Article Text

Abstract
Introduction Diabetic ketoacidosis (DKA) is a serious complication of diabetes. DKA is associated with poorer cognition in children with type 1 diabetes (T1D), but whether this is the case in older adults with T1D is unknown. Given the increasing life expectancy in T1D, understanding the role of DKA on brain health in older adults is crucial.
Research design and methods We examined the association of DKA with cognitive function in 714 older adults with T1D from the Study of Longevity in Diabetes. Participants self-reported lifetime exposure to DKA resulting in hospitalization; DKA was categorized into 0 hospitalization, 1 hospitalization or ≥2 hospitalizations (recurrent DKA). Global and domain-specific cognition (language, executive function/psychomotor speed, episodic memory and simple attention) were assessed. The association of DKA with cognitive function was evaluated via linear and logistic regression models.
Results Twenty-eight percent of participants (mean age=67 years; mean age at diagnosis=28 years; average duration of diabetes=39 years) reported a lifetime history of DKA resulting in hospitalization (18.5% single DKA; 9.7% recurrent DKA). In fully adjusted models, those with recurrent DKA had lower global cognitive function (β=−0.13; 95% CI −0.22 to 0.02) and lower scores on the executive function/psychomotor speed domain (β=−0.34; 95% CI −0.51 to 0.17). Individuals with recurrent DKA were also more likely to have the lowest level of cognitive function on the executive function/psychomotor speed domain (defined as 1.5 SD below the population mean; OR=3.26, 95% CI 1.43 to 7.42).
Conclusions Among 714 older adults with T1D, recurrent DKA was associated with lower global cognitive function, lower scores on the executive function/psychomotor speed domain and 3.3 times greater risk of having the lowest level of cognitive function in our sample on the executive function/psychomotor speed domain. These findings suggest that recurrent DKA may negatively impact the brain health of older patients with T1D and highlight the importance of DKA prevention.
- ageing
- cognition
- type 1
- ketoacidosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
The incidence of type 1 diabetes (T1D) and the life expectancy for those with T1D are both increasing resulting in a growing population of older adults living with T1D.
In children and adolescents with T1D, diabetic ketoacidosis (DKA) is associated with lower cognitive functioning.
In adults with type 2 diabetes, DKA increases risk of dementia.
What are the new findings?
Prevalence of lifetime DKA among older adults with T1D: In a population of 718 older adults with T1D, 28% reported lifetime exposure to DKA resulting in hospitalization.
Prevalence of recurrent DKA in older adults with T1D: Among those who reported DKA, 34% reported a recurrent event.
Recurrent DKA is associated with lower cognitive function scores in older adults with T1D: In older adults with T1D, recurrent DKA was associated with lower global cognitive function scores, lower executive function/psychomotor speed scores and greater likelihood of having the lowest level of cognitive function in our sample on the executive function/psychomotor speed domain.
How might these results change the focus of research or clinical practice?
These findings suggest that recurrent DKA may negatively impact the brain health of older patients with T1D.
They provide another significant reason to focus resources on preventing DKA, especially recurrent DKA, in those with T1D.
Background
Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes characterized by metabolic acidosis, increased ketone concentration and uncontrolled hyperglycemia (glucose >250 mg/dL). In the USA, among individuals with type 1 diabetes (T1D), DKA hospitalization rates are increasing at a rate of ~6% per year and rates of DKA at the time of presentation with T1D have risen from 35% in 2007 to 58% in 2017.1–3 This is in sharp contrast to lower and declining rates in countries such as Finland and Sweden where rates of DKA at diagnosis are closer to 20% and have been declining in recent decades.4–6
Data have consistently shown an association between a number of measures of hyperglycemia and cognitive function in those with T1D. Studies have reported an association between: (1) chronic hyperglycemia (measured via 14 years average hemoglobin (HbA1c) ≥7.5%) and cognitive impairment in middle-aged adults with T1D7; (2) higher HbA1c and higher average nocturnal glucose (measured using continuous glucose monitoring) and cognitive impairment in older adults with T1D8; and (3) long-term exposure to HbA1c ≥8% and increased dementia risk in older adults with T1D.9 Additionally, studies have reported a consistent association between presence of microvascular complications and cognitive impairment in middle-aged and older adults with T1D.7 8 Despite the robust literature on the association between hyperglycemia and microvascular complications and cognition in those with T1D, there are very few studies focusing on the association between DKA and cognitive function in T1D and those that do exist are primarily in children or animal models. In children with T1D, DKA is associated with lower verbal IQ and lower cognitive function on memory, visual and verbal domains.10 11 Studies in animal models have supported these findings with DKA in rats resulting in measurable decreases in cognitive function.12 Additionally, studies in children and animal models have found an association between DKA and altered brain structure, with DKA exposure associated with changes in cerebral white and gray matter.13 14 However, it is unknown if DKA exposure impacts cognitive function in later life. This is especially important as individuals with T1D are living longer than previously and are increasingly at risk for ageing-related diseases such as cognitive decline and dementia.15 In this study, we sought to examine the association between lifetime exposure to DKA and cognitive function among a cohort of older adults with T1D.
Methods
Study population
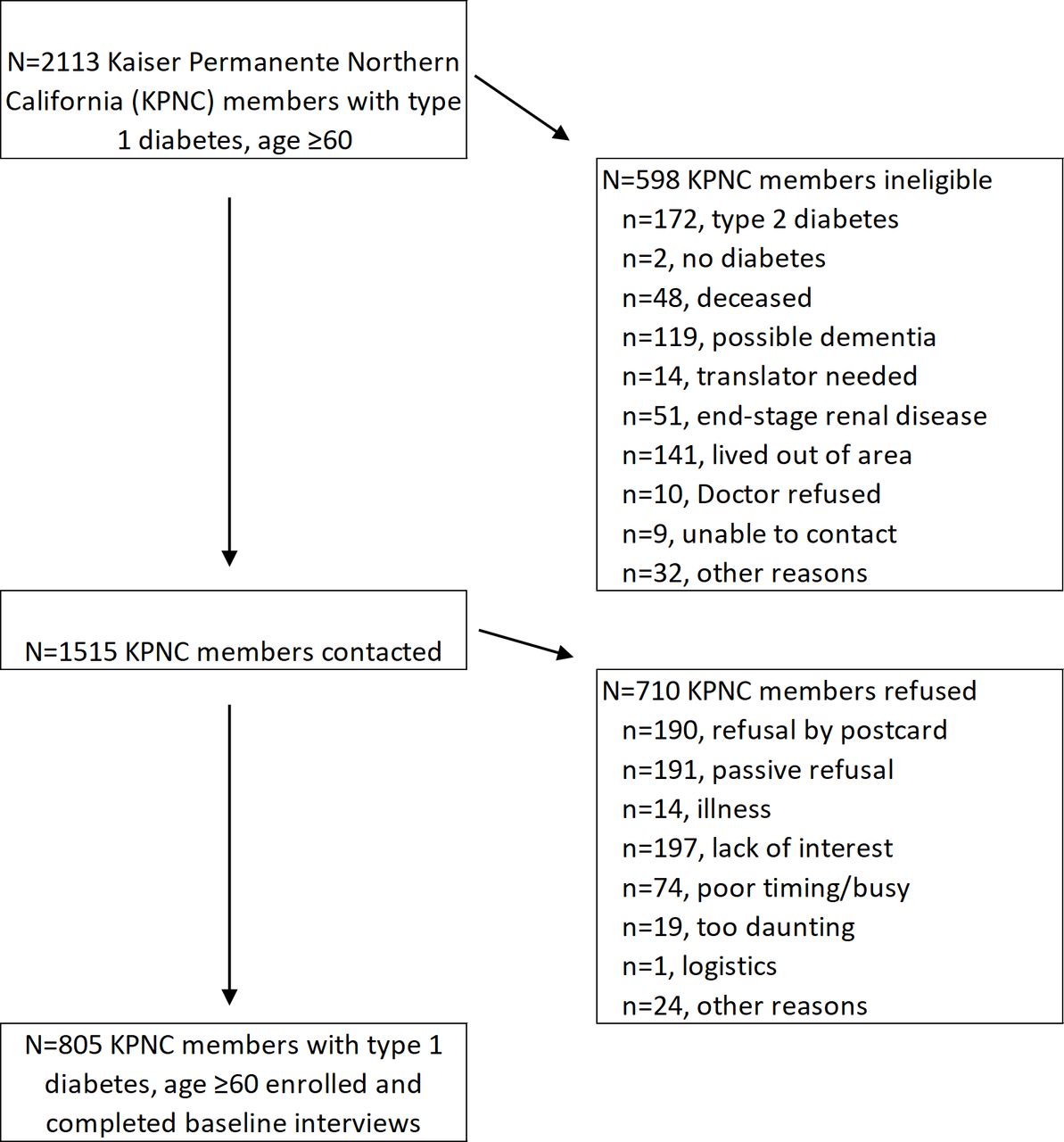
The Study of Longevity in Diabetes (SOLID) is a prospective cohort study of ageing and diabetes that recruited members of Kaiser Permanente Northern California (KPNC) aged 60 and older with T1D. The present analysis focuses only on baseline measures (completed August 2015 to June 2017). Details of eligibility and inclusion have been published previously.16 In brief, eligible T1D individuals were identified using International Classification of Diseases, Ninth Revision (ICD-9) and ICD-10 diagnosis codes extracted from their electronic medical record. Members were classified as having T1D if ≥75% of their diabetes-related diagnostic codes were for T1D (250.x1, 250.x3, or E10.x) and the member was prescribed insulin. Of the 2113 total KPNC members with T1D aged ≥60, 805 individuals were enrolled and completed baseline interviews (see figure 1 for study flow). All enrolled participants provided informed consent.
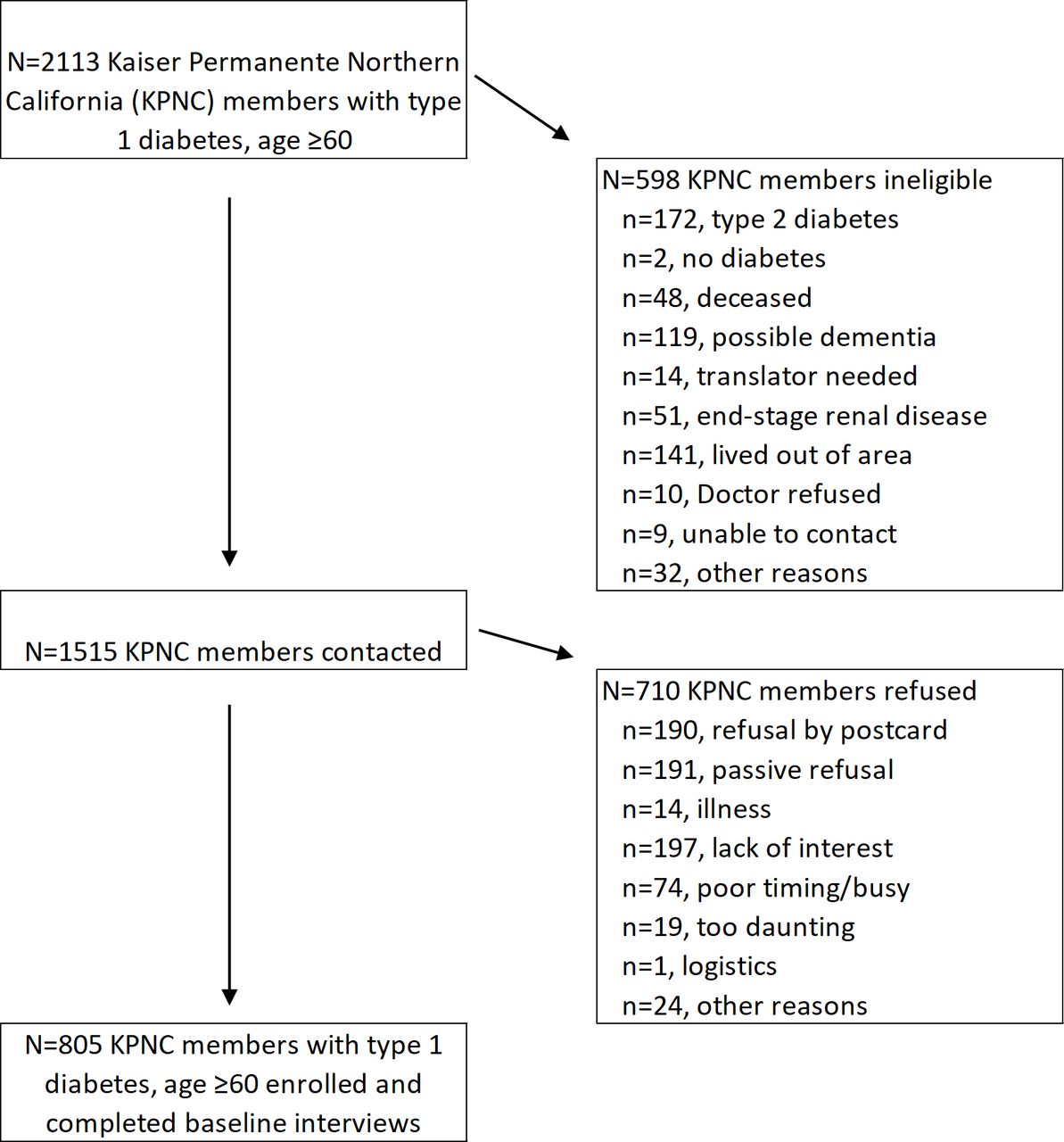
Study enrollment flowchart for participants with type 1 diabetes, the Study of Longevity in Diabetes (SOLID).
Self-reported lifetime DKA
Self-reported lifetime DKA resulting in hospitalization was captured at baseline interview. Among participants reporting any hospitalizations for DKA, they were further asked to quantify the number of times they had been hospitalized for this condition. DKA was categorized as 0 DKA hospitalization in their lifetime (no DKA), 1 DKA hospitalization in their lifetime (single DKA), or ≥2 DKA hospitalizations in their lifetime (recurrent DKA).
Cognitive function
At baseline interview, all participants were administered a comprehensive cognitive battery by trained interviewers. We conducted factor analysis on cognitive assessments from all participants with T1D through which four cognitive domains were identified: language, executive function/psychomotor speed, episodic memory, and simple attention (online supplementary table 1). The language domain comprised the phonemic fluency test (F and L),17 18 the category fluency test (animals and vegetables),19 20 list sorting (two alternative lists),20 21 and Multilingual Naming Test.20 22 The executive function/psychomotor speed domain comprised the Trail Making Test (A and B),20 23 the Digit Symbol Substitution Test,24 25 and the Stroop Color Word Test.26 The episodic memory domain encompassed Word List Learning Test (immediate and delayed)27 and the Benson Complex Figure Copy (immediate and delayed).20 28 The simple attention domain encompassed the Diamond and TMX cancellation tests.29 Each test score was converted to a z-score (mean=0; SD=1). For each domain, a summary score was calculated by summing the z-scores for individuals who completed at least 50% of the relevant tests. A global cognition score was calculated as the average of the four domain-specific summary scores for individuals who competed at least 50% of all cognitive function tests. We used a cut-off of 1.5 SD below the population mean to identify the subset of individuals in our sample with the lowest cognitive function on global and domain-specific scores.
Supplemental material
Covariates
Date of baseline interview and date of birth were used to calculate age at baseline interview. Age of diabetes onset was obtained via participant self-report and was used, in conjunction with age at baseline interview, to estimate diabetes duration. Sex was obtained from KPNC records. Race/ethnicity was based on self-report and was categorized into: White, Black, Hispanic, Asian and Other. Educational attainment was based on self-report and was categorized as: ‘College degree or greater’ or ‘Less than a College Degree’. Prevalent microvascular complications (retinopathy, nephropathy, and neuropathy) were captured through self-report of physician diagnosis at baseline. Participants also self-reported recent (past 12-month) history of severe hypoglycemia resulting in hospitalization.
Analytic sample
The present analysis uses baseline measures for the subset of participants with T1D. Of the 805 individuals with T1D who were enrolled in SOLID, we excluded 52 participants who were missing DKA measures, 33 participants who were missing the global cognition score and 6 participants who were missing key covariates, resulting in a final analytic sample of 714. The following numbers of people completed at least 50% of domain-specific cognitive test for the relevant domain and are included in analyses specific to those domains: language: 698 participants; executive function/psychomotor speed: 700 participants; episodic memory: 682 participants; simple attention: 700 participants.
Statistical analyses
First, we examined the distribution of baseline characteristics in the sample, overall and by DKA status using χ2 tests and one-way analysis of variance for categorical and continuous variables, respectively. Next, we examined mean standardized scores on global and domain-specific cognitive measures across categories of DKA exposure without covariate adjustment. We also examined mean standardized scores across categories of DKA exposure on the individual cognitive tests that comprised each domain. For our main analysis, we specified linear regression models to examine the association between lifetime DKA exposure and performance on global and domain-specific measures of cognition in a series of models with varying degrees of confounder adjustment. First, we fit a base model that was minimally adjusted (age at baseline interview, sex, race/ethnicity, educational attainment, diabetes duration; model 1). Next, to understand the potential contribution of DKA to cognitive dysfunction over and above the effects of prevalent microvascular complications and severe hypoglycemia, we fit three separate models with additional adjustment for (1) prevalent microvascular complications (retinopathy, nephropathy, neuropathy; model 2a); (2) recentexposure to severe hypoglycemia resulting in hospitalization (model 2b); and (3) combination of models 2a and 2b (retinopathy, nephropathy, neuropathy, and recent exposure to severe hypoglycemia resulting in hospitalization; model 3). Finally, we tested for potential effect modification of the association between DKA and cognition by gender, educational attainment (college degree or greater vs less than a college degree), and age at baseline interview by adding cross-product terms to the model. As a sensitivity analysis, we examined the association between DKA and cognitive function among participants with childhood-onset T1D (age of onset <7 and <18 years old).
In secondary analyses, to better understand the association between DKA and having the lowest level of cognitive function, we used a cut-off of 1.5 SD below the population mean as a threshold and used multivariable logistic regression models (adjusting for age at baseline interview, sex, race/ethnicity, education, diabetes duration) to examine the odds of having the lowest level of cognitive function in our sample associated with DKA. All analyses were performed using SAS V.9.4.
Results
In this sample of 714 older adults with T1D, 28.2% reported a lifetime history of DKA resulting in hospitalization (18.5% reported a single DKA event and 9.7% reported recurrent DKA; table 1).
Characteristics of older adults with type 1 diabetes from the Study of Longevity in Diabetes (SOLID) by lifetime exposure to diabetic ketoacidosis (DKA) resulting in hospitalization
Among participants with any DKA in their lifetime, 34% reported recurrent DKA. The average age of participants at the time of baseline exam was 67.2 years (SD 6.4), the average age at T1D diagnosis was 28.2 years (SD 15.2), and the average duration of diabetes was 38.9 years (SD 15.1). Compared with participants with no DKA, participants with recurrent DKA reported a significantly younger age at T1D diagnosis (22.2 years (12.7 SD) vs 29.2 years (15.5 SD) for those with no DKA; p=0.001) and a significantly longer duration of T1D (44.2 years (12.3 SD) vs 38.2 years (15.5 SD) for those with no DKA; p=0.01). Those with recurrent DKA were also more likely to be female (71.0% vs 47.0% for those with no DKA; p=0.0002) and to report a history of retinopathy (72.1% vs 38.6% for those with no DKA; p=<0.0001), nephropathy (18.0% vs 7.1% for those with no DKA; p=0.03), and severe hypoglycemia resulting in hospitalization (66.7% vs 46.8% for those with no DKA; p=0.01).
Findings revealed differences in cognitive function by DKA exposure status on measures of global cognition as well as on the executive function/psychomotor speed domain with the lowest scores observed in individuals with recurrent DKA (figure 2). No differences in cognitive function were observed by DKA status on the language, episodic memory or attention domains. We observed statistically significant differences in standardized cognitive scores across categories of DKA exposure for each of the four cognitive tests that comprise the executive function/psychomotor speed domain (Trail Making Test (A and B), the Digit Symbol Substitution Test, and the Stroop Color Word Test; all p<0.05; online supplementary table 2); no significant differences were observed on any other tests.

{kind=link}
{kind=link}
Mean standardized cognitive scores across categories of lifetime exposure to diabetic ketoacidosis resulting in hospitalization. All scores are unadjusted. DKA, diabetic ketoacidosis.
In linear regression models adjusting for age, sex, race, diagnosis age, education, and diabetes duration (table 2; model 1), compared with individuals with no DKA, those with recurrent DKA had lower scores on global cognition function (β=−0.17, 95% CI −0.28 to 0.06) and on the executive function/psychomotor speed domain (β=−0.40, 95% CI −0.57 to 0.23). These associations were slightly attenuated, but remained statistically significant, with additional adjustment for recent exposure to severe hypoglycemia (model 2a), prevalent microvascular complications (retinopathy, neuropathy and nephropathy; model 2b), and simultaneous adjustment for both recent severe hypoglycemia and prevalent microvascular complications (model 3). In fully adjusted models (model 3), those with recurrent DKA had lower global cognitive function (β=−0.13; 95% CI −0.22 to 0.02) and lower scores on the executive function/psychomotor speed domain (β=−0.34; 95% CI −0.51 to 0.17). There was no evidence of effect modification by sex, educational attainment, or age at baseline interview (all p>0.20).
Association between exposure to lifetime diabetic ketoacidosis (DKA) resulting in hospitalization and cognitive function among older adults with type 1 diabetes
As a sensitivity analysis, we examined the association between DKA and cognitive function among those with childhood-onset T1D (<18 and <7 years old). In our sample of older adults with T1D, 205 participants (28.7%) had childhood-onset T1D (<18 years old); of those with childhood onset, 33 participants (16.1%) had an age of onset <7 years old. Findings from this sensitivity analysis largely reflected our overall findings, however the association between DKA and cognitive function was of a greater magnitude among those with age of onset <7 years old than in the overall sample (global cognition: β=−0.73; 95% CI −1.36 to 0.10; executive function/psychomotor speed: β=−0.98; 95% CI −1.86 to 0.10; online supplementary table 3).
When examining cognitive function as a binary outcome, findings revealed a similar pattern of risk with a strong association between recurrent DKA and having the lowest cognitive function in our sample on the executive function/psychomotor speed domain (OR=3.26, 95% CI 1.43 to 7.42; table 3) and no significant association between DKA and the lowest global cognitive function cognition or on any other domain.
Association between exposure to recent and lifetime diabetic ketoacidosis (DKA) and having the lowest cognitive function in our sample (1.5 SD below population mean)
Discussion
In this study of older adults with T1D, recurrent DKA was associated with poorer cognition. Recurrent DKA was associated with significantly lower scores on global cognitive function, in a range of models with varying levels of adjustment, including presence of microvascular complications and recent exposure to severe hypoglycemia. The most robust association was observed between DKA and executive function/psychomotor speed. Those with recurrent DKA were also 3.3 times more likely to have the lowest cognitive function (defined as 1.5 SD below the population mean) on the executive function/psychomotor speed domain.
To our knowledge, this is the first study to investigate the association between lifetime exposure to DKA and cognitive function in older adults with T1D. Our results complement previous studies in children and adolescents with T1D that have reported an association between DKA and cognitive dysfunction (specifically with memory domains),13 14 16 30 31 and a recent study reporting an increased risk of dementia associated with exposure to DKA in those with type 2 diabetes.32 It also supports findings from a small pilot study (n=38) among middle-aged adults with T1D that found evidence of a gradient association between number of DKA episodes and changes in cognitive function, brain structure and metabolite concentration.33 However, it was previously unknown if lifetime DKA exposure would be associated with cognitive function in older adulthood.
The pathways through which DKA influences cognitive function in the short term have been previously characterized in children and adolescents with T1D. DKA is associated with acute changes in the brain, including neuronal dysfunction (evidenced by reduced N-acetylaspartate/creatinine ratio)13 ,34 and cerebral edema.35 36 One study examined the neurologic impact of recurrent DKA events in T1D and found that, while neuronal function returned to baseline (pre-DKA) levels following one DKA event, after the second DKA event, neuronal function recovered partially, but did not return to prebaseline levels; they conclude that this suggests that recurrent DKA may result in progressive neurologic decline.34 Altered brain growth has been observed up to 4 years after the DKA occurrence in children with T1D.14 37 DKA has been associated with reduced cerebral blood flow, brain cell swelling, and alterations in hippocampal function in animal model studies.38 39 Taken together, these prior studies provide support that cognitive impairment due to DKA may stem from subtle cerebral injury resulting from neuronal dysfunction, reduced cerebral blood flow and/or subclinical cerebral edema.
Of note is the lack of an association between cognition and DKA in those with a single DKA event in their lifetime. Among those with T1D, as many as 58% of individuals have DKA at the time of initial diagnosis with T1D.1–3 Though data are limited, estimates suggest that approximately 20% of patients who experience DKA will go on to experience recurrent DKA40; in the present study 34% of participants who reported any lifetime exposure to DKA went on to experience recurrent DKA. Despite overall improvements in DKA-related mortality, recurrent DKA is still associated with significantly higher mortality rates and early death.40 41 It is possible that recurrent DKA has a cumulative negative impact on both mortality and brain health that single DKA does not; this is an area for future study. It is also possible that the timing of the DKA occurrence during a person’s lifetime modifies its effect on cognitive function; for example, if DKA occurs when a person is young, during a time of critical neurodevelopment, the impact of DKA may be greater than if the DKA occurs later in life. This is another important area for further research.
Another notable finding from our study was the indication that the magnitude of the association between recurrent DKA and cognitive dysfunction was strongest among individuals with childhood-onset T1D (age of onset <7 years old). The magnitude of the associations between recurrent DKA and global cognitive scores and scores on the executive function/psychomotor speed domain was nearly three times greater in those with T1D onset <7 as compared with the overall sample. Prior studies have shown that cognitive dysfunction is greater among those with childhood-onset T1D,42 yet the few studies of T1D in older adults do not have many individuals with childhood onset.8 Indeed, in our study only 33 participants (4.6%) had T1D onset <7 years old. But, among this group, recurrent exposure to DKA was associated with highly significant deficits in cognition. Whether this is a reflection of actual increased risk of cognitive dysfunction resulting from DKA or a reflection of cognitive impairment leading to increased DKA is an area for future study.
This study has a number of strengths including the large sample of ageing patients with T1D, and the ability to adjust for age at diagnosis, duration of T1D, and presence of microvascular complications and severe hypoglycemia. Additionally, the comprehensive cognitive battery allows us to examine the association of DKA with cognition on specific cognitive domains and to show that DKA may affect them differentially. A key limitation of the study is that the exposure to DKA hospitalizations is self-reported and thus may be affected by recall bias. However, this might have been reduced by the focus on severe cases of DKA (those resulting in hospitalization) rather than more mild forms of DKA. A related limitation is that we are unable to ascertain the timing of the DKA occurrences. Participants self-reported DKA exposure over their lifetime but we did not collect data on the timing of these events. Additionally, because the data in this study are cross-sectional we were unable to determine the directionality of the association between DKA and cognitive function. Individuals with poorer cognitive function may have difficulties in managing diabetes self-care and, thus, may be more likely to experience DKA. Additionally, in the present study, we did not have access to HbA1c lab data, a measure which we have previously shown to be associated with dementia risk in older adults with T1D.9 Given our inability to adjust for HbA1c, it is possible that part of the association between cognitive function and DKA may actually be explained by differences in glycemic control. Finally, the participants with T1D in the SOLID study are majority White and well educated, which potentially limits the generalizability of our findings to other populations of older adults with T1D. Despite this limitation, the SOLID study is one of the largest cohort studies of older adults with T1D to date and is well poised to contribute to our understanding of the complex nature of ageing and cognition among individuals with T1D who have been living with this disease for an average of 40 years.
In light of our findings, it is important to underscore the fact that hospitalizations for DKA, particularly for recurrent DKA, are largely preventable. For example, in the UK, structured education programs and multipronged support programs that coordinate care have been shown to reduce DKA hospitalizations.43 44 In the USA, one such example is the Novel Interventions in Children’s Healthcare program which used targeted diabetes-specific text messages to engage youth with T1D and their caregivers; participation in the program resulted in lower rates of DKA.45 A recent commentary in Diabetes Care summarizes prevention programs for DKA and highlights the need for increased prevention efforts for this serious complication.46 Of note, however, we are not aware of any DKA prevention programs that are specifically targeted to older adults with T1D; any prevention efforts in this population would need to consider the complex inter-relationships between ageing, cognitive function, self-care, hypoglycemia and DKA to ensure that efforts targeted towards reducing DKA are effective and do not increase risk for other complications.
In summary, the incidence of both T1D and DKA is increasing. People with T1D are living longer and are at risk for ageing-related health risks such as dementia and cognitive decline. In this study, we identified recurrent DKA as a potential risk factor for poor cognitive function in older adults with T1D. Understanding the long-term impact of DKA on the brain is an important first step. Future studies should identify ways to decrease exposure to DKA in T1D, especially recurrent DKA exposure.
Acknowledgments
The authors gratefully acknowledge funding from the National Institutes on Aging.
References
Footnotes
Presented at Preliminary results from this study were presented at the American Diabetes Association 79th Scientific Sessions, San Francisco, CA: 7–11 June 2019.
Contributors MEL conducted the analyses, wrote the manuscript and assisted with study design/data interpretation. PG, CWE, MSB and AJK assisted with study design/data interpretation and reviewed/edited the manuscript. RAW obtained funding, assisted with study design/data interpretation, and reviewed/edited the manuscript. MEL is the guarantor of this work.
Funding The study received funding from the National Institutes on Aging (NIA R01 AG047500; RAW). MEL and CWE were supported by the UCSF Training for Research on Aging and Chronic Disease (T32 AG049663). MEL was also supported through contract PPRN-1306-04709 from the Patient-Centered Outcomes Research Institute (PCORI).
Disclaimer The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of this report.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Kaiser Permanente Northern California Institutional Review Board (project number: 1276423).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified data from participants in the Study of Longevity in Diabetes (SOLID) are available upon request/approval. For information, please contact the Whitmer Lab at UC Davis: https://rachelwhitmer.ucdavis.edu/contact-0