Article Text

Abstract
Metabolic syndrome (MetS) is a multifarious metabolic disorder that could severely damage multiple organs. The emergence of MetS has markedly increased medical burden for patients. The treatment of MetS involves multitarget regulation, which is the advantage of traditional Chinese medicine (TCM). Many high-quality studies related to TCM for MetS have been conducted in recent years; however, no overall efficacy analysis has been reported. To evaluate the efficacy and safety of TCM against MetS, we reviewed randomized controlled trials of MetS published in the past decade and then selected and analyzed 16 high-quality articles from over 800 papers. The results showed that TCM might be beneficial in improving body weight as well as in regulating glucose and lipid metabolisms; thus, TCM might be an ideal alternative therapy for MetS management. Treatment safety was also estimated in our analysis. A more elaborately designed and long-term observation of TCM for MetS should be performed in the future.
- metabolic syndrome
- traditional Chinese medicine
- high-quality study
- blood glucose
- randomized controlled trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- metabolic syndrome
- traditional Chinese medicine
- high-quality study
- blood glucose
- randomized controlled trials
Introduction
Metabolic syndrome (MetS) is a cluster of risk factors often diagnosed by the co-occurrence of three out of the four following medical conditions: abdominal obesity, hypertension, hyperglycemia (diabetes mellitus (DM) or impaired glucose regulation) and dyslipidemia (hypertriglyceridemia or low high-density lipoprotein (HDL) cholesterol).1 The prevalence of MetS in high-income countries is estimated to exceed 25% of the adult population.2 Moreover, the increased rate of MetS in low-incomed countries is dramatic.3 MetS is regarded as a risk factor for the development of type 2 diabetes mellitus (T2DM),4 cardiovascular disease,5 stroke,6 polycystic ovary syndrome, non-alcoholic steatohepatitis7 and cancer,8 which may all lead to mortality.9 MetS pandemic may cause heavy social and economic burden. Thus, establishing an effective strategy to prevent MetS is urgent. MetS treatment involves an all-round approach aimed to retard weight gain, improve insulin resistance and dyslipidemia, and control blood glucose and blood pressure.10–16 Moreover, during treatment, the dosage of each drug must be evaluated because as the disease progresses, conventional agents often gradually lose their efficacy. Novel treatments for MetS, such as sodium glucose transporter-2 inhibitors, seem to be potential candidate drugs, but they need validation.17
For the treatment of MetS, traditional Chinese medicine (TCM) has a unique advantage owing to its holism concept and multitarget regulation. Several randomized controlled trials (RCTs)18–33 have shown the curative effect of TCM on MetS, with some studies focusing on the independent component of MetS. A multicenter, randomized, positive-controlled, R open-label clinical trial proved that the Chinese herb decoction Jiangtangtiaozhi (JTTZ) improves blood glucose and lipid metabolism, as well as reduces body weight.34 Another study also showed that JTTZ ameliorates T2DM with hyperlipidemia by enriching beneficial bacteria.35 Furthermore, TCM has been reported to be efficacious and safe for hyperlipidemia-associated diseases, as it mediates lipid metabolism disorders.36 Regarding obesity, TCM has been reported to be more effective than placebo or lifestyle modification in reducing body weight, showing similar efficacy but fewer side effects compared with antiobesity drugs.37 Other multicenter RCTs suggested that, compared with conventional pharmaceutical treatment, TCM as an add-on therapy exerts favorable effects on obesity-related hypertension.38 However, not all of the above-mentioned findings were obtained from a high-quality study with a sufficient number of participants or with subjects precisely diagnosed with MetS. Considering these limitations, we selected high-quality studies (according to the Jadad Scale) published in the past decade to evaluate the efficacy of TCM on MetS through an updated systematic review and meta-analysis.
Materials and methods
Search strategy and data sources
This review was conducted under the guideline of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Relevant clinical trials were identified by searching for papers published from January 2009 to December 2019 in the following databases: Web of Science, PubMed, Embase, MEDLINE, Cochrane Library, International Pharmaceutical Abstracts, Global Health, Sinomed, China National Knowledge Internet (CNKI), WanFang and VIP. Search terms included the following: (“metabolic syndrome” or “MetS” or “metabolism syndrome”) and (“randomized controlled trial” or “controlled clinical trial” or “random” or “randomly” or “randomized” or “control” or “RCT”) and (“TCM” or “traditional Chinese medicine” or “Chinese medicinal herb” or “Chinese herbal medicine” or “decoction” or “formula” or “prescription” or “Chinese patent medicine” or “Chinese patent drug” or “Chinese herbal compound prescription”).
Study selection
We included clinical trials that satisfied the following criteria: (1) studies where the participants had a definite diagnosis of MetS and were randomly assigned to receive TCM and Western medicine/placebo; (2) studies with a sample size of ≥60; (3) studies with a treatment duration of ≥12 weeks; (4) studies designed to focus on comparing TCM and Western medicine, or TCM and placebo; (5) studies that included efficacy evaluation on glycosylated hemoglobin (HbA1c), fasting plasma glucose (FPG) and 2-hour postprandial blood glucose (2hPG) for blood glucose; body mass index (BMI) and waist circumference (WC) for obesity; total cholesterol (TC), triglyceride (TG), low-density lipoprotein (LDL) cholesterol, and HDL for lipids; as well as systolic blood pressure (SBP) and diastolic blood pressure (DBP) for blood pressure; (6) studies that were designed to be RCTs; and (7) studies where methodological quality was evaluated for each study with the Jadad score from 4 to 7 (the strongest).39 We excluded clinical studies with the following features: (1) studies that were non-randomized, (2) studies where patients were enrolled with no definite diagnosis, (3) studies that reported only symptomatic changes in patients without laboratory indicators and (4) studies with a Jadad score of <4.
Statistical analysis
Data were analyzed using the RevMan V.5.3 software.40 Continuous outcomes were pooled for calculation of weighted mean differences accompanied by 95% CIs. Categorical outcomes were pooled for calculation of relative risks (RRs) accompanied by 95% CIs. I2 statistics were used to measure heterogeneity. A fixed-effect (FE) model was used if I2 was <50%; otherwise, the random-effect (RE) model was used. Publication bias was explored by means of funnel-plot analysis.
Results
A total of 806 potentially relevant articles were identified during database searching (155 from CNKI, 239 from WanFang, 74 from VIP, 84 from Sinomed, 59 from Web of Science, 50 from PubMed, 50 from MEDLINE, 36 from Cochrane and 59 from Embase). Of these, 372 records were excluded because they were duplicates and 363 were excluded based on the titles and abstracts. A total of 71 articles were extracted from the second-round screening, and, finally, 16 articles remained after the full texts were assessed for eligibility: 14 in Chinese and 2 in English. A flow diagram of the screening is shown in online supplementary figure 1. In total, 1898 patients with MetS from 16 RCTs were included. All characteristics of the included RCTs are displayed in table 1, while the quality assessments and the pharmacological effects of TCM ingredients are summarized in online supplementary tables 1 and 2.
Supplemental material
Supplemental material
Summary of the included studies
TCM versus placebo
Eleven RCTs that investigated TCM efficacy on MetS were analyzed. Sample sizes ranged from 60 to 169 patients, and the intervention duration was 12 weeks. The methodological quality of the studies was assessed by Jadad scores from 4 to 7. The TCM interventions used for MetS included empirical decoctions and Chinese patent drugs combined with basic treatment, including health education, oral hypoglycemic agents, oral antihypertensive agents, and dyslipidemia drugs.
Results of obesity-related indicators indicated that TCM is more efficacious than placebo in reducing BMI (n=1123, RR −1.01, 95% CI −1.71 to 0.32; figure 1) and that TCM decreases WC (n=851, RR −1.65, 95% CI −2.61 to 0.69; figure 2). Liu and Cui33 investigated the efficacy of Wenpi Fuzhen decoction in 70 patients with MetS. Patients in the treatment group lost more weight than those in the control group and showed decreases in BMI and WC compared with those in the control group (p<0.01 and p<0.05). Wang et al25 enrolled 96 patients with MetS with T2DM. All patients were measured for BMI, WC and waist-to-hip ratio (WHtR) to assess obesity; the results showed that these parameters decreased significantly in the treatment group (p<0.01) with significant differences compared with the control group (p<0.05 and p<0.01). The content of each component was also measured; it was shown that patients with central obesity had improved control with Yiqi Huaju formula (p<0.01). In a multicenter, randomized, double-blind, parallel-controlled trial, Wang31 found that the BMI of patients treated with Jiangtang pill significantly declined from 26.68±2.30 to 23.41±2.16 kg/m2 compared with that of those treated with placebo (p<0.01) (table 2).

Data summary of the high-quality RCTs of TCM interventions for BMI. BMI, body mass index; RCT, randomized controlled trial; TCM, traditional Chinese medicine.

Data summary of the high-quality RCTs of TCM interventions for WC. RCT, randomized controlled trial; TCM, traditional Chinese medicine; WC, waist circumference.
Representative formula and components and potential mechanisms
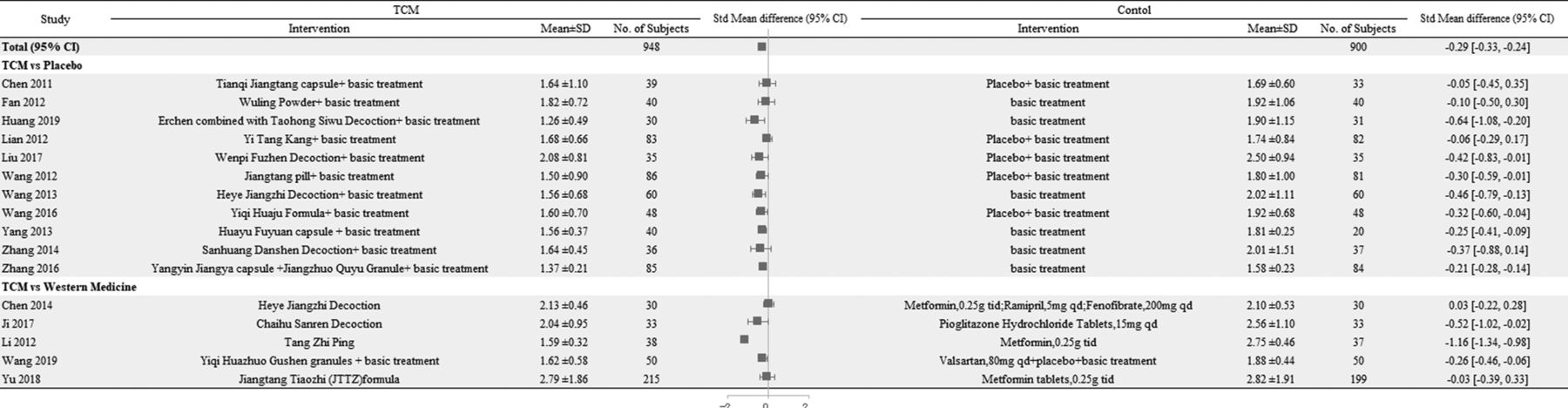
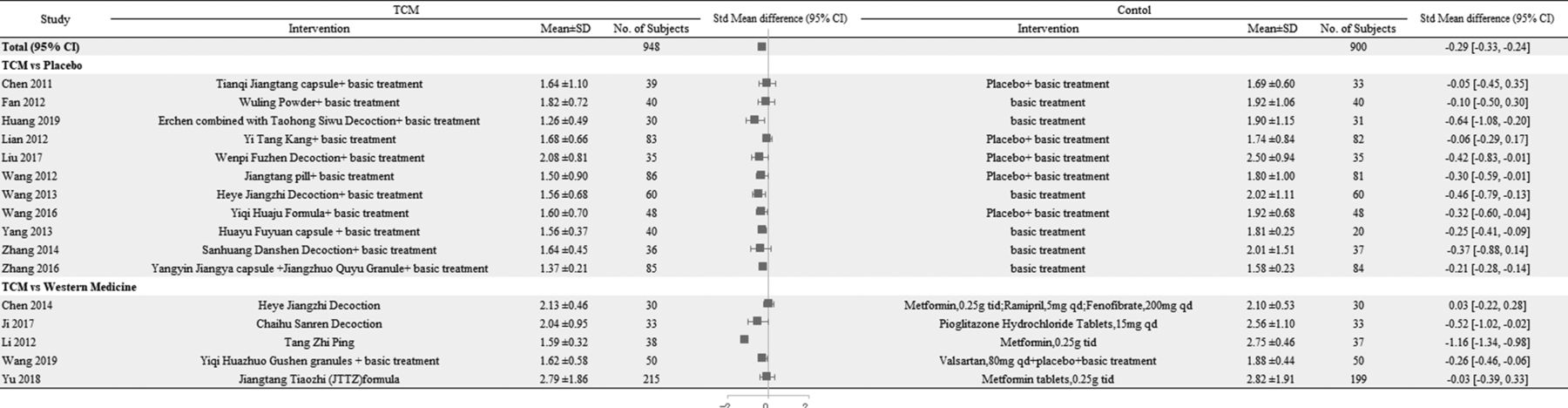
Regarding blood glucose indicators, the efficacy of TCM in reducing HbA1c is shown in figure 3 (n=820, RR −0.25, 95% CI −0.45 to 0.06). The hypoglycemic effect of TCM on FPG and 2hPG is shown in online supplementary figure 2 (n=1183, RR −0.31, 95% CI −0.40 to 0.22) and in online supplementary figure 3 (n=1062, RR −0.68, 95% CI −0.85 to 0.50). Analysis of fasting insulin (FINS) revealed that TCM improved islet function (n=343, RR −1.50, 95% CI −2.17 to 0.83; online supplementary figure 4). The efficacy of TCM in improving insulin resistance was observed by homeostasis model assessment of insulin resistance (HOMA-IR) (n=528, RR −0.46, 95% CI −0.68 to 0.25; online supplementary figure 5). In a multicenter RCT,20 165 patients with MetS with impaired glucose regulation (IGR) were treated with Yi Tang Kang or placebo. The results showed that Yi Tang Kang effectively lowered FPG and 2hPG (p<0.01), especially 2hPG (p<0.01). Another multicenter, double-blind, placebo-control RCT32 recruited 112 patients with MetS with impaired glucose tolerance (IGT) who received Tianqi Jiangtang capsule, which was recommended in the China Guideline for Type 2 Diabetes (2017); 55 IGT patients recovered after more than 3 months of treatment. FPG and 2hPG in the treatment group decreased after treatment with Tianqi Jiangtang capsule (p<0.05), and the efficacy of this TCM on 2hPG was more remarkable than that of the control (p<0.05). Wang et al. (2012)31 also enrolled patients with MetS with IGR who were treated with Jiangtang pill. The data indicated that Jiangtang pill effectively reduced 2hPG, regardless of age difference (p<0.01). Wang et al. (2013)22 reported that Heye Jiangzhi Decoction decreased FINS (p<0.01) and improved HOMA-IR (p<0.05).

Data summary of the high-quality RCTs of TCM interventions for HbA1c. HbA1c, glycosylated hemoglobin; RCT, randomized controlled trial; TCM, traditional Chinese medicine.
Analysis of blood lipid indicators revealed that TCM reduced cholesterol (n=1073, RR −0.27, 95% CI −0.44 to 0.10; online supplementary figure 6) and diminished TG (n=1133, RR −0.23, 95% CI −0.28 to 0.17; figure 4). Changes in LDL and HDL were also observed, suggesting that TCM decreased LDL (n=1072, RR −0.19, 95% CI −0.27 to 0.11; online supplementary figure 7) and increased HDL (n=1132; RR 0.10; 95% CI 0.02, 0.18; online supplementary figure 8). Wang et al. (2013)22 showed that Heye Jiangzhi Decoction decreased TC (p<0.01) and increased HDL (p<0.05), with an efficacy rate of 85% in regulating blood lipids. Another survey23 reported that Erchen combined with Taohong Siwu Decoction showed preponderant efficacy in regulating TC, TG (p<0.01), and LDL (p<0.05), but its effect on HDL was not different than that of placebo (p>0.05). Fan et al (2012)29 showed that a classical formula of Wuling Powder increased LDL to a greater degree compared with placebo (p<0.01). Zhang et al. (2014)26 also showed that TCM decoction reduced TG and TC (p<0.05), indicating its potent efficacy in regulating lipid metabolism.
Data summary of the high-quality RCTs of TCM interventions for TG. RCT, randomized controlled trial; TCM, traditional Chinese medicine; TG, triglyceride.
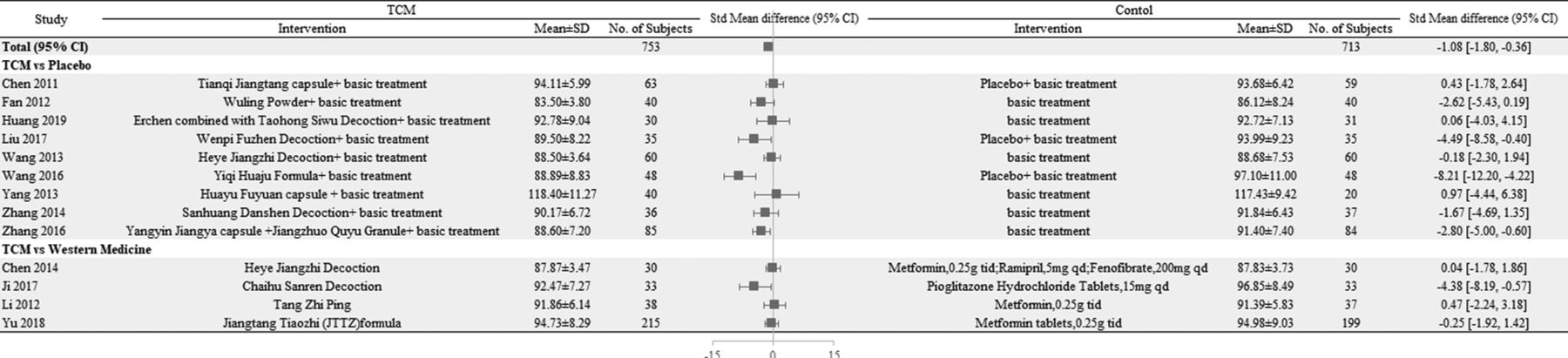
Analysis of blood pressure indicators revealed that TCM decreased SBP (n=1110, RR −4.54, 95% CI −6.90 to 2.19; figure 5) and reduced DBP (n=1110, RR −3.65, 95% CI −5.46 to 1.84; Online supplementary figure 9). Zhang et al. (2016)30 treated patients with MetS with hypertension with two Chinese patent drugs, namely Yangyin Jiangya capsule and Jiangzhuo Quyu Granule, and their results showed significant decreases in SBP and DBP in the treatment group (p<0.05). Another study24 investigating the Chinese patent drug Huayu Fuyuan capsule revealed its remarkable effect in regulating SBP (p<0.05). Moreover, Yi Tang Kang20 led to notable improvement of blood pressure and decreased SBP and DBP (p<0.01).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Data summary of the high-quality RCTs of TCM interventions for SBP. RCT, randomized controlled trial; SBP, systolic blood pressure; TCM, traditional Chinese medicine.
TCM versus Western medicine
Five RCTs comparing the efficacy of TCM with that of Western medicine on MetS were analyzed. The sample sizes ranged from 60 to 414 patients and the treatment duration was 12 weeks. The methodological quality of the studies was assessed by Jadad scores of 4–6. In this comparison, two RCTs18 27 used Chinese patent drugs as TCM intervention, whereas the others [19,21,28] used empirical decoction. Three RCTs19 27 28 used single oral hypoglycemic agents as the control group, one18 used antihypertensive drugs, and one RCT21 used a combination of oral hypoglycemic agents, oral antihypertensive drugs, and dyslipidemia drugs.
Analysis of obesity-related indicators showed no difference in efficacy between TCM and Western medicine in reducing BMI (n=715, RR −1.19, 95% CI −2.50 to 0.12; figure 1) and no significant difference between their efficacy in reducing WC (n=615, RR −0.36, 95% CI −1.44 to 0.71; figure 2). A total of 70 patients with MetS21 were assigned to the treatment group (Heye Jiangzhi Decoction) and the control group (Western medicine). After the 12-week treatment, the TCM group showed improvement of BMI compared with that in the metformin-treated group (p<0.05). A multicenter RCT18 evaluating the effect of Yiqi Huazhuo Gushen granules showed significant (p<0.05) differences in BMI and WHtR between the Yiqi Huazhuo Gushen-treated and valsartan-treated groups. Ji28 reported that Chaihu Sanren decoction ameliorated central obesity by reducing BMI (p<0.01) and WC (p<0.05), showing higher efficacy than that of pioglitazone hydrochloride tablets.
Analysis of blood glucose indicators revealed no remarkable difference in HbA1c between TCM and Western medicine, as shown in figure 3 (n=589, RR −0.07, 95% CI −0.31 to 0.18). There were no differences in hypoglycemic effect on FPG (n=715, RR −0.01, 95% CI −0.40 to 0.39; Online supplementary figure 2) and 2hPG (n=649, RR −0.10, 95% CI −0.32 to 0.13; online supplementary figure 3) between TCM and Western medicine. Moreover, there were no differences in effect on FINS (n=201, RR −0.03, 95% CI −0.46 to 0.40; Online supplementary figure 4) and HOMA-IR (n=715, RR −0.06, 95% CI −0.33 to 0.20; Online supplementary figure 5) between TCM and Western medicine. A multicenter, randomized, positive-controlled, open-label clinical trial19 indicated that the Chinese herbal formula JTTZ effectively improved blood glucose metabolism, reducing HbA1c by 0.75±1.32 (95% CI 0.58 to 0.93), FPG by 1.4±2.4 (p<0.001), 2hPG by 2.42±4.53 (p<0.001) and HOMA-IR by 0.19±0.91 (p<0.01). In another study, 80 patients with MetS27 were randomly assigned to the Tang Zhi Ping group or the metformin group, and the results showed that the Chinese patent drug exerted the same hypoglycemic effect as that of metformin. Furthermore, Ji28 reported that the Chaihu Sanren decoction had the same hypoglycemic efficacy in improving insulin resistance as that of pioglitazone hydrochloride (p>0.05).
Analysis of blood lipid indicators showed that TCM was more effective than Western medicine in reducing TC (n=715, RR −0.35, 95% CI −0.66 to 0.04; Online supplementary figure 6). The TG-lowering effect of TCM was not different from that of Western medicine (n=715, RR −0.53, 95% CI −0.64 to 0.42; figure 4). The outcome also showed that TCM was more effective in decreasing LDL (n=715, RR −0.13, 95% CI −0.21 to 0.04; Online supplementary figure 7) and in increasing HDL (n=301, RR 0.08, 95% CI 0.03 to 0.13; Online supplementary figure 8). A study showed that the Heye Jiangzhi decoction21 regulated lipid metabolism by affecting TC, TG, and LDL, but the effect showed minor difference from that of fenofibrate (p>0.05). In addition, a better response on HDL was reported (p<0.05). Both Yu et al19 and Li et al27 used metformin as treatment for the control group; however, Li et al showed higher efficacy in reducing TC, TG and LDL (p<0.05), whereas Yu et al reported efficacy similar to that of metformin (p>0.05).
Analysis of blood pressure indicators showed no significant difference between the efficacies of TCM and Western medicine in decreasing SBP (n=301, RR −3.81, 95% CI −10.90 to 3.29; figure 5) and DBP (n=301, RR 0.14, 95% CI −3.21 to 3.50; Online supplementary figure 9). Wang et al18 treated patients with MetS complicated with microalbuminuria (MAU) with Yiqi Huazhuo Gushen granules; the results showed that compared with valsartan, TCM exerted higher efficacy on SBP (p<0.05) but similar efficacy on DBP (p>0.05).
Publication bias
A funnel plot was used to investigate potential publication bias. As shown in online supplementary figures 11–16, the symmetrical dispersion points suggested no publication bias in the comparison of TCM with the control group.
Discussion
The findings described previously showed that TCM exerted efficacy on MetS, according to each studied parameter. Analysis of obesity indicators showed that TCM decreased body weight and WC, with efficacy similar to that of Western medicine. Blood glucose analysis showed that TCM, compared with placebo, exerted a DM-curative effect by lowering HbA1c, FPG, and 2hPG levels, as well as improving islet function and easing insulin resistance. TCM also improved lipid metabolism by reducing TC, TG, and LDL, as well as elevating HDL, with efficacy similar to that of Western medicine. Compared with placebo, TCM also exerted a blood pressure-controlling effect, although this effect was not significantly different from that of Western medicine.
In detail, TCM showed efficacy in decreasing body weight, although its efficacy in decreasing WC or central obesity was not significant. TCM showed significant efficacy in improving glucose metabolism compared with placebo, but this effect was not remarkable compared with that of Western medicine. Moreover, TCM exerted marked efficacy in improving lipid metabolism; it decreases TC, TG, and LDL levels and increases HDL level. However, the efficacy of TCM in controlling blood pressure was not notable. In summary, TCM might be more beneficial for decreasing body weight, as well as regulating lipid and glucose metabolisms for the treatment of MetS.
The first definition of MetS was proposed by the WHO in 1998, in which insulin resistance is regarded as the core factor. The WHO diagnosis criteria of MetS were formulated on the basis of IGR, DM, or insulin resistance combined with two additional factors, including increased arterial pressure, central obesity, increased plasma TG or decreased HDL, and MAU.41 In 1999, the European Group for Study of Insulin Resistance thought the definition should include the presence of insulin resistance or fasting hyperinsulinemia, as well as two of the following conditions: hypertension, dyslipidemia, and central obesity.42 Subsequently, the American National Cholesterol Education Programme Adult Treatment Panel III (ATP III) programme was launched in 2001, establishing criteria that included the presence of three of the following five factors: abdominal obesity, elevated TG, reduced HDL, hypertension, and elevated fasting glucose.43 Subsequently, the American Association of Clinical Endocrinologists recommended four components of the ATP III standard except WC and emphasized the importance of clinical symptoms.44 The International Diabetes Federation considered central obesity as the primary risk factor, combined with any two of the following conditions: elevated TG, reduced HDL, elevated blood pressure, elevated FPG, and previous diagnosis of T2DM.45 Considering the differences between these definitions, the transition from insulin resistance to abdominal obesity might provide insights into the mechanism of MetS.
The Chinese Diabetes Society recommended three or all of the following factors as diagnosis criteria: overweightness or obesity, elevated blood glucose (including FPG or 2hPG), hypertension, and dyslipidemia (including elevated TG, reduced HDL).41 In 2007, a joint committee of Chinese experts in endocrinology, cardiology, diabetes, and docimasiology released a guideline that proposed the criteria as three or more of the following characteristics: central obesity, elevated TG, reduced HDL, hypertension, elevated blood glucose, and history of diabetes.46 Though there are differences among these definitions, the definitions are much more suitable for clinical use and for each region.
In our enrolled studies, patients were diagnosed with MetS according to different definitions. Yu et al19 observed the clinical efficacy of TCM on T2DM in terms of obesity and hyperlipidemia, according to the standard of Chinese Diabetes Society.47 The participants of three trials20 31 32 were diagnosed with MetS with IGR; in one trial,30 patients were diagnosed with MetS with hypertension; in another trial, patients were diagnosed with MetS with MAU. Wang et al18 observed the effect of TCM on MetS complicated with MAU. They used a combination of Yiqi Huazhuo Gushen granules and valsartan for 12 weeks and found that the combination showed improved efficacy against MAU (p<0.05). Though MAU was not a primary indicator, TCM was shown to decrease urinary microalbumin and delay the progression of MetS. The study also emphasized that attention should be paid to TCM as a secondary and tertiary preventive agent against MetS, as MetS can have various complications.
The RE and FE models were used for sensitivity analysis of the stability of the included studies. As the accurate numbers of each component in every study and the agents used for basic treatment were not provided in detail, we could not measure the effect of these factors on heterogeneity. In addition, different diagnostic criteria and complications might also cause heterogeneity. Moreover, the agents used as control might cause heterogeneity, as Wang et al18 used valsartan; Li et al27 used metformin; and Chen21 used metformin, ramipril, and fenofibrate. Furthermore, Wang et al included patients with MetS with MAU, which might lead to heterogeneity. The patients in some studies20 21 23 25–28 32 were also selected according to TCM syndrome differentiation and different syndrome patterns. The use of empirical decoction or Chinese patent drugs according to the syndrome differentiation might also cause heterogeneity.
The incidence of adverse events (AEs) was evaluated to assess the safety of TCM. Twelve studies reported AEs and four18 30–32 did not mention any AE. The incidence of AEs in the TCM and control groups was not significantly different (RR 0.66, 95% CI 0.40 to 1.08; Online supplementary figure 10), suggesting that TCM was generally safe. Details on the AEs are shown in Online supplementary table 2. The main AE observed in treatment group was diarrhea, which might be caused by Rheum. Only one patient26 dropped out of the study owing to diarrhea. Because this symptom did not last long and relative examinations showed kidney or liver injury, TCM as a treatment of MetS was considered safe to a certain degree.
A prominent limitation of the present study was the lack of high-quality RCTs. Though we included studies with high Jadad scores, there were four RCTs with a Jadad score of 618 20 31 33 and only one RCT had a Jadad score of 7.32 The quality of the included studies would directly and seriously affect the accuracy of a meta-analysis. Besides, the duration of these RCTs was not long enough to provide a strong evidence, and we could not access the long-term efficacy of TCM on MetS-induced complications; future studies should focus on secondary and tertiary preventions. The efficacy of TCM on MetS might be due to weight loss or improvement of insulin sensitivity from the data mentioned previously. However, there is no definite pathological mechanism yet as MetS is the multifactorial disease. We have no idea which factor would accelerate the disease progression faster and the key pathway of treatment. The long-term observation of MetS and each single-factor study might offer references on exploring the mechanism. Regarding the participants, only one RCT19 included more than 200 patients in each group; thus, the efficacy and the ratio of AEs might be affected by the number of participants. Furthermore, though two RCTs18 19 were in English, all the participants were Chinese. Thus, the lack of other ethnic groups in the included studies might restrict the scope of their application. Data on cardiovascular events, degree of fatty liver, measurement of MAU, and detailed AEs may provide more persuasive evidence in future meta-analyses.
References
Footnotes
Contributors HW and JT drafted the manuscript. FL and XT revised the manuscript. DD, JL, XWa and XWe searched the literature and extracted data. DJ and XA made statistical analysis of data. All of the authors participated in the design and approved the final manuscript.
Funding This work was partially supported by the Young Elite Scientists Sponsorship Program by CAST (YESS20170034, 2018QNRC2-C10), the National Natural Science Foundation of China (numbers 81904187, 81274000 and 81803923), Special Scientific Research for Traditional Chinese Medicine of China (201507001-11) and the Outstanding Young Scientific and Technological Talents Program (ZZ13-YQ-026).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.