Article Text

Abstract
Objective Esterified collagen (EC) can be functionalized with heparin to enhance islet graft stability. Growth factors secreted by human adipose-derived stem cells (hADSCs) can bind efficiently to EC-heparin (EC-Hep), which enhances revascularization and cell protection. We investigated the therapeutic potential of a combined heparin-esterified collagen-hADSC (HCA)-islet sheet to enhance islet engraftment.
Research design and methods This study was designed to assess the efficiency of using EC-Hep as a scaffold for subcutaneous islet transplantation in diabetic athymic mice. After the hADSC-cocultured islets were seeded in the EC-Hep scaffold, islet function was measured by glucose-stimulated insulin secretion test and growth factors in the culture supernatants were detected by protein array. Islet transplantation was performed in mice, and graft function and survival were monitored by measuring the blood glucose levels. β-Cell mass and vascular densities were assessed by immunohistochemistry.
Results The EC-Hep composite allowed sustained release of growth factors. Secretion of growth factors and islet functionality in the HCA-islet sheet were significantly increased compared with the control groups of islets alone or combined with native collagen. In vivo, stable long-term glucose control by the graft was achieved after subcutaneous transplantation of HCA-islet sheet due to enhanced capillary network formation around the sheet.
Conclusions The findings indicate the potential of the HCA-islet sheet to enhance islet revascularization and engraftment in a hADSC dose-dependent manner, following clinical islet transplantation for the treatment of diabetes mellitus.
- human adipose tissue
- bioengineering
- islet transplantation
- revascularization
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Many sites other than the liver have been reported for experimental islet transplantation.
Several studies focused on the subcutaneous space as a clinically applicable site because the transplantation procedure itself is simple, although its efficiency has previously been reported to be extremely low.
The beneficial effect of adipose tissue-derived stem cells on islet survival and engraftment has been reported.
What are the new findings?
Heparin-esterified collagen with human adipose-derived stem cells (hADSCs) (HCA) sheet promoted islet viability, functionality and secretion of angiogenic growth factors in vitro.
HCA-islet sheet has a potent capability to enhance revascularization and engraftment of rat and human islets in subcutaneous transplantation.
How might these results change the focus of research or clinical practice?
This strategy allows growth factors secreted by hADSCs to bind to EC-heparin, leading to enhanced revascularization and graft protection.
The findings will hopefully be translated to clinical islet cell transplantation for the treatment of insulin-dependent diabetes mellitus.
Introduction
Type 1 diabetes is an autoimmune disease in which the immune system is activated to destroy the insulin-producing cells in the pancreas. The therapeutic potential of pancreatic islet transplantation as a treatment for the type 1 diabetes mellitus has fascinated researchers and clinicians for decades.1 2 Islet transplantation is typically accomplished by direct infusion of islets into the liver via the portal vein. However, adequate accommodation of islet engraftment is still challenging, and several alternative sites have been investigated for stable transplantation of islets in animals and humans.3–8 For example, subcutaneous transplantation has attracted great attention as a promising approach because of the facile transplantation of islets and easy removal of the grafts through minimally invasive procedures with local anesthesia. However, efficient application remains hampered because of insufficient early vascularization, induction of local inflammation and mechanical stress on the graft. Transplantation into unmodified subcutaneous sites has routinely failed to reverse the diabetic state,9 10 resulting from inadequate revascularization of transplanted islets.
Revascularization can be promoted by stable anchorage of angiogenic growth factors to supporting scaffolds. Biomaterials that promote angiogenesis have great potential for rapid revascularization and survival of subcutaneously transplanted islets. Collagen is the main structural protein. Chemical modifications of the collagen can increase the adhesion and proliferation of various cells, and we recently reported that esterification of collagen enhances islet viability and long-term insulin release.11
Human adipose-derived stem cells (hADSCs) inhibit the inflammatory response against transplanted islets, and have been used as supportive cells to improve the viability and function of islets for the secretion of some growth factors with improving angiogenesis.12 Heparin is a polysaccharide that is distributed throughout the extracellular matrix, in which growth factors are also bound and protected against enzymatic or thermal degradation.13 Heparin-immobilized scaffolds have been used for the sustained delivery of growth factors to enhance revascularization.14 Use of these scaffolds may also allow the transplantation of a smaller number of islets for the long-term control of type 1 diabetes mellitus, which has been a challenging goal.15 16
We hypothesized that such a composite can enhance revascularization, thus improving islet viability and stable engraftment in subcutaneous transplantation. In this study, we investigated the capability of hADSCs contained in heparinized collagen scaffolds to enhance the stability of the transplanted islets.
Methods
Animals
Male Sprague-Dawley rats and BALB/c-nu mice purchased from Orient Bio (Seongnam, Korea) were used as donors and recipients, respectively. All animal experiments were approved by the Institutional Animal Care and Use Committee of Asan Medical center (IACUC-2014-13-217).
Preparation of heparinized esterified collagen
Esterified collagen (EC) were fabricated by 1% (w/v) EC solution (Dalim Tissen, Korea) in 0.1 M acetic acid (Junsei Chemical, Tokyo, Japan). Lyophilized EC were crosslinked with 20 mM 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC; Tokyo Chemical, Tokyo, Japan) in ethanol (Merck Millipore, Burlington, Massachusetts, USA). For heparin immobilization, freeze-dried EC were soaked in 50 mM 2-(N-morpholino)ethanesulfonic acid hydrate buffer (Sigma-Aldrich, St. Louis, MO, USA) supplemented with 1% (w/v) heparin (Wako Pure Chemical, Osaka, Japan), 20 mM EDC and 7.8 mM N-hydroxysuccinimide (Sigma-Aldrich).
Characterization of heparinized EC and growth factor release assay
The presence of heparin in collagen sponges was verified by toluidine blue staining.17 To quantify heparin crosslinking, sponge was immersed to 1 mL of 0.005% toluidine blue. After shaking, 2 mL of hexane was added. The absorbance of the aqueous phase was measured at 620 nm.18
A Hitachi S800 scanning electron microscope (Hitachi, Tokyo, Japan) was used to examine the morphology of the scaffolds. For in vitro enzymatic degradation of scaffold, EC and EC-heparin (EC-Hep) were incubated in 2 units/mL of collagenase and the residual mass was determined over time. The tensile strength of the scaffold was measured using universal testing machine (ST-1001, SALT, Korea) in accordance with ASTM D-882–83. The tensile strength was determined to be 3.62±1.83 n with a speed of 2 mm/min.
In vitro growth factor release profiles from the EC and EC-Hep were determined. Briefly, 200 μL of basic fibroblast growth factor (bFGF) or hepatocyte growth factor (HGF) solution (2 and 20 ng/mL, respectively; Koma Biotech, Seoul, Korea) was loaded on EC or EC-Hep. The sponges were soaked in 1 mL phosphate buffered saline (PBS) and incubated at 37°C. The entire incubation medium was collected after 4, 8, 24, 48 and 72 hours. After 72 hours of incubation, the remaining growth factors in EC or EC-Hep were obtained with 1 mL of PBS containing 1.5 M NaCl by vigorous shaking and squeezing of the sponges. The amount of bFGF or HGF was determined using ELISA (Koma Biotech).
Isolation of rat islets and hADSCs
Rat islets were isolated by digestion with collagenase type XI (Sigma-Aldrich) and cultured in Roswell Park Memorial Institute (RPMI) 1640 medium (Invitrogen, Carlsbad, California, USA) as previously described.19 Human adipose tissue was obtained from donors who were to receive abdominal surgery. hADSCs isolated from adipose tissue were cultured in Dulbecco’s modified Eagle’s medium (Invitrogen) as previously described by Zuk et al.20 The cells were classified as hADSCs on the basis of their adherence to plastic and expression of the surface markers CD45, CD73, CD90 and CD105 (BD Pharmingen, San Diego, California, USA). All experiments were performed using hADSCs after three to nine passages (online supplementary figure S1a, b).
Supplemental material
Isolation of human islets
Pancreatic tissue collected with appropriate consent (online supplementary table S1) and ethical approval (IRB: 2019–0442) was used for islet isolation. Islets were isolated by the Ricordi method as previously described.21 Following isolation, islets were cultured in CMRL1066 medium (Invitrogen).
Islet and hADSC co-culture
To facilitate the coating of hADSCs to the islet surface, we used the previously reported method.22 Briefly, the hADSCs and islets in RPMI medium were co-incubated at 37°C for 1 hour in culture tubes and subsequently seeded. To compare the number of islets with different diameters and volumes, individual islets were mathematically converted to standard islet equivalents (IEQs) with a diameter of 150 µm. Islets (100 IEQs per well) were cultured with or without hADSCs (1×104 cells) on various dishes for 7 days. Adhesion and shape of the hADSCs on the islet surface were analyzed using inverted microscopy, and viability was determined by calculating the percentage of viable (fluorescein diacetate (FDA)-positive, green, 0.5 µM) versus non-viable (propidium iodide (PI)-positive, red, 75 µM) cells within each islet.
Measurement of insulin release
Islets were stimulated with 1.67 or 16.7 mM glucose concentration in Krebs-Ringer buffer for 1 hour. The concentration of released insulin was analyzed using ELISA (Mercodia, Uppsala, Sweden).
Human growth factor array in the co-culture media
After incubation for 7 days, the conditioned medium was collected. RPMI medium served as the control. We measured 40 different growth factors using the Quantibody Human Growth Factor Array 1 (RayBiotech, Norcross, Georgia, USA). The data were analyzed using the Q-Analyzer (RayBiotech). The amount of each growth factor in the original extracts was measured and subtracted from that in the medium to calculate the amount of additional growth factor produced by the cells.
Transplantation of heparin-esterified collagen-hADSC-islet sheet
Diabetes was induced in BALB/c-nu mice by intraperitoneal injection of streptozotocin (Sigma-Aldrich, 250 mg/kg). Mice were considered to be diabetic when blood glucose (BG) levels were >300 mg/dL for at least two consecutive days. Mice were randomly divided into five experimental groups (n=5 in each group). Rat islets (4000 IEQ) alone and rat islets with ADSCs (1×102, 103, 104, 105) loaded onto EC-Hep were transplanted in the mice’s dorsal subcutaneous region. For human islet transplantation, mice were divided into two experimental groups: 1) human islets (8000 IEQ) or 2) human islets with ADSCs (1×106). Body weight and BG levels were monitored, and blood samples were obtained before transplantation and once a week afterward for measurements of insulin levels.
Intraperitoneal glucose tolerance test
After 6 hours of fasting, the mice received a glucose solution intraperitoneally (2 g/kg). BG levels were determined at 0, 5, 15, 30, 60 and 120 min after injection. Normal and mice with diabetes were used as controls.
Histological study
Retrieved grafts were fixed in 4% paraformaldehyde (Sigma). Samples were serially sectioned and sections were stained for H&E, CD31 (1:100; Abcam, Cambridge, Massachusetts, USA), alpha smooth muscle actin (αSMA, 1:200, Abcam) and insulin (1:200, Abcam). Imaging was acquired using inverted fluorescence microscopy and analyzed using ImageJ software.
For determination of β-cell mass, the total area and insulin positive area of each section was measured using ImageJ software.
Quantification of inflammatory and angiogenic factors using real-time PCR
To evaluate the expression of specific genes in the graft, mRNA levels were evaluated by real-time PCR. Following RNA extraction, as per the manufacturer’s protocol, cDNA was reverse transcribed using an Omniscript RT kit (Qiagen, Mississauga, Ontario, Canada). Real-time PCR was performed using SYBR Green Master Mix kit (Applied Biosystems, Foster City, California, USA). The sequences of used primers are shown in online supplementary table S2. Data were calculated using beta-actin as an internal reference.
Statistical analysis
Data are presented as means±SEM. A paired two-tailed t-test was applied for comparison between two groups or analysis of variance (ANOVA) with Tukey’s post hoc test (GraphPad Prism V.8, GraphPad Software, La Jolla, California, USA) was used when comparisons were made across more than two groups. A p value <0.05 indicated a statistically significant difference.
Results
Fabrication and characterization of heparin immobilized collagen scaffold
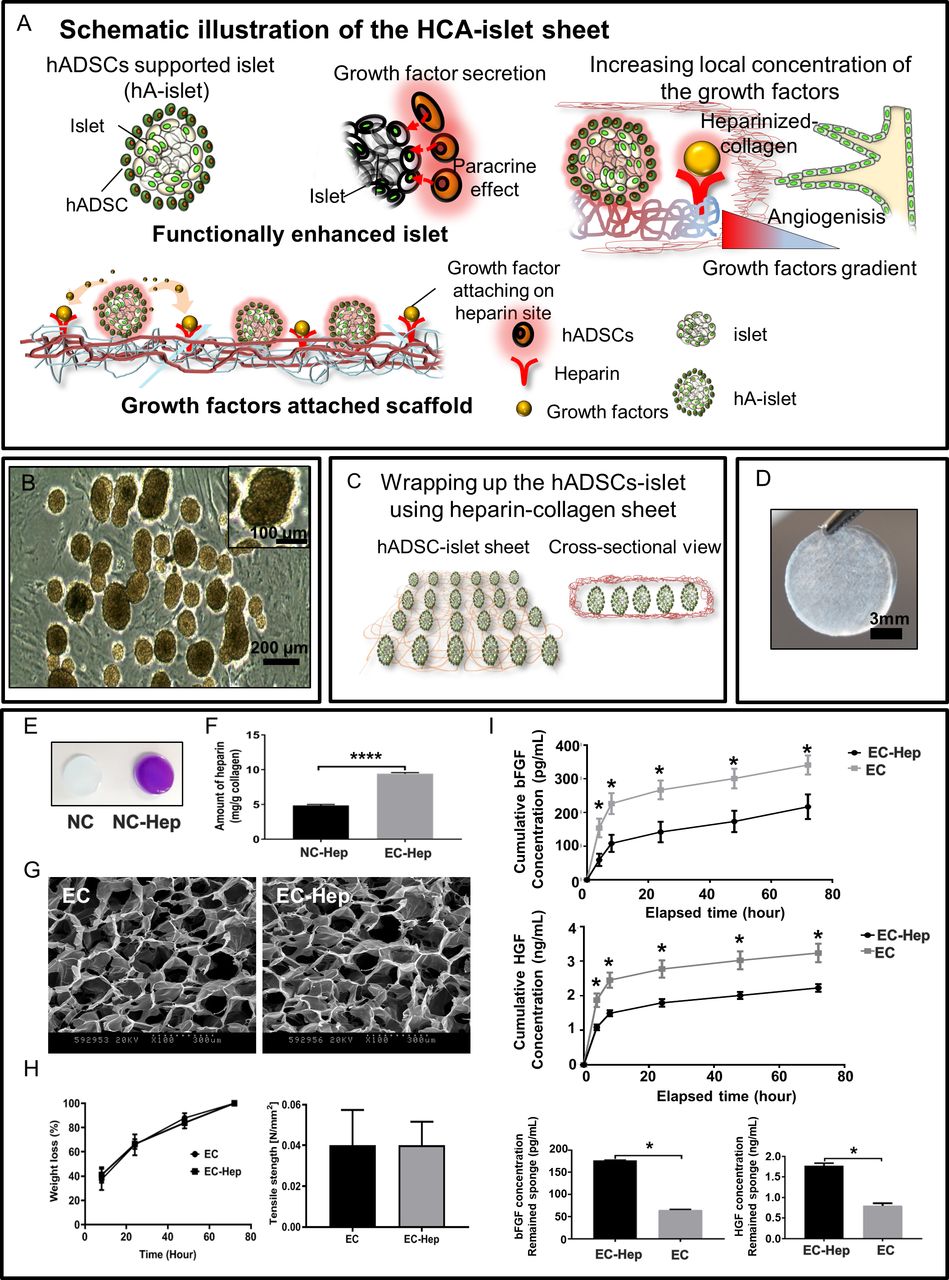
The hypothetical mechanism of scaffold fabrication is schematically illustrated in figure 1A. hADSCs co-cultured with islets (figure 1B) can increase the expression of growth factors. These growth factors can be attached to esterified collagen crosslinked with heparin (EC-Hep; figure 1C), anticipating that this could promote angiogenesis by the local, sustainable release of the growth factors.

(A) Schematic diagram of the hypothetical mechanism of combined heparin-esterified collagen-hADSC (HCA)-islet sheet used in this study. (B) Representative image of human adipose-derived stem cell (hADSC)-islets cultured on esterified collagen-heparin (EC-Hep). (C) For transplantation, islets and hADSCs were formed by suspension co-culture for 24 hours, and seeded onto EC-Hep. (D) Photograph of EC-Hep. Heparins are covalently attached to the EC. Characterization of heparin immobilized collagen scaffold. (E) Toluidine blue staining; the purple color indicates the presence of heparin with non-heparinized collagen stained blue. (F) The amount of heparin in native collagen (NC-Hep (n=4) and EC-Hep (n=4). Data are presented as mean±SEM. ****P<0.0001, unpaired two-tailed t-test. (G) Scanning electron microscopy image of EC and EC-Hep. (H) Left: in vitro enzymatic degradation of the scaffold. EC and EC-Hep were incubated in 2 units/mL of collagenase and the residual mass was determined over time. Right: mechanical properties of the scaffold. (I) In vitro cumulative release of basic fibroblast growth factor (bFGF) and hepatocyte growth factor (HGF) from EC-Hep (n=4) and EC (n=4). *P<0.05, between EC-Hep and EC, two-tailed t-test. Remaining bFGF (n=2) and HGF (n=3) amounts in sponge. *P<0.05, between EC-Hep and EC, two-tailed t-test.
To address the feasibility of this functional scaffold, the scaffolds were fabricated in a disc-form construct (figure 1D) and stained with toluidine blue to confirm the presence of heparin (figure 1E). After the native collagen (NC) and EC were crosslinked with heparin, the amount of heparin bound to the scaffolds was 4.85 and 9.43 mg heparin/g scaffold, for NC-Hep and EC-Hep, respectively (figure 1F). These results showed that a greater amount of heparin was bound to the EC than NC. The relative water solubility of EC produce a relatively larger density of the EC matrix compared with the NC matrix, and thus is attributed to the larger area that binds heparin.
Uniform pores with sizes between 60 and 300 µm in both scaffolds were clearly observed under the SEM (figure 1G). The physical properties of EC were also assessed to evaluate suitability. EC showed a dramatic increase in viscosity in the neutral buffer solution; the wettability of EC was 71±2.61 at the beginning before the slipping of water drops, and 46.17±4.41 after 2 min. In vitro degradation was assessed by measuring the weight loss; at 72 hours, the testing samples had degraded by 100% (figure 1H, left). The biocompatibility and biodegradability of the scaffolds were evaluated in vivo; the sponges had degraded 4 weeks later, and the mechanical strength was similar between the two scaffolds (figure 1H, right).
In vitro release curves of bFGF or HGF from EC and EC-Hep are depicted in figure 1I. The EC displayed a relatively rapid release profile for both bFGF and HGF. In contrast, a slower release of bFGF from EC-Hep was observed. The release profile of HGF was quite similar compared with that of bFGF. We checked the remaining amount of bFGF and HGF in the scaffold at 72 hours. The remaining amount of bFGF from EC-Hep and EC was 176.51±1.01 pg and 65.31±1.21 pg, respectively, and the remaining amount of HGF in EC and EC-Hep was 0.80±0.03 and 1.77±0.06 ng, respectively (figure 1I; online supplementary table S3). These results indicate that the interaction affinity between growth factors and EC-Hep could restrict the release of bFGF and HGF from EC-Hep.
Effect of heparin-esterified collagen-hADSC-islet sheet on islet viability and function
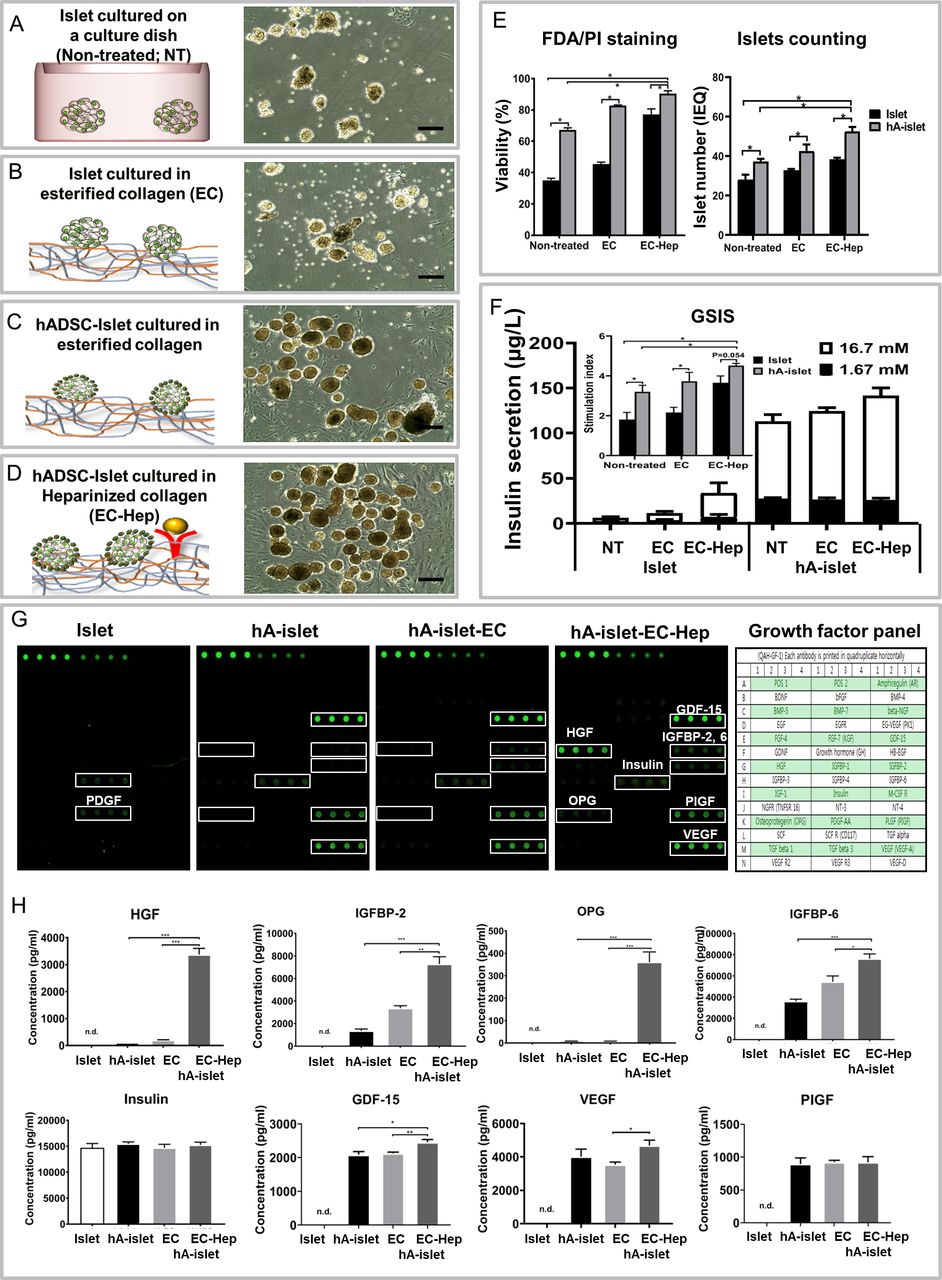
Rat islets were co-cultured with hADSCs, which adhered to the islet complex to form hADSC-rat islets (hA-rat islets). Morphological characteristics were clearly distinguishable. The hA-rat islets in EC-Hep featured more well-defined islet clusters than the rat islets alone (figure 2A–D). The co-culture of rat islets with hADSCs promotes the improvement of islets stability. Both rat islets and hA-rat islets were then loaded into EC or EC-Hep to evaluate long-term stability and morphological changes. Growth factors attached to EC-Hep provide an enriching microenvironment, and the paracrine effect helps the uptake of the islet-stabilizing growth factors. Thus, the function and viability of the complex were assumed to be enhanced. In this regard, cell viability, as determined by FDA/PI staining, was higher in hA-rat islets incubated in EC-Hep than in non-treated rat islets (figure 2E, left). Typically, in vitro culture of rat islets resulted in a tremendous loss of IEQs over time. However, the number of IEQs was remarkably preserved by hA-rat islet formation and heparin functionalization on the EC after 7 days of incubation (figure 2E, right).

Morphological changes, viability and function of islets cultured with or without human adipose-derived stem cells (hADSCs) on esterified collagen-heparin (EC-Hep) as observed after culture for 7 days. (A–D) Morphology of islets was observed under an inverted microscope. The viability of islets cultured with or without hADSCs on EC and EC-Hep was assessed by fluorescein diacetate (FDA)/propidium iodide (PI) vital staining. (E) Left: triplicate aliquots of 15 islets were placed in each well of a 24-well plate with 1 mL PBS. FDA (0.5 µM) and PI (75 µM) stock solutions were added to the sample before assessment using a fluorescent microscope to estimate cell viability as percentage of viable (FDA-positive, green fluorescence) vs non-viable cells (PI-positive, red fluorescence) within each islet. Right: after culture, the islet number was measured by calculating the IEQ under dithizone staining. Results are presented as mean±SEM. Statistical significance was determined by two-way analysis of variance (ANOVA), *p<0.05, n=3. (F) Insulin release at 1.67 and 16.7 mM glucose in islets or hA-islets (non-treated, EC and EC-Hep). Results are presented as mean±SEM. Statistical significance was determined by two-way ANOVA, *p<0.05, n=5. Growth factors secreted by the heparin-esterified collagen-hADSC (HCA)-islet sheet. (G) Signal intensity of growth factors induced by islet alone, hA-islets cultured on non-treated, EC and EC-Hep. After culture for 7 days, culture medium was collected and analyzed with a protein antibody array that detects 40 growth factors. This experiment was repeated once with similar results. (H) Growth factors presenting a detectable fluorescent signal are indicated. Hepatocyte growth factor (HGF), insulin-like growth factor binding protein-2 (IGFBP-2) and osteoprotegerin (OPG) were markedly increased in the HCA-islet sheet compared with the other groups. Values are presented as mean±SEM. Statistical significance was determined by two-way ANOVA, *p<0.05, **p<0.01, ***p<0.001, n=4. GDF-15, growth differentiation factor 15; GSIS, glucose stimulated insulin secretion; IEQ, standard islet equivalents; n.d., not detected; PBS, phosphate buffered saline; PDGF, platelet-derived growth factor; PIGF, placenta growth factor; VEGF, vascular endothelial growth factor.
To further examine the effects of hADSC coating and heparin immobilization on the islet functionality, we evaluated the level of insulin secretion at 1.67 and 16.7 mM glucose. As shown in figure 2F, the amount of insulin released was higher in hA-rat islets than in the rat islets cultured alone. In addition, the heparin functionalization on the EC significantly increased glucose-stimulated insulin secretion. The findings indicated that co-culture with hADSCs improved islet secretory function in vitro. These beneficial effects on islet function could be partly attributed to heparin functionalization on the EC scaffold.
Effect of heparin-esterified collagen-hADSC-islet sheet on secretion of growth factors
To determine the growth factors enhanced by co-culture in EC-Hep, we used a commercially available antibody array. As shown in figure 2G,H, compared with culture with islet alone, hA-rat islet led to a marked increase in growth differentiation factor 15 (GDF-15), placenta growth factor (PIGF), and vascular endothelial growth factor (VEGF) levels. Of the growth factors assayed, the signal intensities of HGF, insulin-like growth factor binding protein-2 (IGFBP-2), osteoprotegerin (OPG), IGFBP-6, insulin, GDF-15 and VEGF were significantly greater in the heparin-esterified collagen-hADSC (HCA)-rat islet sheet than in other groups. Among them, increases in HGF, IGFBP-2, IGFBP-6 and OPG were markedly greater in the HCA-rat islet sheet than hA-rat islet or hA-rat islet-EC.
Glucose monitoring after transplantation of the heparin-esterified collagen-hADSC-islet sheet
To examine the impact of the HCA-rat islet sheet, we transplanted HCA-rat islet sheets into the subcutaneous sites (figure 3). The mice were transplanted with rat islets or rat islets containing hADSCs (1×102 to 1×105 cells). EC only and 4000 IEQ rat islets only were used as controls and did not correct the hyperglycemia. Although rat islets containing 1×102 hADSCs displayed reduced BG levels compared with rat islets alone, the levels were still maintained in the range of 200–300 mg/dL. When the rat islets were transplanted with a higher number of hADSCs (1×103 or 1×104 cells), hyperglycemia was successfully reversed a week after transplantation. In addition, an increased number of hADSCs (1×105 cells) resulted in a stable BG level at the normal range in the first day of transplantation, and the mice immediately recovered to normoglycemia (figure 3A).

Co-transplantation of islets loaded on esterified collagen-heparin (EC-Hep) with or without human adipose-derived stem cells (hADSCs). (A) Blood glucose levels in diabetic recipients subcutaneously transplanted with islets alone or islets plus hADSCs. The rate of euglycemia in the heparin-esterified collagen-hADSC (HCA)-islet sheet group was significantly higher than in the islet-only group and was dependent on the number of hADSCs; n=5 mice for each group. (B) To confirm long-term graft function, normoglycemic mice underwent graftectomy at postoperative days (POD) 45, 80 and 97 (arrows). Diabetes was reversed immediately in mice receiving HCA-islet sheet until the graft was retrieved (C) intraperitoneal glucose tolerance test (IPGTT) in mice receiving islets with hADSCs. IPGTT was performed in mice 30 days after transplantation. The results are expressed as mean blood glucose levels (n=3). (D) Area under the curve of the IPGTT for recipients of HCA-islet sheet and mice with diabetes. After human islet transplantation, changes in blood glucose (E) and body weight (F) were observed (black arrow: graftectomy, red arrow: death of the animals). (G) Serum human insulin levels were measured as a marker of islet graft function. Mice received human islet with hADSCs had higher insulin levels compared with mice receiving human islets alone. (H) IPGTT in mice receiving islets with or without hADSCs. IPGTT was performed in mice 40 days after transplantation. Graftectomy was performed on mice at 60 days post-transplantation. All data are presented as mean±SEM (n=3 in each group). Statistical significance was determined by two-way analysis of variance; *p<0.05. IEQ, standard islet equivalents.
The observed dose-dependent improvement of the BG level control suggested a protective role of hADSCs. The immediate recurrence of hyperglycemia after removing the islet grafts further supported the crucial role of the transplanted rat islets (figure 3B). To evaluate the efficacy of rat islet engraftment, the intraperitoneal glucose tolerance test (IPGTT) was performed on euglycemic recipients. The BG level was significantly lower on glucose injection in the recipients of the HCA-rat islet sheet than in mice with diabetes (figure 3C). The area under the curve of IPGTT, representing the overall response to high glucose challenge, showed remarkable improvement in recipients of HCA-rat islet sheet (figure 3D). To assess the efficiency of our experiment in human islets, we transplanted HCA-human islet sheets. Isolated islets had typical features of the human islet, and functioned well on glucose stimulation (online supplementary figure S2a-d) as well as in vivo (online supplementary figure S3e-f). Based on the rodent islet results, a high number of hADSCs was chosen for human islet experimental group. Human islets and hADSCs loaded within the EC-Hep were transplanted. Graft function was evaluated by BG and body weight measurements (figure 3E-F). BG levels in mice transplanted with HCA-human islet sheet were significantly lower compared with BG levels in mice transplanted with human islet alone sheet. The HCA-human islet sheet transplant group displayed elevated serum human insulin levels compared with the human islet alone sheet (figure 3G). Results of glucose tolerance tests performed on day 40 were significantly better in recipients of hA-human islet than recipients of only human islets (figure 3H).
Histological finding after transplantation of heparin-esterified collagen-hADSC-islet sheet
Finally, we assessed whether the improved islet function was attributable to increased angiogenesis. To determine angiogenesis in the early post-transplantation phase, histological assessment was performed on day 7 after transplantation. To confirm the newly formed microvasculature, retrieved tissues were stained for vascular marker. The numbers of detectable vessels in the HCA-rat islet sheet were significantly higher than in the other groups (figure 4). Thus, addition of hADSCs induced effective early vascularization. The secretion of growth factors from embedded hADSCs was assumed to help induce angiogenesis, and was attributed to the rapid development of islet vasculature in the post-transplantation period. The vessel density was significantly higher in the hA-rat islets than the rat islets in EC-Hep, indicating that one of the beneficial effects provided by hADSCs is increased neovascularization of the graft.

Graft site histological findings. (A) Gross views of the grafted site 7 days after transplantation. (B) H&E of grafted site. (C) The degree of vascularization was evaluated according to the number of vessels for anti-CD31 and alpha smooth muscle actin (αSMA) immunostaining. Immunohistochemistry on graft tissues stained with anti-mouse CD31 antibody by the immunofluorescence methods. CD31 and αSMA staining is shown in green. Nuclei were stained with 4’, 6-diamidino-2-phenylindole (DAPI), blue). Negative controls were mice with transplantation of cell-free esterified collagen-heparin (EC-Hep). (D) CD31 and αSMA positively stained cells counted in five different fields were imaged by confocal microscopy and the mean fluorescence intensity was calculated using ImageJ software. Results were analyzed by analysis of variance and the graphs represent mean±SD (*p<0.01). The intensity (CD31+ and αSMA+) in the heparin-esterified collagen-human adipose-derived stem cells (hADSC) (HCA)-islet sheet were significantly higher than in the other groups (scale bars denote 100 µm). Immunostained samples of representative sections from experimental groups and mice with diabetes are shown. MFI, mean fluorescence intensity.
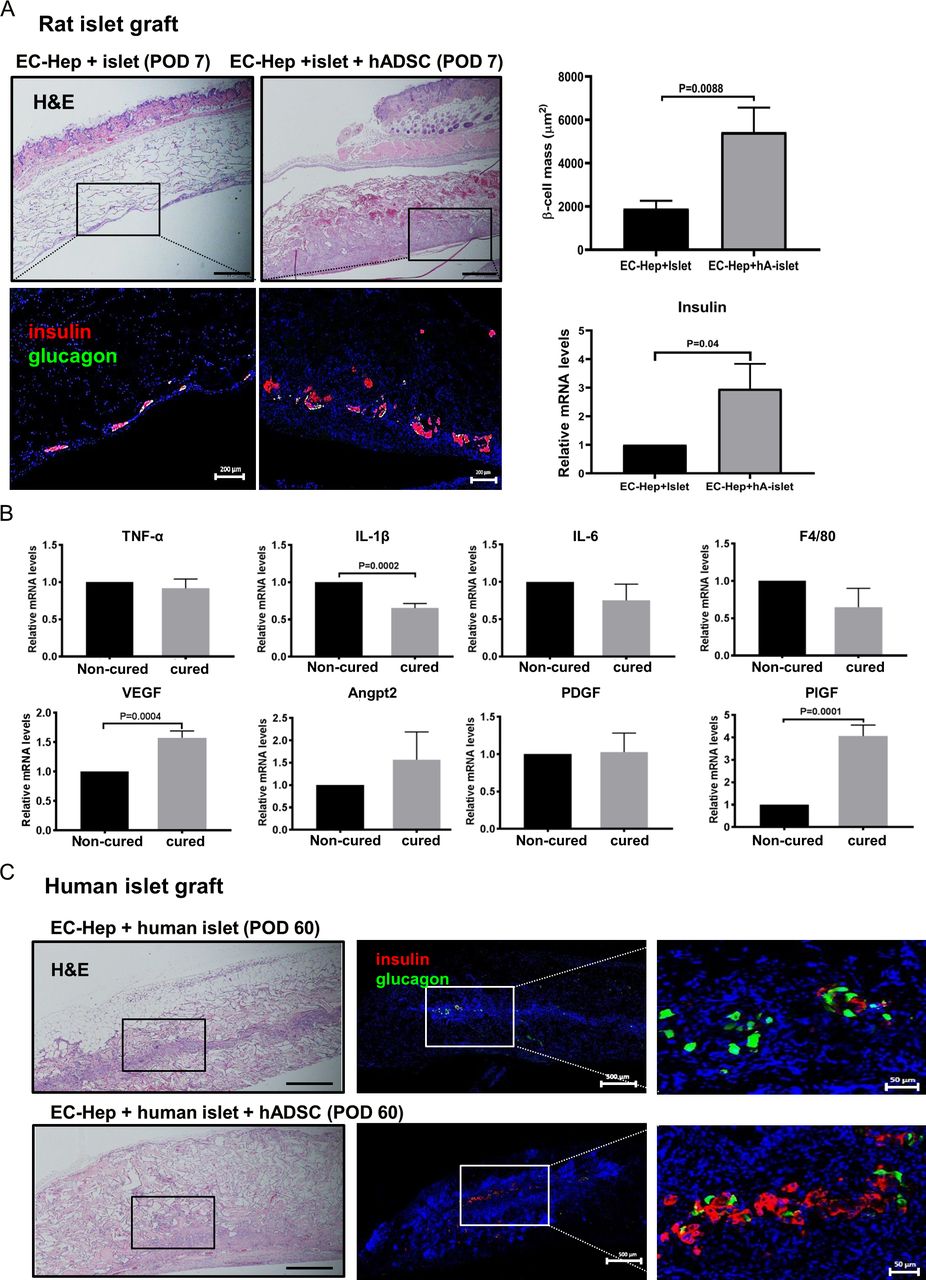
Furthermore, we surgically retrieved the implants and performed histological examinations to investigate the morphologies of the islet grafts. Immunohistochemical analysis confirmed the presence of insulin-stained islet grafts with well-preserved structure in the rat islet-hADSC (figure 5A) and human islet-hADSC (figure 5C) transplant group. The result indicated the benefit of hADSCs and EC-Hep in composing the islet sheet for the stable engraftment and glycemic control in the recipients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histological analysis and gene expression profile in grafts. (A) H&E and immunofluorescence staining of islet grafts after transplantation for 7 days. Immunofluorescence stained samples of representative sections from experimental groups (insulin: red, glucagon: green, nucleus: blue, with three sections for each mouse). Scale bars indicate 500 or 200 µm. The islet graft showed no preserved structures or weak insulin staining, whereas the heparin-esterified collagen-human adipose-derived stem cells (hADSC) (HCA)-islet sheet graft showed preserved structures and positive insulin staining. (B) mRNA levels of inflammatory and angiogenic factors in the diabetes mellitus non-cured group and cured group 7 days after transplantation. For proinflammatory cytokines, such as interleukin (IL)-1β, gene expression was significantly decreased and angiogenic vascular endothelial growth factor (VEGF) and placenta growth factor (PIGF) gene expression was significantly higher in the HCA-islet sheet group than in the islet group. Data are presented as mean±SEM. Analysis was done using unpaired two-tailed t-test. (C) H&E and immunofluorescence staining of human islet grafts after transplantation for 60 days. Staining is representative image. Right panel shows enlarged image. Scale bars indicate 500 or 50 µm. EC-Hep, esterified collagen-heparin; mRNA, messenger RNA; POD, postoperative days; TNF, tumor necrosis factor.
To assess the mechanisms underlying early graft loss, graft inflammation and vascularization were characterized by quantitative RT-PCR on day 7 after transplantation. F4/80 is a macrophage-specific marker and CD3 is expressed by T cells. Real-time PCR analysis for F4/80 and CD3 mRNA expression in the graft showed that F4/80 mRNA expression was slightly decreased in the cured group, compared with the non-cured group. However, CD3 mRNA expression was not expressed in both groups (figure 5B). In cured mice, interleukin (IL)-1β expression was lower, but the VEGF and PIGF mRNA expressions in the graft were significantly higher than in non-cured mice. Thus, the HCA-rat islet sheet may be beneficial for islet engraftment by preventing IL-1β-induced islet injury and promoting angiogenic ability.
Discussion
Recently, we reported that EC provides significant advantages in the long-term culture of islet cells compared with NC.11 Since heparin can recruit angiogenic factors by electrostatic interaction,23 we employed heparin by conjugating to the EC scaffolds. Indeed, our results showed that islets grown on the crosslinked EC-Hep scaffolds had better viability and function than did cells grown on the EC, or compared with the non-treated. Moreover, the presence of hADSCs within the scaffold significantly improved islet viability and function. These results indicate that hADSC and heparin act synergistically to enhance viability and function.
Although stem cells possess great potential for use in revolutionary therapies, there is a lot of concern about the potential for tumorigenic activity associated with their use. Ra et al investigated the potential toxicity and tumorigenicity of hADSCs in animals and humans, and reported that hADSCs are non-toxic and non-tumorigenic.24 We implanted hADSCs as a single subcutaneous injection into NOD scid gamma (NSG) mice to detect tumorigenicity in vivo. No tumor formation was observed in mice transplanted with hADSCs based on macroscopic and microscopic examinations (online supplementary figure S3a, c), whereas mice transplanted with induced pluripotent stem cells developed tumors (online supplementary figure S3b, d). Even with our data, the potential dangers of transplanting stem cells in scaffolds that cannot prevent cell escape remain to be addressed.
Angiogenesis in isolated islets can be stimulated by growth factors and local treatment at the transplantation site is assumed to be beneficial for revascularization and stable function of the islet graft.25 26 By using a growth factor array technique to evaluate the growth factors in EC-Hep and hA-islet culture medium, we found that hA-islet led to a marked increase in GDF-15, PIGF and VEGF level compared with islet alone. Furthermore, HCA-islet sheet significantly enhanced the release of multiple angiogenic growth factors such as HGF, IGFBP-2, IGFBP-6 and OPG at 7 days of culture. High levels of these angiogenic growth factors in the HCA-islet sheets are presumed to support and stimulate islet vascularization.
We investigated the effects underlying enhanced islet function and engraftment using in vivo transplantation of the HCA-islet sheet. Interestingly, islet engraftment was proportional to the doses of hADSCs, and the mice receiving a low dose of hADSCs and islets could not maintain normoglycemia. The hADSCs were crucial for the stable release of insulin, possibly because of their enhanced viability. HCA-islet sheet resulted in long-term survival (up to 100 days) in vivo on transplantation.
We attempt to verify our findings with human islet. Unlike the findings from rodent islet transplantation experiments, normalization of the BG level was not immediately apparent; rather, normalization was delayed because of the islets that were isolated from surgical specimens. BG levels in mice transplanted with HCA-human islet sheet were significantly lower compared with BG levels in mice transplanted with sheet containing only islets. Moreover, the HCA-human islet sheet transplant group had elevated serum human insulin levels compared with mice receiving only islet sheet. Although the numbers of experiments with human islet were limited owing to the restricted availability of intact human pancreatic tissue, our human islet data are consistent with the results obtained with rat islet.
Our results showed that elevated production of growth factors released from hADSCs loaded into an EC-Hep in islet grafts enhances revascularization, contributes to increased islet mass and improves glycemic control in the recipient mice. Indeed, the total number of blood vessels was significantly greater in the graft site implanted with HCA-islet sheet. This result was further supported by CD31 and αSMA immunostaining. VEGF is the most important gene involved in the regulation of blood vessel and PIGF is an angiogenic protein belonging to the VEGF family. PIGF stimulates angiogenesis by acting synergistically with VEGF.27 We observed a marked increase in the VEGF and PIGF levels in the cured group compared with the non-cured group. Elevated production of angiogenic factors locally in islet grafts promoted graft angiogenesis and enhanced islet revascularization, which contributed to significantly improved glycemic control and better preservation of islet mass in diabetic recipient.
There are considerable challenges in clinical trials concerning the scale-up of the device to human patients. In this experiment, we incorporated 8000 IEQ islets and 1×106 hADSCs in the 1×1 cm (1 cm2) patch. If we consider 10 000 IEQ/donor kg for successful allogenic islet transplantation by the portal vein route, and assume that the number of islets needed for subcutaneous implantation was the same or more, 600 000 IEQ will be required for a 60 kg donor and the required space would be 75 times greater than the space used in our experiment. Converted to size, a 7.5×10 cm patch would be needed. This size could be applied to the back or abdomen of patients. However, a decrease in size of the patch is important for the wider application of the patch in various parts of the body, such as axillary area and forearm. We are investigating the possibility of the three-dimensional spatial distribution of our platform.
Our study showed that the combined pancreatic islet cell and an adipose-derived stem cell sheet delivered by surface-immobilized heparin and an engineered collagen scaffold enhance islet revascularization and engraftment in an ADSC dose-dependent manner. The findings will hopefully be translated to clinical islet cell transplantation for the treatment of insulin-dependent diabetes mellitus.
References
Footnotes
YHK, JHK and SL contributed equally.
Contributors YHK: performed research and analyzed data, designed research and interpreted data, wrote the manuscript; JHK and SL: performed research and analyzed data, designed research and interpreted data; JYO, GSJ and S-NP: designed research and interpreted data; SCK and IKS: designed research and interpreted data, supervised data analysis and edited the manuscript.
Funding This work was supported by a grant from Ministry of Science, ICT & Future Planning (2017M3A9C6032060) and Asan Institute for Life Science (2018–7001).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Asan Medical Center Institutional Review Board (IRB: 2012–0244). All animal experiments were approved by the Institutional Animal Care and Use Committee of Asan Medical Center (IACUC-2014-13-217).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.