Article Text

Abstract
Introduction To determine if variations in the neonatal amygdala mediate the association between maternal antenatal glycemia and offspring adiposity in early childhood.
Research design and methods 123 non-obese pregnant women with no pregnancy complications aside from gestational diabetes underwent a 75 g 2-hour oral glucose tolerance test at 26–28 weeks’ gestation. Volume and fractional anisotropy (FA) of the neonatal amygdala (5–17 days old) were measured by MRI. The Body Mass Index (BMI) z-scores and sum of skinfold thickness (subscapular and triceps) of these children were tracked up to 60 months of age (18, 24, 36, 48, 54 and 60 months).
Results Maternal fasting glucose levels were positively associated with the offspring’s sum of skinfold thickness at age 48 months (β=3.12, 95% CI 0.18 to 6.06 mm) and 60 months (β=4.14, 95% CI 0.46 to 7.82 mm) and BMI z-scores at 48 months (β=0.94, 95% CI 0.03 to 1.85), 54 months (β=0.74, 95% CI 0.12 to 1.36) and 60 months (β=0.74, 95% CI 0.08 to 1.39). Maternal fasting glucose was negatively associated with the offspring’s FA of the right amygdala (β=−0.019, 95% CI −0.036 to −0.003). Right amygdala FA was negatively associated with the sum of skinfold thickness in the offspring at age 48 months (β=−56.95, 95% CI −98.43 to −15.47 mm), 54 months (β=−46.18, 95% CI −88.57 to −3.78 mm), and 60 months (β=−53.69, 95% CI −105.74 to −1.64 mm). The effect sizes mediated by right amygdala FA between fasting glucose and sum of skinfolds were estimated at β=5.14 (95% CI 0.74 to 9.53) mm (p=0.022), β=4.40 (95% CI 0.08 to 8.72) (p=0.049) mm and β=4.56 (95% CI −0.17 to 9.29) mm (p=0.059) at 48, 54 and 60 months, respectively.
Conclusions In the offspring of non-obese mothers, gestational fasting glucose concentration is negatively associated with neonatal right amygdala FA and positively associated with childhood adiposity. Neonatal right amygdala FA may be a potential mediator between maternal glycemia and childhood adiposity.
- diabetes
- gestational
- brain
- growth
Data availability statement
Data are available upon reasonable request
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Maternal hyperglycemia increases risk of offspring adiposity later in life.
What are the new findings?
Maternal fasting glucose was negatively associated with the offspring’s fractional anisotropy (FA) of the right amygdala, a brain region that regulates appetite and feeding behavior.
Right amygdala FA was negatively associated with sum of skinfold thickness in the offspring at age 48, 54 and 60 months.
Mediation analyses suggest neonatal right amygdala FA may be a potential mediator between maternal glycemia and childhood adiposity.
How might these results change the focus of research or clinical practice?
This is a novel pathway by which maternal hyperglycemia can potentially contribute to subsequent risk of offspring adiposity.
Introduction
Obesity and gestational diabetes pose major public health challenges as their prevalence increase rapidly worldwide.1 2 Maternal hyperglycemia not only results in excessive fetal growth3 but can also predispose the offspring to risk of adiposity later in life.4–7 Indeed, our study group has previously shown that antenatal fasting glucose was significantly associated with offspring adiposity8 among non-obese women, which was consistent with previous findings.9 Metabolic imprinting and epigenetic modification have been suggested to contribute to childhood obesity.10 11 Some studies have used MRI in neonates and infants to study offspring adiposity. One study observed that the volume of brain region like the insula is inversely related to percentage body fat in babies from birth to 6 months postpartum,12 while another reported negative association between maternal adiposity (a risk factor of offspring adiposity) and global as well regional fractional anisotropy (FA) in neonates.13 However, little research has examined if the brain regions which regulate appetite and feeding behavior may play a role in offspring adiposity associated with maternal glycemia.
Food intake is regulated by hormones14 and neural signals, with most studies focusing on the hypothalamus.15 16 Animal studies have shown that amygdala lesions can affect appetite, food intake (ie, hyperphagia) and weight gain.17–20 Many human studies support that the amygdala may be an important site for food intake regulation21 and may be linked to obesity.22–24 Children who exhibited greater brain response in anticipation of food relative to money, within the appetite-related regions such as the amygdala, also ended up having more food intake.25 Graham et al26 demonstrated that greater neonatal right amygdala volume and connectivity were associated with lower impulse control for a snack delay task at 2 years of age. Indeed, the amygdala volume has been previously linked to preference for fat intake in young adults27 as well as Body Mass Index (BMI) in young adults28 and children.23 24 Functional MRI (fMRI) of obese children demonstrated hyper-responsiveness to food rewards in their amygdala compared with normal-weight children.29 Schur et al30 showed that obese children (9–11 years old) with greater reduction in brain activity in the appetite-processing brain regions (including the amygdala), when shown visual cues of high calorie foods, had greater BMI z-score reduction. Others have observed increased amygdala connectivity with the ventromedial prefrontal cortex in lean individuals compared with obese adult participants.31 The amygdala is susceptible to maternal environment during early development.32–35
However, to date, most studies have emphasized on peripheral metabolism, with little focus on the possibility that in utero maternal effects may be associated with neural mechanisms that regulate energy imbalances associated adiposity. Maternal hyperglycemia has been shown to have long-term effects in the offspring neurodevelopment,36 37 with a lot of focus on memory function in infants38–40 due to the pathophysiology of maternal hyperglycemia (fetal hyperglycemia, fetal hypoxemia and iron deficiency).41 Gestational diabetes has been linked to increased fetal hypothalamic activation towards glucose42 and slower fetal postprandial brain responses.43 Maternal insulin sensitivity, in the absence of gestational diabetes, was also associated with slower fetal brain responses.44 Animal studies showed that regions of the brain, such as the striatum and hippocampus, are vulnerable to prenatal iron deficiency.45 46 However, to the best of our knowledge, little is known about maternal glycemia and how it affects neonatal amygdala. In this study, we examined if variations in the neonatal amygdala, in terms of its volume and FA, mediate the association between maternal glycemia and offspring adiposity. The amygdala volume is a measurement of amygdala size, while FA is used to characterize the microstructure organization of the amygdala.47 We will focus on offspring of non-obese women, as we have previously shown that maternal fasting glucose and offspring adiposity are significantly associated in these women.8 It has been suggested that the effect of maternal glycemia on offspring adiposity is pronounced in non-obese women as maternal obesity shares common biological pathways with hyperglycemia, and presence of maternal obesity may attenuate the association between maternal glycemia and offspring adiposity.48 49 We hypothesize that higher antenatal fasting blood glucose levels may be associated with decrease in volume and FA of the neonatal amygdala, which mediate the positive association between maternal glycemia and offspring adiposity in non-obese mothers. We did not hypothesize that there will be any association between 2-hour postoral glucose tolerance test (OGTT) glucose levels and offspring adiposity measures, in view of earlier null findings in the first 3 years of life, by our study group.8 This study benefited from the unique opportunity to assess neonatal brain structure at birth and a prospective, longitudinal follow-up of growth.
Reseach design and methods
Participants
Pregnant women were recruited in their first trimester from the KK Women’s and Children’s Hospital and National University Hospital in Singapore between June 2009 and September 2010 to participate in the Growing Up in Singapore Towards Healthy Outcomes birth cohort study.50 The children were born either at KK Women’s and Children’s Hospital or National University Hospital between November 2009 and May 2011.
Recruitment of neonates for MRI was previously described.51 Neonatal brain MRI was done between 5 and 17 days after birth in 189 singleton, naturally conceived neonates,52 who all went through the T2-weighted MRI scans. A subset of 124 neonates had diffusor tensor imaging (DTI) scans. Participants with poor image quality were excluded due to large head motion that caused misalignment across slices in T2-weighed MRI and signal loss in DTI (T2-weighted scans: n=7, DTI: n=2). Twenty-one neonates were excluded because they were part of multiple birth and/or had a gestational age of <37 weeks, birth weight of <2500 g, a 5 min Apgar score of <9, born to mothers with pregnancy complications other than gestational diabetes (eg, pre-eclampsia, intrauterine growth retardation and type II diabetes). Eight were excluded because they did not have antenatal maternal blood glucose data, and another 30 neonates were excluded as their mothers had a first trimester BMI of ≥30 kg/m2. A total of 123 mother–child dyads (T2-weighted: n=123, DTI: n=89) were included in this analysis. All this information is summarized in online supplemental figure 1.
Supplemental material
Oral glucose tolerance test
At 26–28 weeks’ gestation, all the women who came for the clinic visit were offered the 75 g OGTT, after overnight fasting. Blood glucose levels were measured at fasting and 2-hour postglucose test. The 1999 WHO diagnostic criteria53 were used to diagnose gestational diabetes mellitus (GDM): ≥7.0 mmol/L for fasting glucose and/or≥7.8 mmol/L for 2 hour post-glucose. Women diagnosed with GDM were treated as per standard hospital protocol.
MRI acquisition and analysis
MRI acquisition in neonates was previously detailed in Qiu et al.52 In brief, neonates underwent fast spin-echo T2-weighted MRI and single-shot echo-plan DTI scans using a 1.5-Tesla GE scanner (GE Healthcare) at the KK Women’s and Children’s Hospital between 5 and 17 days after birth. The neonates were scanned while they were asleep and immobilized using an immobilization bag, without any sedation. The imaging protocols were (1) fast spin-echo T2-weighted MRI (repetition time (TR)=3500 ms, echo time (TE)=110 ms, field of view (FOV)=256×256 mm, matrix size=256×256, 50 axial slices with 2 mm thickness) and (2) single-shot echo-planar DTI (TR=7000 ms, TE=56 ms, flip angle=90°, FOV=200×200 mm, matrix size=200×200, 40–50 axial slices with 3 mm thickness, 19 diffusion-weighted images (DWIs) with b=600 s/mm2; one baseline image with b=0 s/mm2). For T2-weighted MRI, 50 axial slices with 2 mm thickness were acquired parallel to the anterior–posterior commissure line. Two T2-weighted images were acquired per subject. For DTI, 40–50 axial slices with 3 mm thickness were acquired parallel to the anterior–posterior commissure line. Nineteen DWIs with b=600 s/mm2 and 1 baseline with b=0 s/mm2 were obtained.
The delineation of the amygdala was done automatically using Markov random field (MRF).54 We also randomly selected 20 T2-weighted MRI datasets for manual delineation, and the intraclass correlation was 0.77. The leave-one-out validation approach was also used to confirm the MRF accuracy of the amygdala segmentation, and the accuracy was found to be 0.75. The volume of the amygdala was calculated by multiplying the number of voxels in the structural mask and the image resolution.
The DTI analysis was described in detail previously.35 Briefly, geometric distortion of the DTI due to B0-susceptibility differences across the brain was corrected as per Huang et al.55 The diffusion tensor was derived by multivariate least-squares fitting. FA was computed based on the three eigenvalues of the tensor. The mean FA was calculated within the amygdala mask for individual participants when the amygdala mask in the T2-weighted images was applied.
Child anthropometric measurements
All child anthropometric measurements were obtained as previously described.56 The child’s weight and height were measured at ages 18, 24, 36, 48, 54 and 60 months (online supplemental figure 1). Sex-specific and age-specific BMI z-scores were derived using weight measurements and either length at 18 and 24 months or height measurements from 36 months onwards, with the WHO Anthro macro V.3.2.2.57 Skinfold thicknesses (triceps and subscapular) were measured at birth and at 18, 24, 36, 48, 54 and 60 months using Holtain skinfold calipers (Holtain, Crymych, UK). The sum of skinfold is the summation of triceps and subscapular skinfold thickness.
Additional data
Demographic data such as ethnicity, maternal age and education, as well as breastfeeding duration information, were collected with interviewer-administered questionnaires. At 26–28 weeks’ gestation, participants came for a clinic visit where their height and weight were measured and BMI was derived. They were also given a self-administered Edinburgh Postnatal Depression Scale (EPDS) questionnaire to fill in to assess their mood. Birth outcomes (eg, birth weight, sex of child and Apgar score) were recorded by midwives at delivery. BMI at the first trimester and GDM treatment were obtained from the medical records.
Statistical analysis
Independent t-test and χ2 test were used to compare the neonatal and maternal characteristics of participants. Linear regression models were run to assess the associations between (1) maternal blood glucose levels (predictor: fasting or 2-hour post-OGTT) and child anthropometric measurements (outcome: BMI z-scores or sum of skinfold thickness), and (2) maternal blood glucose level(s) (predictor: blood glucose level(s) significantly associated with child anthropometric measurement in (1) and amygdala measurements (outcome: volume or FA), amygdala measurements (predictor: amygdala measurement significantly associated with maternal blood glucose levels in (2) and child anthropometric measurements (outcome: BMI z-scores or sum of skinfold thickness). All regression models were adjusted for ethnicity, maternal age, maternal education, EPDS score and maternal BMI at 26–28 weeks’ gestation. Household income was not included in the model due to the high correlation with maternal education. Our group has shown previously58 that maternal glycemia was positively associated with offspring birth weight. At the same time, other studies have shown that birth weight is an important marker associated with structural differences throughout the brain,59 as well as childhood adiposity and obesity.60 Thus, birth weight may potentially lie on the causal pathway between maternal glycemia and child adiposity, as well as between maternal glycemia and neonatal amygdala. Conditioning on birth weight in these analyses could potentially introduce collider-stratification bias61; hence, birth weight is not included in the model. For all models involving child anthropometric measurements, only one anthropometric measurement (BMI z-scores or sum of skinfold thickness) was included each time. Likewise, for all models involving maternal blood glucose level, only one blood glucose concentration (fasting or 2-hour post-OGTT) was included each time. For models with skinfold thickness as outcomes, sex of the child and age at anthropometric measurement were added as additional covariates. This was not done for models with BMI z-scores as outcomes since the z-scores were already derived based on sex and age at measurement. For models involving amygdala measurements, postconceptual age at MRI visit (gestational age+age at MRI visit) and total brain volume were included as additional covariates. These covariates were chosen because they are known to affect maternal metabolism, amygdala microstructure and/or offspring adiposity. For example, we adjusted for antenatal EPDS as it was previously found by our group to affect the amygdala microstructure.35 Before testing for mediation, potential interactions between fasting blood glucose and amygdala measurements on offspring adiposity were checked using the general linear model. Mediation effect by the amygdala was estimated by regression-based mediation62 using the PARAMED macro63 in STATA version 14, which uses a counterfactual-based approach to mediation. Data were missing on maternal education in 0.8% (n=1), antenatal EPDS score in 5.7% (n=7) and 26 weeks’ BMI in 1.6% (n=2) of the participants included in this analysis. Listwise deletion was used to handle missing data. Missing variables were found to be missing completely at random by Little’s Missing Completely At Random (MCAR) test. In view of our relatively small sample size, no multiple comparison correction was applied for all analyses to minimize type II error,64 to avoid missing out potential important findings.
Sensitivity analyses were done with additional adjustment for GDM treatment and breastfeeding duration, on top of the covariates listed previously. The results were similar and therefore were not presented. All analyses were carried out by using SPSS V.24.0 unless otherwise stated.
Data and resource availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Results
Participant characteristics
One hundred and twenty-three mother–child dyads were included in this analysis; these participants were comparable with those who did no undergo MRI, in terms of sex distribution of offspring and fasting blood glucose levels (table 1). However, neonates included in this study had greater gestational age, higher birth weight and more likely to be of Malay ethnicity. The mothers were younger, less likely to have university or higher education, and had higher EPDS scores. They also had lower first trimester and late second trimester BMI, lower 2-hour post-OGTT blood glucose levels and were less likely to be diagnosed with GDM. Of the 123 women included in this analysis, 14 were diagnosed with GDM, of which 3 (21.4%) did not undergo any treatment; 10 (71.4%) had dietary counselling; and 1 (7.1%) received insulin treatment.
Maternal and child characteristics of participants
Maternal blood glucose levels and childhood adiposity
We observed that maternal antenatal fasting glucose was positively associated with the offspring’s sum of skinfold thickness at age 48 months (β=3.12, 95% CI 0.18 to 6.06 mm) and 60 months (β=4.14, 95% CI 0.46 to 7.82 mm) (figure 1A) and BMI z-scores at 48 months (β=0.94, 95% CI 0.27 to 1.61), 54 months (β=0.74, 95% CI 0.12 to 1.36) and 60 months (β=0.74, 95% CI 0.08 to 1.39) (figure 1B) in offspring of non-obese mothers. A similar positive trend was observed with sum of skinfold thickness at 54 months (β=2.85, 95% CI −0.04 to 5.74 mm). No obvious trends were observed between fasting glucose and childhood adiposity measurements in the earlier time points between 18 and 36 months of age. No significant associations were observed between maternal 2-hour post-OGTT glucose levels and offspring adiposity measures (online supplemental table 1).
Supplemental material
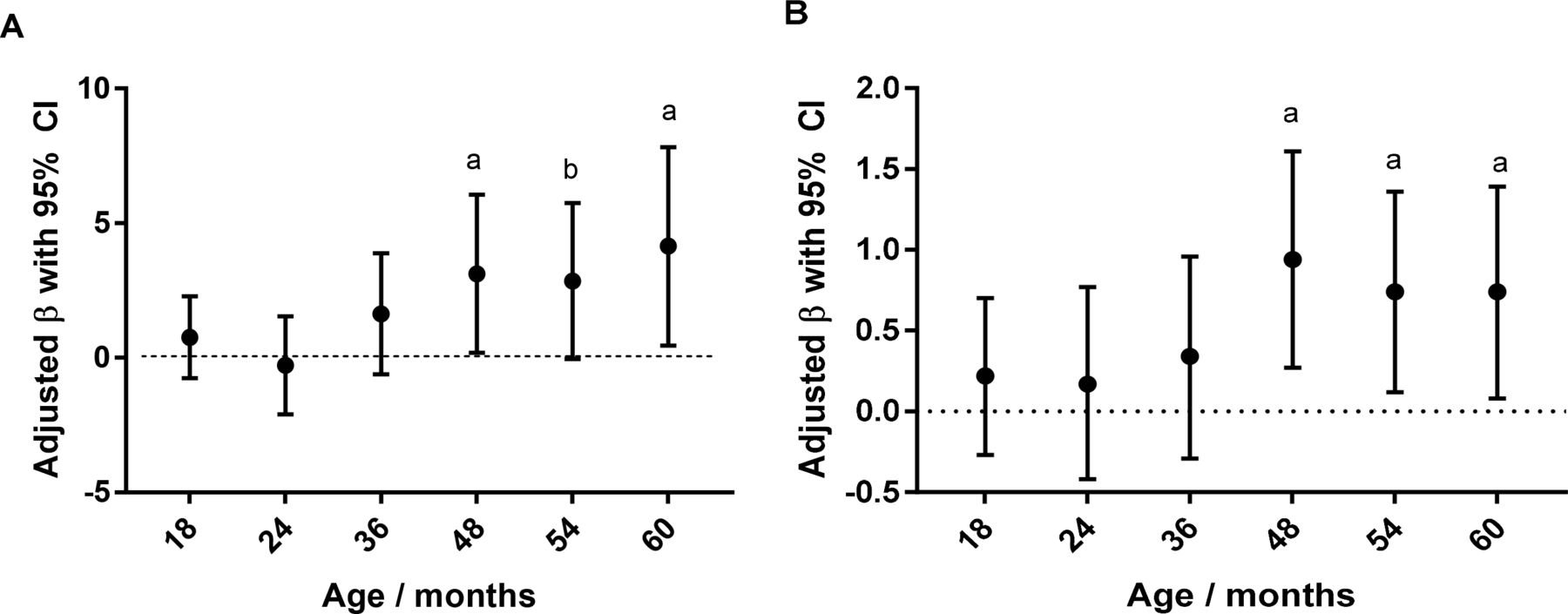
Adjusted regression coefficient (with 95% CI) of maternal antenatal fasting blood glucose levels (per 1 mmol/L) on child adiposity measures in the first 60 months of life for offspring of non-obese mothers. (A) Sum of skinfolds (triceps and subscapular) (mm) and (B) Body Mass Index z-scores. aP<0.05, bP<0.10.
Maternal fasting glucose levels and neonatal amygdala microstructure
The mean and SD of the amygdala volume and FA of the left and right hemispheres are 214±32 mm3, 0.15±0.02, and 187±32 mm3, 0.16±0.03, respectively. A higher maternal fasting glucose level was associated with a significantly lower FA of the right amygdala in the offspring (table 2) of non-obese women. A similar trend was observed in the left amygdala FA but did not reach statistical significance (table 2). Maternal fasting glucose was not significantly associated with the amygdala volume (table 2).
Associations of maternal antenatal fasting blood glucose concentrations with volume and FA of the neonatal amygdala in offspring born to non-obese women
Neonatal amygdala FA and childhood adiposity
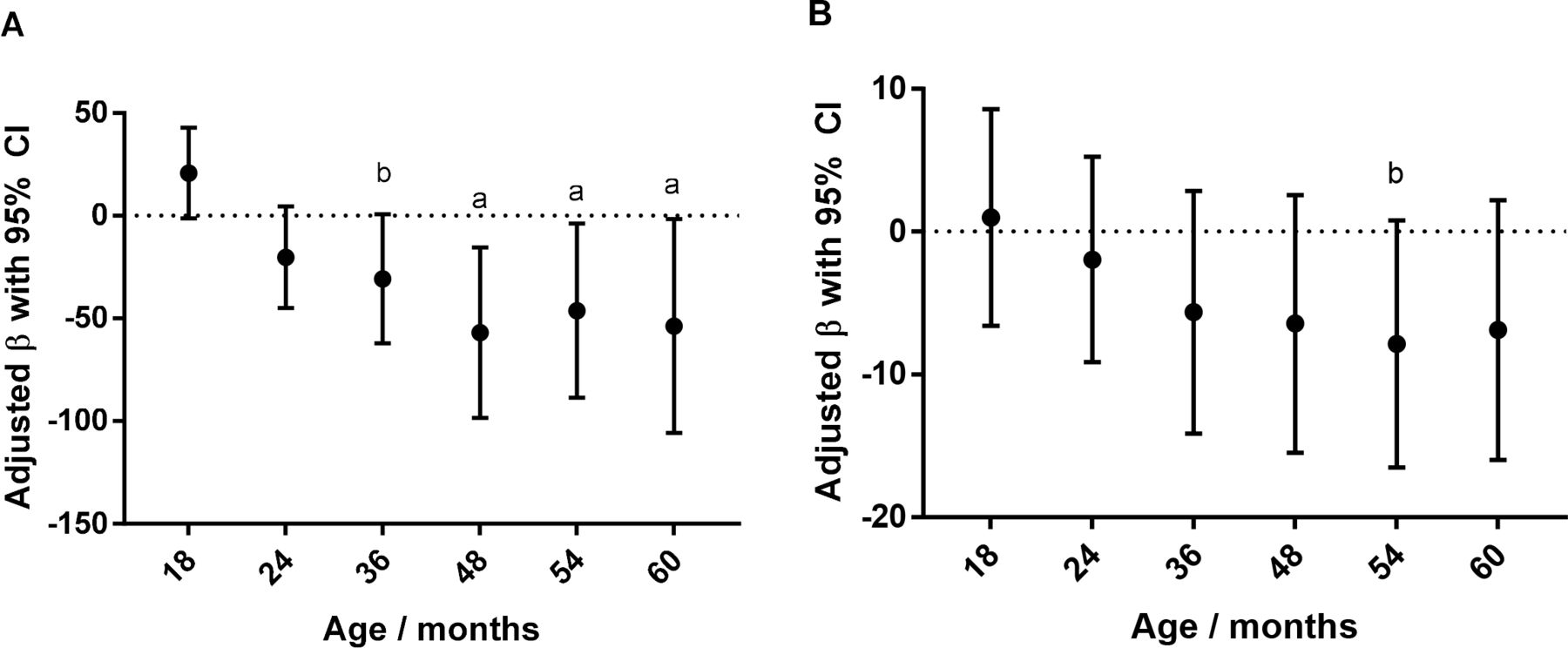
Figure 2 shows the association of the right amygdala FA and adiposity measures, including the sum of skinfold thickness (figure 2A) and BMI z-scores (figure 2B) up to 60 months. The neonatal right amygdala FA was negatively associated with the sum of skinfold thickness at 48 months (β=−56.95, 95% CI −98.43 to −15.47 mm), 54 months (β=−46.18, 95% CI −88.57 to −3.78 mm) and 60 months (β=−53.69, 95% CI −105.74 to −1.64 mm) (figure 2A). For BMI z-scores, although there was no significant association, the same negative pattern was observed (figure 2B).

{kind=link}
{kind=link}
Adjusted regression coefficient (with 95% CI) of neonatal right amygdala fractional anisotropy on child adiposity measures in the first 60 months of life for offspring of non-obese mothers. (A) Sum of skinfolds (triceps and subscapular) (mm) and (B) Body Mass Index z-scores. aP<0.05, bP<0.10.
Mediation by the right amygdala FA on maternal fasting glucose-linked childhood adiposity
Significant interaction was observed between maternal fasting glucose and the right amygdala FA on sum of skinfolds (48 months: p=0.005, 54 months: p<0.001, and 60 months: p=0.027). This exposure–mediator interaction was taken into consideration in the regression-based mediation. The effect sizes mediated by the right amygdala FA between fasting glucose and sum of skinfolds were estimated at β=5.14, 95% CI 0.74 to 9.53 mm (p=0.022); β=4.40, 95% CI 0.08 to 8.72 mm (p=0.049); and β=4.56, 95% CI −0.17 to 9.29 mm (p=0.059) at 48, 54 and 60 months, respectively (table 3). In other words, the effects of 1 mmol/L change in maternal fasting glucose on offspring skinfolds that are attributed to variations in neonatal amygdala FA are 5.14, 4.40 and 4.56 mm at ages 48, 54 and 60 months, respectively.
Estimated effect mediated by neonatal right amygdala FA in the association between antenatal fasting blood glucose and offspring adiposity
The proportions of total effect contributed by the mediator were estimated to be 0.65, 0.68 and 0.52 at 48, 54 and 60 months, respectively (table 3). No significant mediation by the right amygdala FA was found between fasting glucose and BMI z-scores score up to 60 months of age, although a marginal trend was observed at 54 months with β=0.47 (95% CI −0.09 to 1.03) (p=0.097) (table 3).
Discussion
We found that higher maternal antenatal fasting glucose concentrations were associated with increased sum of skinfolds in the offspring of non-obese Asian women, at 48 and 60 months, as well as higher offspring BMI z-scores at 48, 54 and 60 months. Increased maternal antenatal fasting glucose concentrations were also correlated with lower FA in the right amygdala. The right amygdala FA was, in turn, negatively associated with offspring skinfold thicknesses from 48 months onwards. Mediation analyses suggest that right amygdala FA may be a potential mediator in the pathway between maternal antenatal fasting glucose and offspring adiposity as measured by the sum of skinfold thicknesses.
The amygdala is linked to food intake and obesity.21 22 65 The human amygdala is known to respond to food cues,66 67 and amygdala responses have been associated with subsequent consumption of high-fat food.68 Amygdala volume has also been associated with fat intake27 in adolescents and BMI in young adults28 and children,23 24 while increased amygdala connectivity with ventromedial prefrontal cortex has been observed in lean individuals compared with obese adult participants.31 Greater neonatal right amygdala volume and connectivity have also been associated with lower impulse control for a snack delay task at 2 years of age.26 fMRI of obese children showed hyper-responsiveness to food rewards in their amygdala compared with normal-weight children.29 Lower FA has been previously reported in many brain regions of obese individuals (elderly, adults and children),69 70 including brain regions involved in appetite, inhibitory control and reward such as amygdala.71 While a couple of studies have observed a positive association between both right and left amygdala volume and BMI or obesity,24 72 we found a correlation only with the right side of the amygdala, similar to Orsi et al,28 who reported a correlation between the right amygdala volume and BMI. Another study also showed right amygdala volume and connectivity to be linked to poorer impulse control for a food task in 2-year-old toddlers.26 Although we do not have a full explanation of the lateralization differences, differences in hemispheric processing between left and right amygdalae have been previously suggested in humans73 and animals.74 van der Laan et al75 found that hunger modifies the activation of the right amygdala towards images of food.
Overall, while we observed a similar trend with both measurements of adiposity, we had more consistent findings with the sum of skinfolds, which is a surrogate for total adiposity. BMI has been regarded as a more crude measurement of adiposity as it can be influenced by fat free mass, especially in children.76 It is noteworthy that previous studies showed associations between the amygdala and BMI in adolescents or older adults.27 28 31
Our group8 and others7 77 previously reported higher antenatal fasting glucose to be associated with greater adiposity in children, particularly those born to non-obese mothers. In fact, our group has also examined longitudinal effect of antenatal fasting glucose on weight and BMI trajectory in the offspring and has shown that higher antenatal fasting glucose is positively associated with weight and BMI trajectory in the first 36 months among offspring of non-obese mothers.8 We did not observe a significant association between 2-hour post OGTT glucose and offspring adiposity, possibly because of the large variation in 2-hour OGTT glucose; hence, there was a likelihood of larger errors. Moreover, 2-hour OGTT blood glucose may be attenuated through exaggerated glucose steal due to fetal hyperinsulinemia,78 a condition in the offspring of mothers with hyperglycemia, which is also a driver of fetal fat accretion. As a result, some mothers may have ‘normal’ glucose tolerance even though their offspring may exhibit diabetic fetopathy.78 Maternal obesity and hyperglycemia share common biological pathways such as state of inflammation, impairment in regulation of energy and excess of fuel substrates.48 49 Hence, maternal obesity may reduce the independent association observed between maternal glycemia and offspring adiposity. Our results also showed that significant differences in maternal glycemia associated offspring become apparent from 48 months of age onwards. This is consistent with earlier reports of null findings at 2 years of age79 and a study of women with overt diabetes during pregnancy, where the maternal hyperglycemia-related obesity resolved within first 1–2 years of life.80 Many studies showed that the association between maternal diabetes and offspring obesity recurs at a later part of childhood.5 81–83 This is not surprising if food intake and response to food cues are involved. During infancy and toddlerhood, food choices and portion size are largely determined by parents and caregivers, while older children have more autonomy in food choices and portion sizes when they start attending preschool.
The prospective nature of our study is a strength as we examined the association of in utero glucose exposure on the microstructure of the neonatal amygdala and subsequent adiposity in toddlerhood and early childhood. We are also, to the best of our knowledge, among the first to study the mediating role of differences in the amygdala, in the pathway between maternal glycemia and offspring adiposity. Another strength of our study is the large number of covariates considered, including maternal mental well-being. A limitation of our study is the small number of participants, which limited our statistical power. Replication of this study with a larger sample size is necessary. We also recognize that the blood glucose levels were measured once during pregnancy and may not be representative of the in utero exposure throughout pregnancy, especially post-GDM diagnosis and treatment. Insulin levels were also not measured during the OGTT; as such, we were unable to study maternal insulin sensitivity in relation to neonatal amygdala or child adiposity. We acknowledge that a large number of outcomes were investigated and we did not adjust for multiple comparisons; hence, we cannot rule out the possibility of chance findings. However, the findings were in the same direction for both BMI z-scores and sum of skinfolds and consistently at similar time points. We acknowledge that there could be potential selection bias in the participants who agreed to undergo the MRI and were included in this study. For example, they were more likely to be older, have lower education, more depressed and of lower BMI. However, these factors were adjusted, where appropriate, in our analysis.
Conclusions
Our study shows that maternal blood glucose level during pregnancy is associated with early childhood adiposity, and this may be mediated by differences in the microstructure of the amygdala, a brain structure implicated in feeding behaviors. These findings provide a novel pathway by which antenatal maternal blood glucose might influence the later risk of adiposity in the offspring.
Supplemental material
Supplemental material
Data availability statement
Data are available upon reasonable request
Ethics statements
Ethics approval
This study was approved by the institutional review board of the Singapore National Healthcare Group (B/2014/00411) and the centralized institutional review board of SingHealth (2009/785/A).
Acknowledgments
We thank the staff and participants of the Growing Up in Singapore Towards Healthy Outcomes (GUSTO) study as well as members of the GUSTO study group. The GUSTO study group includes Allan Sheppard, Amutha Chinnadurai, Anne Eng Neo Goh, Anne Rifkin-Graboi, Arijit Biswas, Bee Wah Lee, Birit F.P. Broekman, Boon Long Quah, Borys Shuter, Chai Kiat Chng, Cheryl Ngo, Choon Looi Bong, Christiani Jeyakumar Henry, Cornelia Yin Ing Chee, Yam Thiam Daniel Goh, Doris Fok, Fabian Yap, George Seow Heong Yeo, Helen Chen, Hugo P S van Bever, Iliana Magiati, Inez Bik Yun Wong, Ivy Yee-Man Lau, Jeevesh Kapur, Jenny L. Richmond, Jerry Kok Yen Chan, Joanna D. Holbrook, Joshua J. Gooley, Keith M. Godfrey, Kenneth Kwek, Krishnamoorthy Niduvaje, Leher Singh, Lin Lin Su, Lourdes Mary Daniel, Mark Hanson, Mary Foong-Fong Chong, Mary Rauff, Mei Chien Chua, Mya Thway Tint, Neerja Karnani, Ngee Lek, Oon Hoe Teoh, P. C. Wong, Pratibha Agarwal, Rob M. van Dam, Salome A. Rebello, Seang-Mei Saw, Shang Chee Chong, Shu-E Soh, Sok Bee Lim, Chin Ying Stephen Hsu, Victor Samuel Rajadurai, Walter Stunkel, Wee Meng Han, Wei Wei Pang, Yin Bun Cheung and Yiong Huak Chan.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SC and AQ conceptualized the idea, analyzed the data and wrote the manuscript. All the other authors were involved in supervision of data collection, derivation/cleaning of the data and/or design of the cohort study. SC performed the statistical analysis for the paper and takes responsibility for the accuracy of the analysis. All authors critically reviewed the manuscript. AQ had full access to all of the data in the study and takes responsibility for the integrity of the data. AQ is the guarantor of this article.
Funding This research is supported by the Singapore National Research Foundation under its Translational and Clinical Research (TCR) Flagship Programme and administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC), Singapore - NMRC/TCR/004-NUS/2008; NMRC/TCR/012-NUHS/2014. Additional funding is provided by the Singapore Institute for Clinical Sciences, Agency for Science Technology and Research, Singapore. The funding organizations had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and the decision to submit the manuscript for publication.
Competing interests PDG, KMG, and Y-SC have received lecture fees from companies that sell nutritional products. They are part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, and Danone. KMG is supported by the UK Medical Research Council (MC_UU_12011/4), the National Institute for Health Research (NIHR Senior Investigator (NF-SI-0515-10042) and the NIHR Southampton Biomedical Research Centre) and the European Union (Erasmus+ Programme Early Nutrition eAcademy Southeast Asia-573651-EPP-1-2016-1-DE-EPPKA2-CBHE-JP). The other authors have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.