Article Text

Abstract
Objective To assess the prevalence of vitamin B12 deficiency in people with type 2 diabetes mellitus (T2DM) on metformin and without metformin.
Methodology Between May 2018 and January 2019, this prospective multicenter observational study recruited participants from seven centers in four provinces of Pakistan (Sindh, Punjab, Baluchistan and Khyber Pakhtunkhwa). Participants with T2DM treated with metformin for >2 years and those not on metformin underwent assessment of hemoglobin, vitamin B12, homocysteine and diabetic neuropathy (vibration perception threshold (VPT) >15V) and painful diabetic neuropathy (Douleur Neuropathique 4 (DN4) ≥4) and Diabetic Neuropathy Symptom (DNS) score ≥1.
Results Of 932 subjects, 645 (69.2%) were treated with metformin, while 287 (30.8%) were not on metformin. Overall, B12 deficiency (<200 pg/mL) was significantly higher in metformin users of 25 (3.9%), compared with non-metformin users of 6 (2.1%), while B12 insufficiency (200–300 pg/mL) was significantly lower in metformin users of 117 (18.4%) compared with non-metformin users of 80 (27.9%). Subjects with B12 deficiency and insufficiency with hyperhomocysteinemia (≥15) were found in 19 (76%) µmol/L and 69 (60.5%) µmol/L in metformin users compared with 6 (100%) µmol/L and 57 (73.1%) μmol/L in non-metformin users, respectively. VPT>25 and DN4 score ≥4 were significantly higher in B12-deficient metformin users compared with non-metformin users. Similarly, DNS score ≥1 was non-significantly higher in B12-deficient metformin users compared with non-metformin users.
Conclusion This study shows that vitamin B12 insufficiency was frequently found in our population and may progress into B12 deficiency. It is also associated with neuropathy in subjects on metformin. Further interventional studies to assess the benefit of B12 treatment on painful neuropathy in patients on metformin may be warranted. B12 levels may be checked in people with T2DM using metformin for >2 years.
- metformin
- blood glucose monitoring
- clinical research
- control
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Accumulating evidence suggests that metformin as the first choice of therapy for glycemic control may lead to low levels of serum vitamin B12.
What are the new findings?
Vitamin B12 insufficiency was frequently found in our population and may progress into B12 deficiency that is also associated with neuropathy in subjects on metformin.
How might these results change the focus of research or clinical practice?
In clinical practice, B12 levels may be checked especially in people with type 2 diabetes mellitus using metformin for >2 years to confirm B12 deficiency and/or B12 insufficiency.
Introduction
Worldwide, type 2 diabetes mellitus (T2DM) has affected an estimated 463 million people in 2019 and projected to reach 700 million by 2045, reported by the International Diabetes Federation (IDF).1 In the recent second National Diabetes Survey of Pakistan 2016–2017, the prevalence of diabetes was 26.3%.2 The American Diabetes Association (ADA), the European Association for the Study of Diabetes and the IDF recommend metformin as the first choice of therapy for glycemic control.1 3 Accumulating evidence from both observational and interventional studies has revealed that vitamin B12 deficiency may occur with metformin treatment.4 It has also been reported that vitamin B12 deficiency ranges from 9% to 52% in people with T2DM and has been partially attributed to long-term use of metformin.5–7
Vitamin B12 is essential for remethylation of homocysteine (Hcy) to methionine and B12 deficiency could lead to hyperhomocysteinemia, which has been associated with macrovascular complications in people with T2DM.8 B12 deficiency may also increase the severity of peripheral neuropathy in T2DM.9 However, reports are contradictory on the association between metformin-induced vitamin B12 deficiency and peripheral neuropathy.9–11 Furthermore, there are limited studies assessing metformin-induced vitamin B12 deficiency in people with T2DM12–14 and no such study assessing the relationship to diabetic neuropathy in Pakistan.
This study was undertaken to establish the prevalence of B12 deficiency in people with T2DM treated with metformin and its relationship to diabetic peripheral neuropathy (DPN) in Pakistan.
Methodology
This prospective multicenter observational study was conducted by Baqai Institute of Diabetology and Endocrinology (BIDE), Baqai Medical University (BMU), Karachi, Pakistan. Duration of study was between May 2018 and January 2019. An estimated sample size of 1000 subjects of which 750 have T2DM treated with metformin for >2 years and 250 non-diabetics without metformin was calculated. Subjects were selected from seven tertiary care centers across four provinces of Pakistan (Sindh, Punjab, Baluchistan and Khyber Pakhtunkhwa).
Subjects with a history of pernicious anemia, iron deficiency anemia, malabsorption (celiac disease, inflammatory bowel disease, gastrointestinal surgery), malnutrition (pure vegans, anorexia nervosa), history of thyroid disease and thyroxine treatment and/or a history of other organ-specific autoimmune conditions (vitiligo, Addison’s, primary ovarian failure, hypoparathyroidism), peripheral arterial disease and history of another cause of neuropathy were excluded. Subjects with previous gastric resection or bariatric surgery or on a vegetarian diet, who had received oral or intramuscular vitamin B12 supplementation, vitamin D supplementation, multivitamins, calcium supplements and proton-pump inhibitors (PPI) within the last 3 months, pregnancy and hearing or visual impairment or dementia were also excluded.
Baseline demographic and anthropometric details including age, gender, duration of metformin use, daily dose of metformin, blood pressure and body mass index (BMI) were noted using predesigned questionnaire. Blood samples were collected into a dedicated evacuated tube for biochemical parameters including hemoglobin (Hb), serum vitamin B12, and Hcy levels. From all centers, blood samples were transported to the laboratory of BIDE-BMU. Equipment used throughout the study were standardized with measure of quality assurance.
Vitamin B12 was analyzed using the Roche Diagnostic cobas e411 Immunoassay System—a fully automated, random access, software-controlled system for immunoassay analysis. The e411 vitamin B12 assay employs a competitive test principle using intrinsic factor specific for vitamin B12. In the sample, vitamin B12 competes with the added vitamin B12 labeled with biotin for the binding sites on the ruthenium-labeled intrinsic factor complex. Serum vitamin B12 >300 pg/mL was defined as normal, 200–300 pg/mL insufficient and <200 pg/mL as deficient.15
Subjects with vitamin B12 deficiency and insufficiency underwent assessment of Hcy levels (<15 µmol/L normal, ≥15 µmol/L hyperhomocysteinemia).16 17 Subjects underwent assessment of vibration perception threshold (VPT), Douleur Neuropathique 4 (DN4) score and Diabetic Neuropathy Symptom (DNS) score. VPT was measured on the pulp of the large toe on both right and left legs with a neurothesiometer.18 VPT was considered normal (<15V), intermediate (16–25V), and abnormal (>25V).19 The DN4 comprised 10 questions and a score ≥4 was used to define neuropathic pain.20 A DNS score ≥1 was considered to be indicative of neuropathy.21
Statistical analysis
Data analysis was performed in Statistical Package for Social Sciences (SPSS V.20). Student’s t-test, analysis of variance, χ2 test, and Fisher’s exact test were applied to check the significant difference between groups. Pearson’s correlation analysis was used to examine the relationship between vitamin B12 and other parameters. A two-tailed p value <0.05 was considered statistically significant.
Results
Out of 1000 sample size, 932 subjects were recruited of whom 287 (30.8%) were not on metformin supplementation and 645 (69.2%) were on metformin supplementation. The mean age of non-metformin users was 39.77±14.95 years and metformin users were 51.16±14.64 years. Metformin users had a higher BMI (27.91±5.12 vs 26.03±5.42, p<0.0001), systolic blood pressure (134.41±18.58 vs 126.94±18.06, p<0.0001) and diastolic blood pressure (81.61±13.62 vs 78±14.6, p=0.001). Hb was significantly lower in metformin users (13.41±2.32) compared with non-metformin users (14.05±2.3) (table 1).
Comparison of demographic, anthropometric and clinical characteristics between non-metformin users and metformin users
Overall, B12 deficiency (<200 pg/mL) was significantly higher in metformin users of 25 (3.9%) compared with non-metformin users of 6 (2.1%), while B12 insufficiency (200–300 pg/mL) was significantly lower in metformin users of 117 (18.4%) compared with non-metformin users of 80 (27.9%). Subjects with B12 deficiency and insufficiency with hyperhomocysteinemia (≥15) were found in 19 (76%) µmol/L and 69 (60.5%) µmol/L in metformin users compared with 6 (100%) µmol/L and 57 (73.1%) μmol/L in non-metformin users, respectively (table 2).
Vitamin B12 and homocysteine in non-metformin and metformin users
Either the VPT>25 or DN4 score ≥4 was significantly higher in B12-deficient metformin users compared with non-metformin users. Similarly, DNS score ≥1 was non-significantly higher in B12-deficient metformin users compared with non-metformin users (table 3).
Association of VPT, DNS and DN4 scores with B12 deficiency
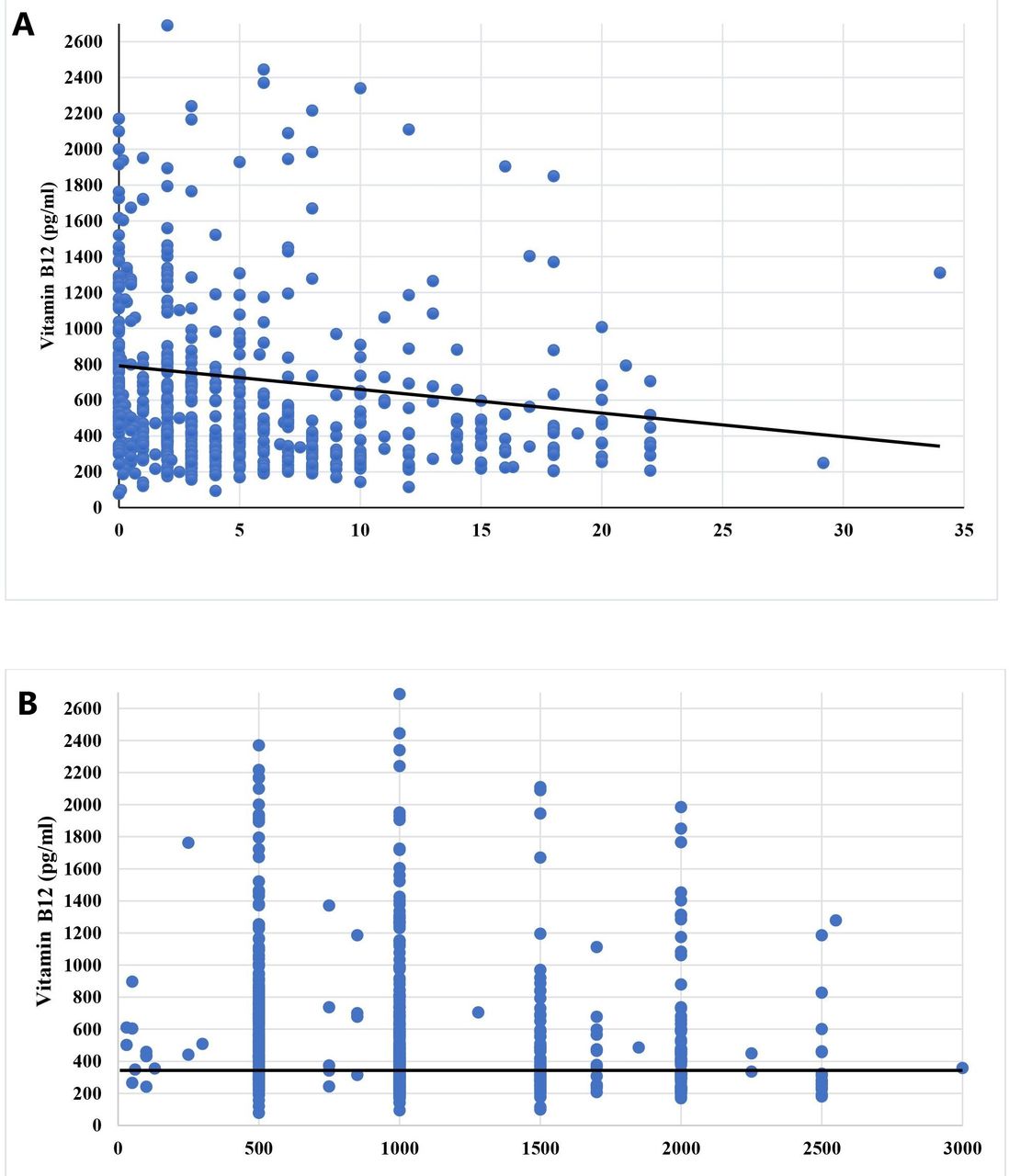
B12 levels were not associated with age (r=0.172, p<0.0001), BMI (r=−0.089, p=0.013), duration of diabetes (r=0.017, p=0.706), VPT (r=0.262, p<0.0001), DNS score (r=0.128, p<0.0001) and DN4 score (r=0.318, p<0.0001), while B12 levels were negatively correlated to duration of metformin use (r=−0.24; p=0.0001) (figure 1A), dose of metformin use (r=−0.21; p=0.0001) (figure 1B), HbA1c (r=−0.09, p=0.378) and Hcy levels (r=−0.147, p=0.038) (table 4).
Correlation between B12 and various parameters

{kind=link}
Correlation of vitamin B12 level with (A) duration and (B) dose of metformin in metformin users.
Discussion
This is the largest multicenter study to date assessing the relationship between metformin use and B12 deficiency, and its association with diabetic neuropathy. In this study, significantly increased prevalence of B12 deficiency was observed in people with T2DM treated with metformin as compared with non-metformin users.9 14 22 On contrary, B12 insufficiency was significantly higher in non-metformin users compared with metformin users. It indicates that B12 insufficiency was generally found in our population, and after initiation of metformin in people with diabetes, the B12 insufficiency may develop into B12 deficiency. Moreover, we observed that subjects with B12 deficiency have high VPT (>25), DNS score (≥1) and DN4 score (≥4) as compared with non-metformin users, similar to Algeffari and Singh et al’s studies.23 24 Indeed, Zalaket et al showed reversal of neuropathy after B12 supplementation.25
Regarding the clinical significance of biochemical vitamin B12 deficiency versus true tissue deficiency, a significant debate already exists. Up to now, the most commonly surrogate markers used for detection of vitamin B12 deficiency are plasma Hcy and methylmalonic acid.26 In our population, concurrently elevated Hcy levels were also observed in people with B12 insufficiency and B12 deficiency.27 However, measurement of additional biomarkers for more comprehensive assessment of B12 deficiency, such as holotranscobalamin, methylmalonic acid, red cell-B12, and plasma concentrations of methylation indices, is beyond the scope of our study.
Vitamin B12 deficiency is a multifactorial condition caused by insufficient intake (nutritional deficiency) as well as acquired or inherited defects that disrupt B12 absorption and processing pathways. Similarly, metformin-induced B12 deficiency is also thought to occur due to vitamin B12 malabsorption such as alteration of bile acid metabolism, small intestinal bacterial overgrowth, or effects on intrinsic factor secretion, but a more currently accepted explanation is the interference by metformin on calcium-dependent membrane action responsible for vitamin B12 intrinsic factor absorption in the terminal ileum.28 The use of PPIs is also thought to contribute to B12 deficiency, although this does not appear to be a factor in our study. Both observational and interventional studies have shown that the duration and dose of metformin are also associated with B12 deficiency and neuropathy.11 29 30 A recent study from Qatar, however, showed no association between metformin use and B12 deficiency or diabetic neuropathy.20 de Groot-Kamphuis et al have shown a lower prevalence of DPN in people with T2DM on metformin compared with those not on metformin.31 Our study confirms a weak but significant correlation between B12 levels and duration and dose of metformin. A significant association has also been found with age, gender, married individuals, BMI and blood pressure with B12 levels in metformin users.29 In the present study, the metformin users were significantly older, but no such association between age and B12 levels exists in related studies.11 32
In current study, significantly increased but low Hb levels were observed in metformin users compared with non-metformin users. In prior studies, the significant association between B12deficiency and low Hb concentration was also noted.33 34 Metformin-induced B12 deficiency has been attributed to alterations in small bowel motility and enhanced bacterial overgrowth or interference of metformin with calcium-dependent intrinsic factor release.35 To date, there are no guidelines recommending routine screening for B12 deficiency in T2DM subjects on metformin, although the recent ADA-ADA consensus guidelines recommended the assessment of B12 in subjects with DPN being treated with metformin.36
Strengths and limitations
This is a cross-sectional multicenter study and therefore a true cause effect between metformin use and B12 deficiency cannot be established. We have attempted to exclude other confounding factors, although the patients on metformin were older. We lack complete data regarding VPT, DNS score and DN4 score from all centers is our limitation. Glycemic control not being assessed is also a limitation of this study. All laboratory assessments were undertaken in a central lab and exactly the same protocols were used to assess for diabetic neuropathy and painful diabetic neuropathy.
Conclusion
This study shows that vitamin B12 insufficiency was frequently found in our population and may progress into B12 deficiency. It is also associated with neuropathy in subjects on metformin. Further interventional studies to assess the benefit of B12 treatment on painful neuropathy in patients on metformin may be warranted. B12 levels may be checked in people with T2DM using metformin for >2 years.
Acknowledgments
We acknowledge the support of Miss Kulsoom Baqa (research officer), Miss Nida Mustafa (statistician) and Miss Tooba Ghazdar (research coordinator) in Research Department and Laboratory Department of BIDE, Karachi, for data management, data entry and data analysis. We also acknowledge the cooperation of Hilton Pharma, Karachi, Pakistan, for providing financial support to the Research Department, BIDE.
References
Footnotes
Correction notice This article has been corrected since it was published. Name and affiliation of MIBD member has been corrected.
Collaborators MIBD members: (1) Sobia Sabir Ali, Assistant Professor, Department of Diabetes and Endocrinology, Lady Reading Hospital, Peshawar, Pakistan; (2) Khalid Usman, MRCP (UK), Associate Professor, Endocrinology, Post Graduate Medical Institute, Hayatabad Medical Complex, Peshawar, Pakistan; (3) Salma Tanveer, FCPS, Professor of Medicine, In-charge Diabetes and Endocrinology, Nishter Medical University, Multan, Pakistan; (4) Qazi Masroor, Professor of Medicine, Head of Department, Quaid-e-Azam Medical College, Bahawalpur, Pakistan; (5) Jamal Zafar, Professor of Medicine, Pakistan Institute of Medical Sciences, Islamabad, Pakistan; (6) Khursheed Ahmed, Consultant Physician, Zahid Medical Centre, Baluchistan, Pakistan; (7) Bilal Tahir, DDE, Research Coordinator and Diabetes Educator, Research Department, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Pakistan; (8) Asher Fawwad, PhD, Chairman and Professor of Biochemistry, Department of Biochemistry, Research Director, Baqai Institute of Diabetology and Endocrinology, Baqai Medical University, Karachi, Pakistan; (9) Rayaz A Malik, Professor of Medicine, Weill Cornell Medicine-Qatar, Qatar Foundation, Education City, Doha, Qatar.
Contributors ZM: concept, design, interpretation of data; wrote, edited and approved the final manuscript. NW: literature search, interpretation of data, wrote the manuscript. MIBD members: responsible for the supervision of the survey, concept, design, involved in the quality control and data management in their respective areas. All members approved the final submitted version.
Funding This work was supported by Hilton Pharma, Karachi, Pakistan, to the Research Department, BIDE.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Institutional Review Board (IRB) of BIDE (Reference No BIDE/IRB/DR.ZMIYAN/10/25/17/0181a).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.