Article Text

Abstract
Introduction We assessed the impact of a diabetic foot ulcer prevention program incorporating once-daily foot temperature monitoring on hospitalizations, emergency department and outpatient visits, and rates of diabetic foot ulcer recurrence and lower extremity amputations for patients with recently healed foot ulcers.
Research design and methods In this retrospective analysis of real-world data, we enrolled 80 participants with a healed diabetic foot ulcer in a year-long foot ulcer recurrence prevention program. Four outpatient centers within a large integrated healthcare system in the USA contributed to enrollment. We evaluated diabetic foot-related outcomes and associated resource utilization for participants during three periods: the 2 years before the program, the year during the program, and after the program ended. We reported unadjusted resource utilization rates during the program and the periods before and after it. We then adjusted rates of outcomes in each phase using an interrupted time series approach, explicitly controlling for overall trends in resource utilization and recurrence during the three periods.
Results Our unadjusted data showed high initial rates of resource utilization and recurrence before enrollment in the program, followed by lower rates during the program, and higher rates of resource utilization and similar rates of recurrence in the period following the end of the program. The adjusted data showed lower rates of hospitalizations (relative risk reduction (RRR)=0.52; number needed to treat (NNT)=3.4), lower extremity amputations (RRR=0.71; NNT=6.4), and outpatient visits (RRR=0.26; absolute risk reduction (ARR)=3.5) during the program. We also found lower rates of foot ulcer recurrence during the program in the adjusted data, particularly for wounds with infection or greater than superficial depth (RRR=0.91; NNT=4.4).
Conclusions We observed lower rates of healthcare resource utilization for high-risk participants during enrollment in a diabetic foot prevention program incorporating once-daily foot temperature monitoring.
Trial registration number NCT04345016.
- diabetic foot
- preventive medicine
- health care costs
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
One of the only evidence-based practices to prevent recurrence of diabetic foot ulcers is once-daily foot temperature monitoring, which is recommended by multiple clinical practice guidelines for those in diabetic foot remission.
What are the new findings?
We found lower rates of hospitalizations (relative risk reduction (RRR)=0.52; number needed to treat (NNT)=3.4), emergency department visits (RRR=0.40; NNT=5.1), and outpatient visits (RRR=0.26; absolute risk reduction (ARR)=3.5) during participation in a prevention program incorporating once-daily foot temperature monitoring. During participation in the program, we also found lower rates of lower extremity amputations (RRR=0.71; NNT=6.4) and foot ulcer recurrence, particularly for wounds with greater than superficial depth or with clinical signs of infection (RRR=0.91; NNT=4.4).
How might these results change the focus of research or clinical practice?
A diabetic foot prevention program incorporating foot temperature monitoring may result in lower rates of healthcare resource utilization and foot ulcer recurrence in high-risk patients.
Introduction
In addition to contributing considerable morbidity and mortality, diabetic foot complications are associated with staggering levels of resource utilization. In a recent analysis of 6.7 million cases, resource utilization in patients with ambulatory visits for diabetic foot complications was similar to or exceeded utilization in those with ambulatory visits for cancer, cerebrovascular disease, and congestive heart failure.1 The OR for hospitalization or emergency department (ED) referral for a diabetic foot infection was 6.7, nearly double the odds for any other condition reported. These results are consistent with other literature suggesting that the severity of diabetic foot ulcers (DFU), for which infection is a key marker, is an important determinant of resource utilization.2–10
Fortunately, preventive care can reduce the incidence of diabetic foot complications. Data from a study in 1640 participants concluded that adherence to recommended practices reduced DFU incidence by 50% over an 18-year period.11 However, the investigators also reported that recurrence rates remained unchanged despite improved preventive foot care, suggesting a more aggressive preventive approach is needed for patients who have healed from a DFU.
One of the only evidence-based practices shown to prevent DFU recurrence is once-daily foot temperature monitoring, which is recommended by multiple clinical practice guidelines for high-risk patients, including those with history of DFU.12–15 Randomized controlled trials found reductions in recurrence as large as 71% using foot temperature monitoring to identify inflammation prior to ulceration and prompt non-invasive interventions to offload pressure to the affected area.16 17 However, despite abundant evidence supporting its use, data are lacking on practical implementations of foot temperature monitoring programs and their real-world impact on outcomes such as resource utilization.
In this retrospective analysis of real-world data, we reported on trends in resource utilization and DFU recurrence before, during, and after participation in a recurrence prevention program incorporating once-daily foot temperature monitoring.
Research design and methods
Study design
Our study had a pragmatic design. We retrospectively analyzed data from medical claims and electronic health records (EHRs) reflecting real-world practice to assess trends in resource utilization and DFU recurrence in 80 patients participating in a prevention program.
We evaluated outcomes for each participant during three distinct periods: the 2 years before participation in the prevention program, the 1 year during participation, and after the program ended. Participants were enrolled in the program between April 2017 and October 2018. Data were extracted and analyzed between January 2020 and June 2020.
The study was conducted across four outpatient centers within a large integrated healthcare system in a geographically concentrated region in the eastern USA. Eligible participants were enrolled in the prevention program until successful completion at 1 year or until dropping out of the study, disenrolling as a beneficiary of the health plan cosponsor, or dying.
All participants gave informed consent prior to participation in the study and consented to data access for retrospective analysis. The study was registered after completion with ClinicalTrials.gov.
Nomenclature
We have adopted definitions consistent with those from the International Working Group on the Diabetic Foot.18 We defined ‘foot ulcer’ as a full thickness loss of epidermis and dermis or involvement of deeper structures. A foot ulcer ‘healed’ with complete epithelialization of the wound absent drainage. To assess DFU severity, we used the University of Texas Classification System.8 We define a ‘partial foot amputation’ as an amputation more distal than the ankle.
We designated all wounds with University of Texas classification greater than UT-1A as ‘moderate and severe.’ Oyibo and colleagues9 have previously reported that only 9% of UT-1A DFU are unhealed and only 3% required amputation during the first 6 months. For comparison, DFU with greater severity were unhealed or required amputation at rates of approximately 20% and 30%, respectively.
Enrollment criteria
Inclusion criteria required diagnosis of diabetes mellitus (type 1 or 2); history of DFU or amputation that had healed within the 24 months before enrollment; presence of palpable bilateral posterior tibial and dorsalis pedis pulses or ankle brachial index exceeding 0.5 documented within the 12 months preceding study enrollment; and ability to provide informed consent. Patients were excluded from participation for baseline inflammatory foot conditions, including unhealed DFU, active Charcot arthropathy, and prevalent foot infection or cellulitis. Additionally, patients were excluded if they had history of lower extremity amputation (LEA) more proximal than transmetatarsal; were unable to walk without the assistance of a wheelchair, walker, or crutches; or had travel plans expected to interrupt participation longer than two consecutive weeks. Finally, patients were ineligible to participate for any condition which, in the investigator’s judgment, rendered the patient unsuitable or unreliable.
Study program
The study program included in-home once-daily foot temperature monitoring, care management to support participants in engagement with the program, and periodic podiatric exams prompted by abnormal foot temperature readings. The foot temperature monitoring device, shown in figure 1, was a daily-use telemedicine foot temperature monitoring mat (Podimetrics SmartMat; Podimetrics Inc; Somerville, Massachusetts, USA). It is marketed in the USA as an FDA 510(k)-cleared medical device for the ‘periodic evaluation of the temperature over the soles of the feet for signs of inflammation’.19

The study device was a telemedicine once-daily foot temperature monitoring mat.
After giving informed consent, study participants received the device and were trained in its proper use. The participants completed the first scan in clinic, with subsequent daily scans unsupervised in the home. All participants received standard medical care, including preventive foot care and foot temperature monitoring, based on recommendations from the American Diabetes Association and the International Working Group on the Diabetic Foot.14 20
The study device includes software that automatically monitors patients for foot inflammation, indicated by differences in temperature exceeding 2.2°C over two consecutive uses between any of six contralaterally matched locations on the plantar surfaces of the feet: the hallux, first, third, and fifth metatarsal heads, midfoot, and heel. For patients missing one or more of these locations due to partial LEA, a spot on the plantar surface most proximal to the missing anatomy was used. Accuracy of this approach using the study device previously has been reported to predict 97% of non-acute plantar DFU in patients in diabetic foot remission,21 and a recent study found no difference in accuracy for those with partial foot amputations.22 The mat form factor of the study device accommodates patients with foot deformity and partial-foot amputations.
Once inflammation was identified, a trained health plan nurse called the participant. The EHR was configured to prompt the nurse to ask the participant if a spouse, child, or other caregiver can inspect the feet; if no one was available to assist, the participant was asked to complete a self-exam. The participant was asked if he or she had recently experienced any acute signs of infection, had been wearing appropriate footwear, had recently changed footwear, had recently changed activity level, or had any other health-related complaints. The participant was instructed to increase diligence and frequency of routine foot checks, reminded of acute signs of infection, and scheduled for a podiatry appointment.
Although treatment plans for care prompted by the study device were at the discretion of the provider, the EHR system recommended the following actions: trim toenails, debride calluses, and aspirate or deroof blisters; inspect and replace footwear, as needed; adjust accommodative insoles to offload the inflamed area; instruct the participant to continue to use the study device, unless developing a wound; and document and treat any DFU per standard diabetic foot care.
Participants were also monitored for non-adherence to daily use of the study device. A participant was deemed non-adherent after four consecutive days without using the study device in accordance with previously studied adherence protocols.21 23 Non-adherence prompted telephonic outreach by a study nurse affiliated with the health plan for re-engagement. During these calls, the nurse was prompted by the EHR to remind the participant of the importance of daily use of the study device to identify foot inflammation that can lead to diabetic foot complications; to continue completing daily foot self-exams; to always use diabetic shoes or other prescribed footwear, even indoors; and to immediately notify the clinic if they notice any concerning changes to their feet.
Participants were instructed to discontinue use of the mat in certain circumstances, including incidence of new DFU, new infection, Charcot arthropathy flare, or when using an offloading device, such as a total contact cast or removable cast walker, that would prevent the participant from using the study device.
Employees of the device manufacturer were not involved in participant care or assessment or documentation of outcomes.
Measurements
We extracted data from the EHR and medical claims databases maintained by the health plan cosponsoring the study. Employees of the device manufacturer were not involved in extracting any data reported or analyzed.
We identified prevalent DFU using diagnosis codes, including standard International Classification of Diseases (ICD) codes and internal designations in the EHR, associated with each participant’s podiatry outpatient visits. We subsequently estimated incidence of DFU, delimited by dates of occurrence and subsequent healing, by grouping contiguous outpatient podiatry visits with prevalent DFU. We reviewed documentation of DFU episodes in the EHR to grade DFU severity.
Details related to hospitalizations for each participant, including Medicare-Severity Diagnosis Related Group (MS-DRG) and length of stay, were summarized from hospital claims. We reported the number of admissions by DRG in the periods before, during, and after participation in the study program for those MS-DRG with more than one occurrence. Remaining admissions were categorized as ‘Other’.
Similarly, we summarized ED visits from claims data and identified LEA by procedure codes. Details related to outpatient visits were also extracted from the EHR.
Analysis approach
Outcomes of interest were rates of resource utilization (including hospitalizations, ED visits, and outpatient visits), DFU recurrence, and LEA. We included in our analysis all outcomes from available data, including from those participants who were non-adherent with use of the study device, became lost-to-follow up during the program, or dropped out of the study program.
To calculate rates for outcomes of interest, we normalized raw counts by the total exposure duration in each period of the study. We modeled aggregate rates for outcomes using an interrupted time series approach, assuming that event counts in each period were generated by a homogeneous Poisson point process. We adjusted for the overall trend over the three periods by including an additive term representing an Poisson point process with linearly varying rate. Such trends may exist due to participant aging or disease progression or regression. We solved for four unknowns (uniform rates during the three periods and slope of the linearly varying rate over the three periods) by maximizing the sum of the likelihood of the Poisson processes over the observed counts expressed at daily intervals.
Because many pre–post studies are biased from inclusion criteria requiring participants to have the outcome-of-interest in the pre-period or before period, we analyzed the subset of participants who developed a DFU during the program. By applying the same inclusion criteria to the period during enrollment in the study program that was applied before enrollment, we attempted to eliminate a potential temporal confounder and isolate the impact of the study program on the outcomes.
These analyses were performed primarily by an author affiliated with the device manufacturer. All analyses and results were available to and reviewed in their entirety by authors from the health plan cosponsor. A confirmatory pre–post analysis was completed by an author of the health plan cosponsor to ensure replicability of the main findings. The confirmatory analysis considered outcomes in the year before enrollment in the foot temperature monitoring program and compared these with rates in the year during the program using repeated-measurement Poisson regression with log-link.
Participant adherence was measured by the average uses-per-week during the foot temperature monitoring program. Consistent with previous research, a threshold of three uses/week over the study period was used to define engagement.21
Results
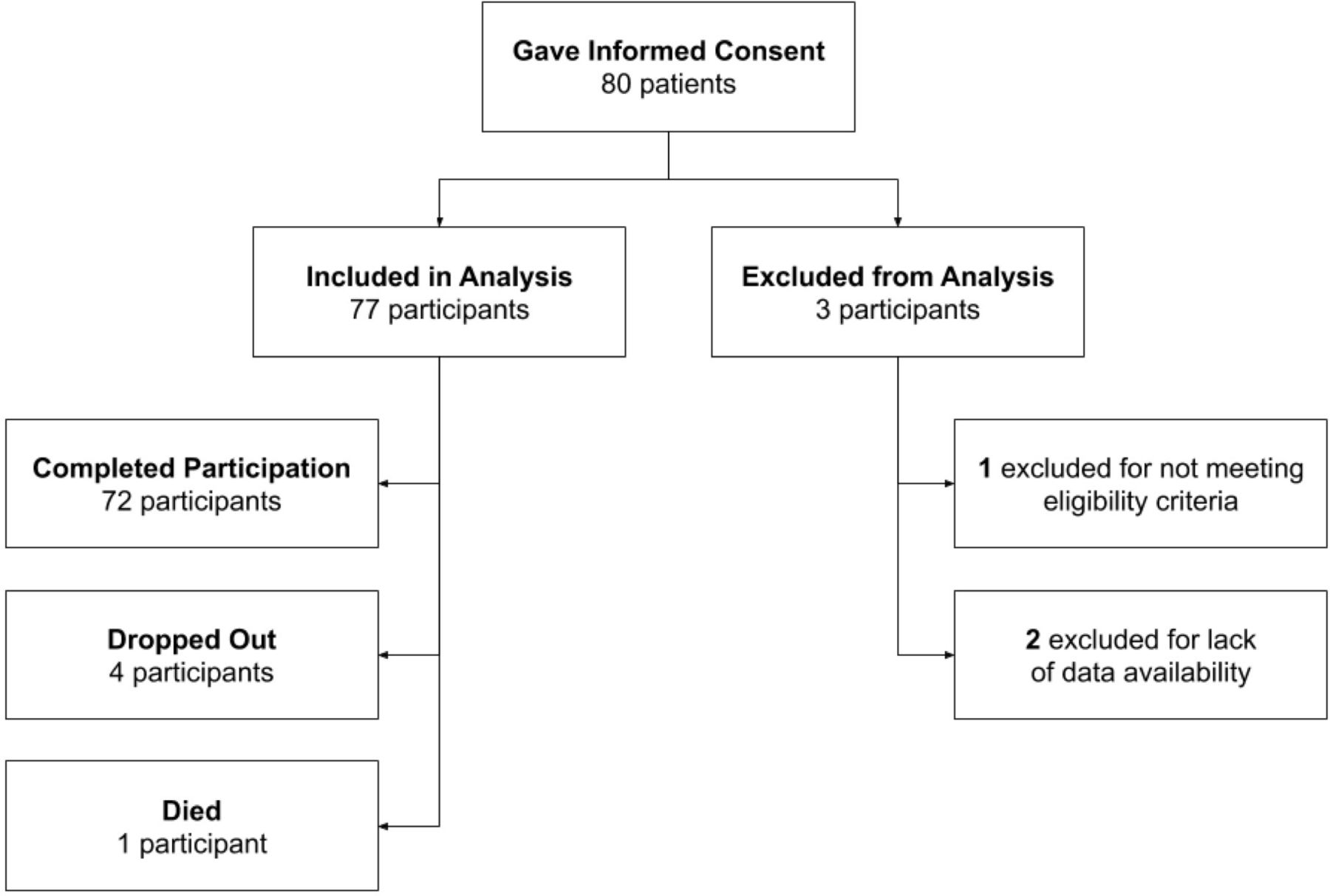
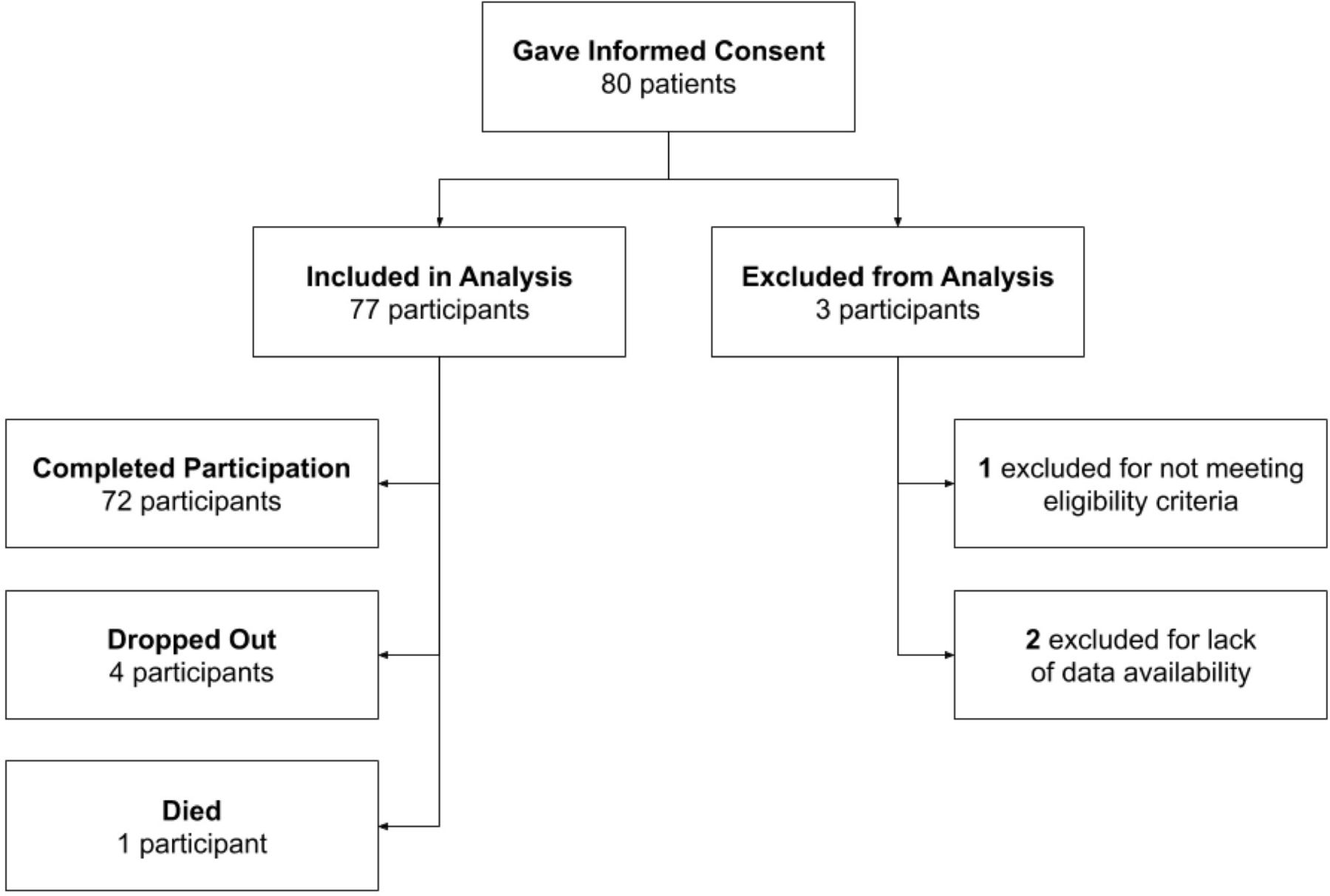
A total of 80 participants consented to participate in the program. Of these, one was excluded from the analysis after a chart review completed shortly after enrollment revealed the participant did not meet eligibility criteria. Two further participants were excluded post hoc due to technical limitations encountered by the health plan while extracting data from the sources described in the Measurements section. Thus, a total of 77 participants contributed data to the analysis. During the program, four participants dropped out before concluding 1 year of follow-up, and one participant died. These endpoints are summarized in figure 2. Table 1 summarizes the demographics of these participants.
Participant demographics entering foot temperature monitoring program
{kind=link}
{kind=link}
Flow diagram summarizing participant endpoints during participation in the foot temperature monitoring program.
Unadjusted results before, during, and after participation in a diabetic foot ulcer prevention program
Table 2 shows unadjusted rates of DFU and healthcare utilization before, during, and after the study program. The rate of hospitalizations during participation in the study program was lower than the rates before and after the program by approximately 50%. Admissions for diabetes and metabolic disorders, peripheral nervous system disorders and procedures, and heart failure were observed at higher rates in the before and after periods than during the program. Rates of admissions for wound care and amputation were disproportionately higher in the before period than during the program. Length of inpatient stay was similar over the three periods, with an average of 5.5 hospital days per admission.
Unadjusted rates of DFU with classification greater than UT-1A were also lower during the program than before. All DFU during the program were of superficial depth (UT-1), whereas nearly 15% of DFU before enrollment penetrated more deeply. More than 95% of DFU during the program were absent infection. Two of the three wounds with severity worse than UT-1A that occurred during this study were to non-adherent participants, and the third was associated with inflammation identified by the study device but which presented weeks after the exam prompted by the inflammation.
Table 3 summarizes the rates of incidence and resource utilization adjusted for trends over the three study periods using the interrupted time series analysis. Relative to the unadjusted results, we found slightly lower reductions during the program for rates of LEA (relative risk reduction (RRR)=0.71) and larger reductions of moderate and severe foot ulcers (RRR=0.91) and all foot ulcers (RRR=0.46).
Incidence and resource utilization rates adjusted for trends
Participants used the study device 4.1±1.6 times per week on average. Inclusive of those who dropped out, became lost to follow-up, or died, 47 participants (47/77=61.0%) had adherence averaging greater than 3 days per week during the year-long program. There were 5.1±4.6 re-engagement calls per participant-year. Of the 77 participants, 74 (96.1%) required at least one re-engagement call, and 58 (75.3%) required more than one call. Approximately 10% of participants required an average of one re-engagement call per month. The average duration between calls for those participants who received more than one was 39±42 days.
We observed 1.6±1.6 inflammation calls per participant-year prompting podiatry outpatient visits resulting from inflammation identified by the study device. Of the 77 participants, 47 (61.0%) required at least one phone call and outpatient visit prompted by the study device, and 32 (27.1%) required more than one outpatient visit.
No device-related adverse events were reported by participants or noted by investigators during the study.
In a subgroup analysis of the 35 participants who developed a DFU during the program, we found the observed lower rate of hospitalizations persisted, although with a smaller absolute reduction (absolute risk reduction (ARR)=0.19 admissions/participant-year in the subgroup). In this subgroup, there were 4.0 and 1.8 re-engagement and inflammation calls per participant-year, respectively. The adherence in this subgroup was 4.3±1.6 uses per week on average.
A confirmatory pre–post analysis was completed, the results of which agreed well with the unadjusted raw data as well as the adjusted results from the interrupted time series analysis. We found lower rates in DFU recurrence (RRR=0.37), hospitalizations (RRR=0.54), LEA (RRR=0.80), and ED visits (RRR=0.43) in the pre–post analysis.
Conclusions
While previous studies have reported the accuracy of once-daily foot temperature monitoring,21 22 24 its effectiveness for preventing DFU recurrence,16 25 and successful real-world applications,23 26–28 our study is the first to report its impact on resource utilization. We observed lower rates of hospitalizations, ED visits, outpatient visits, DFU recurrence, and LEA during enrollment in a DFU recurrence prevention program incorporating foot temperature monitoring.
We found 91% fewer moderate and severe DFU during the program, potentially due to early identification of DFU prompting timely communication with and treatment by healthcare providers. Previous studies have shown DFU outcomes are dependent on timeliness of treatment and DFU severity at presentation.2–10 Unfortunately, many patients at risk for DFU have peripheral neuropathy, diabetic retinopathy,29 and impaired lower joint mobility, which may prevent them from adequately completing daily foot inspections.30 These factors, which were highly prevalent in our study, can delay identification and treatment of DFU.
Our most important finding was that hospitalization rates were approximately 50% lower during the study program than before or after it. The observed trends in hospitalizations may be partially due to lower rates of moderate and severe DFU during the study program. Data from a large international study in Europe suggested that 22% of patients with the lowest severity were hospitalized at least once before healing, amputation, or death, whereas 69% of patients with the most severe DFU were hospitalized.31 These statistics, combined with our results, suggest that approximately 0.13 admissions per participant-year prior to the program may have been associated with moderate and severe DFU. Given the 91% reduction in rates of moderate and severe DFU observed during the program, it is possible that as much as half of the observed lower hospitalization rate during the program (ARR=0.29/year) was due to fewer moderate and severe DFU occurring. We do note, however, that this trend was not observed in raw amputation rates, which increased only modestly in the after period. This may be explained by insufficient follow-up during the after period.
While traditionally viewed as a marker of comorbid disease, there is mounting evidence that foot ulceration is independently associated with poor health outcomes, most notably all-cause mortality. In a recent meta-analysis, Saluja and colleagues32 considered data from 11 studies that reported 84 000 all-cause deaths. They found that foot ulcers were associated with an increased risk for mortality (pooled RR=2.45), especially due to myocardial infarction and stroke. Brownrigg and colleagues33 observed similar findings, and hypothesized several explanations. In the short-term, the authors suggested that DFU may increase susceptibility to infection, sepsis, and multiorgan failure. In the long-term, the intermittent inflammatory cascade with each DFU recurrence may trigger poor cardiovascular outcomes. Consistent with these hypotheses, we observed higher rates of aggregate hospitalizations for heart failure, septicemia, and infectious diseases before and after the program.
Several other factors could have explained the broad impact on resource utilization we have observed. Participants received an average of 5.1 additional telephone interactions with a study nurse at the beginning of non-adherence. The nurse was prompted to ask the participant about the participant’s health and encourage the patient in foot-related preventive practices. Additionally, participation in the program resulted in an additional 1.6 additional podiatry outpatient visits per participant-year and nearly one additional secure message. These additional healthcare interactions, and encouragement to establish a daily routine around preventive foot care by use of the study device, may have resulted in improved self-care for the foot conditions and more broadly. The additional interactions may also have prompted the participants to seek care for foot-related and other conditions earlier than they otherwise would have. The observer effect may also have contributed to the broad impact we observed.
Of note, we observed a smaller reduction in DFU (RRR=0.46) than had been observed by other investigators.16 25 34 However, incidence among this population in the before period was also quite high relative to that observed in other studies, with the ARR=0.52 comparable with the baseline rate of recurrence reported by Frykberg and colleagues.21
We acknowledge several limitations of our work, foremost being that we did not prospectively enroll or retrospectively identify a control group for comparison. Instead, we treated each participant as his or her own control, reporting unadjusted and adjusted rates of outcomes and resource utilization in the periods before, during, and after the participating in the program. We believe this approach is appropriate to our aims for two reasons. First, our interrupted time series approach mitigates many of the limitations of traditional pre–post study designs by including a period after the prevention program ended. The second reason is that several predisposing risk factors for DFU recurrence are not easily assessed using administrative data, which was all that was available to us due to the retrospective nature of this study. The type of pragmatic design and analysis approach we have adopted is not uncommon among studies retrospectively analyzing healthcare claims. Maeng and colleagues,35 for example, analyzed data from a congestive heart failure program within the Geisinger Health System using an interrupted time series approach similar to ours.
An additional limitation is that we excluded patients with amputations more proximal than transmetatarsal amputation and patients being treated for wounds. These patients, who have only one foot to monitor, are at elevated risk for developing diabetic foot complications and could potentially benefit from a program similar to the one we implemented.36 When our study was initiated, there was no evidence-based approach for monitoring a single foot for inflammation. However, in 2019, Lavery and colleagues24 presented an approach with a daily-use telemedicine foot temperature monitoring mat that detected 91% of non-acute plantar foot ulcers 41 days before clinical presentation by comparing temperatures between ipsilaterally matched locations on the foot.
There were also limitations related to the study protocol. Participants were only called at the beginning of non-adherence, whereas best practices with a more comprehensive care management program can achieve 75% engagement at the end of a year.23 Additionally, when inflammation was identified by the study device, participants were required to be seen for an exam immediately. However, the study device has been shown to identify inflammation 35 days before clinical presentation.21 A more comprehensive care management approach for triaging inflammation has proven effective in veterans.23 By following patients telephonically for changes in the feet or signs or symptoms of skin breakdown, these investigators found that 68% of all cases with inflammation resolved via offloading alone without an outpatient visit, and 76% of those cases that did ultimately result in an exam required clinically meaningful preventive care.
Future research should study these best practices for coupling care management and foot temperature monitoring in a prevention program. These studies should also include patients with amputations more proximal than transmetatarsal. Additionally, a study with an explicit control coupled with an explanatory as opposed to pragmatic study design could enable researchers to attribute findings to particular components of the study program, which we were unable to do in the present effort. Comparing against a control may have further supported a causal relationship between enrollment in the study program and broad reductions in resource utilization.
A large study in a more geographically diverse area would also improve the generalizability of our results. For example, more than 60% of our cohort is black, and while data from Skrepnek and colleagues1 suggest similar propensity to ulcerate and use resources for DFU or diabetic foot infection, these demographics are not reflective of the USA more broadly. Finally, a proper economic analysis, including cost–benefit assessment, of our data or future data is also warranted.
Our results suggest that enrollment in a foot ulcer recurrence prevention program coincided with decreases in rates of hospitalizations, ED visits, outpatient visits, DFU recurrence, and LEA. Use of similar programs in high-risk populations may help dramatically decrease morbidity, mortality, and healthcare costs.
Acknowledgments
The authors would like to acknowledge the nurses and clinical staff from the Podiatric Surgery Departments of Kaiser Permanente Mid-Atlantic States for their contributions to patient enrollment, outreach, and engagement throughout the study.
References
Footnotes
Contributors ALI: study concept and design, clinical supervision, patient care, patient recruitment, acquisition of data, interpretation of results, and preparation of the manuscript. TDS: clinical supervision, patient care, patient recruitment, and acquisition of data. MLM and DJS: clinical supervision, patient care and patient recruitment. EAW and JLC: clinical supervision, patient care, and patient recruitment. ESW and HH: acquisition of data, analysis of data, interpretation of results, and preparation of the manuscript. BJP and DRL: study concept and design, analysis of data, interpretation of results, and preparation of the manuscript. JDB: study concept and design, and preparation of the manuscript. NJN: study concept and design, acquisition of data, and preparation of the manuscript. SJS: preparation of the manuscript. JLL: study concept and design. MAH: study concept and design and preparation of the manuscript.
Funding The resources for clinical management of this study were provided by Kaiser Permanente Mid-Atlantic States. Podimetrics Inc provided the study devices and funding to support the data analysis.
Competing interests JDB, BJP, DRL, SJS, and NJN are employees and shareholders of Podimetrics Inc, which manufactures the study device. All other authors report no real or potential conflicts of interest.
Patient consent for publication Obtained.
Ethics approval The study was reviewed by and obtained ethics approval from the Kaiser Permanente Mid-Atlantic States Institutional Review Board (MA-16–134).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request to the corresponding author for research purposes only contingent upon approval by Kaiser Permanente Mid-Atlantic Permanente Research Institute.