Article Text

Abstract
Introduction To assess vascular function and characterize insulin secretion using a physiological approach in Japanese women with family history of type 2 diabetes (FHD).
Research design and methods Standardized mixed-meal tests were performed with multiple postprandial glucose, insulin and free fatty acids (FFA) measurements over a 30–120 min period in 31 Japanese women aged 21–24 years. Arterial distensibility was assessed as well.
Results Fasting glucose, triglyceride and insulin averaged <90 mg/dL, <60 mg/dL and <5 μU/mL, respectively, and did not differ cross-sectionally between 10 with (FHD+) and 21 without FHD (FHD–). FHD+ showed higher insulin responses not only during the first 30 min (p=0.005) but also during the second hour (60–120 min, p<0,05) in spite of identical postprandial suppression of FFA and identical fasting and postprandial glucose and FFA concentrations, except for higher 60 min FFA in FHD+. Further, FHD+ had decreased arterial distensibility (p=0.003). On multivariate regression analysis, arterial distensibility emerged as the only significant independent predictor of FHD+. Endurance training in FHD+ did not alter decreased arterial distensibility whereas it abolished postprandial hyperinsulinemia.
Conclusions FHD was associated with decreased arterial distensibility and postprandial hyperinsulinemia despite nearly identical postprandial glycemia and postprandial FFA suppression, suggesting that impaired vascular insulin sensitivity may precede glucose and lipid dysmetabolism in normal weight Japanese women aged 22 years.
- family diabetes
- vascular function
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Positive family history of type 2 diabetes (FHD) in Asians has been reported to be related to impaired insulin secretion to glucose and less muscle insulin resistance.
What are the new findings?
Normoglycemic, normolipidemic Japanese women with positive FHD had postprandial hyperinsulinemia and decreased arterial distensibility, suggesting that impaired vascular insulin sensitivity may precede glucose and lipid dysmetabolism.
How might these results change the focus of research or clinical practice?
The results may suggest clinical significance of standardized meal tests, a physiological approach, and highlight the importance of vascular insulin sensitivity/resistance in the context of FHD, which has been less studied.
Introduction
Both family history of type 2 diabetes (FHD) and obesity are two major independent risk factors for diabetes. Insulin resistance and β-cell failure are hallmarks of type 2 diabetes. Zhu et al1 have recently demonstrated that among 4.9 million adults in the USA from 2012 to 2013, age-standardized prevalence estimates of both diabetes and pre-diabetes were higher among racial/ethnic minority groups including Asians than among whites, especially at lower body mass index (BMI) values. Normal weight (BMI <25 kg/m2) type 2 diabetes is highly prevalent in Asia and Africa.2 We have previously demonstrated that more than half of Japanese patients with type 2 diabetes are considered normal weight3 4 and that more than half of normal weight diabetics had FHD.4 These observations suggest that poor insulin secretion rather than obesity-driven insulin resistance may be at play in the natural history of diabetes in these populations. Indeed, decreased first-phase insulin secretion to glucose has been reported in young normal weight Japanese offspring of type 2 diabetics.5 6 Further, impaired β-cell function may be present earlier than visceral adiposity in some Japanese Americans who subsequently develop type 2 diabetes although both insulin resistance and impaired β-cell function contribute to the development of type 2 diabetes.7 Use of the intravenous glucose tolerance test or hyperglycemic clamp may provide a more accurate assessment of insulin secretion compared with oral glucose tolerance test-derived measures.8 9 However, exclusion of the gastrointestinal tract limits the physiologic understanding of in vivo β-cell function. Although an oral glucose tolerance test is a standardized tool to evaluate glucose tolerance, meal tests provide us information on daily-life conditions. However, studies on meal testing in people with FHD are limited in general, in Asians in particular, as discussed later.
FHD also was proposed as a significant cardiovascular risk factor.10 Previous studies have found an association between FHD and cardiovascular disease as measured by arterial stiffness.11–13 Again, studies on arterial properties in people with FHD are limited in Asian populations. Therefore, we investigated glucose and lipid responses to a standardized breakfast and arterial distensibility in young Japanese women with FHD. Because our young women comprised collegiate female athletes and untrained women,14–17 we investigated whether chronic exercise training may affect results in women with FHD.
Patients and methods
Among 35 previously reported women (17 collegiate athletes and 18 untrained students),14–16 31 women aged 21–24 years (16 collegiate athletes and 15 untrained students) provided data on family history of diabetes, which was considered positive if they reported that a parent or a grandparent was on anti-diabetic drugs. Unfortunately, information was not available on the extent of family history (ie, how many family members have the condition) and the nature of the family history (paternal or maternal). Ten women with FHD (FHD+) and 21 without FHD (FHD–) were compared cross-sectionally. The athletes were students of the Department of Health and Sports Sciences and had been training regularly for 2 years or longer prior to the study, 5 hours a day, 6 days a week. Non-athletes were students of the Department of Food Sciences and Nutrition and were not engaged in any regular sport activity. Subjects who reported that they were in treatment for acute or chronic inflammatory diseases, endocrine, cardiovascular, hepatic, renal diseases, hormonal contraception, unusual dietary habits were excluded. Nobody reported receiving any medications or having regular supplements. All subjects gave written consent after the experimental procedure had been explained.
At 8:30 after a 12-hours overnight fast, participants completed a standardized meal as previously reported.15 16 This meal was considered as a breakfast meal (total energy 450 kcal) and provided 33.3% of calories from fat (16.7 g), 51.4% from carbohydrates (57.8 g), and 15.3% from protein (17.2 g). Participants were asked to consume the entire meal within 15 min. Venous blood was drawn at baseline (0 min), 30, 60, and 120 min after the start of the meal for the measurement of plasma glucose (PG), serum insulin, triglyceride (TG) and free fatty acids (FFA) concentrations. PG was determined by the hexokinase/glucose-6-phosphate dehydrogenase method (inter-assay coefficient of variation (CV) <2%). Serum insulin was measured by an ELISA method with a narrow specificity excluding des-31, des-32, and intact proinsulin (inter-assay CV <6%). FFA was measured using enzymatic colorimetric method (Wako Chemicals, Tokyo, Japan). In fasted blood samples, the following were measured as previously reported17 ; serum cholesterol, TG, high-density lipoprotein (HDL) cholesterol, adiponectin, leptin and high-sensitivity C-reactive protein (hsCRP).
Early phase insulin responses were calculated as the increment in serum insulin during the first 30 min of the meal test (Δinsulin30). The area under the concentration curve (AUC) of PG, serum insulin, TG and FFA was calculated with the trapezoidal method (glucose- AUC, insulin-AUC, TG-AUC, FFA-AUC, respectively). FFA suppression during the meal test was assessed by percentage changes in FFA (%FFA) calculated as FFA concentrations at 30, 60, and 120 min divided by the fasting FFA concentration in each participant. Adipose tissue insulin resistance (AT-IR) was calculated as a product of fasting insulin and FFA concentrations.18 Homeostasis model assessment-insulin resistance (HOMA-IR) was calculated as previously reported.19
Lean mass, fat mass, and bone mineral mass for arms, legs, trunk and the total body were quantified by whole-body dual-energy X-ray absorptiometry (DXA) (Hologic QDR-2000, software V.7.20D, Waltham, Massachusetts, USA) as previously reported.17 The leg region included the entire hip, thigh and leg. General adiposity was assessed using BMI and fat mass index (FMI), which was calculated as body fat mass in kilograms divided by height in meter squared. Abdominal fat accumulation was assessed by waist circumference and the ratio of trunk fat to leg fat.20 Skeletal muscle mass was assessed by skeletal muscle mass index (SMI) calculated as lean mass in arms and legs in kilograms divided by height in meter squared.
Cardio-ankle vascular index (CAVI) was measured by VaSera device (VS-1000, Fukuda Denshi, Tokyo, Japan).21 CAVI is a new measure of arterial distensibility that reflects the distensibility from the ascending aorta to the ankle arteries and demonstrates little dependence on blood pressure during the evaluation. It has recently been validated to be a reliable screening tool for arterial distensibility.22 23
Data were presented as mean±SD. Due to deviation from normal distribution, HOMA-IR and hsCRP were logarithmically transformed for analyses. Differences between two groups were compared by t-test. Multivariate logistic regression analyses were done for FHD+ as a dependent variable. Independent variables included were those that displayed significant differences between FHD+ and FHD– women. A two-tailed p<0.05 was considered statistically significant. All calculations were performed with SPSS system V.15.0.
Results
As previously reported15–17 and shown in table 1, BMI averaged <22 kg/m2, waist circumference <75 cm, HOMA-IR <1.0 and fasting TG <60 mg/dL, suggesting that young women were insulin sensitive and these surrogate markers of insulin resistance did not differ between 10 FHD+ and 21 FHD– (table 1).
Anthropometric and cardiometabolic features of young Japanese women in the presence and absence of family history of diabetes
Although there was no difference in the percentage of athletes between FHD+ and FHD–, SMI tended to be lower in FHD+ (table 1). FMI, trunk/leg fat ratio, serum adiponectin, leptin and hsCRP did not differ between two groups. There was also no difference in fasting glucose, HbA1c, AT-IR, HDL cholesterol, postprandial TG and TG-AUC. Although systolic and diastolic blood pressure did not differ, CAVI score was higher in FHD+ (figure 1).

Cardio-ankle vascular index (CAVI) scores in each Japanese woman in the presence (FHD+, circles) and absence (FHD–, squares) of family history of type 2 diabetes (FHD). Open and closed symbols denote athletes and non-athletes, respectively. A circle and a square with vertical bars; mean±SD in the two groups. *p=0.003 versus FHD–.
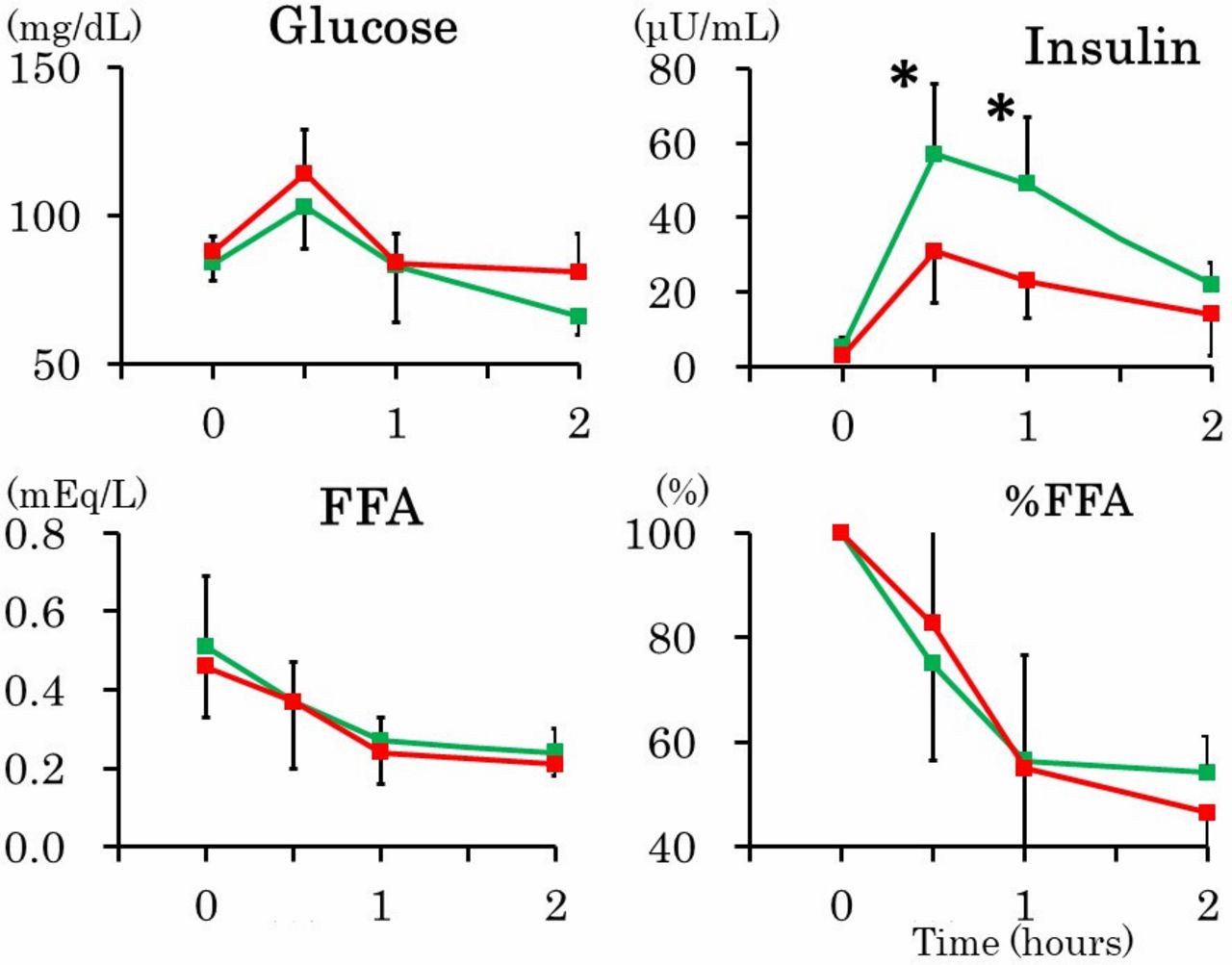
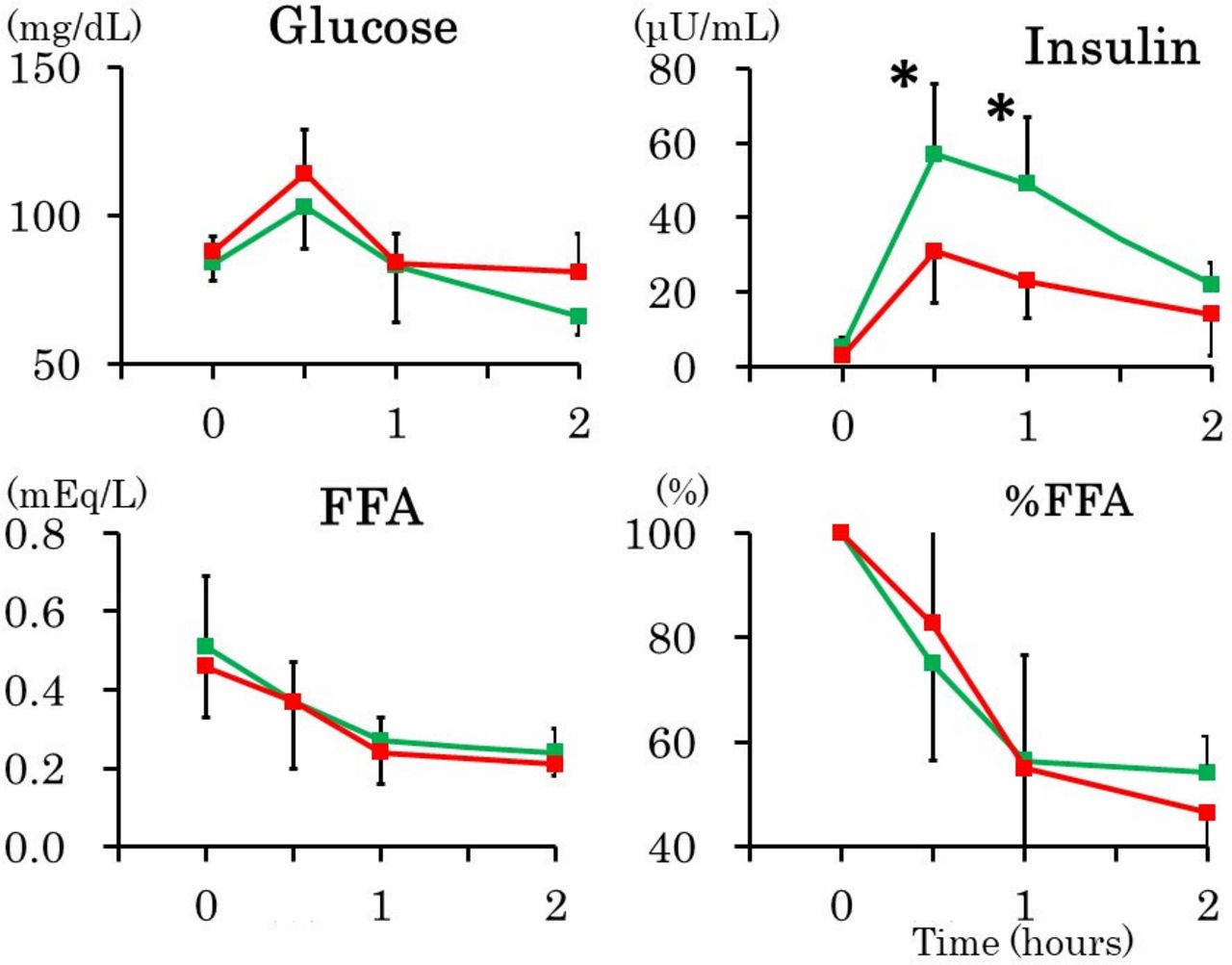
Despite nearly identical postprandial glycemia and glucose-AUC, postprandial insulinemia and insulin-AUC were greater in FHD+ (table 1 and figure 2). In addition, FHD+ had greater Δinsulin30 despite nearly identical incremental glucose concentrations during the first 30 min. Further, postprandial suppression of FFA as assessed by %FFA and FFA concentrations did not differ between FHD+ and FHD– although 60 min FFA was higher in FHD+.

Mean (±SD) plasma glucose, insulin and free fatty acids (FFA) concentration and percent changes in FFA (%FFA) in the presence (red lines) and absence (green lines) of family history of type 2 diabetes. *p<0.05; **p<0.01.
Results were essentially the same in the same analyses described above, in which four women who did not provide data on FHD were included as negative FHD (online supplementary table 1). We believe that it seems reasonable to assume that women who did not provide data on FHD might not have FHD.
Supplemental material
Multivariate logistic regression analyses were done for FHD+ as a dependent variable. Independent variables included were Δinsulin30, insulin-AUC and arterial distensibility. Arterial distensibility emerged as the only significant independent predictor of FHD+ (OR; 12.0, 95% CI; 1.6 to 91.0, p=0.016).
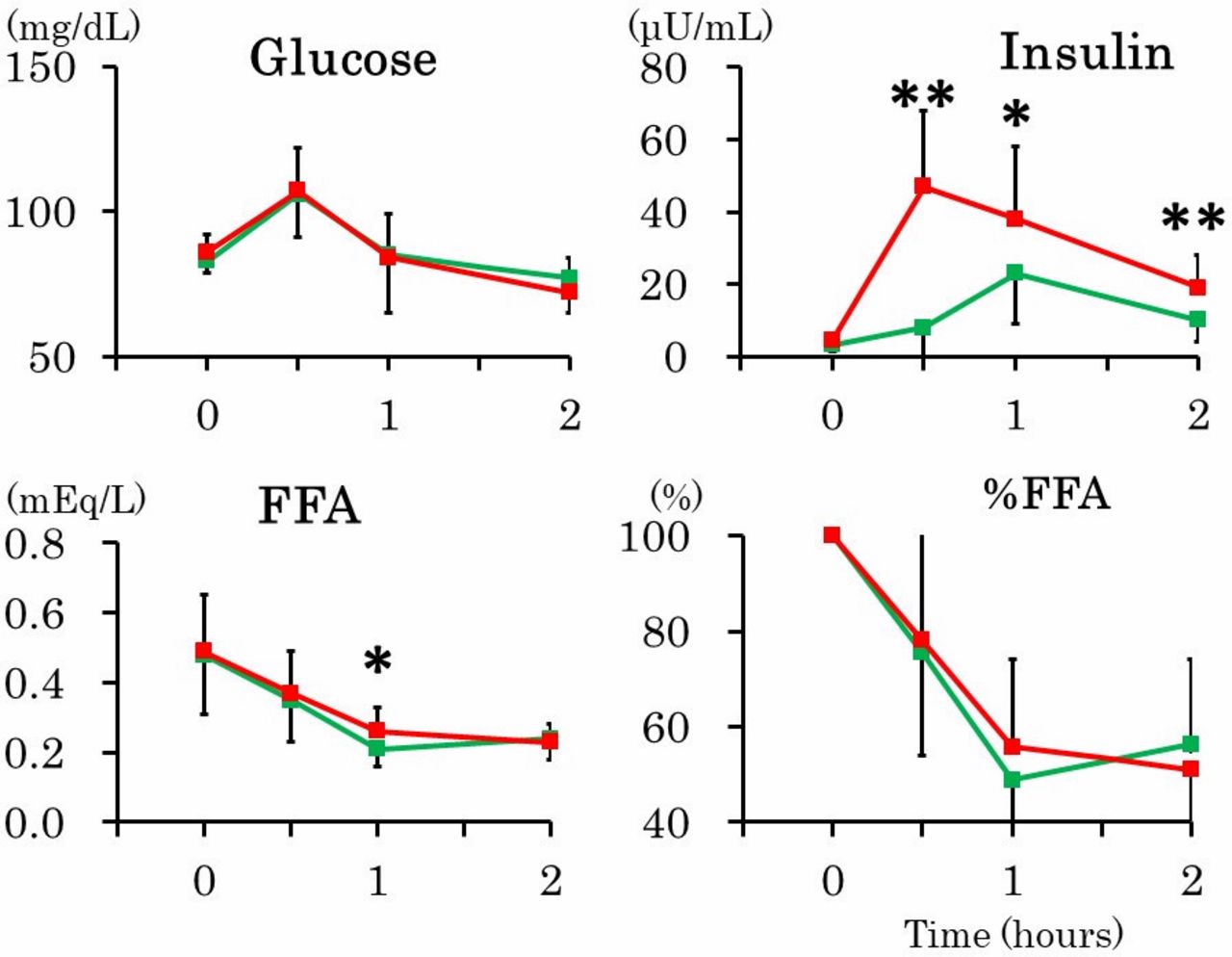
FHD+ athletes compared with FHD+ non-athletes had higher SMI and lower resting pulse rate, the latter of which averaged 48±6 bpm (table 2). As shown in figure 3, postprandial insulinemia was increased in FHD+ non-athletes whereas postprandial insulinemia in FHD+ athletes was lower compared with FHD+ non-athletes but was comparable to FHD– women. Postprandial glycemia and postprandial suppression of FFA did not differ between FH+ athletes and FH+ non-athletes. However, the two FHD+ groups did not differ in CAVI score which was increased compared with FHD– (table 2 and figure 1).
Comparisons between female collegiate athletes and untrained students (non-athletes) with family history of diabetes
{kind=link}
{kind=link}
{kind=link}
Mean (±SD) plasma glucose, insulin and free fatty acids (FFA) concentration and percent changes in FFA (%FFA) in female athletes (red lines) and non-athletes (green lines) with family history of type 2 diabetes. *p<0.05; **p<0.01.
Discussion
In normal weight Japanese women aged 23 years who were not insulin resistant rather insulin sensitive, meal-induced insulin responses were increased rather than decreased not only during the first 30 min but also during the second hour (60–120 min) in FHD+ compared with FHD– in the presence of nearly identical postprandial glycemia and FFA suppression. Moreover, CAVI score was higher in FHD+, suggesting decreased arterial distensibility. On multivariate regression analysis, arterial distensibility emerged as the only significant independent predictor of FHD+. Furthermore, endurance training in FHD+ abolished increased postprandial insulin responses whereas it did not alter decreased arterial distensibility.
Type 2 diabetes in East Asians is well known to be characterized primarily by β-cell dysfunction rather than obesity-driven insulin resistance.24 Japanese offspring of type 2 diabetics whose age and BMI were comparable to those of our young women showed decreased first-phase insulin secretion to intravenous glucose.5 6 Further, impaired β-cell function may be present earlier than visceral adiposity in some Japanese Americans who subsequently develop type 2 diabetes.7 In contrast, in the present study, young normal weight Japanese FHD+ women showed increased early-phase insulin responses after meal ingestion despite nearly identical incremental glucose concentrations, suggesting increased incretin effect. Nyholm et al25 examined profiles of insulin in glucose tolerant but insulin resistant relatives of type 2 diabetics during a 24-hours period including three meals. They found that incremental insulin secretion after each meal appeared normal in relatives. We have no explanation for higher meal-induced early phase insulin secretion in Japanese FHD+ women in the present study.
Insulin is a vascular hormone and regulates vascular tone and reactivity.26 27 In the postprandial state, increased circulating insulin can enhance blood flow to the microvasculature in muscle thus increasing the access of glucose and insulin to the myocytes. And then, insulin binds to receptors on the skeletal muscle cell surface to enhance glucose uptake. In healthy humans, physiological doses of insulin and mixed meals each increased microvascular perfusion volume.28 29 Therefore, it seems reasonable to assume that postprandial hyperinsulinemia in the presence of nearly identical postprandial glycemia may be related to the impaired vasodilatory action of insulin to deliver insulin to skeletal muscle. In the same way, postprandial hyperinsulinemia in the presence of nearly identical postprandial FFA suppression may be related to the impaired vasodilatory action of insulin in adipose tissue. Fasting glucose averaged <90 mg/dL and TG <60 mg/dL in our FHD+ women. These observations suggest that impaired microvascular insulin sensitivity may precede glucose and lipid dysmetabolism in young FHD+ Japanese women. Experimental studies in diet-induced obesity have shown that vascular insulin resistance (impaired insulin-induced phosphorylation of endothelial nitric oxide synthase) and endothelial dysfunction (reduced nitric oxide production) preceded the onset of insulin resistance in muscle, liver, and fat, suggesting a heightened susceptibility of the vasculature to the detrimental effects of nutrient excess relative to tissues involved in glucose homeostasis and fuel storage.30 Postprandial hyperinsulinemia was not found in FHD+ athletes, suggesting that endurance training improved impaired insulin sensitivity in FHD+ offspring as previously reported.31–33 Exercise has been reported to increase human skeletal muscle insulin sensitivity via coordinated increases in microvascular perfusion and molecular signaling.34
A standardized meal test gives a more clinically relevant metabolic status whereas the primary function of glucose tolerance tests is to amplify any glucose intolerance, thus aiding diagnosis.35 However, studies using a mixed meal to represent normal physiological feeding in people with FHD+ were limited.25 36 37 In agreement with our observations, postprandial hyperinsulinemia in the presence of comparable/slightly raised glycemia and comparable FFA have been found in non-obese relatives in mid-to-late thirties.25 36 However, Allerton et al37 have shown that responses to a mixed meal, which was similar to that used in the present study, of glucose, insulin and FFA assessed by respective AUC did not differ between normal-weight offspring of mothers with type 2 diabetes aged 21 years and controls.
CAVI is a new measure of arterial distensibility that reflects both the elastic (the ascending aorta) and muscular (the leg artery) artery stiffness and has recently been validated to be a reliable screening tool for arterial distensibility.22 23 CAVI score was higher in FHD+ compared with FHD–, suggesting decreased arterial distensibility in FHD+ as previously reported.11–13 It is noted that an independent association between decreased arterial distensibility and FHD+ was observed in young normal weight Japanese FHD+ women. Furthermore, endurance training did not improve decreased arterial distensibility in our FHD+ women whereas it improved impaired microvascular insulin sensitivity as described above. Arterial distensibility was not associated with insulin sensitivity in FHD+ subjects whose age and BMI were comparable to those of our participants12 but was associated in FHD+ subjects who tended to be obese and older.10 13
This study has several strengths, including a homogeneous study population with scarce confounding factors, and accurate and reliable measures of body composition by DXA. The main limitation of our study is small sample size. The cross-sectional design of the present study complicates the drawing of causal inferences, and a single measurement of biochemical variables may be susceptible to short-term variation, which would bias the results toward the null. We used several surrogate markers in the present study, which may be less accurate. As we studied young Japanese women only, results may not be generalized to other gender, age populations, races or ethnicities. Studies with more patients are needed.
Conclusions
Young insulin sensitive Japanese women with FHD may have decreased arterial distensibility and impaired microvascular insulin sensitivity in skeletal muscle and adipose tissue, suggesting that impaired vascular insulin sensitivity may precede glucose and lipid dysmetabolism. Although female athletes with FHD did not show the metabolic changes, they had decreased arterial distensibility. These observations may suggest a genetic effect on early arterial physiology that may be relevant to later clinical disease.
Acknowledgments
We are indebted to all the participants for their dedicated and conscientious collaboration.
References
Footnotes
Contributors MT, BW, MH, AT, KK, SM and MK have made substantial contributions to acquisition, analysis and interpretation of data. KF has been involved in drafting the manuscript. TK has been involved in revising it critically for important intellectual content; has given final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committees of the University (No. 07-28) to be in accordance with the Helsinki declaration.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The Ethics Committee of Mukogawa Women’s University does not allow us to open data except for a manuscript.