Article Text

Abstract
Introduction Sitagliptin is a dipeptidyl peptidase 4 inhibitor for the treatment of type 2 diabetes (T2D). Limited real-world data on its effectiveness and safety are available from an Italian population.
Research design and methods We evaluated long-term clinical data from the single-arm PERsistent Sitagliptin Treatment & Outcomes (PERS&O) study, which collected information on 440 patients with TD2 (275 men, 165 women; mean age 64.1 years; disease median duration: 12 years) treated with sitagliptin ‘add-on’. For each patient, we estimated the 10-year cardiovascular (CV) risk using the UK Prospective Diabetes Study (UKPDS) Risk Engine (RE). Drug survival was evaluated using Kaplan-Meier survival curves; repeated measures mixed effects models were used to evaluate the evolution of glycated hemoglobin (HbA1c) and CV risk during sitagliptin treatment.
Results At baseline, most patients were overweight or obese (median body mass index (BMI) (kg/m2) 30.2); median HbA1c was 8.4%; median fasting plasma glucose: 172 mg/dL; median UKPDS RE score: 24.8%, being higher in men (median 30.2%) than in women (median 17.0%) as expected. Median follow-up from starting sitagliptin treatment was 5.6 years. From Kaplan-Meier curves, the estimated median drug survival was 32.8 months when considering discontinuation for any cause and 58.4 months when considering discontinuation for loss of efficacy. A significant improvement in HbA1c was evident during treatment with sitagliptin (p<0.01): the reduction was rapid (median HbA1c after 4–6 months: 7.5%) and continued at longer follow-up. When comparing patients treated with sitagliptin versus those stopping sitagliptin and switching to another antihyperglycemic drug, we detected a significant difference in the evolution of HbA1c in favor of patients who continued sitagliptin treatment. The UKPDS RE score at 10 years and the BMI significantly improved during treatment with sitagliptin (p<0.001). Adverse events were relatively uncommon.
Conclusion Patients with T2D treated with sitagliptin achieved an improvement in metabolic control and a reduction in CV risk and did not experience relevant adverse events.
- dipeptidyl peptidase 4
- drug-related side effects and adverse reactions
- risk assessment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Sitagliptin is an orally active dipeptidyl peptidase 4 inhibitor for the treatment of type 2 diabetes (T2D), commercially available in Italy since 2008, which improves glycemic control in patients with TD2 and does not increase the risk of cardiovascular (CV) diseases.
What are the new findings?
Estimated median sitagliptin survival was 32.8 months when considering discontinuation for any cause, and 58.4 months when considering discontinuation due to loss of efficacy.
A significant reduction in glycated hemoglobin was evident during treatment with sitagliptin; the UK Prospective Diabetes Study Risk Engine score at 10 years and body mass index significantly improved over time. No major side effects were registered.
How might these results change the focus of research or clinical practice?
The PERsistent Sitagliptin Treatment & Outcomes project (a real-world single-arm retrospective observational study) confirms that patients with T2D treated with sitagliptin achieve an improvement in metabolic control, obtain a reduction in CV risk and do not experience relevant adverse events.
Introduction
The PERsistent Sitagliptin treatment & Outcomes (PERS&O) study1 was a ‘real-world’ retrospective, observational, single-center study performed in a general hospital in Northern Italy in order
To validate the UK Prospective Diabetes Study (UKPDS) Risk Engine (RE) in a cohort of Italian participants with type 2 diabetes (T2D) without prespecified diabetes duration, with/without cardiovascular (CV) disease, treated with sitagliptin. UKPDS RE2 3 was selected because it provides the best risks estimates available for people with T2D.4 As suggested by the NICE 20095 guideline, it should be assessed annually if the person is considered not to be at high CV risk. It is to be underlined that this guidance has been updated and replaced by NICE guideline NG28.5
To confirm CV risk gender difference.
To evaluate the effect on metabolic control and CV risk evolution obtained by ‘add-on’ persistent sitagliptin treatment.
In short, sitagliptin, a DiPeptidyl Peptidase 4 inhibitor (DPP4-i), available in Italy since 2008, was taken by 462 participants with T2D up to 31 December 2015: 170 of them (men: 106, age: 63.6±8.8, T2D duration: 11.58±7.33; women: 64, age: 65.6±7.95, T2D duration 13.5±7.9) were treated for 48 months with the same dosage (100 mg once a day). The evaluation of CV risk evolution by gender confirmed the expected statistical difference (p<0.0001) between women and men suffering from T2D. Sitagliptin obtained significant results after 12 months, and at the end of the observation, both on metabolic control (expressed by glycated hemoglobin (HbA1c)) and on UKPDS RE. Analysis of variance test revealed a significant effect on CV risk after 12 months (p=0.003) and after 48 months (p=0.04). We concluded suggesting that these real-world data obtained applying UKPDS RE may reflect patients’ and clinicians’ interest in realizing individual CV risk, and its evolution.
The main aim of this actual project was to update, on the basis of a longer investigation period, our findings previously published on a medium-term to long-term follow-up. Our interest is the evaluation of the impact of sitagliptin-persistent treatment on metabolic control, as well as on the evolution of CV risk. We have also described persistence with sitagliptin (drug survival) and reasons for sitagliptin discontinuation.
Materials and methods
Since 2008, when sitagliptin initially entered in the market in Italy, 462 outpatients suffering from T2D with HbA1c>7.5% (58mmol/mol) despite the usual antihyperglycemic treatment being prescribed the drug at the ASST Bergamo Ovest, in Treviglio (Bg), Italy. Anthropometric factors, clinical variables and history of selected conditions were recorded at sitagliptin add-on (baseline) and were available for 440 subjects (excluding patients who never took the prescribed medication): 275 men and 165 women, with a mean age of 64.1 years (SD 9.2) and estimated glomerular filtration rate (eGFR) of >60 mL/min when starting sitagliptin treatment. All patients were managed by endocrinologists of our hospital team, performing visits every 6 months (earlier if complications occurred). Data on several factors during follow-up, including body weight, fasting plasma glucose, HbA1c, systolic and diastolic blood pressures, lipid profile, any change in the antihyperglycemic plan, together with the reason for stopping sitagliptin (inefficacy, adverse events or other reasons) and adverse events, were retrospectively collected by consulting our local Health Electronic Recording system (Smart Digital Clinic, METEDA, Italy). Using available data, the 10-year UKPDS RE score was calculated for each patient at baseline and at various follow-ups.2 6 When, at a specific follow-up time point, some measurements necessary for score calculation were missing for a patient, these were replaced by the nearest patient value in a 12-month period, before score calculation. Such missing imputation was performed only if the patients had no more than two missing measurements at that follow-up time; otherwise, the score was considered as missing.
Statistical methods
We analyzed data from the PERS&O database that includes information of 440 patients with T2D treated with sitagliptin, of whom 84 are still under treatment (n=79 for ≥72 months). Continuous variables were presented as mean values (SD) or medians (IQRs), and categorical variables as numbers and percentages. Drug survival was defined as the time patients remained under treatment with sitagliptin and was evaluated using Kaplan-Meier survival curves. Discontinuation of treatment because of any cause (eg, lack of efficacy, adverse events and other reasons) and because of lack of efficacy was considered as an endpoint. Time trends in HbA1c, 10-year UKPDS RE, body mass index (BMI), systolic blood pressure and lipids during sitagliptin treatment were evaluated through repeated measures mixed effects models. If necessary, variables were transformed to improve normality before model fitting. We also evaluated differences in overall time trends of HbA1c, 10-year UKPDS RE and BMI between patients under sitagliptin treatment and patients treated with other antidiabetic drugs after discontinuing sitagliptin. In this analysis, patients stopping sitagliptin and switching to another antidiabetic drug at variable time points during the observation period were considered as the comparison group. For this purpose, we used repeated measures mixed effects models adjusted for age, sex and diabetes duration. Sitagliptin treatment was entered in the models as a time-dependent dichotomous factor to account for switching from sitagliptin to another antidiabetic drug. We also tested whether HbA1c, UKPDS RE and BMI were different between patients under sitagliptin treatment and patients having switched to other antihyperglycemic agents at specific follow-up times by fitting separate linear regression models (one at each follow-up time point) with the factor under consideration as the dependent variable and a dichotomous variable for sitagliptin treatment as the independent one; models were adjusted for age, sex and diabetes duration. Data analyses were conducted using SAS V.9.4 statistical software.
Results
The analyzed population included 440 subjects with T2D subjects receiving sitagliptin. The median duration of T2D at sitagliptin add-on was 12 years (IQR 8–16 (if not other indication, IQR is now reported)) (table 1).
Baseline demographic and clinical data of patients with type 2 diabetes on sitagliptin treatment.
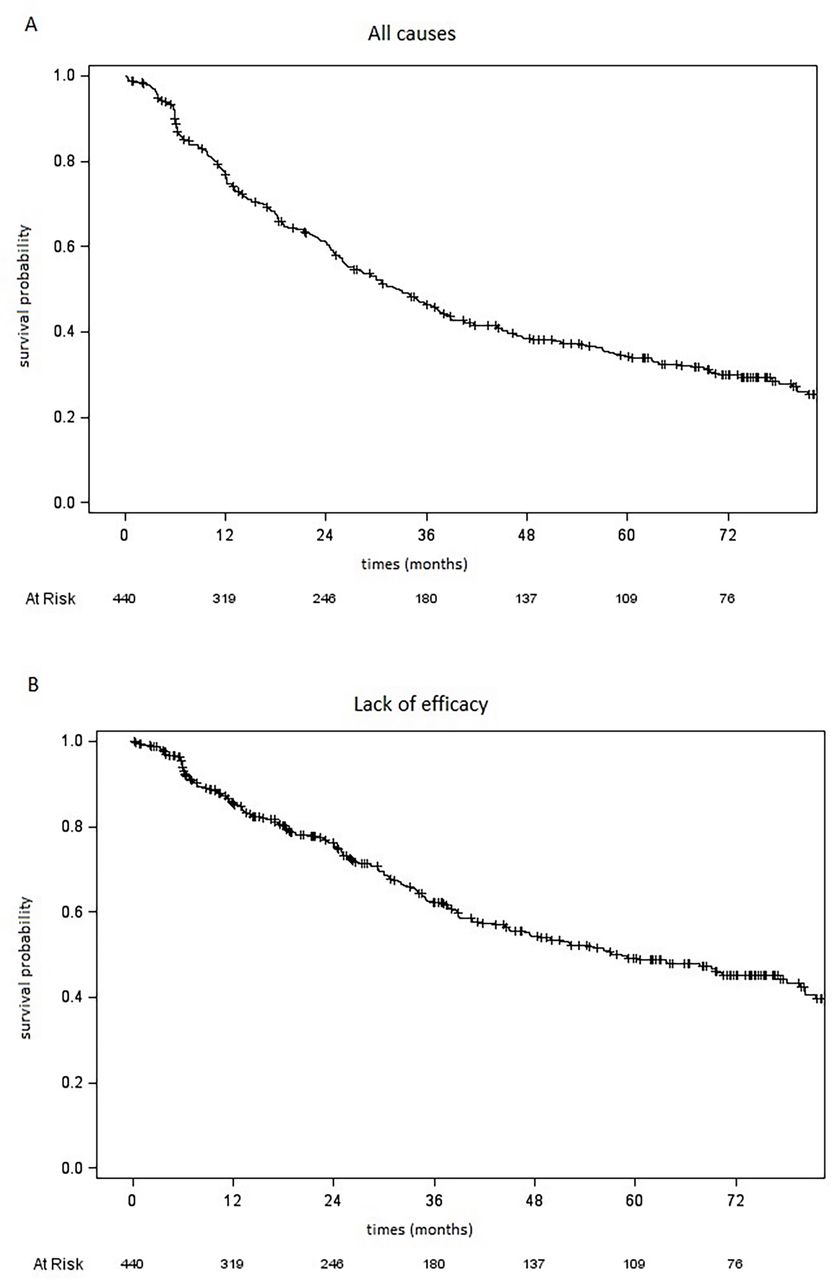
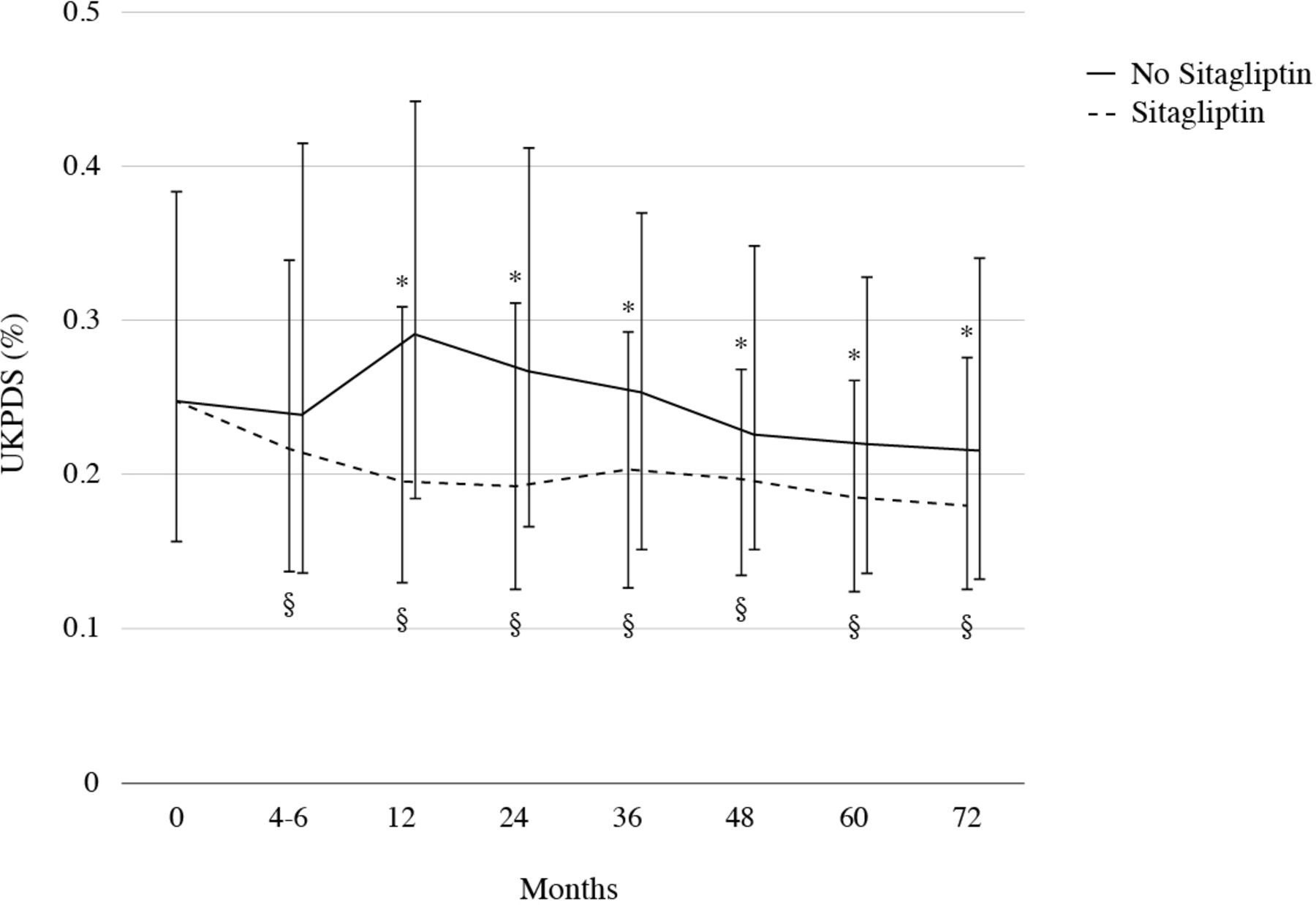
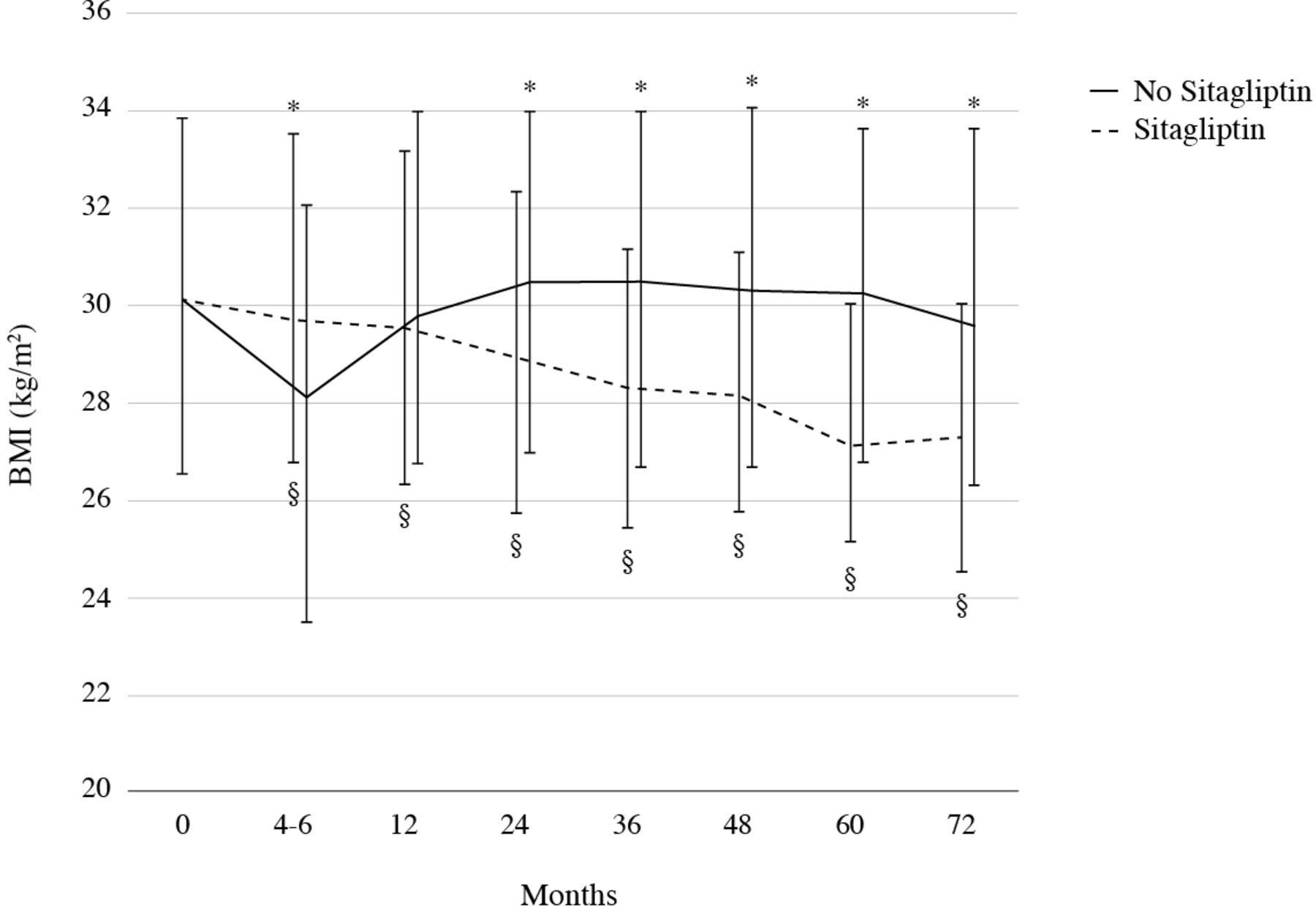
Among them, 278 (63.2%) never smoked. They were overweight or obese, with a median BMI of 30.2 kg/m2 (26.6–33.9). Their diabetes was not well balanced at baseline: median HbA1c and fasting plasma glucose were, respectively, 8.4% (7.9–9.0) and 172 mg/dL (153–200). Blood pressure was quite controlled, with median values of 140 mm Hg (125.5–15.0) for systolic blood pressure and 80 mm Hg (70–80) for diastolic blood pressure. Lipids were slightly increased (medians were 192 mg/dL (164–218) for total cholesterol, 46 mg/dL (39–54) for high-density lipoprotein cholesterol, 110.8 mg/dL (82.2–132.4) for low-density lipoprotein cholesterol, and 136 mg/dL (106–187) for triglycerides). The median baseline 10-year UKPDS RE score was 24.8% (15.6–38.3); as expected, the score was higher in men (median 30.2% (21.3–43.5)) than in women (median 17.0% (11.1–25.3)). Clinical history revealed the presence of previous coronary heart disease (CHD) in 63 subjects (14.3%), with history of heart failure (HF, one or more hospitalization) in 23 patients (5.2%), evidence of carotid plaque (detected by means of ultrasonography) in 57 patients (13%) and previous non-fatal stroke in 6 patients (1.4%). Patients’ antihyperglycemic plans at baseline are described in online supplementary table 1. Patients were mainly prescribed sitagliptin plus metformin (30.7%) or sitagliptin plus metformin and sulphonylurea (SU) (35.9%). The median observation time considering the overall cohort of patients, including those who stopped sitagliptin during the follow-up period at variable time points, was 6.2 years (q1–q3: 4.4–7.4), which can be considered a medium–long follow-up time. Information on follow-up from starting sitagliptin treatment is available in online supplementary table 2. Of the whole cohort of 440 subjects, about 19% are still on sitagliptin treatment (n=84), with a median duration of 75 months (68–87), while more than 67% (n=296) suspended the treatment because of lack of efficacy during time (n=188, 63.5%), therapy not being renewable for administrative reasons (n=47, 15.9%) or other reasons (n=33, 11.2%). DPP4-is and Glucagon-Like Peptide 1-Receptor Agonists (GLP1-RAs) were first marketed in Italy in 2008, while Sodium-GLucose co-Transporter 2-inhibitors (SGLT2-i) appeared later (2015). Among individuals who discontinued sitagliptin, GLP1-RAs were prescribed in 45 patients, while an SGLT2-i was taken by 58 subjects (including 6 patients who received both classes of drugs during the follow-up). Two hundred forty-nine patients (56.5%) were treated with sitagliptin for ≥24 months, 183 (41.6%) for ≥36 months, 139 (31.6%) for ≥48 months, 112 (25.5%) for ≥60 months and 79 (18%) for ≥72 months (online supplementary table 3). Sixty patients were lost to follow-up or died after a median treatment duration of 28 months (7–42). Online supplementary table 4 shows the baseline characteristics of patients according to sitagliptin treatment duration. Patients who were treated with sitagliptin for ≥48 months were quite similar in term of baseline cardiometabolic factors to those treated for shorter periods. Kaplan-Meier survival curves for time to sitagliptin discontinuation due to any cause (figure 1A) and lack of efficacy (figure 1B) are shown in figure 1. Estimated median drug survival was 32.8 months (95% CI 27.3 to 37.3) when considering discontinuation for any cause and 58.4 months (95% CI 45.1 to 78.1) when considering discontinuation due to lack of efficacy. We observed a significant improvement in HbA1c (median 8.4%, 68 mmol/mol at baseline) during treatment with sitagliptin (*p<0.001): the reduction was quite rapid (median HbA1c after 4–6 months: 7.5%) and persisted during time (significant changes from baseline, p<0.005, at each follow-up time point) with a significant difference in the evolution of HbA1c during the time when comparing patients treated with sitagliptin versus patients who had stopped the drug and had switched to another antidiabetic drug (§p=0.006) (figure 2). At baseline, 5.3% of patients had an HbA1c of <7% (53mmol/mol). We observed a higher percentage of patients who reached this target among those treated with the DPP4-i compared with those who had switched to another antidiabetic drug at each time point of observation. After 72 months, 33.8% of sitagliptin-treated patients had HbA1c<7%; the corresponding percentage among those treated with other antidiabetic drugs was 18.5% (online supplementary table 5). The UKPDS RE score at 10 years was evaluated over time during sitagliptin treatment (figure 3): there was a significant trend of risk reduction over time (*p<0.001), with significant reductions from baseline at each time point of observation (p<0.05). Moreover, when comparing patients treated with sitagliptin to those under another antidiabetic drug, a significant difference (p<0.05) in the score was observed starting from 12 months of follow-up, after adjusting for age, sex and diabetes duration, in the absence, however, of a significant difference in the overall trends of UKPDS RE score over the entire follow-up (§p=0.125). BMI significantly reduced over time during treatment with sitagliptin (*p<0.01), with median values of 30.2 kg/m2 at baseline and 27.4 kg/m2 at 72 months of treatment. Different time trends in BMI were observed when comparing patients treated with sitagliptin to those who had switched to other antidiabetic drugs (§p<0.01) (figure 4). We did not detect a gender-related effect of sitagliptin, with improvement in HbA1c, UKPDS RE score and BMI during treatment observed in both men in women (data not shown). During sitagliptin treatment, no significant reduction in systolic blood pressure was observed over time (p=0.403, data not shown), while lipids improved (p<0.01 for total cholesterol and for triglycerides): total cholesterol decreased from baseline (median 192 mg/dL, IQR 164–218) to 24 months of treatment (median 170 mg/dL, IQR 143–197), then it remained approximately stable throughout the follow-up (median at 72 months of treatment: 167.5 mg/dL, IQR 148–188); as for triglycerides, median values were 136 mg/dL (IQR: 106–187) at baseline, 122 mg/dL (96-172) at 12 months, 115 mg/dL (93-163) at 24 months and 111 mg/dL (81-172) at 72 months of treatment. Adverse events (mainly abdominal pain or abnormal liver tests) and microvascular and macrovascular complications were relatively uncommon during sitagliptin treatment and also after sitagliptin discontinuation (online supplementary table 6). Carotid plaques of >30% were detected in nearly 11% of patients during sitagliptin treatment; CHD was observed in 5.7% and 4.4% of patients, respectively, during and after sitagliptin treatment. The corresponding values for microalbuminuria or macroalbuminuria were 6.8% and 10.8%. No pancreatic cancer or acute pancreatitis was detected.
Supplemental material
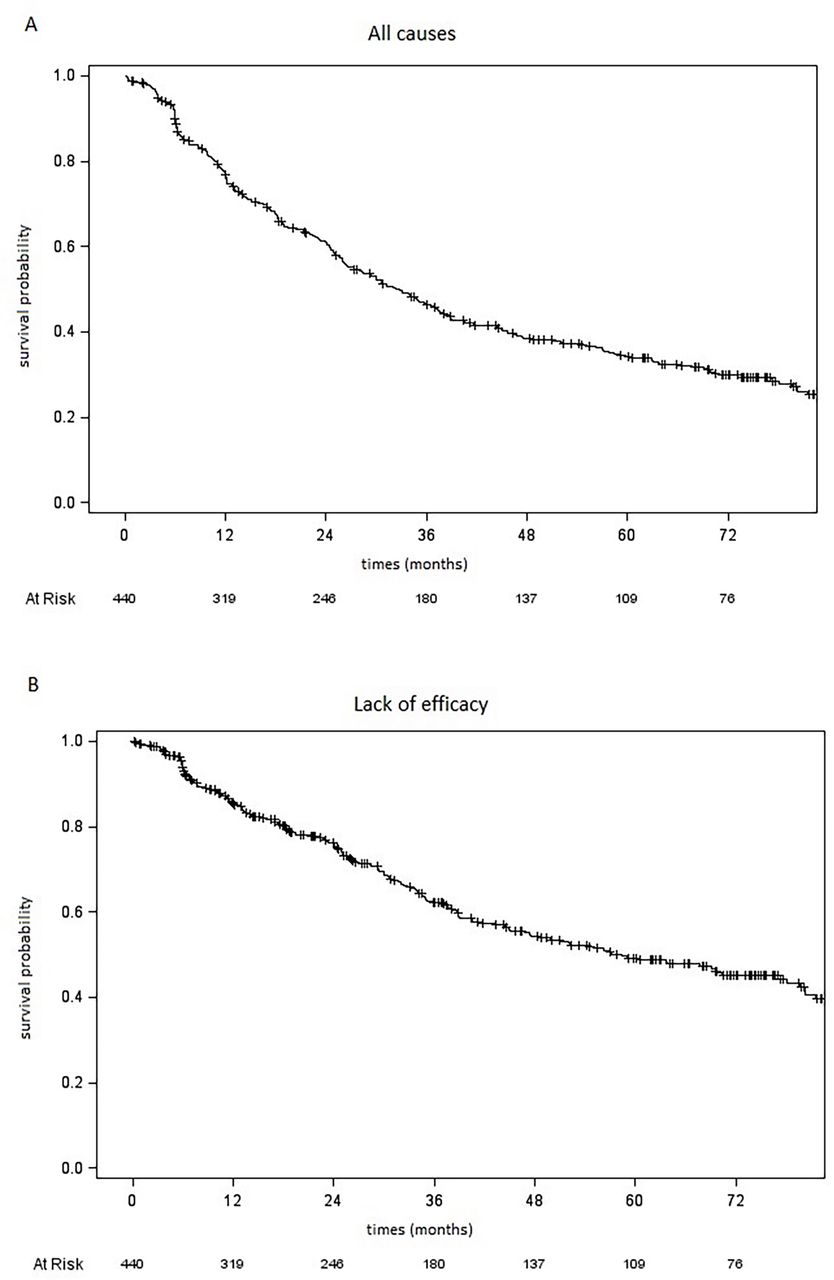
Kaplan-Meier survival curve for time to sitagliptin discontinuation due to any cause (A) and lack of efficacy (B).
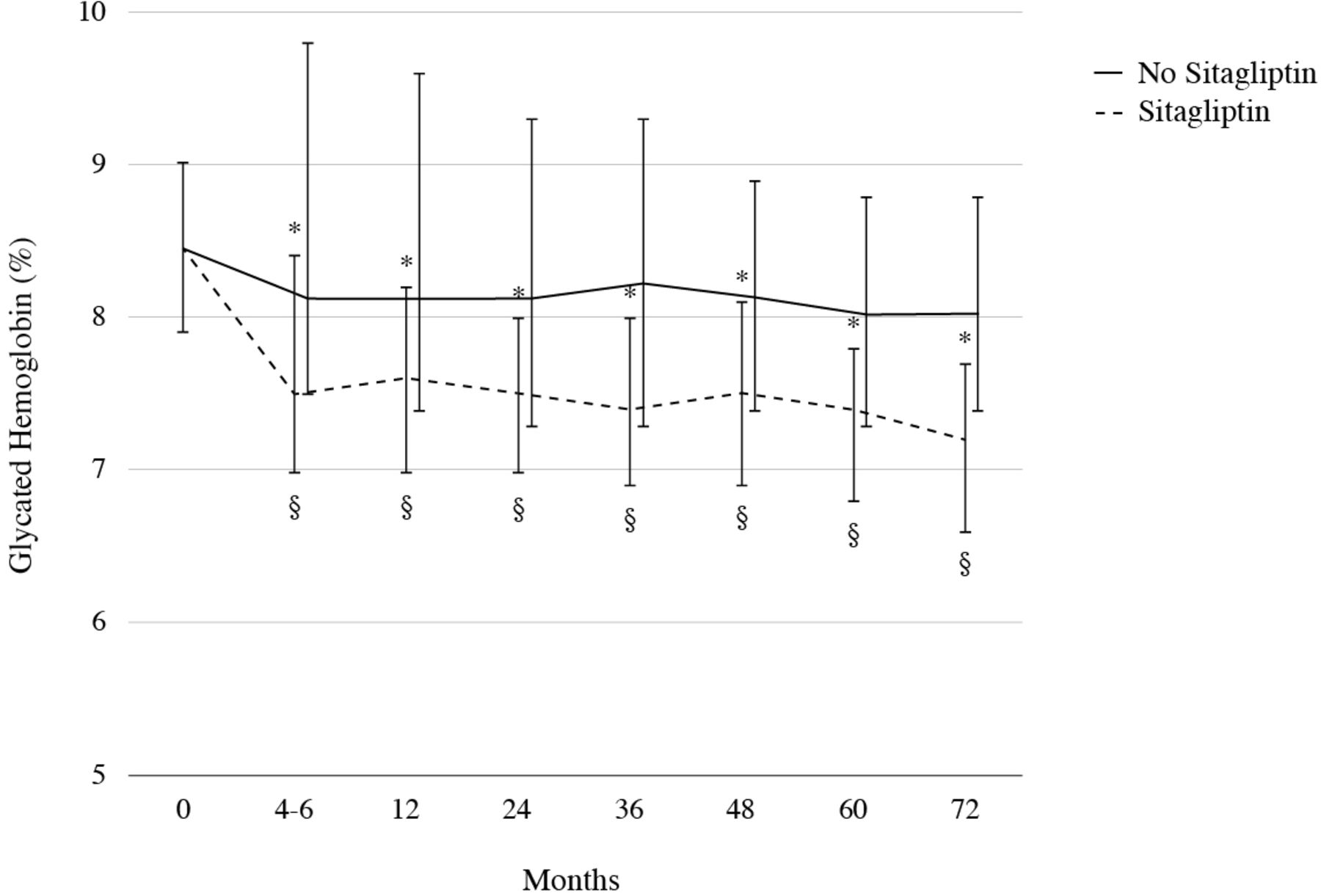
Glycated haemoglobin over time in patients treated with sitagliptin (dashed line) and in those who stopped sitagliptin and switched to another antidiabetic drug (continuous line). Data are shown as median values. The bars indicate IQRs. p for time trend in glycated haemoglobin during treatment with sitagliptin <0.001; p for the overall difference in glycated haemoglobin trend over time by sitagliptin treatment =0.006; §significant (p<0.05) change from baseline during treatment with sitagliptin; *significant (p<0.05) difference between sitagliptin treatment and no sitagliptin treatment.
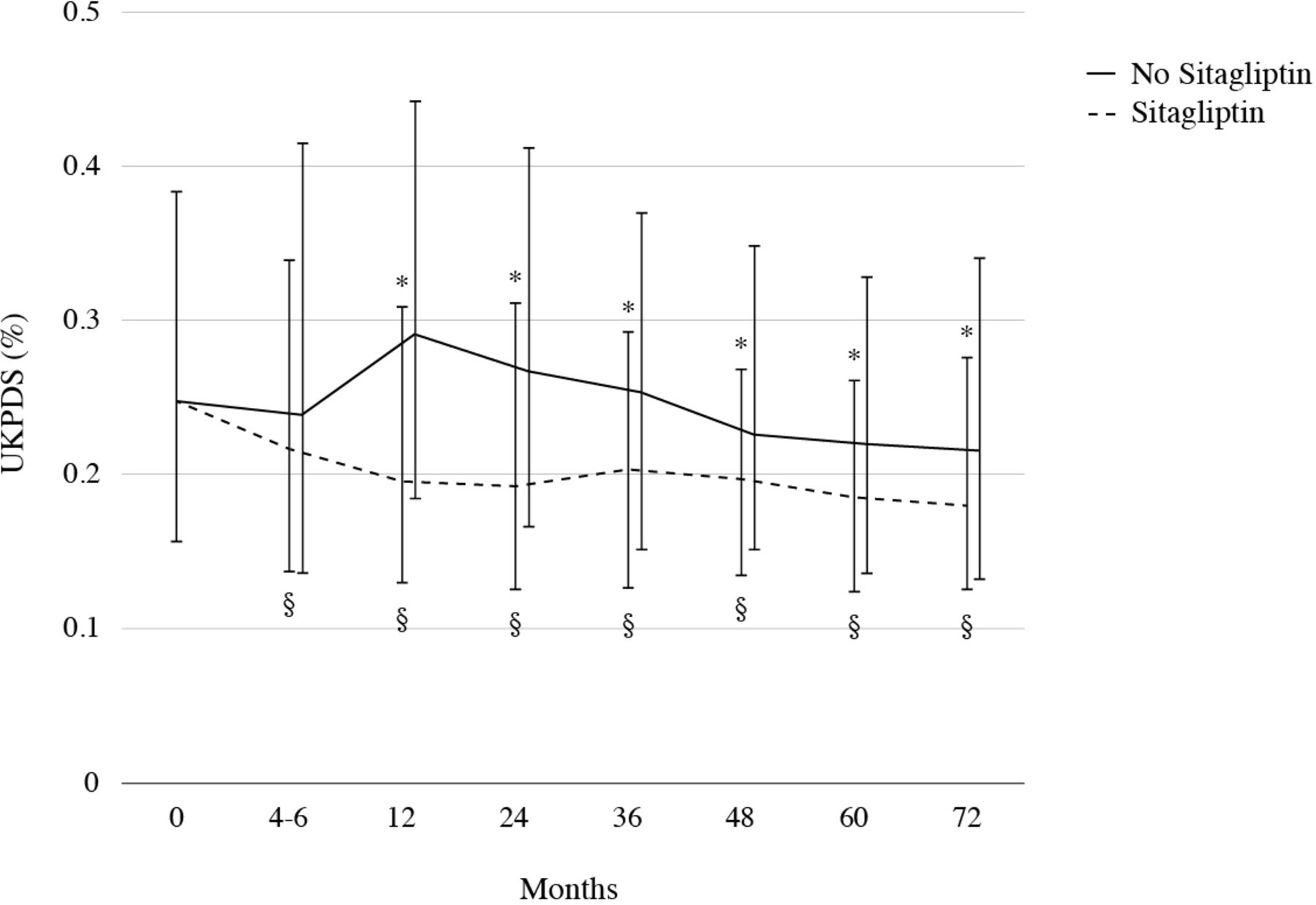
UKPDS risk engine score at 10 years over time in patients treated with sitagliptin (dotted line) and in those who stopped sitagliptin and switched to another antidiabetic drug (continuous line). Data are shown as median values. The bars indicate IQRs. p for time trend in the UKPDS risk engine score during treatment with sitagliptin <0.001; p for the overall difference in the UKPDS risk engine score trend over time by sitagliptin treatment =0.125; §significant (p<0.05) change from baseline during treatment with sitagliptin; *significant (p<0.05) difference between sitagliptin treatment and no sitagliptin treatment. UKPDS, UK Prospective Diabetes Study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
BMI over time in patients treated with sitagliptin (dotted line) and in those who stopped sitagliptin and switched to another antidiabetic drug (continuous line). Data are shown as median values. The bars indicate IQRs. p for time trend in BMI during treatment with sitagliptin <0.001; p for the overall difference in BMI trend over time by sitagliptin treatment <0.01; §significant (p<0.05) change from baseline during treatment with sitagliptin; *significant (p<0.05) difference between sitagliptin treatment and no sitagliptin treatment. BMI, body mass index.
Discussion
The DPP4-is are a class of antihyperglycemic agents orally available for the treatment of T2D. Actually, alogliptin, linagliptin, saxagliptin, sitagliptin and vildagliptin are present on the Italian market: they differ in terms of their chemistry, presenting some diversities about their pharmacological properties (metabolism and elimination being the most interesting in clinical practice), but in terms of efficacy and duration of action, they appear to be similar. With their use, glycemic control is improved both on fasting and on postprandial levels, with a reduction in HbA1c.7 They do not determine weight gain and, as monotherapy, they do not usually cause hypoglycemia,8 but certain attention is required when sitagliptin is added to ongoing insulin therapy (with or without concomitant metformin).9 With reference to CV safety, sitagliptin (or placebo) was added to usual care in 14 671 patients with T2D and established CV disease in the randomized, double-blind TECOS (Trial Evaluating Cardiovascular Outcomes with Sitagliptin) study, whose primary CV outcome was a composite of four major adverse cardiovascular events (MACE): CV death, non-fatal myocardial infarction, non-fatal stroke or hospitalization for unstable angina. During a median follow-up of 3.0 years, sitagliptin did not increase the risk of MACE, neither determined a higher number of hospitalizations for HF nor other adverse events.10 The present study (PERS&O 2.0) is a long-term real-world retrospective, observational, single-center, longitudinal study performed in a general hospital in Northern Italy.1 We collected data about 440 patients with T2D prescribed sitagliptin in accordance with the Italian Pharmacological Agency (AIFA), meaning that some limitations (in terms of HbA1c values and possible drug association) were present. Nevertheless, the most important thing was to obtain a better glycemic control (stated by HbA1c evolution), independently of diabetes duration, body weight, previous CV disease. The baseline demographic and clinical data are quite representative of our T2D outpatients as far as age (64.1±9.2 years), gender (62.5% men), diabetes duration (median 12 years), and BMI (median 30.2) are concerned (table 1). Fasting plasma glucose and HbA1c at baseline represent the poor metabolic control that allowed the prescription of the so-called ‘innovative therapies’, such as DPP4-i and (at that time) GLP1-RAs (glucagon like peptide 1–receptor agonists). Since 2008, every year, patients were prescribed sitagliptin, so we were able to retrospectively collect information on short, medium and longer follow-up with a median of observation of 6.2 years (IQR 4.4–7.4). A certain rate of discontinuation is common in T2D treatment, because of the evolutive nature of the disease: so, it is understandable that 63.5% of our patients suspended sitagliptin therapy because of lack of efficacy (online supplementary table 3). Nevertheless, we underline that sitagliptin efficacy demonstrates a certain ‘durability’ (figure 1): treatment median survival was 58.4 months (95% CI 45.1 to 78.1), and this represents an interesting start point when prescribing any antidiabetic oral drug for the first time. Moreover, persistent sitagliptin treatment demonstrates certain effectiveness during time, as confirmed by HbA1c evolution. HbA1c reduction occurs early (from 8.4% at baseline to 7.5% after 4–6 months) and continues for the whole observational period, with a significant decreasing trend (figure 2). Of certain interest is the evolution of UKPDS RE score over time (figure 3). Patients in persistent sitagliptin treatment show a progressive reduction of their score during time, with a statistically significant trend. However, when comparing trends of patients with and without sitagliptin, we did not observe any significative difference (p=0.125). It is conceivable that the effect on UKPDS RE could be largely determined by age, BMI, lipids and glucose homeostasis because we did not find an improvement over time in systolic blood pressure. Finally, we were able to collect adverse events and the evolution of some diabetic chronic complication (online supplementary table 6): AEs were evident in a very small percentage of patients (6.3% of the whole cohort) and mainly related to a specific abdominal pain or abnormal liver tests, rapidly normalized after drug discontinuation. Reassuringly, no pancreatic cancer or acute pancreatitis were detected. In the same table, microvascular and macrovascular complications are summarized, even though our population was too small to allow a comprehensive evaluation of the issue. Concerning this point, we have to refer to larger randomized controlled trials (RCTs), as the TECOS study,10 in which no significant difference was observed in terms of CV and non-CV outcomes in more than 14 600 patients with T2D. Unfortunately, we were not able to record hypoglycemic episodes due to the retrospective nature of our study. About this, a reference point may be considered a post-hoc analysis of TECOS11 in which the association between severe hypoglycemic episodes and a composite CV endpoint was examined. A common at-risk T2D frail patient phenotype was detected: older people with longer T2D duration, lower body weight, lower eGFR, more frequently women, non-white, insulin-treated and with microalbuminuria or macroalbuminuria. Other retrospective population-based cohort studies evaluated the safety and effectiveness of sitagliptin in patients with T2D. Eurich et al,12 in the setting of large national commercially insured US claims and integrated laboratory database, took into consideration new users of oral antidiabetic drugs being the main outcome measure a composite endpoint of all cause hospital admission and all-cause mortality. Sitagliptin use, mainly as add-on treatment in accordance with clinical guidelines, was not associated with an excess risk of such endpoints compared with other glucose-lowering agents. Another retrospective evaluation ‘A Study of Safety and Efficacy of Sitagliptin Added to Insulin Therapy in the Treatment of Type 2 Diabetes in Kanagawa’ (the ASSIST-K study)13 performed on more than 1000 patients with T2D investigated the efficacy and safety of sitagliptin when added to various insulin regimens. Findings demonstrate that sitagliptin add-on to insulin was useful in T2D subjects with poor glycemic control, irrespective of the insulin regimen.
The present study has some limitations. First, it is a retrospective investigation. Second, the number of patients with T2D is relatively limited. Third, patients with eGFR<60 mL/min are not included in this cohort. Fourth, we did not assess all the factors that could have contributed to HbA1c reduction, including markers of β-cell function and the basal level of active GLP-1. Fifth, we did not perform any evaluation about sitagliptin price because the Italian National Health Service provides the drug without any adjunctive cost for patients with T2D, apart from the limitation in the prescription set by AIFA. We may recall that a recent post hoc observation of the TECOS trial14 revealed that lower hospitalization rates across time with sitagliptin slightly offset sitagliptin treatment costs over 3 years in patients with T2D at high risk of CV events. Sixth, we acknowledge that a peculiar phenotype ‘DPP4-i responder’ should be selected during time, but, once again, we were not able to perform specific cluster analysis (GADA, HOMA 2B and HOMA2-IR based on C-peptide concentrations) as interestingly suggested by some authors.15 Nevertheless, some points of strength may be highlighted: this is a study with a relatively long period of follow-up. The use of Electronic Health Record (EHR) allowed the collection of an interesting series of data. As a matter of fact, our interest is the evaluation of the impact of sitagliptin-persistent treatment on metabolic control, as well as on the evolution of CV risk (determined by UKPDS RE score), being aware that larger and longer studies are mandatory to verify sitagliptin effectiveness and durability over time.
Conclusion
These results, derived by real-world data from the PERS&O study, in which the UKPDS RE score was applied to 440 subjects with T2D treated with sitagliptin, confirmed that the DPP4-i achieves an improvement in metabolic control, as well as a reduction in CV risk. Data obtained by applying UKPDS RE may be appreciated by patients and clinicians in realizing individual CV risk and its evolution during time.
Acknowledgments
The authors thank Maddalena Iannantuoni for graphic design support and Arianna Bossi for professional proof-reading of the manuscript.
Footnotes
Contributors ACB, VDM, CG, and FT formulated ideas and designed the study; VDM, DPB, MG, DB, AB, FF and GM collected clinical data; CG and FT performed the statistical analysis; ACB, CG and FT wrote the manuscript; all authors reviewed and signed the final version of the manuscript.
Funding This study was funded by Treviglio Hospital Health Management.
Disclaimer Preliminary reports of the study have been accepted (as e-poster presentation) at the 28th SID Annual Meeting (Rimini, Italy, 2–5 December 2020).
Competing interests ACB reports grants from Lilly Italia SpA, grants from Novo-Nordisk Italia SpA, personal fees from Sanofi Italia SpA, personal fees from Johnson & Johnson Italia SpA, personal fees from Boehringer Ingelheim Italia SpA, grants from Bayer SA, personal fees from MSD Italia SpA, personal fees from Astra Zeneca Italia SpA, and grants from Pikdare Italia SpA, outside the submitted work.
Patient consent for publication Not required.
Ethics approval Bergamo Ethic Committee approved the study (n. 231/18).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data will be available for 1 year after publication upon reasonable request to the corresponding author.