Article Text

Abstract
Introduction A growing body of evidence suggests that specific, naturally occurring gut bacteria are under-represented in the intestinal tracts of subjects with type 2 diabetes (T2D) and that their functions, like gut barrier stability and butyrate production, are important to glucose and insulin homeostasis. The objective of this study was to test the hypothesis that enteral exposure to microbes with these proposed functions can safely improve clinical measures of glycemic control and thereby play a role in the overall dietary management of diabetes.
Research design and methods We evaluated whether a probiotic comprised of these anaerobic bacteria would enhance dietary management by (1) manufacturing two novel probiotic formulations containing three (WBF-010) or five (WBF-011) distinct strains in a Current Good Manufacturing Practice (cGMP) facility, (2) establishing consistent live-cell concentrations, (3) confirming safety at target concentrations dispensed in both animal and human studies and (4) conducting a 12-week parallel, double-blind, placebo-controlled, proof-of-concept study in which subjects previously diagnosed with T2D (n=76) were randomly assigned to a two times a day regimen of placebo, WBF-010 or WBF-011.
Results No safety or tolerability issues were observed. Compared with the placebo group, subjects administered WBF-011 (which contains inulin, Akkermansia muciniphila, Clostridium beijerinckii, Clostridium butyricum, Bifidobacterium infantis and Anaerobutyricum hallii) significantly improved in the primary outcome, glucose total area under the curve (AUC): −36.1 mg/dL/180 min, p=0.0500 and also improved in secondary outcomes, glycated hemoglobin (A1c): −0.6, glucose incremental-AUC: −28.6 mg/dL/180 min.
Conclusions To our knowledge, this is the first randomized controlled trial to administer four of the five strains to human subjects with T2D. This proof-of-concept study (clinical trial number NCT03893422) shows that the intervention was safe and well tolerated and that supplementation with WBF-011 improves postprandial glucose control. The limited sample size and intersubject variability justifies future studies designed to confirm and expand on these observations.
- diabetes mellitus, Type 2
- glycated hemoglobin A
- fatty acids
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Previous trials testing the efficacy of probiotics have used commercially available species that are not known to be absent or decreased in type 2 diabetes.
Type 2 diabetes has been associated with abnormalities of the gut microbiome, particularly decreases in abundance of Akkermansia muciniphila and microbes involved in the conversion of dietary fiber to butyrate and other short-chain fatty acids.
An increase in the abundance of butyrate producers and Akkermansia muciniphila induced by metformin treatment has been proposed as a supporting mechanism for the efficacy of this critical antidiabetic drug.
What are the new findings?
Subjects with type 2 diabetes, currently using metformin, improved glucose control relative to placebo after 12-week administration of a novel probiotic formulation containing both butyrate producing bacteria and Akkermansia muciniphila.
Improvement was observed via standard clinical measures for both short-term (meal-tolerance test glucose area under the curve) and long-term (A1c) glucose control, in a subject cohort that was stable on first-line treatment, predominantly metformin.
No major probiotic supplementation-related side effects were observed.
Significance of this study
How might these results change the focus of research or clinical practice?
Administration of disease-relevant microbial species may be a promising new dietary management tool for improving glucose control in type 2 diabetes, or delaying disease progression.
These findings support additional trials with a larger patient population, longer intervention period, and new or different probiotic formulations.
Introduction
Diabetes is the seventh leading cause of death in the USA and in 2017 accounted for an estimated $327 billion in direct costs and lost productivity.1 2 Over 20 million individuals are currently diagnosed with type 2 diabetes (T2D), some 90% of total diabetes diagnoses.3 While genetic factors affect susceptibility,4 it is also evident that Western lifestyle and diet plays a large role5 6 and may be mediated by differences between the gut microbiomes of healthy and T2D individuals.7 8
Abnormalities of the T2D microbiome are characterized by a decreased abundance of Akkermansia muciniphila9 and reduction in microbes involved in the saccharolytic fermentation of dietary fiber to short-chain fatty acids (SCFAs), especially butyrate.10 11 Fecal microbiome transplants from healthy human subjects resulted in metabolic improvements in a small pilot study of individuals with T2D.12 Although this study provided early evidence of a causal relationship between the gut microbiome and T2D, fecal transplants are not viewed as a widely applicable therapeutic, given challenges in social acceptance, safety, manufacturability and consistency.13 14 Probiotics can potentially resolve these issues, and a number of randomized controlled trials have been conducted using commercially available probiotics for the treatment of T2D,15 and multiple meta-analyses find that the results are strain-specific and mixed,16 but encouraging.17 However, many of the species included in probiotics employed in these trials are lactic acid producers associated with food production (Lactobacillus spp, Bifidobacteria spp, Bacillus coagulans, Streptococcus thermophilus, and Saccharomyces boulardii), and all are oxygen tolerant or even capable of facultative growth (with the exception of some species of Bifidobacteria). This is in contrast to A. muciniphila and many of the key butyrate producers of the human gut, which are obligate anaerobes. We hypothesize that a functionally targeted probiotic formulation containing key, strictly anaerobic members of the healthy human microbiota can enhance dietary management and improve clinical measures of glycemic control in individuals with T2D. Accordingly, we selected the following species for exploration as a potential probiotic for T2D, A. muciniphila, Anaerobutyricum hallii (formerly Eubacterium hallii18), Clostridium beijerinckii, Clostridium butyricum, and Bifidobacterium infantis.
First isolated in 2004 from mucin-degrading enrichment cultures of human feces,19 A. muciniphila appears to be specialized for residence in the human gut mucosa20 and is detected in most healthy human feces, typically comprising 1%–5% of the healthy human gut microbiota.21 A decreased abundance of A. muciniphila has been correlated with prediabetes,22 obesity,23 and T2D;24 and increased abundance of A. muciniphila induced by metformin treatment has been proposed as a supporting mechanism for the efficacy of this critical antidiabetic drug.25 Elucidation of the mechanism(s) by which A. muciniphila positively affects human health are ongoing, but proposals include the improvement of gut barrier function and metabolic parameters through an outer membrane protein binding to TLR2,26 intestinal levels of endocannabinoids that control inflammation and gut peptide secretion,20 as well as epithelial-localized SCFA production from mucin-derived glycans.27 28 A. muciniphila has been proposed as a promising candidate for probiotic therapy,9 and the first reported human administration of A. muciniphila found that it was well-tolerated, and appeared to improve metabolic markers in overweight and obese volunteers relative to placebo.29
Butyrate is the preferred energy source for colonocytes, and also acts as a signaling molecule that (1) binds to specific g-protein coupled receptors (eg, GPR41) on the surface of gut epithelial cells and immune cells, regulating the secretion of pro-inflammatory cytokines (eg, interleukin-18 (IL-18)); (2) acts on central-nervous system regulation of food intake and energy expenditure through glucagon-like peptide 1 (GLP-1) and peptide tyrosine-tyrosine; and (3) acts as a histone deacetylase inhibitor in immune cells and adipocytes, regulating these cells’ transcription through chromatin state.30 31 Human gut microbes typically synthesize butyrate via an energy-conserving (net reduction) condensation of two molecules of acetyl-CoA, the latter derived from a variety of pathways and substrates32 but with the predominant extracellular substrates being acetate and (to a lesser extent) lactate produced during primary fermentation of carbohydrates.31 33 34 A recent pilot study reported a 4-week single-blinded single-strain administration of the butyrate producer Anaerobutyricum soehngenii, a species recently distinguished from A. hallii,18 to human males with metabolic syndrome. No significant changes were detected in primary outcomes, but the authors describe hopeful trends.35
Here, we describe the identification, controlled manufacture, and evaluation of a novel multistrain probiotic formulation specifically designed for individuals with T2D. This probiotic contains members of the complex oligosaccharide consuming species A. muciniphila and B. infantis, the butyrate producers A. hallii, C. beijerincki, and C. butyricum, as well as a dietary fiber, inulin, derived from chicory root. This formulation has multiple opportunities for mutualistic interactions related to butyrate production. These can be formulated as the hydrolysis and fermentation of mucin to acetate by A. muciniphila36 or mucin-derived oligosaccharides to lactate by B. infantis,37 coupled with the butyrogenic consumption of acetate by C. beijerinckii and C. butyricum, or of either compound by A. hallii.31 37 Examples of related syntrophic interactions have been described for A. muciniphila-A. hallii,38 B. infantis-A. hallii,33 37 and B. infantis-C. butyricum.39 We present the design and results from this initial proof-of-concept clinical study, including clinical endpoints for T2D, qPCR confirming presence of formulation strains in subject stool, general microbiome profiling, and an assessment of fecal SCFA concentrations. To our knowledge, this is the first randomized controlled trial to administer a probiotic containing the strains A. muciniphila, A. hallii, C. beijerinckii, or C. butyricum to humans diagnosed with T2D.
Methods
Proof-of-concept clinical study
Study overview
We conducted a multicenter, randomized, double-blind, parallel-group, placebo-controlled proof-of-concept study at six sites across the US (start date: 22/10/2017; registration: 28/03/2019; trial identifier NCT03893422). Adults with T2D - defined as fasting glucose ≥126 mg/dL or glycated hemoglobin (A1c) of ≥6.8% - treated with diet and exercise alone, or in combination with metformin with or without a sulfonylurea and body mass index between 25 and 45 kg/m2 were eligible. Subjects were excluded if they had received an antibiotic, antifungal, antiparasitic, or antiviral treatment within 30 days prior to study entry. Study Protocol, Statistical Analysis Plan, and CONSORT 2010 checklist list complete details of inclusion/exclusion criteria (online supplementary texts S1–S3, respectively).
Supplemental material
Supplemental material
Supplemental material
Study design
Independent random sequences of study product assignments were generated separately for each clinical site prior to initiation and enrollment. The assignments were generated in permutation blocks of three to minimize potential imbalance within a clinical site. To ensure that proper blinding was maintained at clinical sites and minimize the impact of inadvertent or explicit unblinding, study product was labeled uniquely for each subject via a subject-specific “kit code” that was assigned to a subject at their baseline (postscreening) visit, and for which study product bottles had already been labeled centrally during manufacture of the two formulations and placebo. As this was a double-blind study, the sponsor staff involved in study conduct, clinical site staff and study participants were unaware of the mapping between the kit code labels and the study product assignment or capsule contents. Each subject received 12 identical product bottles containing 45 size 0 capsules (1 week supply+3 extra capsules). At each visit, subjects were given the number of bottles required to cover dosing until the next scheduled visit. Empty bottles and any unused capsules were returned to the clinic at the subsequent visit, where unused capsules were recorded to assess compliance. All study participants were instructed to swallow three capsules two times a day within 30 min of morning and evening meals.
A sample size of between 20 and 25 subjects per arm with compliant endpoint data was selected to achieve 80% power at the 5% level using an unadjusted standard two-sample t-test. We reasoned that products capable of a 0.5% or larger A1c decrease relative to placebo would warrant further exploration and used 0.5 for the SD based on McDonald and Warren.40 The comparison of glucose control outcomes between arms was predefined in the Statistical Analysis Plan (online supplementary text S2).
Study procedures and endpoints
Safety was measured by monitoring administration emergent adverse events along with routine safety laboratory measures. The primary metabolic endpoint examined was the 12 week change from baseline in area under the curve (AUC) for glucose during a standard 3 hour meal-tolerance test (total glucose AUC0-180 min) using two servings of Boost Plus Nutritional Drink (Nestle Health Science, Epalinges, Switzerland), containing a total of 720-calories per challenge. The primary endpoint related to systemic inflammation was the 12 week change from baseline in C-reactive protein (CRP).
Exploratory outcomes
A number of exploratory outcomes were investigated in an attempt to elucidate potential effects of the active interventions. Additional metabolic outcomes included the 12-week change from baseline in incremental glucose AUC0-180 min, A1c, fasting glucose and insulin as well as both incremental and total area under the insulin curve during the meal-tolerance tests. Additional markers of systemic inflammation were measured, including IL-6, IL-10, tumor necrosis factor α (TNFα) and transforming growth factor β (TGF-β).
Statistical analyses of primary outcomes
All analyses of primary outcomes and the per-protocol cohort were predefined in the statistical analysis plan prior to unblinding and performed using R V.3.6.1. Stepwise modeling of 12-week change to total glucose AUC0-180 min and CRP was performed using a generalized linear modeling framework assuming conditional normality of response variables. The adjusted models provide estimates of between group (formulation—placebo) effects, their respective 95% CIs, and p values for the t-test of the null hypothesis while accounting for potential between-group nuisance effects. To control the study-wise error rate at 0.05, a sequential testing procedure was used. The four null hypotheses corresponding to the primary outcomes were tested sequentially until the first non-significant hypothesis was encountered (one-sided, p>0.1). The order of measures tested was: total glucose AUC for WBF-011, total glucose AUC for WBF-010, CRP for WBF-011, CRP for WBF-010. Reported p values from the unadjusted model and from key exploratory measures are provided exclusively for descriptive purposes. Complete details of the statistical analyses performed are available in the statistical analysis plan (online supplementary text S2).
Protocol approval
The trial protocol (online supplementary text S1) was approved by a central institutional review board (Allendale, Old Lyme, Connecticut, USA). The trial was conducted in accordance with the Declaration of Helsinki as amended in 2013 and Good Clinical Practice guidelines. Written informed consent was obtained from each subject prior to participation in any trial activities.
Additional methods
Additional methods include descriptions of the protocol amendments, production of the study product formulations, as well as microbiome and SCFA measurements from subject stool (online supplementary text S4). When explicitly referring to the strains included in this study product and not their bacterial species designation in general, we use the following 4-letter identifiers also shown in parenthesis in figure 1 panel B: A. muciniphila, AMUC; A. hallii, EHAL; C. beijerinckii, CBEI; C. butyricum, CBUT; B. infantis, BINF.
Supplemental material

Summary of trial. (A) CONSORT flow diagram of subject enrollment, allocation, and follow-up counts. A total of 76 subjects were randomized at one of six US study sites and allocated by block to one of three experimental arms. Withdrawal from study participation was similar across arms, whereas those on placebo were more likely to discontinue the intervention. (B) Ingredients present in respective formulation capsules. Specific per-strain viability is provided in online supplementary table S1. A description of study formulation production is provided in online supplementary text S4. (C) Graphical summary of glucose control measurement outcomes. Primary endpoint was total glucose AUC0-180 min, while incremental glucose AUC0-180 min and A1c were key secondary measures. Additional detail is provided in table 2 and online supplementary figure S1. AUC, area under the curve.
Supplemental material
Mean changes in glycemic control parameters between baseline and week 12
Results
Trial population
From October 22, 2017 to June 1, 2018, 76 subjects were enrolled at six centers across the USA; 26, 27, and 23 individuals were randomly assigned to receive placebo, WBF-010, and WBF-011, respectively (figure 1). Baseline characteristics were generally similar across experimental arms in both intent-to-treat and per-protocol populations (table 1).
Baseline demographics for intent-to-treat and per-protocol populations by arm
Safety
A total of 27 and 23 participants were exposed to two microbiome formulations, WBF-010 and WBF-011 for an average of 77 and 78 days, respectively. Online supplementary table S2 lists the adverse events, by system organ class, that occurred in ≥4% of subjects in any group throughout the period of study product administration. The intensity of all events was rated as mild to moderate by the investigators and occurred with lowest frequency in the WBF-011 group. All study products were well-tolerated with tolerability issues limited to gastrointestinal complaints (diarrhea, nausea, and vomiting), which were reported somewhat less frequently in the WBF-011 group (online supplementary table S2).
Primary endpoints: glycemic control and inflammation
No significant change compared with placebo was observed in inflammatory markers, including the primary endpoint measure, CRP (WBF-011: log ratio CRP effect=0.04, p=0.6797; WBF-010: 0.02, p=0.8018; see online supplementary figures S7–S9).
Significant improvement in total glucose AUC0-180 min was not detected in the WBF-010 group. Incremental glucose AUC0-180 min and A1c were both nominally decreased in the WBF-010 group relative to the placebo group, but were not statistically significant under this analysis framework (table 2, online supplementary figure S1).
Compared with placebo, a statistically significant decrease in total glucose AUC0-180 min was observed in WBF-011 group (−36.1 mg/dL/180 min; p=0.0500; t-test of the null hypothesis: WBF-011—placebo≥0.0), corresponding to a median within-group decrease of 7.0% for WBF-011 and a median within-group increase of 3.2% for placebo. Incremental glucose AUC0-180 min was also lower in WBF-011 group (−28.56 mg/dL/180 min; p=0.0066; t-test of the null hypothesis: WBF-011-placebo ≥ 0.0); corresponding to a median within-group decrease of 32.5% for WBF-011 and a median within-group increase of 26.4% for placebo. The validated measure of long-term glucose control, A1c, was reduced by 0.6 compared with placebo (p=0.0540; t-test of the null hypothesis: WBF-011-placebo≥0.0), a within-group reduction of 0.2 (table 2, online supplementary figure S1).
Strain-specific qPCR
We were able to detect individual probiotic strains in subject stool via custom qPCR primer pairs (online supplementary table S3, text S4); and the pattern was largely consistent with the study design (figure 2). In particular, AMUC and BINF primers had positive reactions in nearly all of the subject stool samples at weeks 4 and 12 for their corresponding formulation groups, but virtually no positive hits at baseline or for any samples from subjects in the placebo group (figure 2). Detection of the other three strains was less consistent. EHAL was detected more frequently (45%–75%) at weeks 4 and 12 among subjects administered WBF-011 than at their baseline (15%) or for the samples of the other study arms not receiving EHAL (0%–25%). Detection of CBEI and CBUT was poorly distinguished from baseline or placebo, indicating that fecal concentrations were below the limit of detection. At week 16, 4 weeks after the cessation of intervention (washout period), detection frequency of AMUC, BINF, and EHAL decreased substantially (figure 2 and 80%–95% decrease).
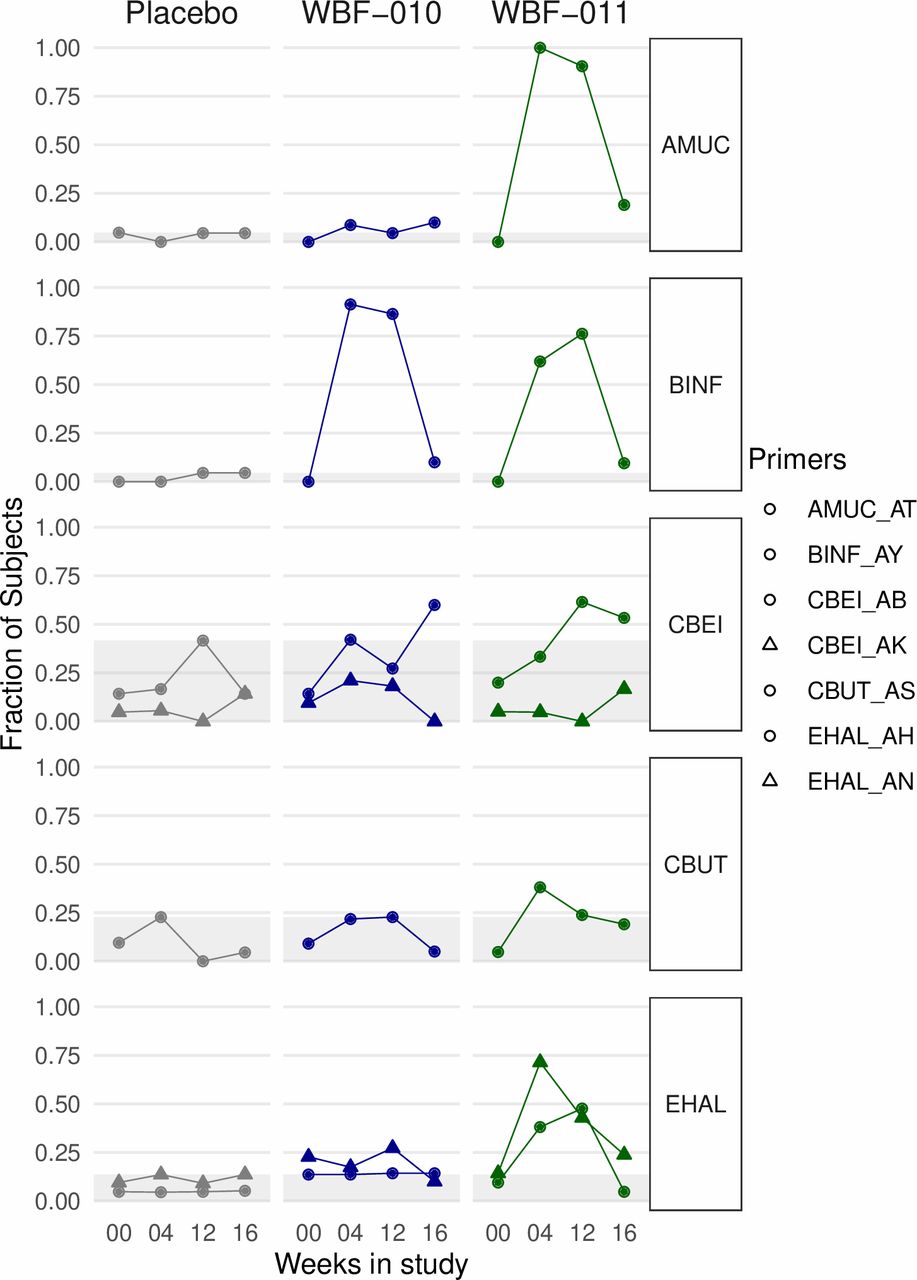
Rates of detection of probiotic strains via qPCR at each of four collection timepoints. Each point indicates the fraction of subjects in a study arm that had at least two replicates with positive detection. Light gray box indicates the y-axis range of proportions observed in samples from subjects randomized to the placebo group. Point shape distinguishes separate primer-pairs for the same strain. Primer sequences are defined in online supplementary table S1. All stool homogenate samples were measured in at least quadruplicate reactions for each primer-pair.
Amplicon sequencing of 16S rRNA gene V4 region
In microbiome profiling via amplicon sequencing of the 16S rRNA gene V4 region (heretofore “16SV4”), we did not detect any large changes to a subject’s overall microbial community following intervention. The log-ratio of alpha diversity at week-12 to baseline was not significantly different from zero for any arm, nor were arms significantly different from each other (online supplementary figure S3B). Similarly, beta-diversity distance between a subject’s stool at week-12 and baseline was low in value (<0.1) and typically in the bottom one-fourth of the distribution of between-subject distances for each arm (online supplementary figure S3C). At baseline, we did not detect systematic differences in stool microbiome profiles between arms, which could have otherwise confounded the relationship between intervention and outcome (online supplementary figure S3).
The phylogenetic resolution of 16SV4 often does not allow discrimination between strains of the same species. Nevertheless, we assessed whether sequences matching the 16SV4 region of the formulation strains were present and correlated with the strain-specific qPCR results. We observed some important differences between the 16SV4 and qPCR detection profiles, including an elevated frequency of A. muciniphila detection in the placebo arm (~50%) relative to the others (25%), and a high frequency (75%–100%) of A. hallii detection across all study arms and time points. B. infantis were detected in ~25% samples across all study arms and timepoints, C. butyricum and C. beijerinckii were mostly below the limit of detection (online supplementary figure S4).
Short-chain fatty acid analysis
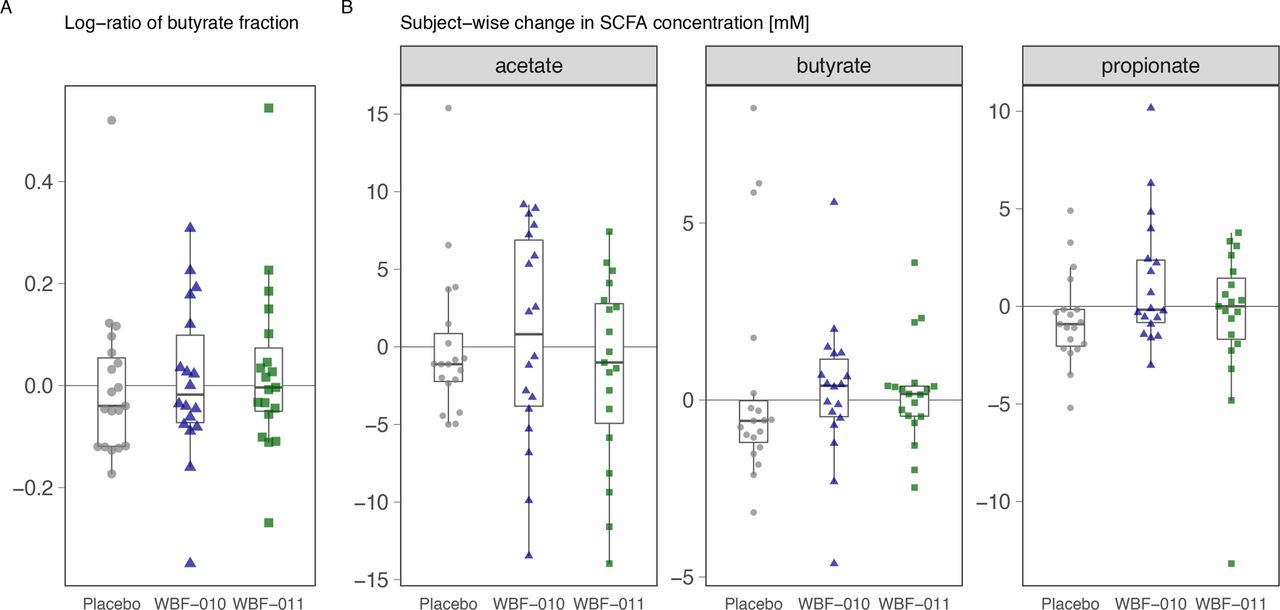
In measurements of stool SCFA, we did not observe statistically significant changes. However, we did observe a small increase in butyrate concentration over 12 weeks relative to baseline for both the WBF-010 and WBF-011 groups, as well as a difference in the sign of median change (figure 3B) relative to placebo. No trend was observed for the ratio of butyrate to the sum of acetate, propionate and butyrate (figure 3A), though acetate does appear more variable in WBF-010 and WBF-011 groups compared with placebo. A slight trend between the change in butyrate concentration and change in A1c was observed, only for the WBF-011 group (online supplementary figure S5).

{kind=link}
{kind=link}
{kind=link}
Summary of subject-wise changes in stool SCFAs. Each point in each panel represents a different subject in the study. (A) Change in the stool butyrate fraction of total SCFA (acetate, propionate, butyrate), shown as the per-subject Log10-ratio of week-12 to baseline. (B) Changes in the millimolar concentration in stool. Changes are represented as baseline subtracted from week-12 (median difference for technical replicate pairs). Panels separate the values for each SCFA. Further detail is provided in online supplementary text S4. SCFA, short-chain fatty acid.
Discussion
Three new classes of therapies for T2D have been introduced since 2005: GLP-1 receptor agonists, DPP-IV inhibitors, and SGLT2 inhibitors. Each of these therapeutic classes has been plagued by significant safety concerns including pancreatitis, congestive heart failure, increased genital infections, gangrene, and increased risk of lower extremity amputation. A major hope underpinning the search for a probiotic intervention for use in the management of T2D is that a product can be formulated which confers benefit with limited incremental safety risks.41 42 This expectation is premised on inclusion of specific strains that have been sourced from healthy donors and are among taxonomic groups that have coevolved with the human body for millennia without pathologic effect. By selecting strains that satisfy these requirements and also restore or augment specific functions missing in disease, we hypothesize a lower overall safety risk during clinical use.
Correspondingly, safety was an important outcome in this proof-of-concept evaluation of two formulations in subjects with T2D. As expected, all strains were sensitive to multiple antibiotics and no genomic signals related to pathogenicity were detected. Prior to the present study, WBF-010 and WBF-011 safety was assessed in a 30-day rodent study (Sprague Dawley rat), without clinical, biochemical, or histopathologic evidence of concern. These strains were also administered to healthy human subjects for 14 days with an escalating serving quantity, observing no evidence of toxicity. In the present study, no safety issues were observed, and adverse events occurred at a similar (WBF-010) or lower (WBF-011) rate compared with the placebo group. Possible side-effects related to study products were limited to transient mild nausea, loose stools, and diarrhea during the initial 3–5 days of use. There was no observed effect on body weight, lipid parameters, or multiple measures of systemic inflammation. No change was seen in the inflammatory markers CRP, IL-6, IL-10, TNF-α, or TGF-β (online supplementary figures S7–S9), which were also monitored as potential indicators of improved gut barrier function. Stool microbiome profiling via 16S rDNA amplicon sequencing did not reveal any large or consistent changes to the stool microbiota as a result of taking either product (online supplementary figure S3B,C), suggesting that neither probiotic formulation caused a large or consistent disruption to the resident microbiome and that subjects were likely compliant in avoiding substantive changes to their diet during the study period, as instructed.43 44
Ingestion of WBF-011 for 12 weeks resulted in a statistically significant (p=0.0500) reduction compared with placebo in the primary endpoint, total glucose AUC0-180 min during a standardized meal challenge test (table 2). Key secondary measures of glucose control also improved relative to placebo, namely incremental glucose AUC0-180 min and A1c. Each of these between-group improvements are explained by a parallel decrease in the WBF-011 group and an increase in the placebo group. Respective total and incremental glucose AUC0-180 min decreased within-group by 14.9 and 11.7 for WBF-011, while placebo increased within-group by 21.2 and 16.9 (mg/dL/180 min). Consistent with these improvements in the meal challenge test, the WBF-011 group A1c decreased by 0.6% compared with placebo, corresponding to a within-group decrease of 0.2%, and a placebo within-group increase of 0.4% (table 2). As A1c measures an approximate 3-month average glucose concentration in blood, it is a lagging indicator that is challenging to capture in a study of only 12 weeks duration. These results suggest a potential for longer studies with A1c included among the primary endpoints to further establish improvements in glucose homeostasis.
No change was detected in fasting glucose concentrations in subjects administered WBF-010 or WBF-011. Without a change in fasting glucose concentrations, and considering a larger proportionate decrease in incremental glucose AUC0-180 min, the improvements in glycemic control in WBF-011 appear to be driven by a reduction in the plasma glucose concentrations during the postprandial period. Body weight and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) also remained unchanged throughout the study period indicating that the improvements in glucose control may be independent of both weight loss and changes in insulin sensitivity. Although not significant, changes in postprandial insulin concentrations, assessed as the difference in incremental and total area under the insulin curve during the meal tolerance tests, show a trend for WBF-011 consistent with increased insulin secretion (table 2).
A heterogenous dropout rate was observed between the randomized groups, including a notably higher dropout rate in the placebo group (placebo: 10, WBF-010: 6, WBF-011: 2), that coincided with a shift in mean baseline A1c between the intent-to-treat and per-protocol populations (placebo: 8.9, 8.2; WBF-010: 8.5, 8.2, WBF-011: 8.8, 8.9, respectively, table 1). This warranted further scrutiny in case it revealed a possible risk of structural bias or informed future study designs. The most differential mode of dropout occurred via study product compliance failure (placebo: 5, WBF-010: 1, WBF-011: 0), which was defined prior to unblinding as reported capsule consumption lower than 85% for the overall study or lower than 85% for the final 4 weeks of probiotic supplementation (online supplementary text S2). That the subjects remaining in the per-protocol population were product compliant is corroborated by the pattern of qPCR detection of AMUC and BINF at weeks 4 and 12 of intervention (figure 2). Study withdrawal was the other major mode of dropout, although less differential among the arms (placebo: 4, WBF-010: 4, WBF-011: 2). A related study design concern for new microbiome-targeted products is that differential gastrointestinal symptoms will complicate or even invalidate blinding; for example, subjects randomized to placebo would notice the absence of gastrointestinal effects and subsequently withdraw participation or decrease their enthusiasm for product compliance. However, in this study, incidence of gastrointestinal symptoms was slightly lower in the WBF-011 group compared with the other arms (placebo: 27%, WBF-010: 26%, WBF-011: 15%). An underlying explanation for the higher dropout rate in placebo remains unclear. Additional studies will be needed to determine if modifications to recruitment or design can improve the homogeneity of dropout rates between arms, and whether this influences the observed effects.
The WBF-011 formulation was the same as WBF-010 but with an additional two strains, namely AMUC and EHAL (figure 1, online supplementary table S1). While WBF-010 group measures of glycemic control trended in the direction of improvement relative to placebo, they were not statistically significant, and only incremental glucose AUC0-180 min achieved a within-group decrease of nominal significance (table 2, online supplementary figure S1). It therefore seems likely that one or both of {AMUC, EHAL} are necessary for the observed effect on glycemic control, but understanding whether they are sufficient for the effect will require additional study. The competing explanations include that one or more of {CBUT, CBEI, BINF} are also required for sufficiency, and the present study design cannot distinguish among these alternatives. Future studies should explore which subset of the presently described strains are sufficient to recapitulate the observed improvements in glycemic control and whether any of the previously hypothesized synergistic interactions can be demonstrated in vivo.
The challenges and limitations of interpreting measurements of DNA from human stool are well documented,45 particularly when the site of biological interest is expected to be localized at or near the mucosa.46 Nevertheless, some intriguing patterns were: (1) The three butyrogenic strains were detected more weakly via qPCR than AMUC and BINF, with EHAL detected the most frequently among them (50%–75%, figure 2). These detection differences in stool did not correlate with clinical response. (2) In 16SV4 microbiome profiling data, there was detection of A. muciniphila and A. hallii species in samples naive to WBF-011, particularly A. hallii detected in most samples (online supplementary figure S4). This observation is consistent with a previous metagenomic meta-analysis in which A. hallii is among the few known butyrogenic species that appear overrepresented in T2D relative to healthy control subjects.32 (3) The qPCR detection signal-to-noise was reasonable for all strains except CBUT and CBEI, which were difficult to detect even with multiple rounds of primer-pair development.
Stool is also a challenging proxy for understanding SCFA concentrations or flux at the intestinal mucosa,47 and subject-specific variability was high relative to changes. Nevertheless, we observed a small positive change in nominal concentration of propionate and butyrate in stool from subjects treated with both WBF-010 and WBF-011 compared with placebo. There was also a wider range of changes in subject stool acetate concentration, with more and larger decreases in acetate observed for WBF-010 and WBF-011 than placebo. The ratio of butyrate to the sum of acetate, propionate, and butyrate was slightly more positive than placebo (figure 3). We also observed a small trend between changes in A1c and changes in butyrate in subjects administered WBF-011 (not statistically significant; online supplementary figure S5). While it is tempting to speculate that these trends are consistent with a role of SCFA, and butyrate in particular, they should be interpreted with caution given the low signal-to-noise and the limitations of stool as a proxy.
Limitations of this initial proof-of-concept study include statistical power due to the small sample size, imbalance created by the higher discontinuance rate in the placebo group, and participants with relatively short duration of disease as reflected by their treatment regimens. A potential confounder is the heterogeneity in the study population introduced by the protocol amendment to allow inclusion of subjects treated with metformin plus a sulfonylurea agent, as these subjects likely have a longer duration of diabetes, and they responded worse as a (poorly powered) subset of those randomized to WBF-011. This study did not measure a dose-response relationship, the optimal duration of administration, or the durability of effect. GLP-1 levels were not directly measured; however, a marker of GLP-1 action was measured: plasma insulin concentrations during meal tolerance tests. While the WBF-011 group showed a possible trend towards enhanced insulin secretion, the difference was not statistically significant.
In summary, this double-blind, randomized, placebo-controlled study provides an initial demonstration of a novel 5-strain probiotic formulation, WBF-011, that significantly improved total glucose AUC0-180 min relative to placebo in subjects with T2D that are primarily on metformin monotherapy. Key secondary endpoints for glucose control also appeared to improve, including A1c. No changes were detected in body weight, HOMA-IR, or fasting glucose concentrations, suggesting that much of the effect is a reduction in plasma glucose concentration during the postprandial period. To our knowledge, this is the first randomized controlled trial to administer four of the five species to human subjects with T2D. These results justify future studies designed to confirm and expand on these observations.
References
Footnotes
FP and PM are joint first authors.
Contributors FP and JB participated in study design, statistical analysis, and manuscript preparation and review. PM participated in study design, study logistics, data analysis, and manuscript preparation and review. AC and AD participated in manufacture of study product. CC participated in study design and manuscript review. JE and MI participated in study design, study logistics, and manuscript review. JG participated in study logistics and fecal analyses. NJ oversaw the fecal analyses. WTL participated in data analysis. MN and ST participated in fecal analysis. MaSc oversaw manufacture of study product. MiSo participated in data analysis. BS participated in manufacture of study product. OK participated in study design, study conduct, data analysis, and manuscript preparation and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors are employees and stock/stock option shareholders of Pendulum Therapeutics, Inc (formerly known as ‘Whole Biome Inc.’). OK owns stock in GlySens, Inc, has stock options in ViaCyte, Inc, and is a consultant to NuSirt BioPharma, Circius, and NanoPrecision Medical.
Patient consent for publication Not required.
Ethical Approval This study was approved by the Allendale institutional Review Board (30 Neck Road, Old Lyme, CT, 06371) and informed consent was obtained from each subject prior to participation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data and reproducible examples of data analysis are made available at the following public git-tracked repository: https://github.com/wholebiome/NCT03893422.