Article Text

Abstract
Introduction To estimate the prevalence of and trends in diabetes according to sociodemographic indicators and cardiovascular risk factors in a Swiss population.
Research design and methods Annual cross-sectional study of adults residing in the state of Geneva. We included 9886 participants (51% women; mean age (SD) of 48.9 (13.4) years). Diagnosed diabetes was self-reported; undiagnosed diabetes was defined as having fasting plasma glucose level of ≥7 mmol/L and no previous diagnosis; total diabetes as the sum of diagnosed and undiagnosed diabetes. To assess trends, we grouped survey years into three time periods: 2005–2010, 2011–2014, and 2015–2017. To assess inequalities, we constructed the relative index of inequality (RII) and the slope index of inequality (SII) for education, income, and health insurance subsidy (state program based on socioeconomic disadvantage).
Results In total, 683 diabetes cases were identified. In 2015–2017, total diabetes prevalence was 11.8% (8.6%–14.9%) among lowest income participants, and 4.7% (3.4%–5.9%) among highest income participants (p<0.01). Similar findings were observed for education. Among participants with full health insurance subsidy, diabetes prevalence was 19.4% (12.1%–26.8%), and 6.1% (5.3%–7.0%) among those without (p<0.01). High diabetes prevalence was observed among participants who were men, older, overweight or obese, hypertensive, and hypercholesterolemic. Among participants with diabetes, 74.0% (63.5%–84.4%) in the lowest income group were diagnosed, compared with 90.2% (81.9%–98.4%) in the highest income group (p=0.04). Over the 13-year period, widening relative and absolute inequalities in total diabetes prevalence were observed for education and income. The education-RII (95% CI) increased from 1.51 (95% CI 1.01 to 2.32) in 2005–2010 to 2.54 (95% CI 1.58 to 4.07) in 2015–2017 (p=0.01), and the education-SII (95% CI) from 0.04 (95% CI 0.01 to 0.08) to 0.08 (95% CI 0.04 to 0.10; p<0.01). The income-RII increased from 2.35 (95% CI 1.44 to 3.84) to 3.91 (95% CI 2.24 to 6.85; p<0.01), and the income-SII from 0.08 (95% CI 0.04 to 0.12) to 0.011 (95% CI 0.07 to 0.14; p=0.01). Inequalities by health insurance subsidy were large (RII 3.56 (95% CI 1.90 to 6.66) and SII 0.10 (95% CI 0.05 to 0.15)) but stable across the study period.
Conclusion Among adults living in Geneva, Switzerland, substantial differences were observed in diabetes prevalence across socioeconomic and cardiovascular risk groups over a 13-year period, and relative and absolute socioeconomic inequalities appeared to have increased.
- adult diabetes
- social inequalities
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Diabetes prevalence continues to increase worldwide, and this increase disproportionally affects socioeconomically disadvantaged populations.
No previous study has reported on trends in socioeconomic inequalities in diabetes prevalence in Switzerland.
What are the new findings?
Clear socioeconomic inequalities in diabetes prevalence are present in the adult population of the state of Geneva, Switzerland.
Socioeconomically disadvantaged adults with diabetes are less likely to know they have diabetes compared with more advantaged adults with diabetes.
Relative and absolute inequalities in diabetes prevalence appear to have widened over a 13-year period.
How might these results change the focus of research or clinical practice?
The medical community needs to improve their approach to screening for and diagnosing diabetes in socioeconomically disadvantaged groups who are disproportionally more likely to have diabetes but less likely to be aware that they have it.
Introduction
Diabetes represents a major public health crisis—it is a major contributor to chronic disease morbidity and mortality,1 and its prevalence continues to increase worldwide.2 The NCD Risk Factor Collaboration consortium reported that Switzerland was one of the few countries worldwide whose populations experienced no increase in diabetes prevalence between 1980 and 2014.2 However, this report excluded any disaggregation of findings by socioeconomic indicators, while extensive research has consistently shown that the prevalence of diabetes differs widely across different socioeconomic groups, whereby socioeconomically disadvantaged individuals tend to be disproportionally more likely to suffer from diabetes, compared with their more privileged counterparts.3–5 Surprisingly, to date, reliable and accurate data on diabetes prevalence, in the overall population as well as within different sociodemographic groups, remain scarce in Switzerland.6 A nationwide study reported that individuals with primary/lower secondary education had a higher prevalence of diabetes relative to those with higher education, but this was based on self-reported diagnosed diabetes.7 Another study from the city of Lausanne, Switzerland, found that the prevalence of diabetes, based on fasting plasma glucose, among individuals with less than secondary education was three times as high as that among individuals with tertiary education, yet this study did not report trends over time.8 As such, there remains a need to objectively assess the prevalence and trends of diabetes disaggregated by different indicators that capture different socioeconomic circumstances in the Swiss population. This is an imperative in order to ensure that public health interventions for diabetes awareness, prevention and control are tailored to reach vulnerable population groups at high risk of diabetes, and to properly address their specific needs and challenges.
Thus, we aimed to examine the prevalence and trends of diabetes according to a series of sociodemographic and cardiovascular risk factor indicators using data from a population-based study over a 13-year period (2005–2017).
Methods
We used data from the Bus Santé Study, an ongoing yearly cross-sectional population-based health examination survey in the state of Geneva, Switzerland (approximate population of 500 000 inhabitants). Detailed description of the study methodology has been published elsewhere.9 Briefly, annual surveys took place between 1992 and 2017, drawing from independent samples of the non-institutionalized residents of the state of Geneva aged 35–74 years until 2011 and aged 20–74 years thereafter. Eligible participants are identified with a standardized procedure using a residential list established annually by the state government. Random sampling in age and sex-specific strata matches the corresponding frequencies in the population. Potential participants unreachable on three mailings and seven phone calls are replaced using the aforementioned protocol, but subjects reached and unwilling to participate are not replaced. Included participants become ineligible for future surveys. The analytical sample for this paper was drawn from surveys starting in 2005, when fasting plasma glucose began being measured in the study. Participation rates ranged from 55% to 65% between 2005 and 2017. A decrease in participant recruitment was observed for the period between 2005 and 2008 due to a concomitant study taking place, sharing logistical resources but not the same target population.
Data collection
Each participant received three self-administered, standardized questionnaires covering a series of risk factors for major lifestyle-related chronic conditions, sociodemographic characteristics, educational and occupational histories, dietary intake, and physical activity. Two clinics and one mobile medical unit conducted health examinations from January to December each year.10 Body weight and height were measured using standard procedures, and body mass index (BMI) (kg/m2) was calculated. Blood pressure was measured thrice in the sitting position on the right arm after at least 10 min rest using a standard protocol and a validated automated oscillometric sphygmomanometer. Fasting plasma blood samples were collected and glucose, total plasma cholesterol, high-density lipoprotein (HDL) plasma cholesterol and triglycerides were assayed using commercially available enzymatic kits (Bayer Technicon Diagnostics, CV 1.4%, 1.2%, and 1.5% for glucose, cholesterol and triglycerides, respectively).
Socioeconomic, demographic, and cardiovascular risk factors
As proxies for socioeconomic circumstances, we used education, income, and health insurance subsidy, the latter forming part of the social assistance program in the state of Geneva. To determine qualification to receive a health insurance subsidy, state officials evaluate the applicant’s household income and family composition—it is thus a strong proxy for overall socioeconomic disadvantage. We classified self-reported education into three groups: (1) primary/lower secondary education; (2) secondary education/apprenticeship; (3) tertiary education. Monthly household income (SFr1=US$1) was categorized into four groups: (1) <5000; (2) 5000–6999; (3) 7000–9499; (4) >9500. Health insurance subsidy was categorized into three groups: (1) no subsidy; (2) partial subsidy; (3) full subsidy. Age was categorized into three groups: (1) 18–44 years; (2) 45–64 years; (3) 65 years and older. Hypertension was defined as having a previous diagnosis or blood pressure ≥140/90 mm Hg. Hypercholesterolemia was defined as having a previous diagnosis or having total blood cholesterol >6.5 mmol/L and HDL <1 mmol/L.
Diabetes prevalence
Drawing from published research,3 11 we defined the prevalence of diagnosed diabetes as having a previous diagnosis of diabetes; the prevalence of undiagnosed diabetes as having fasting plasma glucose level of ≥7 mmol/L and not having a previous diagnosis of diabetes; the prevalence of total diabetes as the sum of diagnosed and undiagnosed diabetes; and the prevalence of diabetes awareness as the ratio of diagnosed diabetes to total diabetes.
Statistical analysis
We excluded participants who had not fasted for at least 8 hours prior to blood sample collection (5% of the original sample), as well as those with incomplete self-reported diabetes-related responses (<1%) (online supplementary figure S1 shows the flowchart for the analytical sample). To assess secular trends, we grouped survey years into three groups (to maximize power) as follows: 2005–2010, 2011–2014, and 2015–2017. Numbers and frequencies are presented for categorical values, and means (SD) for continuous values. We first calculated the prevalence (%, 95% CI) of each diabetes outcome according to sociodemographic and cardiovascular risk factor indicators for the most recent survey period, 2015–2017, applying logistic regression with the estimates adjusted for age, sex, and survey year. To assess trends in socioeconomic inequalities, we constructed the relative index of inequality (RII) and the slope index of inequality (SII) for education, income, and health insurance subsidy. These measures describe the relative and absolute differences between the two extremes groups while taking into account the intermediate categories.12 For example, RII=1.10 indicates that the least educated group has an additional 10% prevalence of an outcome relative to the most educated group. Similarly, an SII=0.10 indicates that there are 10 more participants with the outcome per 100 individuals in the lowest educated group compared with the most educated group. To calculate the RII (95% CI), we used Poisson regression adjusting for age, sex, and survey year, and linear regression to calculate the SII (95% CI), adjusting for age, sex, and survey year. P values for linear trend in RII and SII were calculated from interaction terms between RII/SII and survey periods. To assess trends in diabetes prevalence according to sex, age and cardiovascular risk factors, we used multivariable logistic regression stratified by survey period, and linear trend was assessed separately in models with an interaction term between the predictor and survey period as continuous. Although fasting glucose measures were introduced in 2005, self-reported diabetes was available in surveys from 1995. We then extended the trends analysis with data from 1995 to 2017, using self-reported diabetes, and disaggregating prevalence by age group, sex, educational level, BMI group, and hypertension and hypercholesterolemia status. A two-sided p<0.05 was considered significant. All data were analyzed using STATA V.15 (College Station, TX: StataCorp).
Supplemental material
Results
Description of sample
Our analytical sample comprised 9886 participants (from an initial sample of 10 805), whose characteristics are presented in table 1. The mean age (SD) was 48.9 years (13.4) and 51% were women. Most of the participants had a secondary or tertiary level of education, a household monthly income of at least SFr7000, and received no health insurance subsidy. The proportion of overweight (32%) and obese participants (13%) was similar over the 13-year period, while that of hypertension and hypercholesterolemia appeared to decrease over time (table 1).
Description of sample, overall and by survey period, Bus Santé Study, 2005–2017
Diabetes prevalence by sociodemographic and cardiovascular risk factors in 2015–2017
The prevalence of diabetes according to sociodemographic and cardiovascular risk factors for the 2015–2017 period appears in table 2. The sex-adjusted prevalence of total diabetes was higher among those aged 65 years or older (16.8% (95% CI 13.3% to 20.2%)) compared with those aged 45–64 years (7.9% (95% CI 6.4% to 9.4%)) and those younger than 45 years (2.8% (95% CI 2.0% to 3.6%); p<0.01). The age-adjusted prevalence of total diabetes was slightly higher among men (7.8% (95% CI 6.5% to 9.1%)) than women (5.7% (95% CI 4.6% to 6.8%); p=0.02). Among men with diabetes, 73.1% (95% CI 65.0% to 81.1%) were diagnosed compared with 88.3% (95% CI 81.4% to 95.2%) among women with diabetes (p=0.01).
Diabetes prevalence per 100 adults living in the state of Geneva, Bus Santé Study, 2015–2017
The age and sex-adjusted prevalence of total diabetes differed across socioeconomic groups. Participants with a primary/lower secondary education had a higher prevalence of total diabetes (9.2% (95% CI 7.4% to 11.1%)), compared with those with a higher secondary/apprenticeship education (7.0% (95% CI 5.3% to 8.8%)) and with participants with a tertiary education (5.3% (95% CI 4.2% to 6.4%); p<0.01). Similarly, participants in the lowest income group had a higher prevalence of total diabetes (11.5% (95% CI 9.0% to 13.9%)) compared with those in the second highest income group (7.3% (95% CI 5.3% to 9.3%)) and those in the highest income group (4.7% (95% CI 3.4% to 5.9%); p<0.01). Among those in the lowest income group who had diabetes, only 74.0% (95% CI 63.5% to 84.4%) were diagnosed, while among those in the highest income group, 90.2% (95% CI 81.9% to 98.4%) were diagnosed (p=0.04). Participants who received a full health insurance subsidy also had a higher prevalence of total diabetes (19.4% (95% CI 12.1% to 26.8%)) than participants who received a partial health insurance subsidy (8.1% (95% CI 5.1% to 11.1%)) and participants who did not receive any health insurance subsidy (6.1% (95% CI 5.3% to 7.0%); p<0.01).
The sex and age-adjusted prevalence of total diabetes was higher among participants with higher BMI, those with hypertension and those with hypercholesterolemia. The same pattern of prevalence was observed for diagnosed and undiagnosed diabetes prevalence across all sociodemographic and cardiovascular risk groups (table 2).
Trends in diabetes prevalence by sociodemographic and cardiovascular risk factors
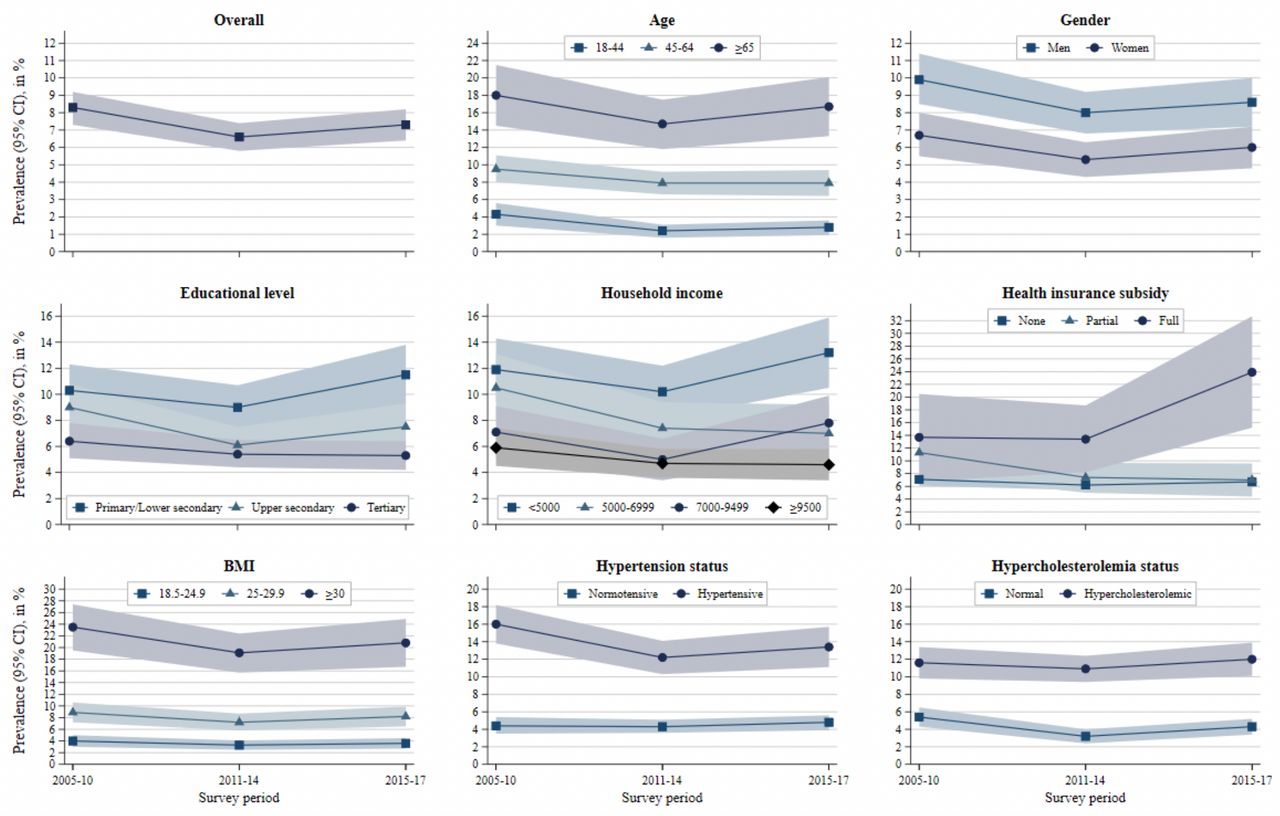
Figure 1 presents the prevalence of total diabetes according to sociodemographic and cardiovascular risk factor groups across three survey periods. The prevalence appeared to remain relatively constant across survey periods for all sociodemographic and cardiovascular risk groups. A clear exception was observed among participants who received a full health insurance subsidy, among whom the prevalence increased from 13.7% in 2005–2010 to 23.9% in 2015–2017. Similar trends were observed for diagnosed diabetes (online supplementary figure S2) and undiagnosed diabetes (online supplementary figure S3). The prevalence of diabetes awareness appeared to have decreased slightly overall and across most sociodemographic and cardiovascular risk factor subgroups, except among participants in the highest income group, among whom it appeared to have increased over time (online supplementary figure S4).
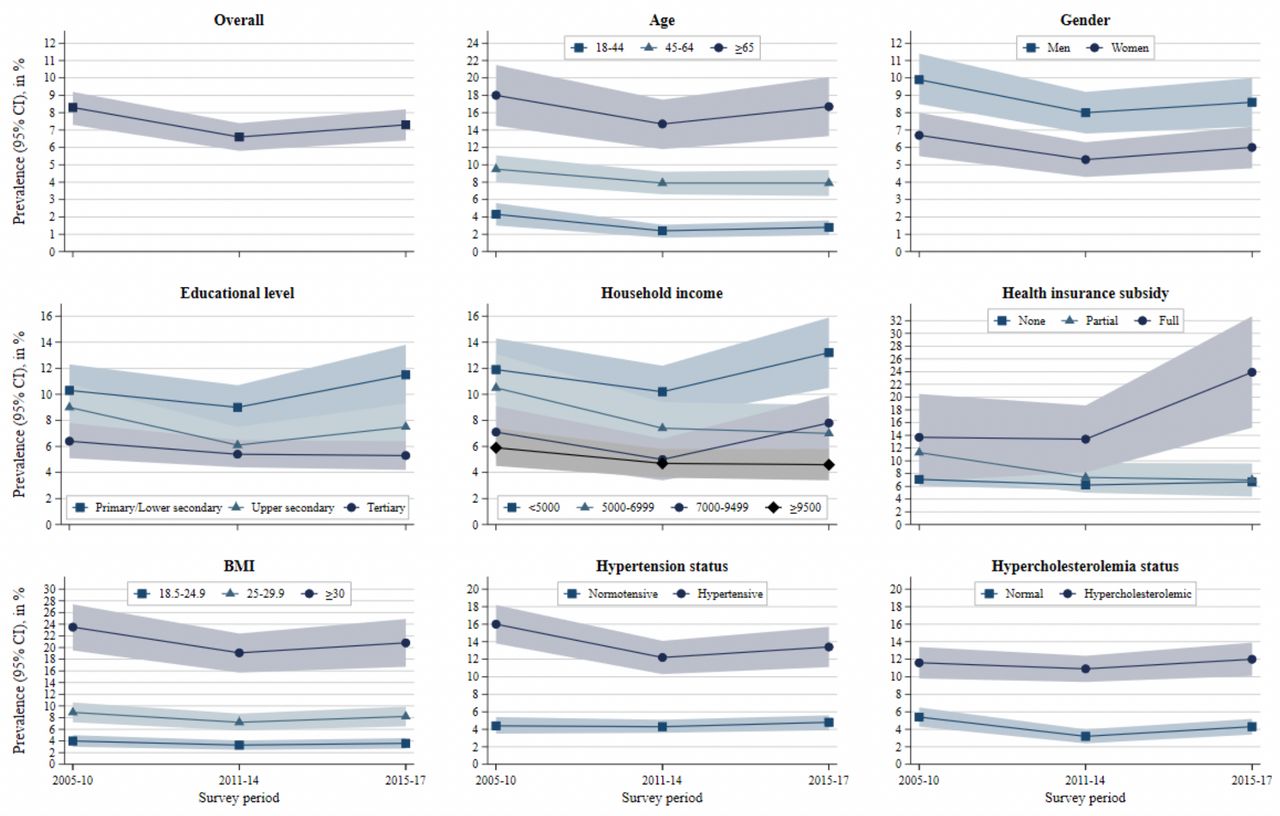
Trends in prevalence of total diabetes according to sociodemographic and cardiovascular risk factor indicators, Bus Santé Study, 2005–2017. Prevalence and 95% CIs are from logistic regression models adjusted for age, gender, and survey year. BMI, body mass index.
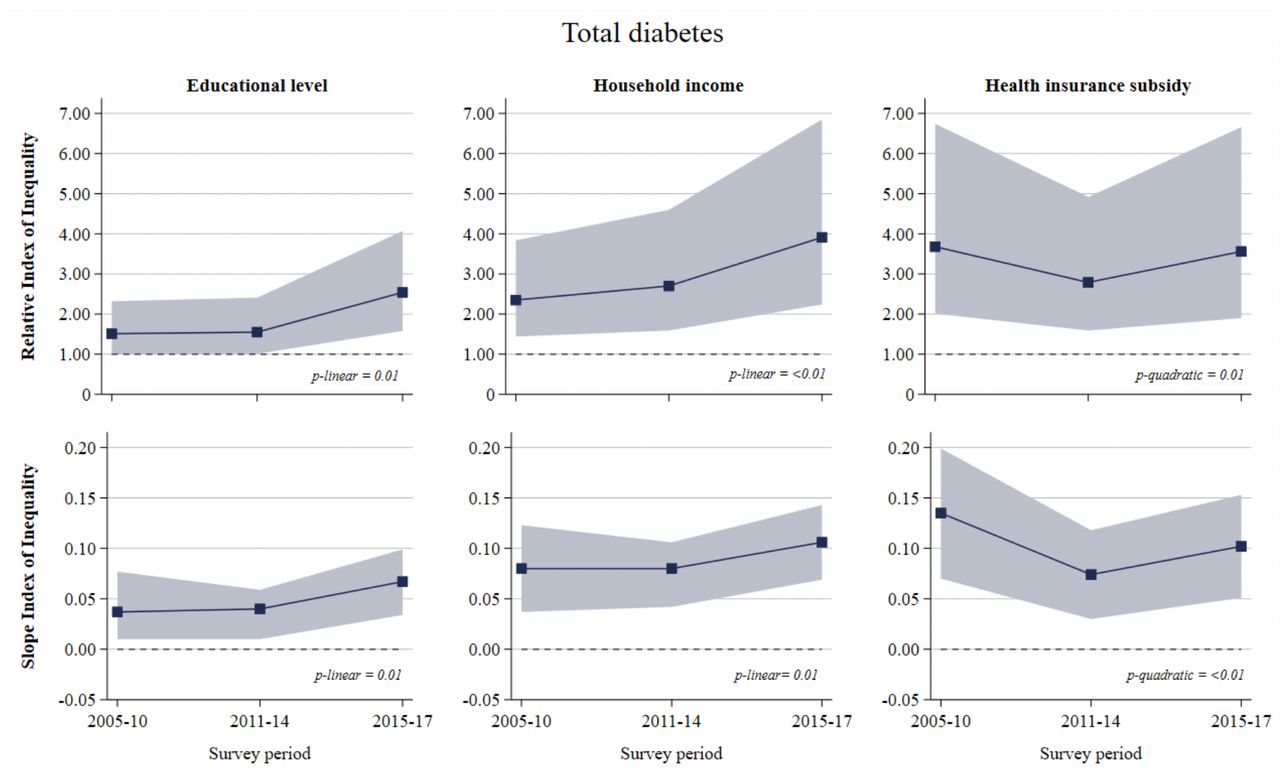
Figure 2 shows the trends in relative and absolute socioeconomic inequalities for the prevalence of total diabetes. Relative and absolute inequalities by educational level were present in each survey period and appeared to widen over time. The RII (95% CI) for education increased from 1.51 (95% CI 1.01 to 2.32) in 2005–2010 to 2.54 (95% CI 1.58 to 4.07) in 2015–2017 (p=0.01), and the SII for education increased from 0.04 (95% CI 0.01 to 0.08) to 0.08 (95% CI 0.04 to 0.10) (p=0.01). Relative inequalities in total diabetes prevalence were also present for income in each survey period, and widened over time; the RII for income increased from 2.35 (95% CI 1.44 to 3.84) to 3.91 (95% CI 2.24 to 6.85) (p<0.01), and the SII increased from 0.08 (95% CI 0.04 to 0.12) to 0.11 (95% CI 0.07 to 0.14) (p<0.01). Even greater relative inequalities were observed for health insurance subsidy in each survey period. The RII decreased from 3.68 (95% CI 2.01 to 6.74) in 2005–2010 to 2.79 (95% CI 1.59 to 4.92) in 2011–2014, but increased again to 3.56 (95% CI 1.90 to 6.66) by 2015–2017 (p quadratic <0.01). The SII decreased slightly overall from 0.14 (95% CI 0.07 to 0.20) to 0.10 (95% CI 0.05 to 0.15) (p quadratic=0.01) (figure 2).
{kind=link}
{kind=link}
Trends in socioeconomic inequalities in total diabetes prevalence, Bus Santé Study, 2005–2017. Relative index of inequality and 95% CI are from Poisson regression, adjusted for age, gender and survey year. Slope index of inequality and 95% CI are from linear regression, adjusted for age, gender, and survey year. P value for linear trend in relative index of inequality (RII) and slope index of inequality (SII) from interaction term between socioeconomic score and survey period.
Similar findings were seen in relative and absolute inequalities for diagnosed diabetes prevalence (online supplementary figure S5). For undiagnosed diabetes, while no relative or absolute inequalities were seen in 2005–2010, relative inequalities emerged by 2011–2014 for income (4.92; 95% CI 1.19 to 20.33), and by 2015–2017 for education (3.35; 95% CI 1.13 to 9.91) and health insurance subsidy (4.61; 95% CI 1.12 to 19.06) (online supplementary figure S6). For diabetes awareness, relative and absolute inequalities were observed in 2015–2017 for income only ((RII=0.72; 95% CI 0.54 to 0.96) and (SII=−0.26; 95% CI −0.50 to –0.02)) (online supplementary figure S7).
Table 3 presents the association of total diabetes prevalence with age, gender and cardiovascular risk factors over time. Relative to younger participants, those aged 45–65 years and 65 years or older were at least two times more likely to have diabetes, and there was a suggestion that this increased risk became more pronounced over time for the oldest age group (p linear=0.02). Men were more likely to have diabetes than women, though this association no longer held in 2015–2017. Participants with obesity were approximately four times more likely to have diabetes, compared with participants with BMI below 25 kg/m2, and this association remained stable over time. Hypertensive participants and those with hypercholesterolemia were more likely to have diabetes relative to non-hypertensive and non-hypercholesterolemic participants. Similar findings were observed for diagnosed diabetes prevalence (online supplementary table S1). Fewer association were seen over time for undiagnosed diabetes (online supplementary table S2); however, men were more than three times more likely to have undiagnosed diabetes than women, and this association persisted over time. Accordingly, men with diabetes were approximately 70% less likely than women to be aware of their condition (online supplementary table S3).
Trends in the association of total diabetes prevalence with demographic and cardiovascular risk factors, Bus Santé Study, 2005–2017
In extended analyses, the prevalence of self-reported diabetes between 1995 and 2017 reflected our main findings, remaining largely unchanged within each sociodemographic and cardiovascular risk factor group. The exception was among participants with primary/secondary education, whose prevalence of diabetes increased slightly over time from 5.4% (95% CI 4.6% to 6.1%) to 7.4% (95% CI 6.1% to 8.7%), while that among participants with tertiary education remained constant (online supplementary table S4). Accordingly, while no inequalities were seen before 2005–2010, relative and absolute inequalities became evident afterwards (online supplementary figure S8).
Discussion
In a large representative sample of adults living in the state of Geneva, Switzerland, the age and sex-adjusted prevalence of diabetes differed substantially across sociodemographic and cardiovascular risk factor groups in 2015–2017. Between 2005–2010 and 2015–2017, the prevalence of diabetes appeared to remain relatively stable across different groups according to sociodemographic and cardiovascular risk factor characteristics. However, relative and absolute socioeconomic inequalities in diabetes prevalence appeared to have widened over time.
The 2015–2017 prevalence of total, diagnosed and undiagnosed diabetes was higher among men, older participants, those with lower educational and income levels, participants receiving a health insurance subsidy, those with higher BMI and participants with hypertension or hypercholesterolemia. These findings reflect those from another Swiss population,8 12 which showed clear inequalities in diabetes prevalence across different educational levels as well as between men and women, age and BMI groups. These findings are also in line with findings on socioeconomic inequalities in diabetes prevalence as well as in diabetes awareness that have been consistently reported in other high-income countries,2–5 including in neighboring Germany,11 France,13 and Italy.14
Our results also showed that the association between socioeconomic circumstances and diabetes prevalence extends beyond education and income. This included inequalities between those who received and did not receive health insurance subsidy from the government of Geneva, which provides further support for the link between socioeconomic disadvantage and diabetes prevalence. Furthermore, our findings revealed that between 2005–2010 and 2015–2017, socioeconomic inequalities, in relative and absolute terms, have increased over time across different education and income groups, which are consistent with findings showing an increase in socioeconomic inequalities over time in England,15 Ireland and Northern Ireland,16 Scotland,17 and Spain,18 as well as in the USA.3
Strengths and limitations
To our knowledge, this is the first study to show trends in prevalence of diabetes according to a series of sociodemographic and cardiovascular risk factors in a Swiss population. It is also the first study to show such trends with regard to health insurance subsidy. Strengths of our study included the objectively measured fasting plasma glucose level used to identify cases of diabetes, which the NCD Risk Factor Collaboration consortium recommends for population-based studies above other methods such as using HbA1c,19 the relatively long period of time period covered, the array of different socioeconomic and demographic indicators and cardiovascular risk factors, and the use of absolute and relative measures of inequality. Limitations include the size of our sample, which likely contributed to the wide CIs and the fact that participants self-reported a diagnosis of diabetes, which may have underestimated the prevalence of diagnosed diabetes, and thus underestimated the prevalence of diabetes awareness. Finally, the question on diabetes diagnosis posed to participants did not distinguish between type 1 and type 2 diabetes, a common limitation in surveys as it is difficult to differentiate between the two types in adults20 21; however, 85%–95% of diabetes cases in adults are type 2 diabetes,2 22 so the identified cases in our sample are likely to be predominantly type 2 diabetes.
Public health implications
The fact that socioeconomic inequalities were present, persisted, and even increased over a period of 13 years (23 years when evaluating self-reported diabetes) should act as a reminder that past and current public health strategies have failed to promote and facilitate health among all socioeconomic groups in the population. The higher prevalence of diabetes among socioeconomically disadvantaged groups likely translates to higher diabetes-related healthcare expenses, which in Switzerland rank among the highest in the world,23 and to higher risk of diabetes-related complications.24 25 These in turn can adversely affect mental health, social relationships, employment, and educational opportunities, and further worsen the socioeconomic and psychosocial circumstances of diabetic individuals and those around them.26 27 To tackle this vicious cycle, two types of interventions are needed: (1) population-wide efforts to promote healthy lifestyles, such as healthy eating and physical activity; and (2) targeted interventions to address the specific needs and challenges of socioeconomically disadvantaged groups, such as affordable and safe housing, access to green spaces, access to healthy foods and community life, among others.28 Surprisingly, to date, few interventions to prevent diabetes have focused on socioeconomic inequalities.29 Even in Switzerland, the national health strategy to prevent diabetes in the population fails to incorporate any action plan to tackle socioeconomic inequalities,30 while the national health strategy for health equity focuses primarily on access to healthcare and fails to incorporate any action plan to address the underlying causes of health inequalities.31
Conclusion
In this representative sample of Swiss adults living in Geneva, Switzerland, we found substantial, persistent and widening socioeconomic inequalities in diabetes prevalence. Public health interventions are urgently needed in order to address the specific needs and challenges of socioeconomically disadvantaged groups that are at higher risk of diabetes.
Acknowledgments
The authors express their gratitude to the participants of the Bus Santé Study, and to Dr José L Sandoval and David De Ridder for their valuable statistical and analytical support.
References
Footnotes
Contributors All authors designed the present study. CdM performed its statistical analyses and wrote the first draft of the manuscript. SS, IG and FRJ supervised the analyses, reviewed and provided critical comments on all drafts of the manuscript. IG and FRJ are the guarantors of the present study.
Funding This work was supported by a grant from the Fondation pour la Recherche sur le Diabète (Geneva, Switzerland).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Bus Santé Study was approved by the University of Geneva Ethics Committee (IRB00003116) and all study participants provided informed written consent to participate in the study. The study complied with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request from the corresponding author.