Article Text

Abstract
Introduction Circulating orosomucoid, an acute-phase protein, predicted type 2 diabetes mellitus risk in several Western countries. Here, we assessed serum orosomucoid (ORM) in relation to prediabetes in the Japanese.
Research design and methods Participants consisted of 83 middle-aged Japanese subjects with normal glucose tolerance (NGT), 37 with prediabetes and 4 with newly identified diabetes, whose homeostasis model assessment-insulin resistance (HOMA-IR) averaged 1.1±0.7, 1.4±0.9 and 1.7±0.8, respectively. Body composition, serum inflammatory markers, adiponectin, β-cell function and insulin resistance inferred from serum insulin kinetics during an oral glucose tolerance test were compared cross-sectionally between those with prediabetes and NGT.
Results Serum orosomucoid, but not high-sensitivity C reactive protein, was elevated in prediabetes (190±29 vs 141±31 mg/dL) with further elevation in diabetes (295±52 mg/dL) (all p<0.001). Prediabetes was associated with lower Oral Disposition Index (the product of the Insulinogenic Index and Matsuda Index) with further depression in diabetes. No association was found with skeletal muscle mass, HOMA-IR, serum triglyceride, high-density lipoprotein (HDL) cholesterol and adiponectin.
Conclusions Higher circulating ORM and reduced glucose induced insulin secretion were found in middle-aged Japanese people with prediabetes in the absence of insulin resistance.
- acute-phase proteins
- prediabetic state
- insulin secretion
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Although studies are missing in the Japanese, population studies in Western countries have shown the association between orosomucoid, one of the major acute-phase proteins of glycoprotein acetyls (GlycAs), and type 2 diabetes and between GlycAs and an increase in glycemia and a decrease in insulin secretion.
What are the new findings?
Japanese people aged 50 years with prediabetes had higher circulating orosomucoid, reduced glucose induced insulin secretion and insulin resistance which is indistinguishable from that in normal glucose tolerance.
How might these results change the focus of research or clinical practice?
Elevated orosomucoid may be related to reduced glucose induced insulin secretion in middle-aged Japanese people with prediabetes.
Introduction
Chronic low-grade inflammation can contribute to the pathogenesis of many diseases including type 2 diabetes and cardiovascular disease.1 2 Prediabetes is a well-known risk factor for type 2 diabetes and has been reported to be associated with cardiovascular disease.3 4 Elevated concentrations of C reactive protein (CRP), a prime acute-phase protein, were found in people with prediabetes.5–9 Associations between CRP and increased risk of developing type 2 diabetes were demonstrated in studies including those from East Asia.10–14
Orosomucoid (ORM), also known as α−1 acid glycoprotein, is another acute-phase protein and is produced by liver and peripheral tissues in response to systemic reaction to inflammation.15 In addition to acting as an acute-phase reactant and disease marker, ORM has many activities including modulating immunity, binding and carrying drugs, maintaining the barrier function of capillary, and mediating the sphingolipid metabolism.15 Studies conducted in US or European populations have shown that ORM is associated with increased risk of developing type 2 diabetes.13 16–18 Associations between circulating ORM and glycemia during an oral glucose tolerance test (OGTT) have previously demonstrated in middle-aged Finnish people.19 We found similar associations in young Japanese women and their middle-aged parents.20 21 However, studies on the relation between ORM and prediabetes are limited as discussed later. Here we evaluated the relation between ORM and prediabetes in middle-aged Japanese people.
Methods
We cross-sectionally studied 65 premenopausal middle-aged women and 59 middle-aged men, whose details have been reported elsewhere.21 22 They were Japanese and biological parents of students of Mukogawa Women’s University. Subjects who reported that they were under treatment for clinically diagnosed acute or chronic inflammatory diseases, endocrine, cardiovascular, hepatic, renal diseases, hormonal contraception, and unusual dietary habits were excluded. Nobody reported receiving any medications or having regular supplements. The study was in accordance with the Declaration of Helsinki. All subjects were recruited as volunteers and gave written consent after the experimental procedure had been explained.
After a 12-hour overnight fast, at 8:30, they underwent a standard 75 g OGTT with measurement of glucose and insulin at 0 min (fasting), 30 min, 1 hour, and 2 hours after glucose ingestion. Prediabetes (impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT)) and diabetes were diagnosed based on glycemia criteria (fasting and 2-hour glucose concentrations) of the American Diabetes Association.23 OGTT revealed prediabetes in 14 women and 23 men, and newly identified diabetes in 4 men. Among 37 subjects with prediabetes, 12 had isolated IFG, 14 isolated IGT and 11 IFG/IGT.
Plasma glucose (PG), hemoglobin A1c (HbA1c), serum insulin, triglyceride, high-density lipoprotein (HDL) cholesterol, adiponectin, leptin, high-sensitivity CRP (hsCRP) and tumor necrosis factor-α (TNF-α) were measured as previously reported.24 ORM concentrations were measured in fasted samples by an immunoturbidimetric method using a commercially available kit (N Antiserum to Human α1-acid Glycoprotein, Siemens Healthcare Diagnostics, Tokyo, Japan) and an autoanalyzer (JCA-BM6010, JEOL, Tokyo, Japan). Intra-assay and interassay coefficients of variation at 87 mg/dL were 1.4% and 1.7%, respectively. The area under the concentration curves of PG and insulin (AUCg and AUCi, respectively) were calculated by the trapezoid method. Homeostasis model assessment-insulin resistance (HOMA-IR), the Matsuda Index and the Insulinogenic Index (IGI) were calculated as previously reported.25–27 The Oral Disposition Index (ODI) was calculated as the product of IGI and Matsuda Index.
Fat mass, bone mass and lean mass for arms, legs, trunk and the total body were measured using whole-body dual-energy X-ray absorptiometry (DXA) (Hologic QDR-2000, software V.7.20D, Waltham, Massachusetts, USA) as previously reported.24 The leg region included the entire hip, thigh and leg. General adiposity was assessed using body mass index (BMI), the percentage of body fat (% body fat) and Fat Mass Index (FMI), the last of which was calculated as body fat mass in kilograms divided by height in square meters. Abdominal fat accumulation was assessed by waist circumference and the ratio of trunk to leg fat.28 Skeletal muscle mass was assessed using appendicular Skeletal Muscle Mass Index (SMI) calculated as lean mass in extremities in kilograms dividing by height in square meters.
Data were presented as mean±SD unless otherwise stated. Due to deviation from normal distribution, IGI and ODI were logarithmically transformed for analyses. Comparisons between two groups were made with two-sample t-test. Differences among three groups were analyzed using analysis of variance and then Bonferroni’s multiple comparison procedure. Although there were gender differences in associations between body composition and cardiometabolic risk factors,22 middle-aged men and women did not differ in ORM and glycemia and insulinemia during OGTT (online supplemental tables 1 and 2), therefore, two groups were combined for analyses. Correlations between ORM and glycemic and other variables were investigated by Pearson’s analysis. Stepwise multivariate linear regression analyses were performed to identify most important determinants of ORM. Independent variables included were all variables that showed a significant association with ORM. Because of multicollinearity, glucose values at four time points and AUCg were analyzed in separate models. A two-tailed value of p<0.05 was considered statistically significant. Statistics were performed with SPSS system V.17.0 (SPSS, Chicago, Illinois, USA).
Supplemental material
Results
Although BMI and waist circumference were higher in women with prediabetes compared with normal glucose tolerance (NGT) (online supplemental table 1), women with prediabetes had a mean BMI <25.0 kg/m2 (a cut-off value of obesity) and their waist circumference was far below a cut-off value of abdominal fat accumulation for Japanese women (<90 cm). However, men in three groups had mean waist circumference >85 cm (a cut-off value of abdominal fat accumulation for Japanese men) although BMI averaged <25.0 kg/m2 even in men with prediabetes and diabetes (online supplemental table 2). Their mean HOMA-IR ranged from 1.1 to 1.7 (table 1). Women with prediabetes had higher FMI, % body fat, trunk/leg fat ratio as well.
Anthropometric and biochemical characteristics of middle-aged Japanese people with normal glucose tolerance (NGT), prediabetes and newly identified type 2 diabetes (DM)
In spite of highly significant differences in glucose concentrations at four time points during OGTT (all p<0.001) (figure 1), there was no significant difference in insulin concentrations at four time points. Although 30 min insulin concentrations and Matsuda Index (table 1) showed a stepwise decrease from NGT to diabetes, these changes were not statistically significant. Those with prediabetes and diabetes had lower IGI than those with NGT. ODI decreased in prediabetes as compared with NGT with further decrease in diabetes. AUCg and HbA1c showed stepwise increase from NGT to diabetes whereas AUCi did not differ. Serum ORM showed a stepwise increase (figure 2) whereas SMI, HOMA-IR, serum triglyceride, HDL cholesterol, adiponectin, leptin, TNF-α and hsCRP did not differ.
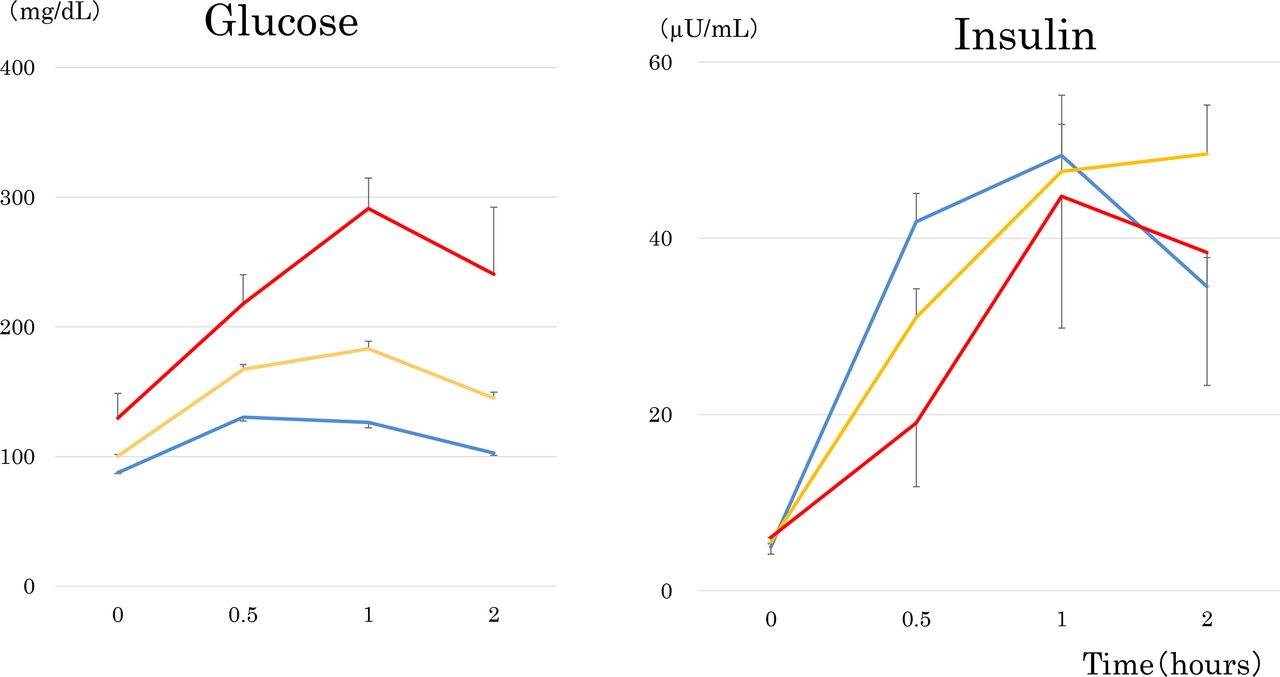
Glucose and insulin responses during 75 g oral glucose tolerance tests in middle-aged Japanese people with normal glucose tolerance (blue lines), prediabetes (yellow lines) and newly identified type 2 diabetes (red lines). Mean±SD. In spite of highly significant differences in glucose concentrations at four time points (all p<0.001), there was no significant difference in insulin concentrations at four time points. Although 30 min insulin concentrations showed a stepwise decrease from normal glucose tolerance to diabetes, these changes were not statistically significant.

Serum orosomucoid in middle-aged Japanese people with normal glucose tolerance (blue bar), prediabetes (yellow bar) and newly identified type 2 diabetes (red bar). Mean±SD. Means not sharing common letter are significantly different each other at p<0.05 by Bonferroni’s multiple comparison procedure.
Although the sample size of prediabetes was small, we compared isolated IFG (n=12) and IGT with and without IFG (IGT group, n=25) (online supplemental table 3). The IGT group had elevated AUCg (334±38 vs 285±30 mg/dL/2 hours, p<0.001) and serum ORM (196±29 vs 177±24 mg/dL, p=0.05).
Serum ORM showed strong and positive associations with fasting PG (r=0.683, p<0.001) and postload glycemia and AUCg (r=0.759–0.961) (figure 3 and online supplemental table 4). In models which included trunk/leg fat ratio, IGI, Matsuda Index and glucose concentrations at four time points as independent variables, three postload glucose concentrations emerged as independent determinants of ORM and explained 94.1% and 96.2% of ORM variability in women and men, respectively. In models including AUCg instead of glucose concentrations at four time points, 90.7% and 92.9% of ORM variabilities were explained by AUCg in women and men, respectively.

{kind=link}
{kind=link}
{kind=link}
The scatter plot between serum orosomucoid and plasma glucose at 30 min (A), 1 hour (B) and 2 hours (C) and the area under the glucose curve (D) during a 75 g oral glucose tolerance test. Blue, yellow and red circles represent normal glucose tolerance, prediabetes and newly identified type 2 diabetes, respectively.
Discussion
The present study has shown that higher circulating ORM and reduced glucose induced insulin secretion were found in middle-aged Japanese people with prediabetes. The relation was independent of several other known risk factors for type 2 diabetes including general and central adiposity (FMI and trunk/leg fat ratio, respectively) and insulin resistance/sensitivity. The present study confirmed strong and positive association of ORM with postload glycemia and glucose excursion (AUCg) as previously reported in middle-aged Finnish individuals19 and young Japanese women.20 Although sample size was small in those with diabetes, there was a graded increase in serum ORM, with the highest levels observed in individuals with diabetes, intermediate levels in individuals with prediabetes, and the lowest levels in individuals with NGT. It is noteworthy that fasting insulin averaged 5.5±3.5 μU/mL (table 1) in middle-aged Japanese people with prediabetes in the present study, suggesting that they were not insulin resistant.
Studies which investigated the association between ORM and prediabetes/diabetes are limited and, to the best of our knowledge, the present study is the first to demonstrate ORM elevations in Japanese people with prediabetes. In the study by Pickup et al,29 there was a graded increase in ORM, with the highest levels observed in type 2 diabetic individuals with the metabolic syndrome, intermediate levels in type 2 diabetic individuals without the syndrome, and the lowest levels in controls. McMillan30 is one of the first to demonstrate that serum ORM increased in people with glucose intolerance as in diabetes compared with healthy controls.
ORM is one of the major acute-phase proteins of glycoprotein acetyls (GlycA), which has been shown to be a risk of incident type 2 diabetes.31 Fizelova et al32 investigated the association of hsCRP and GlycA with insulin secretion, insulin sensitivity, insulin resistance-related traits, and glucose levels. They found that GlycA was a strong predictor of an increase in glycemia (FPG, 2 hours PG, and AUCg) and a decrease in insulin secretion. These observations may be in line with the current finding that elevated circulating ORM and reduced glucose induced insulin secretion were evident in Japanese middle-aged adults with prediabetes. We have previously demonstrated that elevated ORM was associated with postload hyperglycemia in Japanese women (aged 20 years) with NGT,20 some of whom were daughters of middle-aged people (aged 50 years) in the present study. These observations suggest that ORM-associated subtle hyperglycemia for decades may be related to reduced glucose induced insulin secretion in middle-aged Japanese people with prediabetes, suggesting glucotoxicity on β-cells.33
The strengths of the present study include a homogeneous study population with scarce confounding factors,24 and accurate and reliable measures of body composition by DXA. The deduction from the results of family members (daughters in this case) appear to be unique in reducing confounding factors for insulin sensitivity including genetic, dietary, educational and socioeconomic factors.34 Several limitations of this study warrant consideration. The small sample size is the major limitation. The cross-sectional design of the present study complicates the drawing of causal inferences, and a single measurement of biochemical variables may be susceptible to short-term variation, which would bias the results toward the null. We used crude measures of insulin sensitivity in muscle and adipose tissue, which may be less accurate. Statistical power was not calculated. As we studied Japanese only, results may not be generalized to other races or ethnicities.
In conclusion, higher circulating ORM and reduced glucose induced insulin secretion were evident in non-obese middle-aged Japanese subjects with prediabetes independently of general and abdominal adiposity and insulin resistance. It is suggested that subtle but chronic (for decades) hyperglycemia associated with elevated circulating ORM may be related to reduced glucose induced insulin secretion.
Acknowledgments
The authors thank all participants for their dedicated and conscientious collaboration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AT, KK, MY, MT, SM-I, MH, MK and BW collected and analyzed data. TK wrote the manuscript, and KF reviewed and edited it. All authors approved the final version of the manuscript to be published. TK supervised the study, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Mukogawa Women’s University Ethical Committee (No. 07–28 on February 19, 2008).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information. The ethical committee of the University does not allow us to open data except for a manuscript.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.