Article Text

Abstract
Objective Reduction of muscle mass and strength is an important treatment target for patients with type 2 diabetes. Recent studies have reported that high-intensity resistance training improves physical function; however, all patients found it difficult to perform high-intensity resistance training. Radio calisthenics, considered as therapeutic exercises to promote health in Japan, are simple exercises that can be performed regardless of age and help move the muscles and joints of the whole body effectively according to the rhythm of radio. We investigated the efficacy of radio calisthenics for muscle mass in patients with type 2 diabetes in this retrospective cohort study.
Research design and methods A total of 42 hospitalized patients with type 2 diabetes were recruited. The skeletal muscle mass index (SMI, kg/m2) was calculated as appendicular muscle mass (kg) divided by height squared (m2). We defined the change of SMI as the difference of SMI between the beginning and end of hospitalization.
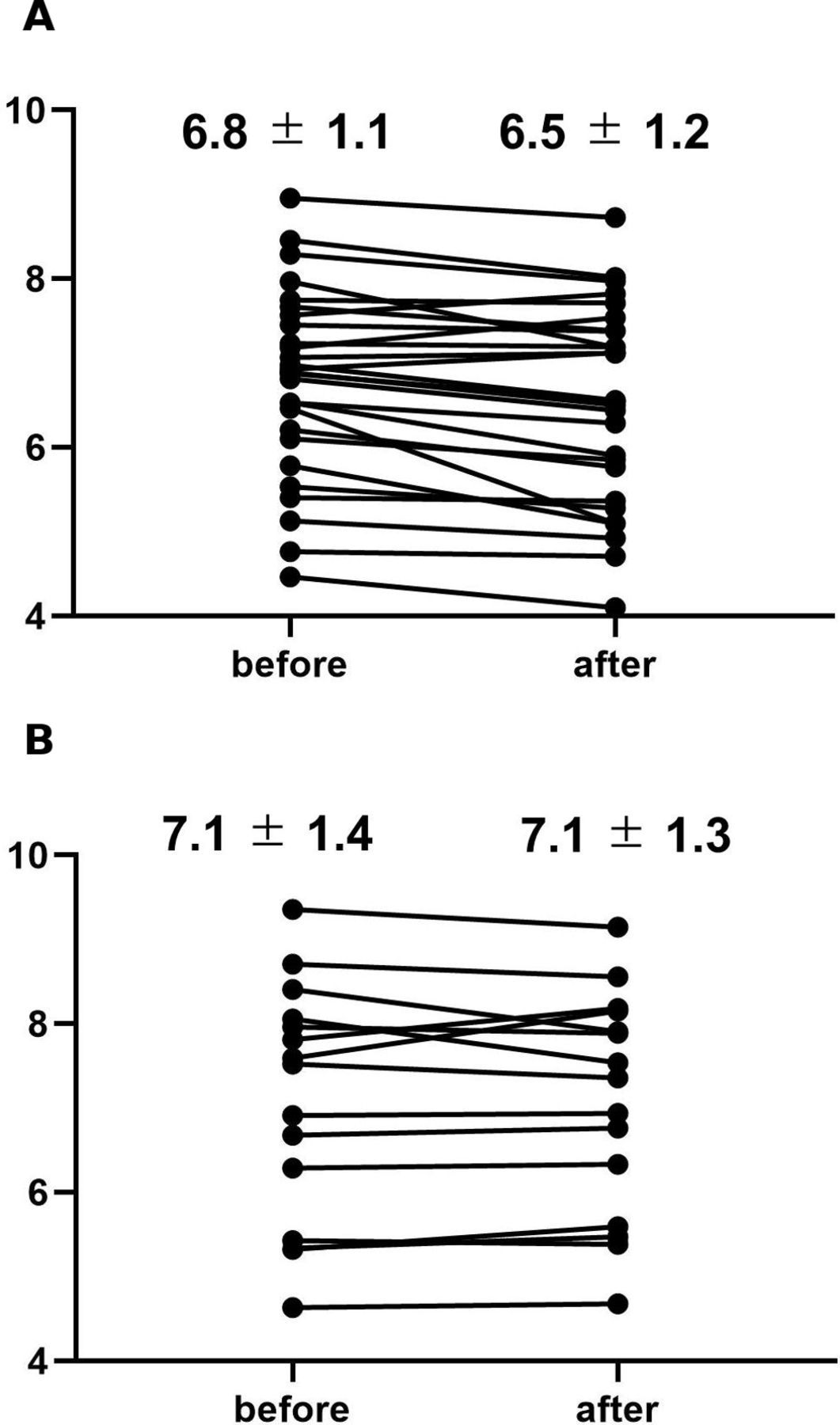
Results Among 42 patients, 15 (11 men and 4 women) performed radio calisthenics. Body weights of both radio calisthenics exercisers and non-exercisers decreased during hospitalization. The change of SMI was significantly lesser in radio calisthenics exercisers than in non-exercisers (7.1±1.4 to 7.1±1.3, –0.01±0.09 vs 6.8±1.1 to 6.5±1.2, –0.27±0.06 kg/m2, p=0.016). The proportion of decreased SMI was 85.2% (23/27 patients) in non-radio calisthenics exercisers, whereas that in radio calisthenics exercisers was 46.7% (7/15 patients).
Conclusions Radio calisthenics prevent the reduction of skeletal muscle mass. Thus, radio calisthenics can be considered effective for patients with type 2 diabetes.
- exercise
- radio calisthenics
- muscle mass
- sarcopenia
- type 2 diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Reduction of muscle mass and strength is an important treatment target for patients with type 2 diabetes.
High-intensity resistance training improves physical function.
Radio calisthenics, which is a Japanese traditional exercise, are simple exercises that can be performed regardless of age and can move the muscles and joints effectively.
What are the new findings?
Skeletal muscle mass index (SMI, kg/m2) and lean body mass decreased in non-radio calisthenics exercisers during hospitalization.
The decrease of SMI was significantly lesser in radio calisthenics exercisers than in non-exercisers.
How might these results change the focus of research or clinical practice?
Radio calisthenics are useful for maintaining skeletal muscle mass in patients with type 2 diabetes without adverse effects.
Introduction
The number of patients with type 2 diabetes has been rapidly increasing, and these patients often suffer from a reduction of muscle mass and strength.1 The reduction of muscle volume and weakness of muscle tissues with ageing is called sarcopenia, which often leads to motor function disorders, falls, fractures, and difficulty in participating in activities of daily life.2 The presence of sarcopenia also increases the risk of chronic heart failure,3 cardiovascular disease,4 pneumonia,5 and mortality.6
To maintain the human body’s muscle volume, prolonged resistance training is required.7 Moreover, exercise can raise the efficiency of muscular glucose uptake because of an increase in muscle forkhead box protein O18 and glucose transporter 4,9 which controls blood glucose levels.10 These rules are also applicable to patients with type 2 diabetes.9 Recent studies have reported that high-intensity resistance training improves physical function and balance11–13 and reduces the fear of falling.14 The American College of Sports Medicine and the American Diabetes Association demonstrated that resistance training enhanced the skeletal muscle volume and recommended a combination of aerobic and resistance training for controlling blood glucose levels.9 However, about half of the patients with diabetes did not perform the exercise regularly and a main reason for this was lack of time to exercise.10
In Japan, we habitually practice a Japanese traditional exercise called ‘radio calisthenics’. These are simple exercises that can be performed regardless of age and can move the muscles and joints effectively according to the rhythm of the radio. It is considered a therapeutic exercise to promote health in Japan. The required time for calisthenics is approximately 3 min, and it has an exercise intensity of 4–4.5 metabolic equivalents (METs).15 Radio calisthenics require a moderate-intensity aerobic activity that is considered to be suitable for the training of patients with type 2 diabetes. However, no studies have investigated the efficacy of radio calisthenics in patients with type 2 diabetes so far.
In addition, we have observed the reduction of muscle volume in patients with type 2 diabetes without prior physical inactivity during hospitalization for controlling blood glucose levels. Here, we investigated the efficacy of radio calisthenics for muscle mass in patients with type 2 diabetes in this retrospective cohort study.
Materials and methods
Study patients
We enrolled 42 patients with type 2 diabetes without physical inactivity who were all inpatients at the Kyoto Prefectural University of Medicine from April 2016 to March 2017. In this retrospective cohort study, 15 patients (11 men and 4 women), who were hospitalized from September 2016 to March 2017, practiced the radio calisthenics.
Lifestyle factors and medications
We administered a standardized questionnaire to all patients at the beginning of hospitalization. Patients were divided into non-smokers, ex-smokers, and current smokers. In addition, patients recorded the kinds and frequencies of their participation in sports or recreational activities in the questionnaire.16 We categorized patients who performed any kind of sports regularly at least once a week as regular exercisers.17 In addition, patients recorded the presence of drinking habits and insulin use on the questionnaire.
Data collection
At the beginning of hospitalization, patients underwent an examination of the concentrations of several factors in venous blood, including fasting plasma glucose, creatinine, and C-peptide after an overnight fast. Hemoglobin A1c (HbA1c) was measured using high-performance liquid chromatography, and results were expressed as a National Glycohemoglobin Standardization Program unit. We used the Japanese Society of Nephrology equation for estimated glomerular filtration rate (eGFR): eGFR (mL/min/1.73 m2)=194×serum creatinine−1.094×age−0.287 (×0.739 for women).18
Body composition of patients was evaluated using the body composition analyzer with a multifrequency impedance called InBody 720 (InBody Japan, Tokyo, Japan).19 20 The multifrequency impedance analyzer provided results that showed a good correlation with those obtained using the dual-energy X-ray absorptiometry method.21 We collected data of body weight (BW, kg), skeletal muscle mass (kg), appendicular muscle mass (kg), and body fat mass (kg). Then, skeletal muscle mass index (SMI, kg/m2) was calculated by dividing the appendicular muscle mass (kg) by the square of the height (m).22 Weight-adjusted SMI was derived by dividing skeletal muscle mass (kg) by the BW (kg). Body mass index was defined as BW (kg) by dividing the square of the height (m). We investigated the body composition twice, once at the beginning and then at the end of hospitalization, and analyzed the difference between the values at two points. We defined the change of SMI as the difference of SMI between the beginning and end of the hospitalization. We also defined decreased SMI as a change of SMI of <0 kg/m2.
Retinopathy was assessed by chart review and graded as follows: no diabetic retinopathy, simple diabetic retinopathy, and proliferative diabetic retinopathy.23 Neuropathy was diagnosed using criteria for diabetic neuropathy proposed by the Diagnostic Neuropathy Study Group.24 Nephropathy was graded as follows: normoalbuminuria, urinary albumin excretion <30 mg/g of creatinine (Cr) (mg/gCr); microalbuminuria, 30–300 mg/gCr; and macroalbuminuria, >300 mg/gCr.25
Performance of radio calisthenics
Radio calisthenics were established for improving people’s physical strength and promoting public health by Japan post in the 1950s and have been popular among many people regardless of age or sex in Japan. Radio calisthenics have two types: the first radio calisthenics involves moving muscles and joints of the whole body to the rhythm, and the second radio calisthenics is aimed to improve muscle strength. We adopted the second radio calisthenics in this study. The required time for the calisthenics is approximately 3 min, and it has an exercise intensity of 4.5 METs.
The duration of hospitalization was approximately 14 days, and we instructed the patients to perform the second radio calisthenics twice daily, once before breakfast and once after dinner on the bedside, during hospitalization. The training scheme of radio calisthenics was in accordance with a movie on DVD. We did not instruct any resistance training other than the radio calisthenics and aerobic training, mainly fast walking, for a total of 60 min/day.26
Meals during hospitalization
The meals served to the hospitalized patients were set as follows: total energy was calculated as ideal BW×25–30 kcal/kg BW/day; carbohydrates comprised 50%–60% of the total energy; protein 1.0–1.2 g/kg BW/day; and the rest as fat, according to the recommendations of the Japanese Diabetes Society on dietetic therapy in Japanese patients with diabetes.27 Moreover, patients were not allowed to take snacks or supplements other than the meals served during hospitalization.
Statistical analysis
Statistical analyses were performed using JMP V.12.0 software (SAS Institute, Cary, North Carolina). A p value of <0.05 was considered statistically significant. The means or frequencies of potential confounding variables were calculated. Continuous variables were presented as mean±SD. Categorical variables were presented as numbers (percentage, %). P values were analyzed using the Mann-Whitney U test for continuous variables, and χ2 test for categorical variables was employed to assess the statistical significance of differences between the groups. Moreover, a paired t-test was performed to assess the statistical significance of differences between the beginning and end of the hospitalization. Then, we also analyzed the difference of change in SMI of patients with and without radio calisthenics according to the having exercise habit or not.
Results
Clinical characteristics of the 42 patients (24 men and 18 women) who participated in the survey are shown in table 1.
Characteristics of patients at the beginning of hospitalization
Among them, 15 (11 men and 4 women) performed radio calisthenics during hospitalization. The average age of patients who did not exercise and those who exercised was 65.8±12.6 and 62.9±14.5 years, respectively. HbA1c levels in patients who did not exercise and in those who exercised were 9.3%±1.8% and 10.2%±1.2%, respectively. Every night during hospitalization, we asked the patients whether they had performed the radio calisthenics, and we confirmed that all of them have certainly done it twice a day.
The change of SMI (kg/m2) is shown in figure 1 and table 2. BWs of both non-radio calisthenics exercisers and radio calisthenics exercisers decreased during hospitalization, whereas SMI and lean body mass decreased in non-radio calisthenics exercisers but not in radio calisthenics exercisers during hospitalization. The change of SMI was significantly lesser in radio calisthenics exercisers than in non-radio calisthenics exercisers (−0.01±0.00 vs −0.27±0.06 kg/m2, p=0.016). The proportion of decreased SMI was 85.2% (23/27 patients) in non-radio calisthenics exercisers, whereas that in radio calisthenics exercisers was 46.7% (7/15 patients). Moreover, weights of appendicular skeletal and upper limb muscles significantly increased in radio calisthenics exercisers compared with those in non-radio calisthenics exercisers. In contrast, weight reduction of the lower limb muscles tended to be lesser in the radio calisthenics exercisers than in non-radio calisthenics exercisers. Fat content in the radio calisthenics exercisers was significantly decreased compared with non- radio calisthenics exercisers (table 2).
{kind=link}
Change of SMI between (A) non-radio calisthenics exercisers and (B) radio calisthenics exercisers and during the hospitalization. SMI, skeletal muscle mass index.
Characteristics of patients at the beginning and end of hospitalization
In patients without exercise habit, the change in SMI of the patients with radio calisthenics tended to be lesser than that of patients without (−0.07±0.26 kg/m2 vs −0.25±0.34 kg/m2, p=0.168). In addition, in patients with exercise habit, the change in SMI of the patients with radio calisthenics was lesser than that of patients without (−0.12±0.33 kg/m2 vs −0.30±0.37 kg/m2, p=0.047).
There were no adverse effects related to the radio calisthenics, such as hypoglycemia, fall, fracture, and musculoskeletal pain.
Discussion
Our study showed clear effects of radio calisthenics on muscle mass in hospitalized patients with type 2 diabetes. The change of SMI was significantly lesser in radio calisthenics exercisers. Weights of both appendicular skeletal muscles and upper limb muscles increased in radio calisthenics exercisers. Our past experience demonstrated that muscle volume reduces due to long-term hospitalization. In fact, about 85% of patients who did not perform radio calisthenics showed reduced muscle mass during hospitalization in this study. As a part of the treatment for patients with type 2 diabetes during hospitalization, it was necessary to determine an easy exercise therapy that could prevent reduction of skeletal muscle mass. In this study, we revealed that performing the radio calisthenics twice a day could help in maintaining the muscle mass of hospitalized patients.
Our study showed that radio calisthenics is associated with maintaining muscle mass in hospitalized patients with type 2 diabetes and helps in moving the appendicular skeletal muscles effectively. Exercise training improves insulin sensitivity in the skeletal muscles by increasing the muscular glucose uptake.9 Despite the simple procedures, it guarantees an exercise intensity of 4.5 METs and improves the glycemic control among patients with type 2 diabetes. Moreover, maintaining muscle mass prevents the deterioration of type 2 diabetes and the development of sarcopenia.1 In addition, there were no adverse effects related to the radio calisthenics.
A previous report revealed that people, who perform radio calisthenics more than 5 days a week for more than 3 years, were superior in muscle mass quantity, index of subclinical atherosclerosis and lung function compared with general population.28 Moreover, a previous study reported that radio calisthenics is the second exercise therapy followed by walking in Japanese outpatients with diabetes,29 and radio calisthenics is very popular in Japan. We also revealed that radio calisthenics is useful for preventing reduction of skeletal muscle mass more in patients with exercise habit than in patients without. This might be because many patients with exercise habit performed walking in Japan,29 one of the aerobic exercises; thus the patients with exercise habit can prevent decreasing SMI through obtaining both aerobic and resistance training effect.
Additionally, we could not demonstrate the association between the performance of radio calisthenics and improvement of glucose control. In this study, there was no significant difference between radio calisthenics and glucose control (37.0±69.6 mg/dL vs 31.3±52.2 mg/dL, p=0.784). A possible explanation is that pharmacotherapy is a major factor affecting blood glucose, especially during hospitalization, and thus no significant difference in blood glucose improvement was detected between two groups. Additionally, because radio calisthenics is mainly resistance training, there is a possibility that radio calisthenics did not contribute to improving short-term glycemic control during hospitalization.
There was no incidence of hypoglycemia associated with radio calisthenics in this study. However, during hospitalization, the blood glucose of the patients has been checked at least four times a day, before every meal and at bedtime, and we have checked them every day and adjusted insulin and oral antidiabetic drugs appropriately in order to prevent hypoglycemia, which might result in the finding.
There are several limitations to this study that have to be mentioned. First, this study was not a randomized controlled trial, but a retrospective cohort study. Therefore, some bias might exist. To clarify the effect of radio calisthenics on skeletal muscle mass, further studies, especially randomized controlled trials, would be needed. Second, the study population consisted only of Japanese. Thus, it is unclear whether the same results can be obtained in the Western population with different physiques. Third, the sample size was not large. Fourth, we did not follow-up the data of body composition after discharge. Therefore, the long-term effect of radio calisthenics remains unclear. Additionally, we could not demonstrate the association between the performance of radio calisthenics and improvement of glucose control. In this study, there was no significant difference between radio calisthenics and glucose control (37.0±69.6 mg/dL vs 31.3±52.2 mg/dL, p=0.784). In this point, further studies would be needed as well. Lastly, because we used data using a body composition analyzer with a multifrequency impedance, change of body water balance might affect this result.
In conclusion, our study showed the effect of radio calisthenics on skeletal muscle mass in patients with type 2 diabetes. In order to elucidate this causal relationship, further accurate analyses, such as a randomized controlled trial, will be required.
Acknowledgments
We thank Editage (www.editage.com) for English language editing.
References
Footnotes
Presented at Part of this manuscript has been published and presented in poster presentation of American Diabetes Association 79th Annual meeting of 2019 (752-P: Japanese radio calisthenics prevents reduction of skeletal muscle volume in patients with type 2 diabetes).
Contributors TK designed the study, analyzed the data and wrote the manuscript. TO designed the study, researched, analyzed and interpreted the data and reviewed/edited the manuscript. YH researched and interpreted the data and contributed to discussion. KI, TS, EU, MH, MA and MY researched the data and contributed to discussion. MF interpreted the data and reviewed/edited the manuscript. MF is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The sponsors were not involved in the study design, in the collection, analysis, or interpretation of data, in the writing of this manuscript, or in the decision to submit the article for publication.
Competing interests YH has received grant support from Asahi Kasei Pharma and honoraria from Mitsubishi Tanabe Pharma and Novo Nordisk Pharma, outside the submitted work. TS has received payment for development of educational presentation from Ono Pharmaceutical, Mitsubishi Tanabe Pharma, Astellas Pharma, Kyowa Hakko Kirin, Sanofi, MSD, Kowa Pharmaceutical, Taisho Toyama Pharmaceutical, Takeda Pharmaceutical, Kissei Pharmaceutical, Novo Nordisk Pharma and Eli Lilly Japan. MH has received grant support from Asahi Kasei Pharma, payment for development of educational presentations from MSD, Mitsubishi Tanabe Pharma, Kowa and Sumitomo Dainippon Pharma, and royalties from US 10,238,714 B2, outside the submitted work. EU has received personal fees from AstraZeneca, Astellas Pharma, Daiichi Sankyo, Kyowa Hakko Kirin, Kowa Pharmaceutical, MSD, Mitsubishi Tanabe Pharma, Novo Nordisk Pharma, Taisho Toyama Pharmaceutical, Takeda Pharmaceutical, Nippon Boehringer Ingelheim, Sumitomo Dainippon Pharma and Johnson & Johnson, outside the submitted work. MA has received payment for development of educational presentation from Novo Nordisk Pharma, Abbott Japan, AstraZeneca, Kowa Pharmaceutical, Ono Pharmaceutical and Sumitomo Dainippon Pharma. MY has received payment for development of educational presentation from MSD, Sumitomo Dainippon Pharma, Kowa, AstraZeneca, Takeda Pharmaceutical, Kyowa Hakko Kirin, Daiichi Sankyo, Kowa Pharmaceutical, and Ono Pharmaceutical. MF has received research support and payment for development of educational presentation from AstraZeneca, Astellas Pharma, Nippon Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly Japan, Kyowa Hakko Kirin, Kissei Pharmaceutical, MSD, Sumitomo Dainippon Pharma, Kowa, Mitsubishi Tanabe Pharma, Novo Nordisk Pharma, Sanwa Kagaku Kenkyusho, Sanofi, Ono Pharmaceutical, Taisho Pharmaceutical, Bayer Yakuhin, Mochida Pharmaceutical, Johnson & Johnson Medical, Nippon Chemiphar, Terumo, Teijin Pharma, and Takeda Pharmaceutical.
Patient consent for publication Not required.
Ethics approval The Ethics Committee of Kyoto Prefectural University of Medicine approved this study (No RBMR-E-466-7). All people provided informed consent and written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.