Article Text

Abstract
Introduction The International Association of Diabetes and Pregnancy Study Group (IADPSG) criteria for gestational diabetes mellitus (GDM) increased the morbidity significantly, but the cost and effectiveness of its application are still unclear. This study aimed to analyze the impact of the IADPSG criteria for diagnosing GDM in China on the perinatal outcomes, and medical expenditure of GDM women versus those with normal glucose tolerance (NGT).
Research design and methods We conducted a retrospective cohort study involving 7794 women admitted at the First Affiliated Hospital of Jinan University (Guangzhou, China), from November 1, 2010 to October 31, 2017. The perinatal outcomes and medical expenditure were retrieved from the electronic medical records in the hospital. Propensity score matching (PSM, in a 1:1 ratio) algorithm was used to minimize confounding effects on the difference in the two cohorts.
Results PSM minimized the difference of baseline characteristics between women with and without GDM. Of 7794 pregnant women, half (n=3897) were all of the pregnant women with GDM admitted to the hospital during the period, the other half women had NGT and were selected randomly to match with their counterparts. Adopting the IADPSG criteria was associated with reduced risk of emergency cesarean section, polyhydramnios, turbid amniotic fluid and perineal injury (p<0.01 for all) and having any one of the adverse fetal outcomes (p<0.01), including fetal distress, umbilical cord around the neck, neonatal encephalopathy, admission to neonatal intensive care unit, birth trauma, neonatal hypoglycemia and fetal death. After PSM, the median total medical expenditure by the GDM women was ¥912.9 (US$140.7 in 2015) more than that of the the NGT women (p=0.09).
Conclusions Despite the increasing medical expenditure, screening at 24–28 gestational weeks under the IADPSG guidelines with the 2-hour, 75 g oral glucose tolerance test can improve short-term maternal and neonatal outcomes.
- diabetes, gestational
- diagnosis
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
An agreement on how to screen, diagnose and manage gestational diabetes mellitus (GDM) to optimize healthcare and minimize adverse perinatal outcomes has not yet been reached.
There is paucity of data with respect to reports on the medical expenditure, clinical efficacy and cost-effectiveness of diagnostic criteria for GDM in China using real-world data.
Early management of GDM can prevent further complications.
What are the new findings?
Adopting the International Association of Diabetes and Pregnancy Study Group (IADPSG) criteria was associated with reduced risk for maternal outcomes including emergency cesarean section, polyhydramnios, turbid amniotic fluid and perineal injury (p<0.01 for all) and many neonatal adverse outcomes in GDM women.
GDM women showed even better perinatal outcomes than the normal glucose tolerance women after management.
Implementing the IADPSG criteria increased the incidence of GDM by 3.95-times, and caused an extra economic burden in GDM women.
How might these results change the focus of research or clinical practice?
The economic burden added to the GDM management may lead to the non-adherence to treatment among women with GDM, thus ambulatory management of GDM might be feasible.
IADPSG criteria are associated with increase of medical expenditure and with improvement in maternal and neonatal outcomes, therefore, the current implementation of IADPSG criteria is appropriate.
Close monitoring of blood glucose levels could result in an overall reduction of complicated pregnancies.
Introduction
Gestational diabetes mellitus (GDM) is a condition of temporary hyperglycemia or glucose intolerance with onset or first recognition during pregnancy and which typically resolves after birth but with associated increased risk of adverse perinatal outcomes.1–3 Although the glucose tolerance of pregnant GDM women reverts to normal shortly after the delivery, these women are still potentially susceptible to type 2 diabetes mellitus (T2DM).4 5 GDM is also related to specific fetal and maternal outcomes including birth trauma, hypoglycemia, hyperbilirubinemia, respiratory distress, long-term obesity and childhood diabetes as well as maternal hypertensive disorders in pregnancy where women with GDM have been reported to have about 1.5-fold increased risk.6 7
In 2010, the International Association of Diabetes and Pregnancy Study Group (IADPSG) put forward new criteria for diagnosing and classifying GDM, namely the IADPSG criteria, based on the data of the Observational Hyperglycemia and Adverse Pregnancy Outcomes study.8 In the following year, the American Diabetes Association (ADA) 2011 criteria were put forward based on the IADPSG criteria, and China immediately adopted the ADA 2011 criteria.
Given that ever more women are being diagnosed as GDM since the two-child policy commenced in 2016,9 and that with more advanced age the incidence of GDM increases, thus the cost-effectiveness of the guidelines remains in doubt.2 3 Moreover, China, an enormous country including various lifestyles, climates and economic conditions, is a microcosm of the world, full of controversies on the diagnosis standards of GDM. 5 10 Importantly, most of the articles concerning GDM diagnostic methods address the Western countries. Hence, to achieve a consensus on the criteria for the diagnosis of GDM, it is necessary to provide insights into the situations in China.
Our previous study found that after the implementation of the IADPSG guidelines, the estimated incidence of GDM and national medical costs increased significantly.11 In 2016, there were 3 million more patients with GDM diagnosed by the IADPSG criteria than those diagnosed by the previous Chinese guidelines (the guidelines published in the seventh edition of the Chinese Obstetrics and Gynecology textbook published by the People’s Medical Publishing House, noted as the ‘previous Chinese guidelines’, or ‘ seventh edition textbook criteria’).11 According to the previous criteria (the seventh edition textbook criteria), the prevalence of GDM was 8.9% and, Zhu Weiwei et al showed that the prevalence of GDM was 18.9% in Beijing after the implementation of the ADA 2011 (IADPSG) diagnostic criteria in 2015.12
Nevertheless, an agreement on how to screen, diagnose, and manage GDM to optimize healthcare and minimize adverse perinatal outcomes has not yet been reached.13 Nevertheless, there is paucity of data with respect to reports on the medical expenditure, clinical efficacy and cost-effectiveness of diagnostic criteria for GDM in China using real-world data . Therefore, this study aimed to investigate the impact of the IADPSG gestational diabetes diagnostic criteria on perinatal outcomes and economic burden brought on in China by analyzing the real-world data of perinatal outcomes and medical expenditure of a 7-year cohort.
Methods
Subjects
This is a retrospective cohort study involving 7794 pregnant women who delivered a singleton baby from November 1, 2010 to October 31, 2017 at the First Affiliated Hospital of Jinan University (Guangzhou, Guangdong, China). Of the 7794 pregnant women, half (n=3897) were all of the pregnant women with GDM admitted to the hospital during the period, and the other half women had normal glucose tolerance (NGT) who we selected randomly to match with their counterparts. After data filtering, a total of 3265 pregnant women were eligible for inclusion in the study and were classified into two groups: 1810 women with NGT (NGT women) and 1455 women with GDM (GDM women) (figure 1). All pregnant women received 2-hour, 75 g oral glucose tolerance test (OGTT) abiding by the IADPSG criteria. The IADPSG diagnostic criteria for GDM states that the upper limits of the blood glucose for fasting, 1 hour postprandial and 2 hours postprandial blood glucose are ≥5.1 mmol/L (92 mg/dL), ≥10.0 mmol/L (180 mg/dL) and ≥8.5 mmol/L (153 mg/dL), respectively (online supplementary table S1). Those with one or more abnormal value (s) will be diagnosed as GDM.14 The missed diagnosis group is defined as the women who are NGT according to the OGTT results abiding by the previous Chinese guidelines but now are diagnosed as GDM using the IADPSG criteria. The previous Chinese guidelines, was a two-step 50 g and 75 g OGTT, where the upper limits of the blood glucose for fasting, 1 hour postprandial, 2 hours postprandial and 3 hours blood glucose are ≥5.6 mmol/L (101 mg/dL), 10.3 mmol/L (185 mg/dL), 8.6 mmol/L (155 mg/dL) and 6.7 mmol/L (121 mg/dL), respectively, any two of which exceeding the upper limits will be regarded as GDM.15
Supplemental material

Flow chart of the algorithm used for study inclusion. A total of 7794 women were initially screened by the International Association of Diabetes and Pregnancy Study Group criteria using 75 g oral glucose tolerance test (OGTT). Ultimately, 3180 pregnant women were included in the cohort study. ADA, American Diabetes Association; GDM, gestational diabetes mellitus; NGT, normal glucose tolerance.
Source of data
The clinical data of perinatal outcomes were extracted from the electronic databases of the First Affiliated Hospital of Jinan University, including the clinical baseline characteristics and maternal and neonatal complications, together with their healthcare expenditure. The healthcare expenditure consisted of the total expenditure, hospitalization expenses and fees for Western medicine, Chinese traditional medicine, registration, consultation, laboratory tests (clinical lab of the hospital, including certain blood tests, urinalysis, tests on tissue specimens and screening tests performed after hospitalization), surgery, examination, blood transfusion, delivery and others. The medical expenditure was incurred after the pregnant women were hospitalized, where the fees for antenatal care were not included. Moreover, the method of payment and the occupation of the pregnant women were also reported. The occupations were recoded according to the International Standard Classification of Occupations 2008 versions structure.16
The clinical characteristics include age at conception, height, weight and gestational age at delivery, body mass index (BMI) at delivery, number of gestation and parity, offspring birth weight, offspring body length and ultrasound examination data, including biparietal diameter, abdominal circumference and femur length of the fetus. The mode of delivery and the methods of induction of labor were also reported. Perinatal outcomes include both maternal and neonatal outcomes. The maternal outcomes include rates of premature deliveries (prior to the 37th gestational week), pregnancy-induced hypertension (PIH; systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg for the first time during pregnancy after 20 weeks without proteinuria), pre-eclampsia (PIH with proteinuria of at least 300 mg/24 hours or a score of ≥3 on dipstick testing in a random urine sample), uterine scar after cesarean section or trauma, premature rupture of membrane, placental abruption, volume and turbidity of amniotic fluid and rates and grades of perineal injury and episiotomy.
Fetal outcomes included Apgar score, fetal respiratory distress, nuchal cord (umbilical cord encircling the neck during pregnancy, labor or delivery), jaundice, caput succedaneum, neonatal anemia, infection, encephalopathy, hypocalcemia, hypokalemia, metabolic acidosis, pulmonary pathologies or congenital anomalies, cardiac damage, patent foramen ovale, prematurity, cephalohematoma and rates of macrosomia, small-for-date infant and high-risk infants.
All clinical outcomes were diagnosed and adjudicated by experienced clinicians.
Exclusion criteria
Any patients meeting the following criteria were excluded from the analyses: not Chinese, multiple gestations, if OGTT was performed prior to 12 gestational weeks, delivery in another hospital, major fetal malformations or GDM diagnosed after the initial test.
Statistical analysis
Propensity scores are useful in reducing selection biases by matching exposed and unexposed women based on the baseline covariates.17 This approach identifies neighborhood that are identical to each other with respect to the probability of being in the exposed group. The following PSM algorithm is used in the present study:
1/N1×Var (Y|GDM=1)+sum (w_i2; i in GDM=0)/(N1)2×Var (Y|GDM=0), where N1 is the number of matched treated, GDM=1 denotes the GDM women, GDM=0 the NGT women and w_i is the weight given to control i.
We conducted the selection process without replacement so that a candidate comparison group member could be matched to only one GDM woman, after which, the distribution of the covariates between two groups was expected to be the same.18 19
After one-to-one PSM algorithm, with the confounding variables being maternal age, weight, height and gestational age, 1157 cases were ruled out.18 Therefore, the remaining total cohort (n=2108) were then labeled as the Matched Normal Glucose Level Group (n=1054) and the Matched Gestational Diabetes Mellitus Group (n=1054), whose age, weight, height and duration of pregnancy were statistically insignificant (p>0.05), indicating that the data are comparable.
Continuous variables were tested for normal distribution using the Kolmogorov-Smirnov test. Multiple comparisons of continuous variables were performed by analysis of variance, and the Scheffe post hoc test was used. The Kruskal-Wallis test was used to analyze continuous variables that did not follow the normal distribution; χ2 tests were used to compare categorical variables. The data are presented as means and SD for symmetrically distributed continuous variables, the total number and percentages for categorical variables and median and IQR for skewed continuous variables. Multivariable logistic regression analysis with adjustments for confounding variables was also adopted to estimate the effect of GDM on women. Statistical analyses were performed using Stata V.14.0 (StataCorp, USA). Differences were considered significant for p values <0.05. The heat map was created using GraphPad Prism V.5.0 (GraphPad Software, San Diego, California, USA).
Results
In the present study, we investigated a total of 7794 pregnant women screened by the 75 g OGTT under the IADPSG criteria. After data cleaning, 3265 eligible women were included, of which 1455 were diagnosed as GDM, 1810 women were NGT when implementing the IADPSG criteria. After one-to-one PSM, both the matched NGT group and matched GDM group included 1054 women.
Propensity score matching reduced the confounding effects
After the PSM, the differences in baseline characteristics between the NGT and GDM women were barely discernible (table 1). As for the delivery mode when comparing the NGT and GDM women after PSM, where a slight plethora of rates of planned cesarean section and a lower emergency cesarean rate of GDM women were found in GDM women compared with the NGT women (table 1). Moreover, the induction method differed greatly, in which less GDM women were shown to use induction for the delivery, and the NGT women used oxytocin for induction more often than their counterparts (p<0.01, table 1).
Clinical characteristics in women screened with 75 g oral glucose tolerance test by the IADPSG criteria
Comparison of perinatal outcomes between NGT and GDM women
The maternal and neonatal outcomes among all deliveries are presented in table 2. Regardless of the propensity score matching, there were significant differences in the occurrence of the uterine scar after cesarean section or trauma, perineal injury, episiotomy and polyhydramnios between the NGT women and GDM women, where the NGT women tended to have more adverse maternal outcomes than the GDM women (p<0.01 for all, table 2). The rate of uterine scar after cesarean section or trauma was almost sixfold higher in the NGT women (5.7%) than that in the GDM women (1.0%), and the NGT women (4.4%) exhibited a threefold higher rate of polyhydramnios than the GDM women (1.4%) (p<0.01 for all, table 2). We detected no differences in gestational hypertension and pre-eclampsia comparing the NGT and GDM women after PSM (p=1, table 2).
Comparison of maternal and neonatal outcomes in NGT and GDM women among women selected and matched according to the propensity score†
Nevertheless, the mean time the neonates stayed in the NICU, the occurrences of neonatal admission to NICU, fetal distress and umbilical cord around the neck and high-risk infants remained statistically different when comparing NGT and GDM women even after the PSM (p<0.01 for all, table 2), where the neonates of NGT women were more susceptible to adverse outcomes. Moreover, interestingly, after PSM, the occurrences of neonatal infection, cephalohematoma and metabolic acidosis were not significantly different (p=1, table 2). Moreover, the neonates of GDM women have higher rates of pulmonary pathologies, patent foramen ovale and macrosomia (p<0.05 for all, table 2).
The clinical features of the missed diagnosed group by the previous Chinese guidelines
According to the previous Chinese guidelines, we re-classified the GDM women diagnosed using the IADPSG criteria into the missed diagnosis group (missed GDM, n=1087) and definite GDM group (GDM, n=368). The missed diagnosis group was defined as the women diagnosed as GDM under the IADPSG criteria but as NGT using the previous Chinese guidelines (Textbook guidelines). The baseline characteristics and perinatal outcomes of these groups are reported in online supplementary table 2 and online supplementary table 3, respectively. The incidence of GDM increased 3.95-times after implementing the IADPSG criteria.
Generally, the definite GDM women had greater age and weight than the missed GDM and NGT women (p<0.01 for all, online supplementary table 2). The BMI increased across the three groups, and there was a larger proportion of women with high BMI in the definite GDM group (p<0.01, online supplementary table 2). Moreover, across the NGT, missed GDM and definite GDM groups, the rates of Cesarean section greatly increased while the emergency cesarean section dramatically decreased (p<0.01 for all, online supplementary table 2).
Regarding the perinatal outcomes, we found that the missed diagnosed group had much fewer occurrences in pre-eclampsia, gestational hypertension, NICU admission, neonatal anemia and neonatal infection than the other two groups (online supplementary table 3). Also, the definite GDM women had much higher occurrences of neonatal complications (online supplementary table 3).
GDM women spent more medical expenditure than NGT women
The median total medical expenditure of the GDM women throughout the hospitalization was ¥2826.3 (US$435.5 in 2015), while that of the NGT women was ¥2243.1 (US$345.7), in which the GDM women spent ¥583.2 (US$89.9) more than the non-GDM women (p=0.14, online supplementary table 5).
After the PSM, the median total medical expenditure of the GDM women throughout the hospitalization was ¥3018.1 (US$465.1), which is ¥912.9 (US$140.7) more than that of the NGT women, who spent ¥2105.2 (US$324.4) (p=0.09, online supplementary table 5). After PSM, only the laboratory tests differed significantly between the NGT and the GDM women (¥456.6 (US$70.4) vs ¥572.0 (US$88.1), p<0.01, online supplementary table 5). Moreover, the NGT women spent more on the examination and blood transfusion than the GDM women (online supplementary table 5).
We further analyzed the medical expenditures in the missed diagnosis GDM women and definite GDM women (online supplementary table 5). There was a stepwise increase in the total medical expenditure across the NGT, missed GDM and definite GDM groups. An increase of expenditure for western medicine (¥664.5 (US$102.4), p=0.02) and surgery (¥800.0 (US$123.3), p=0.87) were found among the missed GDM women relative to the other two groups, while the blood transfusion cost (¥1060.0 (US$163.3), p=0.08) was considerably lower in the missed GDM women (online supplementary table 5). Moreover, the definite GDM group had a much greater laboratory test cost (¥714.0 (US$110.0), p<0.01, online supplementary table 5).
Matrix correlation of occupation and payment method with the medical expenditure
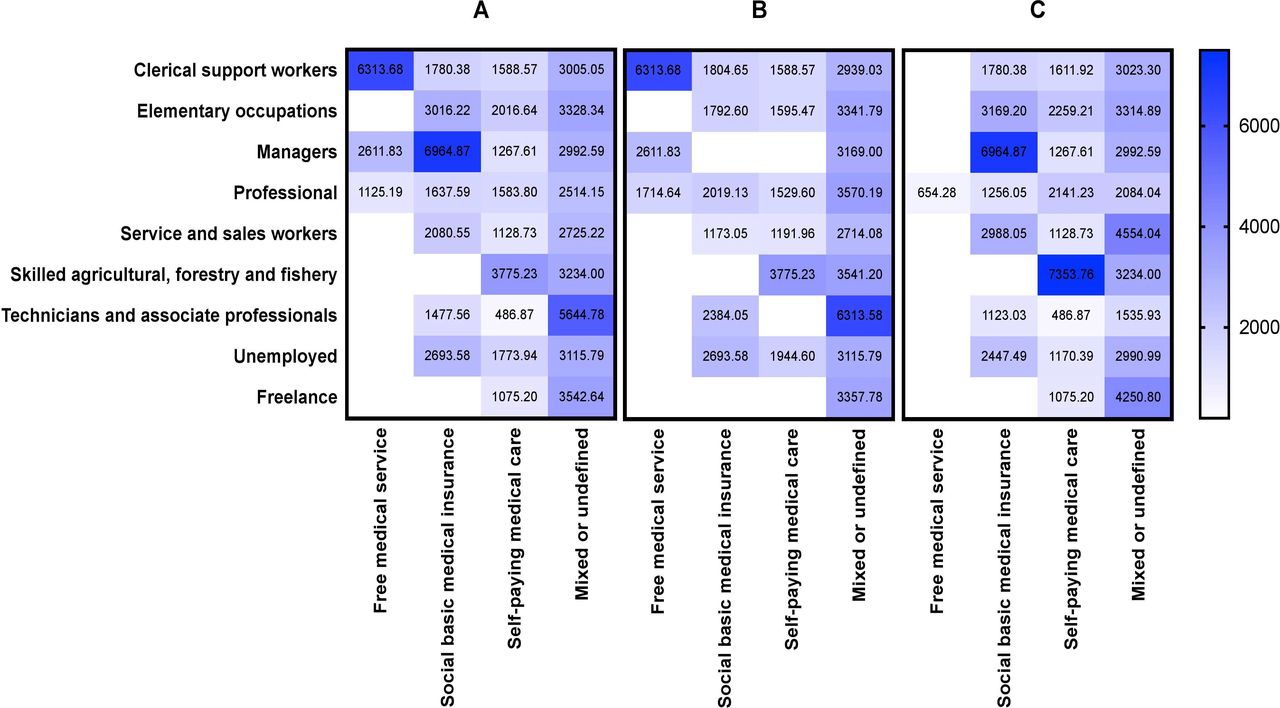
The correlation of the occupations of the GDM women with the methods of payment were further analyzed (figure 2). We found except for the three occupations (clerical support workers, managers and professionals) who had the possibilities of free medical service, most people tended to pay their medical expenditure by self-paying or mixed-method, especially the NGT women (figure 2A,B). A large number of pregnant women self-paid the whole amount of medical expenditure, especially the GDM women (figure 2C).
{kind=link}
{kind=link}
The matrix heat map of mean medical expenditure associated with occupation and payment type. (A) All women; (B) women with normal glucose tolerance; (C) women with gestational diabetes mellitus. The occupations were recoded according to the International Standard Classification of Occupations 2008 versions (ISCO-o8) structure.
Discussion
In the present study, we applied PSM to counterbalance confounding effects of maternal age, height and weight at delivery, as well as the duration of pregnancy. The implementation of the IADPSG criteria improved the perinatal outcomes, but the incidence of GDM increased by 3.95-times after implementing the IADPSG criteria, and the medical expenditure also increased, causing an economic burden of ¥912.9 (US$140.7).
We observed that the GDM women diagnosed according to the IADPSG criteria, despite their higher medical expenditures, showed better perinatal outcomes than the NGT women, after PSM of baseline differences using one-to-one matching. This finding indicates that the IADPSG criteria are beneficial from the clinician’s perspectives. And the results were also proven by the linear regression (online supplementary tables 4 and 5). Many scholars have stressed untreated GDM might lead to higher rates of maternal and perinatal morbidity and mortality,20 21 and we found that the adverse perinatal outcomes can be reversed through proper management and treatment of GDM (table 2). Besides, the overall occurrences of adverse perinatal outcomes of the GDM women were significantly less than that of the NGT women, both maternal and neonatal outcomes (table 2), or in other words, the NGT women and their neonates were more susceptible to adverse outcomes. This might be accounted for by more attention and the better obstetric care of the GDM women, by both themselves and the clinicians. There may also be a remote possibility that the NGT women may have had a false negative result and underdiagnosed.
Nevertheless, the neonates of GDM women tended to be more susceptible to pulmonary pathologies, patent foramen ovale and macrosomia, which are the diseases more congenital in nature than the other outcomes (p<0.05 for all, table 2). This finding is as expected following a general knowledge of influence of maternal hyperglycemia on developing fetuses and it coincides with the studies by Boney et al, who reported that macrosomic offsprings were exposed to a hyperglycemic intrauterine environment are at increased risk of developing metabolic disorders in childhood.22–24 del Rosario et al found that due to the intrauterine exposure to hyperglycemia, the neonates might have an increased risk of developing T2DM through DNA methylation, causing epigenetic changes via an effect on β-cell function in the offspring.25 Moreover, owing to the mitotic stability of DNA methylation, the effects can be long-standing as time passes, producing long-term changes in the gene expression.25
However, we cannot dismiss the potential role of social determinants of health, especially socioeconomic factors—such as the access to medical care, income and education level.26 In our study, we found that the total medical expenditure of the GDM women spent throughout the hospitalization was ¥583.2 (US$89.9) more than the NGT women (¥912.9 (US$140.7) after the PSM) (p=0.14 before PSM and p=0.09 after PSM, table 3), which does not coincide with the findings by Xu et al, who found that, on average, the medical expenditure of a GDM woman was ¥6677.37 (US$1929.87 in 2015) more than an NGT women.13 And Xu et al estimated the economic burden of GDM to be ¥19.36 billion.13
Comparison of medical expenditures in NGT and GDM women, and the medical expenditures in women with NGT, GDM and the missed diagnosed group†
The inconsistencies might be a result of variation in management plans and algorithms for different types of GDM, and the follow-up expenditure (viz. pharmaceutical and ambulatory services, as well as the lifestyle management). Xu et al only calculated the direct medical expenditure using insulin, dismissing other hyperglycemic drugs for GDM, including metformin. The percentage of patients with GDM needing pharmacological treatment varies from 20% to 60% in various studies, not to mention that the use of insulin therapy itself clinically is seldom.27–29 According to the 2011 National Diabetes Fact Sheet of Center of Disease Control, only 12% of adults diagnosed with diabetes are receiving treatment with insulin in the USA, and this number could be much lower in low-income and middle-income countries like China.30 Therefore, this result might infer that the actual capacities or willingness of the residents to pay for the management of GDM might remain far below the present economic burden of GDM care brought on by the introduction of the IADPSG criteria in China.
Also, after relegating the GDM women diagnosed under the IADPSG criteria to the missed diagnosed group (missed GDM, n=1087) and GDM (definite GDM, n=368) according to the previous Chinese guidelines, we inferred that the incidence of GDM increased 3.95-times after implementing the IADPSG criteria (online supplementary table 2). These results were consistent with our previous data, where the incidence of GDM was 22.94% when implementing the IADPSG criteria.11 However, under the previous Chinese criteria (the Textbook guidelines), the occurrence rate of GDM was only 8.9%, and Zhu et al found that in Beijing, the prevalence rate of GDM is 18.9% after the implementation of the IADPSG diagnostic criteria in 2015.12
We further analyzed the medical expenditures in the missed diagnosed GDM women and definite GDM women (table 3). There was a stepwise increase in total medical expenditure across the NGT, missed and definite GDM groups. Moreover, in order to evaluate how medical expenditure was influenced, we correlated the occupations of the GDM women with the payment methods (figure 2). Despite the introduction and application of social basic medical insurance, a large number of pregnant women, especially GDM women, self-paid the total amount of the medical expenditure, or in fact they paid less money with the basic medical insurance (figure 2C).
Some global qualitative studies report that one of the barriers to GDM treatment is the financial barriers related to healthcare and unaffordability, which accounts for the non-adherence to treatment among women with GDM in low-income and middle-income countries and in high-income countries like the USA.31–33 However, in low-income and middle-income countries, this situation could be much worse, as not all of the rural primary health centers are accessible to insulin treatment or the early screening for GDM.34
In this regard, ambulatory management of GDM might be feasible. In theory, the blood glucose level of most pregnant women with GDM can be controlled merely by dietetic treatment, indicating that the adoption of the IADPSG criteria in China may be reasonable. Some studies also point out there is no strict difference in glycemic control and perinatal outcomes in women with GDM between the hospitalization and the ambulatory management. 31 35 Therefore, ambulatory management, including telemedicine, diet and exercise management, as well as preconception education, can be considered feasible to lessen the current economic burdens of GDM management.31 In 80% of cases, interventions were shown to significantly reduce GDM complications and their final costs, and only 20% of women with GDM needed additional medications.36 37
Recently, Ming et al performed a meta-analysis, finding a modest but statistically significant improvement in hemoglobin A1c associated with the use of a telemedicine technology.38 Overall, the clinicians should pay greater attention to the preconception counseling, weight management prior to and during pregnancy, self-monitoring of blood glucose levels, medication, medical nutrition therapy and exercise, especially in low-income and middle-income cities and countries.38
An important strength of our study is the utilization of PSM algorithm to reduce the selection bias. By measuring and adjusting for all known and measurable confounding variables, this approach yields efficient estimates for observational studies. Nevertheless, we cannot exclude some bias due to residual confounding.39 Moreover, owing to the nature of the retrospective study, we failed to follow-up the conditions of glycemic control in the women with GDM and to distinguish the medical expenditure of different GDM managements undertaken, which are the limitations of this study.
Conclusion
In sum, this study has shown that by applying the IADPSG criteria for diagnosing the GDM in China, despite the increasing medical expenditure, improvements were found for both short-term and long-term maternal and neonatal outcomes. And the increased medical costs may be offset by the benefits gained in the long run.
Acknowledgments
The authors would like to thank the First Affiliated Hospital of Jinan University for providing the platform and resources needed for the conduction of this study.
References
Footnotes
ZH, YT and HX are joint first authors.
Contributors XX and W-kM conceptualized the design of the study, and drafted and revised the manuscript. ZH and YT conceptualized and drafted the article, with the assistance of XX and W-kM. HX and SL collected the clinical data from the First Affiliated Hospital of Jinan University. YX, ZC, JS, XB, MP and L-zW helped collect and analyze the data regarding the medical expenditure in the Department of the Obstetrics and Gynecology of the First Affiliated Hospital of the Jinan University and drafted the manuscript. All authors have contributed significantly, and all authors have approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study design was approved and waived from ethical application abiding by the regulation of the Ethics Committee of the First Affiliated Hospital of Jinan University. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. Data were obtained from a Tertiary Hospital, and in view of the protection of the privacy of the patients, the data are not publicly available, but on reasonable request, the data are available.