association of the 1.3≤ABI group with nephropathy (while it was significant for the rest of microvascular outcomes) and of the 0.4≤ABI<0.5 group with neuropathy. Online supplementary table S2 details the variables selected by Bayesian Information Criterion to optimize the adjustment of the Cox models for each outcome. Online supplementary figure 1 shows the Kaplan-Meier curves for these models. The unadjusted HRs for each outcome are included in figure 2.
The results of the analysis of complete cases were similar to those with the imputed dataset. These analyses comprised descriptions of the population by ABI categories (online supplementary table S3), incidence rates (online supplementary table S4), and HRs by ABI categories and for each outcome (online supplementary figure S2).
DISCUSSION
In longitudinal studies in patients with diabetes, graded low ABI has only been analyzed as a risk factor for mortality (all-cause mortality or cardiovascular mortality)35–37; to our knowledge, its relation with macrovascular and microvascular complications has not been previously addressed (even though the association of graded ABI with microvascular complications has been examined in cross-sectional studies).38–40 We studied persons with diabetes mellitus, categorizing their ABI levels within ABI<0.9 and including the contribution of high ABI. These ABI categories were associated with different incidence of mortality; macrovascular complications of diabetes: AMI, ischemic stroke, and a composite of these two; and microvascular complications: nephropathy, retinopathy, and neuropathy.
The relation of ABI with the occurrence of mortality and vascular complications of diabetes presented a J-shaped form. The risk of such outcomes was increased in the low ABI categories and kept increasing as the ABI diminished. These different incidences within the low ABI categories summon the consideration of specific recommendations for patients in each ABI level and different intensities of preventive measures. Thus, the binary division of persons between low ABI or not-low ABI may be insufficient to identify persons at different risks of future events.41 The group with high ABI (≥1.3) also presented an increased risk of the outcomes, similar to that of the group with 0.7≤ABI<0.9 for AMI, all-cause mortality, and retinopathy. In persons with diabetes, therefore, preventive recommendations in these two groups could be similar, although the incidence in persons with 0.7≤ABI<0.9 was higher for ischemic stroke, nephropathy, and neuropathy.
Additional to the analysis of an array of ABI categories, the study population—with diabetes, no symptoms of PAD, and no previous cardiovascular disease—was another highlight in our report. Only two previous longitudinal analysis evaluated persons with asymptomatic PAD, like in our study, but they included persons at higher risk, for example, with previous coronary artery disease,15 or with cerebrovascular disease15 16; furthermore, they did not specify subcategories within low ABI nor did they examine the effect of high ABI levels. The association of ABI with mortality and with macrovascular and microvascular complications of diabetes has not been previously analyzed in persons with diabetes, asymptomatic for PAD, and in primary prevention. This population is particularly important because they may be at the initial stages of the arterial damage (depending on their ABI category), and thus patient-tailored preventative measures could be implemented to avoid further arterial damage and MCEs.
The presence of high ABI values in patients with diabetes has been related to medial calcinosis42 that coexists with occlusive PAD in 50% of cases.42 43 Thus, patients with high ABI in our study likely suffered from various degrees of occlusive PAD additional to medial arterial calcification. The scarcity of hypothesis to explain the consequences of medial arterial calcification include myocardial remodelling, which could contribute to a chronic increase of the ventricular after-load.44 This mechanism might be independent of the presence of occlusive PAD,44 additional, or even synergistic with it in patients with diabetes.26 Further studies to clarify the pathways through which high ABI could increase the risk of complications in patients with diabetes would be of interest.
Direct comparison of our findings with other reports was difficult due to the above-mentioned differences between populations, ABI definitions, and methods of analysis. Previous studies in patients with diabetes obtained higher estimates for mortality and cardiovascular events than our study. For all-cause mortality, HRs of 2.01–2.10 were observed in participants with low15 26 and high ABIs26; for MCEs, an HR of 2.5 was estimated.15 However, lower risk figures have also been reported in these patients (with diabetes). The HR for myocardial infarction was 1.88 in participants with ABI of <1 from the Multi-Ethnic Study of Atherosclerosis, and 1.52 in participants from the Cardiovascular Health Study.45 Likewise, lower estimates for ABI have been presented in the general population, with diabetes included in the adjustment: a relative risk of 1.38 in participants with ABI values of ≤0.9 for myocardial infarction and of 1.58 for all-cause mortality.46 Finally, ABI values of<0.6 were associated with an unadjusted HR of 1.24 in a model to predict mortality in persons with PAD and diabetes but did not enter the final model when adjusted for other predictors.47 Our results regarding macrovascular outcomes would be within the lower range among the wide variety found in the literature.
As for the microvascular complications, Lee et al found a twofold risk of retinopathy in persons with altered ABI, defined as ABI values of <0.9 or ≥1.3,48 similar to the risk of neuropathy reported by Cardoso et al, and both being slightly higher than our results.15 Cardoso et al did not find a relation of low ABI with retinopathy or renal outcomes,15 whereas in our study, low ABI was significantly associated with all the microvascular outcomes.
Our results suggest that ABI assessment may be considered at the initial risk assessment of acute and chronic complications of diabetes mellitus to aid in decision-making aspects. For example, our population with no previous cardiovascular disease would be candidate for a consideration of more astringent HbA1c goals.49 Within this population, the HbA1c goals could vary according to ABI levels.
The ABI could also orient on the blood pressure targets. For example, in persons with diabetes and hypertension, in primary prevention, and a 10-year risk of atherosclerotic cardiovascular disease (ASCVD) of >15% a blood pressure target of <130/80 mm Hg should be considered.49 In our study, this corresponds to the groups with ABI values of 0.9 or lower. Similarly, high-intensity statin therapy, in addition to lifestyle therapy, is recommended in persons in primary prevention with a 10-year ASCVD risk of >20%.49 In our study, this corresponds to the groups with ABI values of 0.7 or lower. The risk indicated by ABI values could also help in decision-making concerning aspirin therapy as a primary prevention strategy, which may be considered in persons with diabetes at increased cardiovascular risk.49
Regarding renal complications of diabetes, the assessment of urinary albumin could be more frequent in persons with higher risk of this complication, indicated with ABI values. Further studies could even examine the benefit of agents acting on the renin-angiotensin system in patients with normal blood pressure, normal urinary albumin to creatinine ratio, and normal eGFR.
Finally, current recommendations suggest ABI assessment only in persons with symptoms of claudication or decreased pedal pulses in the context of foot care. However, up to 50% of diabetic peripheral neuropathy may be asymptomatic50; therefore, ABI assessment should be considered even in the absence of claudication or decreased pedal pulses. Moreover, foot exam frequency could be increased if ABI indicated a higher risk of neuropathy. However, we did not assess the incidence of foot ulcers in particular in our study, and not all cases of incident neuropathy would lead to foot ulcer. Further studies could examine how the ABI levels may affect the incidence of diabetic neuropathy distinguishing its subtypes.
Our findings support the screening with ABI in persons with diabetes, as recommended in the guidelines,42 and add the usefulness of this index in itemizing the risk of mortality, and macrovascular and microvascular complications. These patients could be treated considering a personalized estimation of their risk and receiving accordingly adapted recommendations.
Study characteristics that merit consideration
The analyses of electronic medical records provide sound opportunities for research. SIDIAPQ is a quality-ensured database that supplies a high number of participants that would be otherwise difficult to recruit. Moreover, the use of both ICD-10 and ICD-9 coding minimized the under-recording of predictors and outcomes, improving the accuracy of the risk models. The characteristics of the study population should be considered when extrapolating the results: we analyzed persons with an ABI measurement, asymptomatic for PAD with no previous cardiovascular disease. Heart failure was not an exclusion criterion, although most cases of heart failure in this population were likely ischemic and thus not eligible to enter the study. Further studies to specify preventive recommendations in patients with heart failure would be of interest. We acknowledge certain limitations. First, the observational nature of this retrospective cohort retains the possibility of residual confounding, but we selected all the available variables that could mask the relation of ABI categories with the outcomes as candidates for adjustment. Second, the presence of missing data could bias the results. We used chained equations to impute the missing values of the continuous variables.30 Imputation was intended to avert the potential selection bias that may result from analyzing only records from participants with complete data.51 Results from sensitivity analysis restricted to the complete-cases dataset were comparable to the imputed (online supplementary tables 2 and 3 and online supplementary figure 2). Finally, further studies to analyze time-to-event would be of interest, although they would require another study design.
In conclusion, different ABI categories were associated with different risks of mortality, macrovascular, and microvascular complications in persons with diabetes, asymptomatic for PAD, and in primary prevention. This could help improve preventive interventions in these patients, differentiating each group according to the level of vascular impairment.
Acknowledgments
The authors thank the Minimum Basic Data Set (Conjunt Mínim Bàsic de Dades) Division of Demand and Activity Registers, Quality and Services Area, Catalan Health Service for providing data on hospital discharges.
References
Footnotes
Contributors LA-C designed the research, researched data, interpreted the results, and wrote the manuscript. MC-C researched data, performed statistical analysis, interpreted the results, and reviewed/edited the manuscript. AP researched data, interpreted the results, and wrote the manuscript. MG-G designed the research, interpreted the results, and contributed to the discussion. RM-L researched data, and interpreted the results. JB researched data and performed statistical analysis. ME-B researched data and interpreted the results. DP interpreted the results and contributed to the discussion. LC contributed to the discussion. LG reviewed/edited the manuscript. RR designed the research, researched data, interpreted the results, and reviewed/edited the manuscript. RR and MG-G are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This project was supported by clinical research grants from Spain’s Health Ministry (ED10-83, EC10-84) and Science and Innovation Ministry (Carlos III Health Institute), cofinanced with European Union ERDF funds (Network for Prevention and Health Promotion in Primary Care, RedIAPP RD16/0007), and the Agency for Management of University and Research Grants (2014 SGR 902). The funding sources were not involved in study design; collection, analysis, and interpretation of data; report writing; or the decision to submit the article for publication. The authors take sole responsibility for the integrity of the data and the accuracy of the analysis.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval to use SIDIAPQ data for observational research was obtained from the Ethics Committee for Clinical Research IDIAP Jordi Gol (P14/052).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data may be obtained from a third party and are not publicly available.