Article Text

Abstract
Introduction To describe diabetes trends among adults with incident tuberculosis (TB) disease and examine diabetes-associated TB characteristics and patient outcomes in the USA.
Research design and methods We examined all 71 855 persons aged ≥20 years with incident TB disease reported to the National Tuberculosis Surveillance System during 2010–2017. We performed multivariable logistic regression, comparing characteristics and outcomes among patients with TB reported to have diabetes and those whose diabetes status was unknown.
Results An overall 18% (n=13 281) of the 71 855 adults with incident TB disease were reported as also having diabetes; the annual proportion increased from 15% in 2010 to 22% in 2017. Among patients aged ≥45 years with both TB and diabetes, the adjusted OR for cavitary or sputum smear-positive TB was 1.7 and 1.5, respectively (95% CIs 1.5 to 1.8 and 1.4 to 1.6). Patients with TB and diabetes had 30% greater odds of dying and took longer to achieve negative Mycobacterium tuberculosis cultures and complete treatment.
Conclusions The prevalence of reported diabetes among adults with TB disease has increased. Having diabetes as a comorbidity negatively affects patient outcomes. In accordance with national recommendations, all patients aged ≥45 years and all younger patients who have risk factors for diabetes should be screened for diabetes at the start of TB treatment.
- tuberculosis
- epidemiology
- disease association
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
This is the first national analysis describing diabetes among persons with incident tuberculosis (TB) disease in the USA.
What are the new findings?
During 2010–2017, 18% of adult patients with TB in the USA were reported as also having a diabetes diagnosis.
Non-US-born patients with TB aged ≥45 years were reported as having the highest prevalence of diabetes.
Consistent with studies in other parts of the world, patients with TB who also had diabetes had more severe TB presentations (70% greater odds of having cavitary TB and 50% greater odds of smear-positive TB).
Patients with TB and diabetes had greater odds of death; among adults who did not die, however, TB treatment completion was >93%.
How might these results change the focus of research or clinical practice?
These findings underscore the national recommendation for baseline diabetes screening among all patients with TB aged ≥45 years and all younger patients who have risk factors for diabetes.
Introduction
For persons infected with Mycobacterium tuberculosis, having diabetes is thought to triple the risk of developing tuberculosis (TB) disease.1 Worldwide growth in diabetes prevalence is counteracting many countries’ otherwise successful TB control strategies.1 More advanced, infectious forms of TB disease is associated with lung cavities that are visible on chest radiograph and sputum that is smear positive for acid-fast bacilli.2 An international meta-analysis of pulmonary TB’s radiologic presentations found that compared with patients without diabetes, those with diabetes had more cavitary lesions.3 Prospective studies of newly diagnosed TB cases in Mexico and China found that compared with patients with TB without diabetes, those with diabetes who had started TB treatment experienced delays in achieving negative sputum smears and cultures for M. tuberculosis. They were also more likely to die.4 5 This greater risk for death was also the conclusion of an international systematic review and a recent analysis of TB cases in California.6 7
Since 1953, the Centers for Disease Control and Prevention has worked with local and state health departments to collect information about each case of TB disease in the USA. TB incidence has declined since 1993.8 9 However, because of increased concern about diabetes’ role as a frequent TB comorbidity, the National Tuberculosis Surveillance System (NTSS) added diabetes status to the standardized TB case data collection form in 2009.9 This is the first national analysis since the addition of that diabetes variable. We describe diabetes trends among adults with incident TB disease during 2010–2017 and examine TB disease characteristics and patient outcomes associated with diabetes.
Methods
Data source and definitions
We analyzed all verified TB cases reported to NTSS from the 50 US states and District of Columbia for 1 January 2010 to 31 December 2017. We excluded 6535 patients with TB aged <20 years because only 45 of these young people were also reported as having diabetes. We also excluded 13 persons with unknown age, none of whom were reported as having diabetes. During 2010–2017, a total of 71 855 persons aged ≥20 years were reported as having TB disease. Standard NTSS patient-level variables include demographics, clinical characteristics, and social risk factors associated with TB (eg, homelessness and substance use). Nativity was considered US-born if the patient had been born in the USA, a US territory, or abroad to at least one US citizen parent.
The diabetes variable, added in 2009, has been reported by all reporting areas since 2010. NTSS defines diabetes as diagnosis of diabetes mellitus either before or concurrent with the TB diagnosis.9 Health department staff completing the NTSS form must verify that the diagnosis is documented by a healthcare provider, but whether it is type 1 or 2 is not collected. Further, until 2020, NTSS did not collect any diabetes-related laboratory results, nor did it have a variable to indicate that diabetes had been ruled out (ie, anyone without a known diabetes diagnosis was coded for this analysis as having unknown diabetes status). Additional medical comorbidities collected in NTSS include HIV infection, end-stage renal disease, history of organ transplantation, or immunosuppression caused by another medical problem.
Prevalence calculations
For each year during 2010–2017, we determined the annual number and proportion of adults with incident TB who were reported as also having diabetes. To more accurately compare diabetes prevalence across racial/ethnic groups of patients with TB, age-adjusted prevalence for each racial/ethnic group was calculated by using the 2010 US population standard.10
Statistical analysis
We used logistic regression to assess which characteristics were associated with a reported diabetes diagnosis. Our multivariable model initially included any variables that were significant (p<0.05) on univariate analysis. The referent group was persons with unknown diabetes status, and we separately analyzed those aged 20–44 years and those aged ≥45 years. P values for comparing risk factors with continuous counts (eg, time to sputum conversion and time to treatment completion) were obtained by using the Wilcoxon rank-sum test.
Patient protections
NTSS operates under an Assurance of Confidentiality issued under Sections 306 and 308(d) of the US Public Health Service Act (42 USC 242k and 242m(d)). TB case reports were collected as part of routine public health surveillance; this retrospective analysis using existing and non-identifiable data was not considered research and did not require approval by an institutional review board.
Results
Prevalence of diabetes among patients with TB
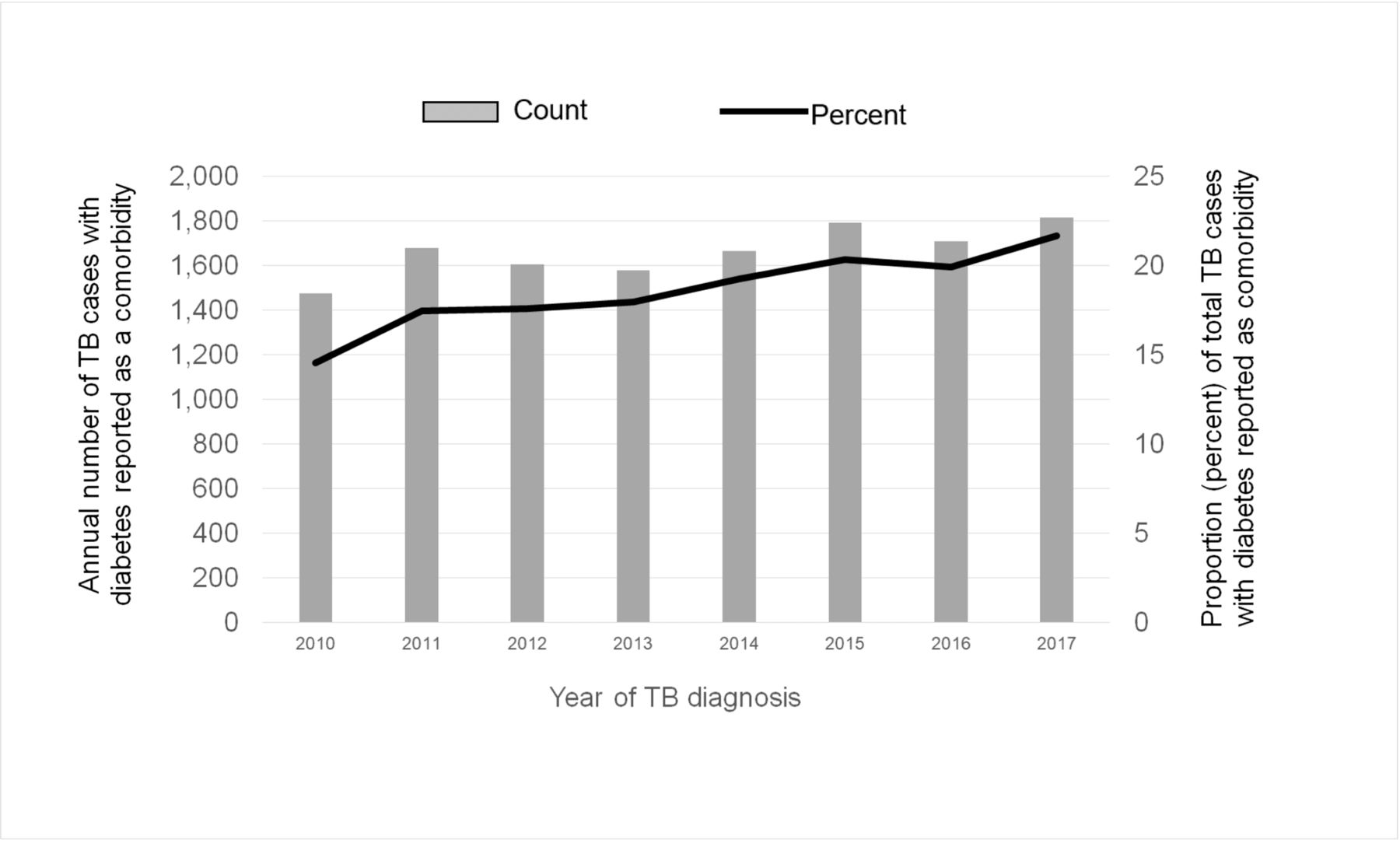
Of the 71 855 persons aged ≥20 years who were reported as having TB disease during 2010–2017, 18% were reported as also having a diagnosis of diabetes (n=13 281). Across the 8-year period, the annual proportion of adults with TB who also had diabetes increased from 15% in 2010 to 22% in 2017, and the annual case count of adults with both conditions increased from 1469 to 1815 (figure 1).
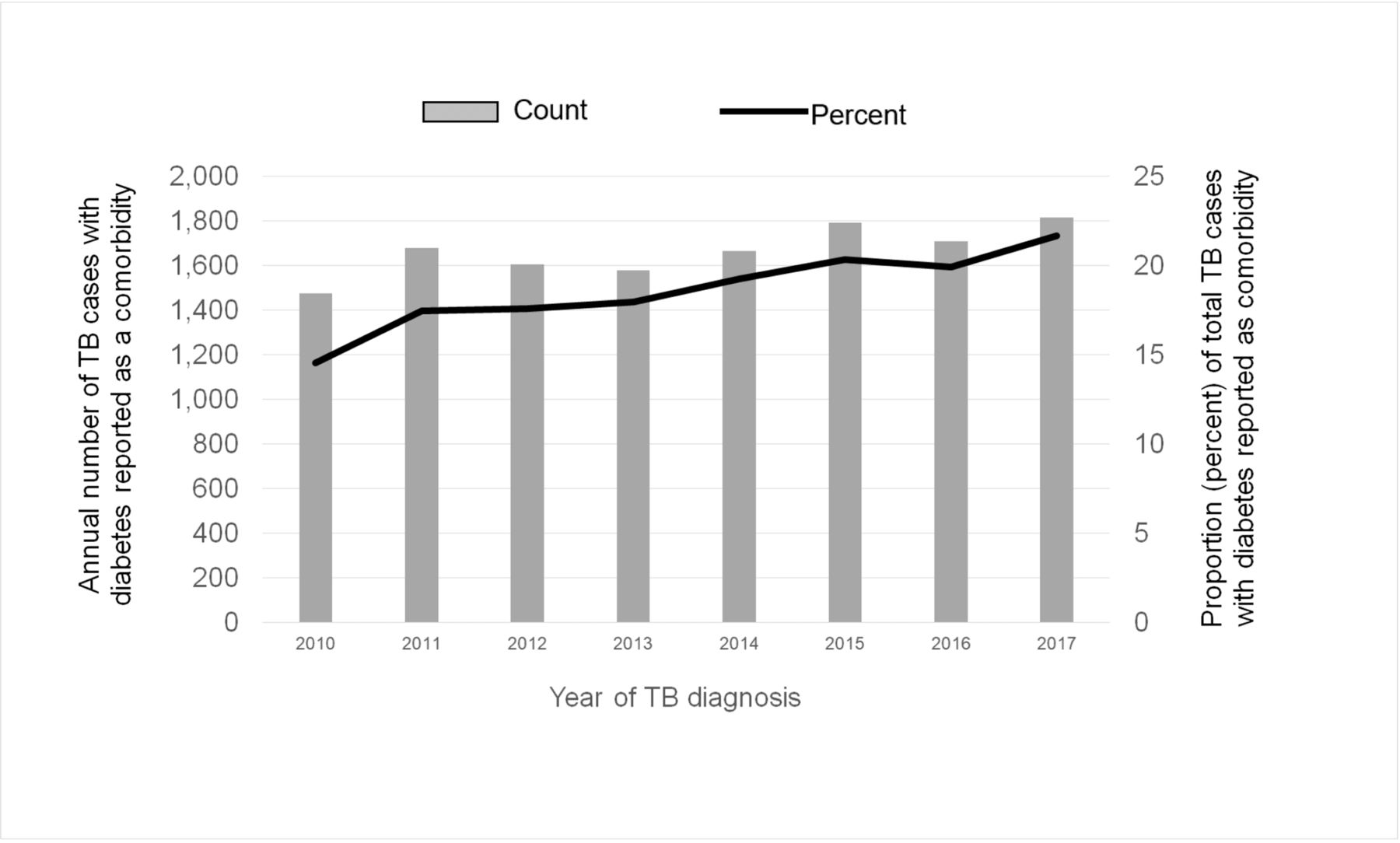
Diabetes reported as a comorbidity among adults with newly diagnosed tuberculosis (TB) disease, as annual count and proportion of total TB cases, USA, 2010–2017.
Descriptive results
Non-US-born patients with TB aged ≥45 years had the highest prevalence of diabetes (figure 2). After age adjustment, Native Hawaiian/Other Pacific Islander patients with TB had the highest prevalence of diabetes (37%), followed by Hispanic patients (23%) and non-Hispanic Asians (17%). (Age-adjusted prevalence by race/ethnicity is not shown in table 1, where the presented proportions are based on diabetes status.)

Age-specific prevalence of diabetes reported as a comorbidity among adults with tuberculosis (TB), by nativity and year, USA, 2010–2017.
Characteristics of adults with tuberculosis, by diabetes status, USA, 2010–2017
Approximately half of patients with TB who also had diabetes had pulmonary forms of TB that were smear positive for acid-fast bacilli, and nearly a third had evidence of cavitary TB on chest radiograph (table 1). Social risk factors for TB, including incarceration at the time of diagnosis, recent homelessness, and recent substance misuse, were less prevalent among patients with TB and diabetes. An exception to this pattern was residence in a long-term care facility at diagnosis, which was more prevalent among patients with TB who also had diabetes as a comorbidity (table 1).
Multivariable model results
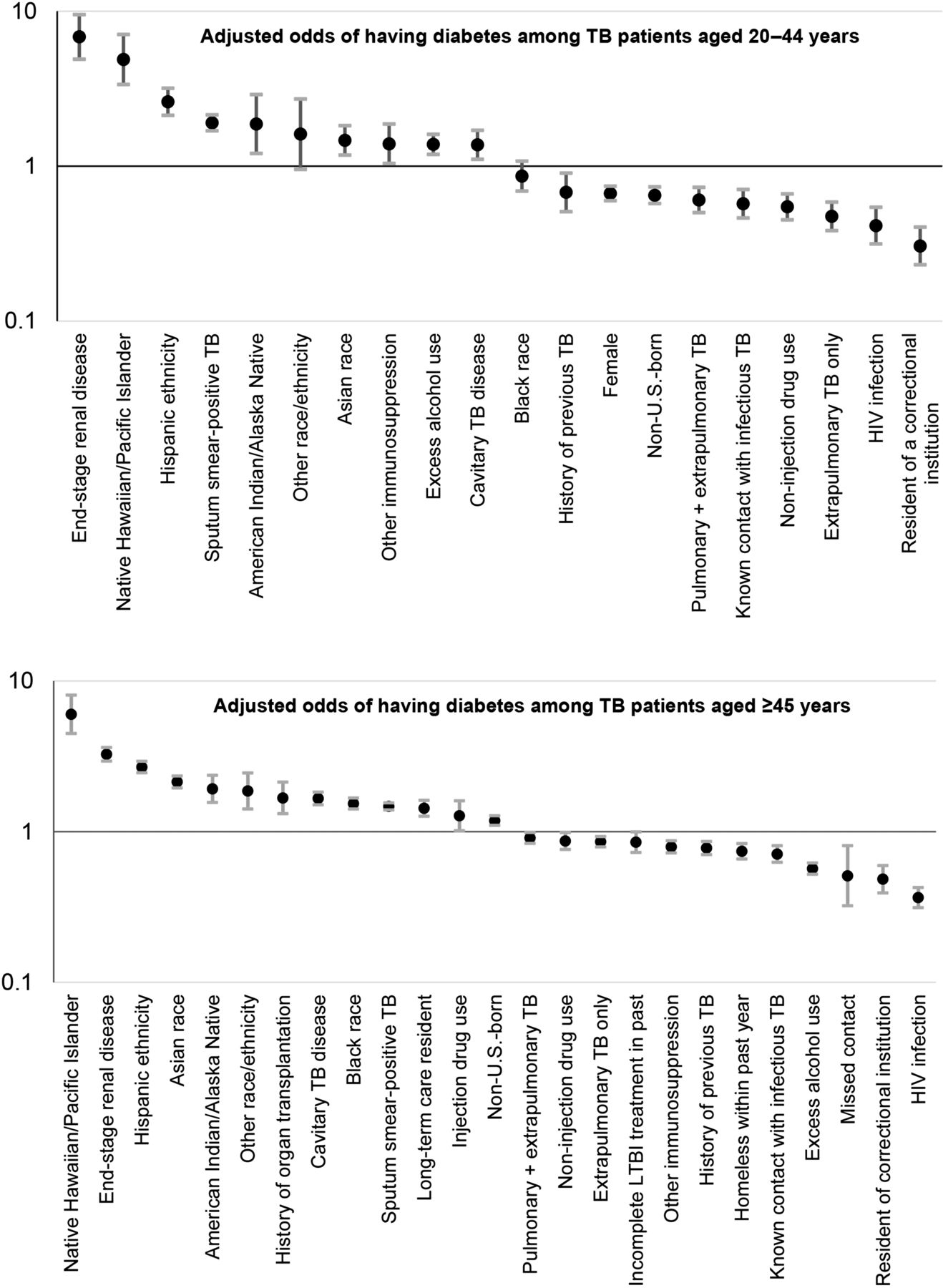
Figure 3 presents the adjusted odds of having diabetes as a comorbidity at the time of TB diagnosis; the ORs are presented in descending order from the strongest positive association to the strongest negative association. All variables included in the two age-based models are shown in figure 3. The adjusted odds of also having diabetes was higher among patients with end-stage renal disease (adjusted OR (aOR) if aged 20–44 years: 6.8; 95% CI 4.9 to 9.5; aOR if aged ≥45 years: 3.3; 95% CI 2.9 to 3.6). Among patients with TB aged 20–44 years, lower odds of diabetes was associated with residence in a correctional facility (aOR 0.3; 95% CI 0.2 to 0.4), HIV infection (aOR 0.4; 95% CI 0.3 to 0.5), and non-US-born nativity (aOR 0.7; 95% CI 0.6 to 0.7). In contrast, non-US-born nativity was positively associated (aOR 1.2; 95% CI 1.1 to 1.3) with diabetes among older patients with TB. Among patients with TB aged 20–44 years with diabetes, the aOR for cavitary or sputum smear-positive TB was 1.4 (95% CI 1.1 to 1.7) and 1.9 (95% CI 1.7 to 2.1), respectively, compared with that of patients in the same age group without a diabetes diagnosis reported. Among patients with TB aged ≥45 years with diabetes, the aOR for cavitary or sputum smear-positive TB was 1.7 (95% CI 1.5 to 1.8) and 1.5 (95% CI 1.4 to 1.6), respectively, compared with that of patients in the same age group without a diabetes diagnosis reported.

{kind=link}
{kind=link}
{kind=link}
Adjusted odds of having diabetes reported as a comorbidity among adults with tuberculosis (TB), by age group, USA, 2010–2017. LTBI, latent TB infection.
Patient outcomes
Patients with TB who had diabetes as a known comorbidity were more likely to die, either before TB treatment could begin or during treatment (table 2). However, the deceased patients with diabetes had an older age distribution than those with unknown diabetes status (table 2). Even after accounting for this older age distribution and excluding the deaths at time of diagnosis, patients with TB and diabetes had 1.3 (95% CI 1.1 to 1.5) the adjusted odds of death during the monthslong treatment period for TB.
Outcomes among adults with tuberculosis, by diabetes status, USA, 2010–2015*
After excluding all deaths, TB treatment completion was >93% for both adults with and without diabetes reported (table 2). However, those with diabetes required slightly more time to attain negative M. tuberculosis cultures (median days to sputum conversion: 47 vs 42; p<0.001) and an additional month to complete treatment (median days to complete TB treatment: 249 vs 212; p<0.001).
Discussion
Even as overall TB case counts declined 18% in the USA during 2010–2017,8 the prevalence of diabetes as a reported comorbidity among adults with TB disease steadily increased from 15% in 2010 to 22% in 2017. An initial interpretation might be that these findings are not surprising—given the high prevalence of diagnosed and undiagnosed diabetes in the USA—but the age-adjusted prevalence of diabetes during the same period is thought to have stabilized at an estimated 9.4% of the adult US population.11
An important limitation of this analysis is potential misclassification (under-reporting) of diabetes as a comorbidity. The 58 574 patients listed in table 1 as ‘diabetes status unknown’ include both adults who had diabetes ruled out and adults who were not evaluated for diabetes. Although this analysis could not discriminate between the two possibilities, that important distinction is part of the NTSS case report form revised in 2020. Diabetes was added to the form in 2009, so one might expect that health departments more systematically ascertained diabetes status toward the end of the 2010–2017 period. In addition, screening for diabetes might have increased after the 2016 recommendation to screen all patients aged ≥45 years at the start of TB treatment.2 Nevertheless, a strength of this first national analysis of diabetes among persons newly diagnosed with TB disease is that it is based on 71 855 patients with TB, including 13 281 reported to have diabetes as a comorbidity.
Despite this potential misclassification (which would be predicted to bias comparisons toward the null), having diabetes as a comorbidity at time of TB diagnosis appears associated with more severe presentations and poorer outcomes in the USA. Patients with TB who were aged ≥45 years and had diabetes had 70% greater odds of having cavitary TB and 50% greater odds of smear-positive TB. We also found 30% greater odds of dying during treatment. These findings are consistent with previous studies from other parts of the world.3–6 12
In our US analysis, patients with diabetes responded more slowly to TB treatment, as evidenced by a median of 5 more days to attain negative M. tuberculosis cultures. TB treatment regimens for persons with diabetes took a median of 37 days longer to complete. But in contrast with the findings of other studies,4 6 having diabetes did not appear to impede TB treatment completion, despite more complicated case management features, including end-stage renal disease, postorgan transplantation, and long-term care settings. In fact, after excluding deaths, TB treatment completion was >93% (table 2). And although a 2011–2014 study in Tbilisi, Georgia, found that patients with diabetes were more likely to have drug-resistant TB,12 our study found that patients with both TB disease and diabetes in the USA during 2010–2017 were not (table 1).
Our findings underscore the recent national recommendation for baseline diabetes screening among all patients with TB aged ≥45 years and all younger patients with risk factors for diabetes (ie, body mass index >25 kg/m2; first-degree relative with diabetes; Hispanic ethnicity; or African–American, Asian, American Indian/Alaska Native, or Hawaiian Native/Pacific Islander race).2 Like other infections, M. tuberculosis infection can worsen blood glucose control and complicate the clinical management of diabetes. Further, Harries et al have appealed for TB screening among persons with diabetes (ie, bidirectional screening).13 Indeed, global concern about the ‘converging epidemics of tuberculosis and diabetes’ has helped draw attention to the synergistic influence each might have on the other.14 15
The progression of untreated latent TB infection (LTBI) causes most of the TB disease in the USA.8 In older persons, diabetes and the ageing process itself synergistically reduce levels of interferon gamma, impairing cell-mediated immunity and helping to activate progression of long-standing LTBI.16 Both TB disease and LTBI in the USA occur primarily among non-US-born persons.8 17 18 Preventing active, infectious forms of TB disease thus requires scaling up of interventions to detect and treat LTBI in this population.19
The International Diabetes Federation projects that 693 million adults will have diabetes by 2024.20 Our analysis revealed that non-US-born patients with TB aged ≥45 years were reported as having a much higher prevalence of diabetes than US-born patients with TB in the same age group (figure 2), suggesting that the increasing diabetes prevalence worldwide could be affecting TB’s epidemiology in the USA. Addressing that challenge will require coordination between the private sector, where case management of diabetes often resides, and the public health sector, which has been charged with the responsibility for controlling and eventually eliminating TB in the USA.
Acknowledgments
We gratefully acknowledge the contributions and efforts of local and state health departments that report cases into the National Tuberculosis Surveillance System. We thank Kristen Renneker for her earlier unpublished analysis with 2009–2011 data and C Kay Smith for editorial services.
References
Footnotes
Contributors LRA conceived and executed the analysis. JSK provided analytic assistance. JSK and MBH reviewed interim results, provided interpretation, and suggested additional analyses. LRA created the first draft of the article, and MBH revised the article. All authors approved the final version.
Funding This is a publicly funded research by employees of the Centers for Disease Control and Prevention, Atlanta, Georgia.
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The National Tuberculosis Surveillance System operates under an Assurance of Confidentiality issued by the Centers for Disease Control and Prevention (CDC) under Sections 306 and 308(d) of the Public Health Service Act (42 USC 242k and 242m(d)). Data are reported voluntarily to CDC by state and local health departments on a case report form called the Report of Verified Case of Tuberculosis (OMB No. 0920-0026). The Assurance of Confidentiality prevents disclosure of any information that could be used to directly or indirectly identify patients. For more information, see the CDC/ATSDR Policy on Releasing and Sharing Data (at http://www.cdc.gov/maso/Policy/ReleasingData.pdf). A limited dataset is available at http://wonder.cdc.gov/TB-v2013.html. Researchers may apply to analyze additional data at CDC headquarters by contacting TBInfo{at}cdc.gov.