Article Text

Abstract
Introduction Associations of pre-pregnancy impaired fasting glucose (IFG) and body mass index (BMI) with large for gestational age (LGA) and preterm birth (PTB) have been poorly understood. We aimed to investigate the associations of maternal BMI, separately and together with pre-pregnancy IFG, with LGA and PTB in Chinese population. We also aimed to quantify these associations by maternal age.
Research design and methods This was a retrospective cohort study of women from the National Free Preconception Health Examination Project with singleton birth from 121 counties/districts in 21 cities of Guangdong Province, China, from January 1, 2013 to December 31, 2017. Women were included if they did not have pre-existing chronic diseases (diabetes, hypertension, etc). Participants were divided into eight groups according to their BMI (underweight (BMI <18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2), and obesity (≥28.0 kg/m2)) and pre-pregnancy fasting glucose status (normoglycemia (fasting glucose concentration <6.1 mmol/L) and IFG (6.1–7.0 mmol/L)). Adjusted incidence risk ratios (aIRRs) and 95% CIs of LGA, severe LGA, PTB and early PTB were estimated.
Results We included 634 030 women. The incidences of LGA, severe LGA, PTB and early PTB for the study population were 7.1%, 2.5%, 5.1% and 1.1%, respectively. Compared with normal weight mothers with normoglycemia, overweight and obese mothers irrespective of IFG had a higher risk of LGA (eg, obesity with IFG aIRR 1.85 (1.60–2.14)) and severe LGA (eg, obesity with IFG 2.19 (1.73–2.79)). The associations of BMI and pre-pregnancy fasting glucose status with LGA were similar found among women of all age groups. Underweight with normoglycemia had 6.0% higher risk of PTB (1.06 (1.03–1.09)) and 8.0% higher risk of early PTB (1.08 (1.02–1.17)), underweight with IFG had 14.0% higher risk of PTB (1.14 (1.02–1.27)), and obese mothers with IFG had 45.0% higher risk of PTB (1.45 (1.18–1.78)). The associations of BMI and pre-pregnancy fasting glucose status with PTB differed by maternal age.
Conclusion Overweight and obesity regardless of IFG were associated with an increased risk of LGA, and these associations were similarly observed among mothers of all age groups. Underweight regardless of IFG, and obesity with IFG were associated with an increased risk of PTB, but the associations differed by maternal age. Findings from this study may have implications for risk assessment and counselling before pregnancy.
- prediabetic state
- pregnancy
- high-risk
- body mass index
- cohort studies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Associations of pre-pregnancy impaired fasting glucose (IFG) and obesity with large for gestational age (LGA) and preterm birth (PTB) are controversial and inconclusive.
No study has investigated the joint associations of IFG and body mass index with LGA and PTB.
What are the new findings?
Overweight and obesity regardless of IFG were associated with an increased risk of LGA.
Underweight regardless of IFG, and obesity with IFG were associated with an increased risk of PTB.
How might these results change the focus of research or clinical practice?
This study indicates that assessing both body mass index and fasting glucose before pregnancy should be considered in further recommendations for adverse pregnancy outcomes prevention.
Introduction
Large for gestational age (LGA) is associated with multiple risks for both the mothers and the neonates. Short-term risks of LGA include an increase in intrauterine death rate, a higher probability of shoulder dystocia, obstetric brachial plexus injury and birth fractures.1 2 There are also long-term risks of LGA, such as obesity and chronic disease in later life.3 4 Preterm birth (PTB) is also a public health and clinical concern. It is the leading cause of death for children below 5 years of age globally.5 PTB complications are estimated to be responsible for 35% of deaths among neonates annually, and surviving preterm neonates are at higher risk of respiratory and neurodevelopmental complications.6 Both LGA and PTB are associated with significant costs to health services, and families of LGA and PTB often experience considerable psychological and financial hardship.7 8 These data highlight the critical and urgent need to identify risk factors for LGA and PTB.
Unlike non-modifiable risk factors, such as ethnicity and genetic predisposition, pre-pregnancy impaired fasting glucose (IFG) and body mass index (BMI) are potentially modifiable and preventable causes of adverse pregnancy outcomes.9 Pre-pregnancy IFG, a status of hyperglycemia before conception, is associated with increased levels of insulin, and obesity is characteristic of elevation of triglyceride levels and a concomitant transient reduction in high-density lipoprotein levels during the pregnancy, both of which could contribute to the risks of LGA and PTB. However, the associations of pre-pregnancy IFG and obesity with LGA and PTB are controversial and inconclusive. Although pre-pregnancy IFG or obesity was a risk factor for LGA and PTB in some studies,10 11 in others null12 13 or even inverse14 associations of pre-pregnancy IFG and obesity with LGA and PTB were noted. In addition, there was no study which has investigated the joint associations of IFG and BMI with LGA and PTB.
In this study, we used data of the National Free Preconception Health Examination Project (NFPHEP) from Guangdong Province to investigate the associations of pre-pregnancy IFG, alone and jointly with maternal BMI, with the risks of LGA and PTB. We also aimed to identify the effects of maternal age on the association of pre-pregnancy IFG and BMI with LGA and PTB, which are important to enable physicians to provide tailored advice and prenatal care to mothers before and during pregnancy, although the underlying mechanisms of maternal age on the associations of pre-pregnancy IFG and BMI with LGA and PTB have yet to be elucidated.
Methods
Study design and population
We conducted a retrospective cohort study of women who participated in the NFPHEP between January 1, 2013 and December 31, 2017, successfully became pregnant and then had pregnancy outcome from 121 counties/districts of 21 cities in Guangdong Province, China. The study design, organization and implementation have been described previously15 (online supplemental appendix 1). The study was executed jointly by Guangzhou Medical University and Guangdong Institute of Family Planning Science and Technology, in which the review boards determined that this study was exempt for ethical approval owing to the use of de-identified data.
Supplemental material
In the current analysis, women were eligible for inclusion if they measured fasting serum glucose (FSG) and weight and height before pregnancy. Because chronic diseases have a known impact on adverse pregnancy outcomes and are prone to take interventions before conception and during the pregnancy, women with self-reported anemia, hypertension, diabetes, heart disease, hepatitis B, epilepsy, thyroid disease, chronic nephritis and cancer were excluded; women with newly identified hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg) and newly identified diabetes (FSG≥7.0 mmol/L) were also excluded. We also excluded women with multiple births or post-term pregnancies (gestation age >42 weeks), and with outcomes of miscarriages, induced abortions, birth defects or stillbirths, as there are either no criteria to define LGA, or gestational age or birth weight is unavailable for these neonates.16
Exposure
BMI was calculated by dividing the weight in kilograms by the square of the height in meters and was classified into four categories based on the Chinese criteria17: underweight (BMI <18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2) and obesity (≥28.0 kg/m2). Based on WHO guidelines,18 IFG was defined as FSG concentration of 6.1 mmol/L or greater and lower than 7.0 mmol/L.11 Normoglycemia was defined as FSG concentration lower than 6.1 mmol/L. All the participants included were categorized into eight groups based on FSG categories and BMI categories.
Outcomes
The primary outcomes were PTB, early PTB, LGA and severe LGA. PTB was defined as births delivered at gestational age less than 37 weeks and early PTB as births delivered at gestational age less than 34 weeks. Gestational age was measured by ultrasound at the first trimester of pregnancy. Based on the international standards in the INTERGROWTH-21st Project,19 LGA was defined as birth weight by gestational age and gender beyond the 90th percentile, and severe LGA as birth weight by gestational age and gender beyond the 97th percentile.
Statistical analysis
Mean and SD were reported for continuous variables, and frequencies and percentage were reported for categorical variables. Statistical interactions between BMI (four categories) and maternal pre-pregnancy IFG (yes or no) on PTB, early PTB, LGA and severe LGA were assessed. As our data covered over the 4 -year period, in which there was a possibility that women with more than one pregnancy have been included, we employed log-binomial models with generalized estimating equations to estimate the adjusted incidence risk ratios (aIRRs) and 95% CIs of PTB, early PTB, LGA and severe LGA for women with different status of IFG and BMI. The reference group was normal weight with normoglycemia. In each outcome, three models were fitted.
In model 1, we adjusted for participants’ sociodemographic characteristics, including age at baseline, ethnicity, educational level, occupation, region and migrant population. In model 2, we additionally adjusted for history of pregnancy and history of adverse pregnancy outcomes, including first pregnancy (primipara), history of PTB, miscarriage, induced abortion, birth defects or stillbirth. In model 3, we additionally adjusted for the lifestyles of the women and the husband, including smoking status of husband before pregnancy and during the early stage of pregnancy, smoking and alcohol consumption of women before pregnancy and during the early stage of pregnancy, and passive smoking of women before pregnancy. Because infant’s sex is associated with PTB and early PTB, we also adjusted for this variable in all analysis of PTB and early PTB in addition to others listed (online supplemental table 1).20
Supplemental material
Stratified analysis was undertaken according to maternal age to explore potential disparities in the association of BMI and FSG with LGA and PTB. Because the number of women aged 35–39 years and 40–50 years were relatively small, we merged these two groups into one group in stratified analysis. In addition, we adjusted for the length of time from pre-pregnancy examination to the last menstrual period (continuous data) or the year participated NFPHEP (five categories) to examine the robustness of the association of IFG and BMI with the four outcomes.
Missing covariates were inputted by using the monotone logistic regression method based on other sociodemographic covariates by creating 50 imputed data sets.21 The significance level was set at 0.05 and all tests were two sided. Statistical analyses were conducted by using Stata (V.14.0; Texas USA).
Results
Participant characteristics
The selection of participants for this study is shown in online supplemental figure 1. After excluding women who had chronic diseases, and who had miscarriage, induced abortion, stillbirth or birth defect and had multiple births or post-term pregnancy, the analytic sample size comprised 634,030 participants. In total, 44.2% of the participants were from nine cities in the Pearl River Delta and 10.2% were migrant populations. The sample size and the proportion of the migrant population in each city are shown in online supplemental table 2. The age of the participants included in the study ranged from 19 to 50 years, the median age was 26 years (IQR 24–29) and 6.1% of the women were older than 35 years. In addition, 99.3% of the participants were Han ethnicity. Maternal characteristics with respect to pre-pregnancy status of FSG and BMI are shown in online supplemental table 3.
Supplemental material
Supplemental material
Supplemental material
Associations of IFG and BMI with LGA and severe LGA
The median length of time from pre-pregnancy examination to the last menstrual period was 3.1 months (IQR 1.7–5.2). Among 630,430 included singleton births, 44,901 births were LGA, and the LGA rate was 7.12% (95% CI 7.06% to 7.18%), ranging from 5.74% in underweight women with normoglycemia to 14.18% in obese women with IFG. Moreover, 15,936 births were severe LGA, and the severe LGA rate was 2.53% (2.49% to 2.57%), ranging from 2.07% in underweight women with normoglycemia to 5.82% in obese women with IFG (table 1). Statistically significant interactions were found between maternal pre-pregnancy IFG and BMI on both LGA (χ2=769.72, p<0.001) and severe LGA (χ2=301.20, p<0.001). In the fully adjusted model (model 3), for mothers with pre-pregnancy normoglycemia or IFG, the aIRRs for both LGA and severe LGA increased gradually as maternal BMI increased. For example, mothers who were obese with normoglycemia had 26.0% higher risk of LGA (aIRR 1.26; 95% CI 1.19 to 1.33) and 44.0% higher risk of severe LGA (1.44; 1.31 to 1.58). Obesity plus IFG had the highest risk of LGA (1.85; 1.60 to 2.14) and severe LGA (2.19; 1.73 to 2.79). In addition, underweight mothers with normoglycemia had a markedly lower risk of LGA (0.83; 0.81 to 0.85) and severe LGA (0.85; 0.81 to 0.89).
aRRs for LGA and severe LGA according to pre-pregnancy status of FSG and BMI
Associations of IFG and BMI with PTB and early PTB
Among 630,430 included singleton births, 32,294 were PTB, and the PTB rate was 5.09% (5.04% to 5.14%), ranging from 5.01% in normal weight women with normoglycemia to 7.55% in obese women with IFG. In addition, 7123 of 634,030 births were early PTB, and the early PTB rate was 1.12% (1.09% to 1.15%), ranging from 0.92% in overweight women with IFG to 1.31% in obese women with normoglycemia (table 2). Statistically significant interactions were found between pre-pregnancy IFG and BMI on PTB (χ2=36.16, p<0.001) but not on early PTB (χ2=13.16, p=0.068). The aIRRs for PTB and early PTB according to pre-pregnancy status of IFG and BMI are shown in table 2. In the fully adjusted model (model 3), compared with normal weight mothers with normoglycemia, underweight mothers with normoglycemia had 6.0% higher risk of PTB (1.06; 1.03 to 1.09) and 8.0% higher risk of early PTB (1.08; 1.02 to 1.17); underweight mothers with IFG had 14.0% higher risk of PTB (1.14; 1.02 to 1.27); and obese mothers with IFG had the highest risk of PTB (1.45; 1.18 to 1.78). In all the three models of PTB, early PTB, LGA and severe LGA, the aIRRs did not substantially change.
aRRs for PTB and early PTB according to pre-pregnancy status of FSG and BMI
Associations of IFG and BMI with LGA and PTB according to maternal age
The associations of pre-pregnancy FSG and BMI with LGA were similarly observed among all the age groups (figure 1). Obesity and overweight with normoglycemia or IFG were associated with increased risk of LGA among all the age groups, except for overweight with normoglycemia or IFG among mothers aged 19–24 years, while underweight with normoglycemia was inversely associated with LGA among all age groups.
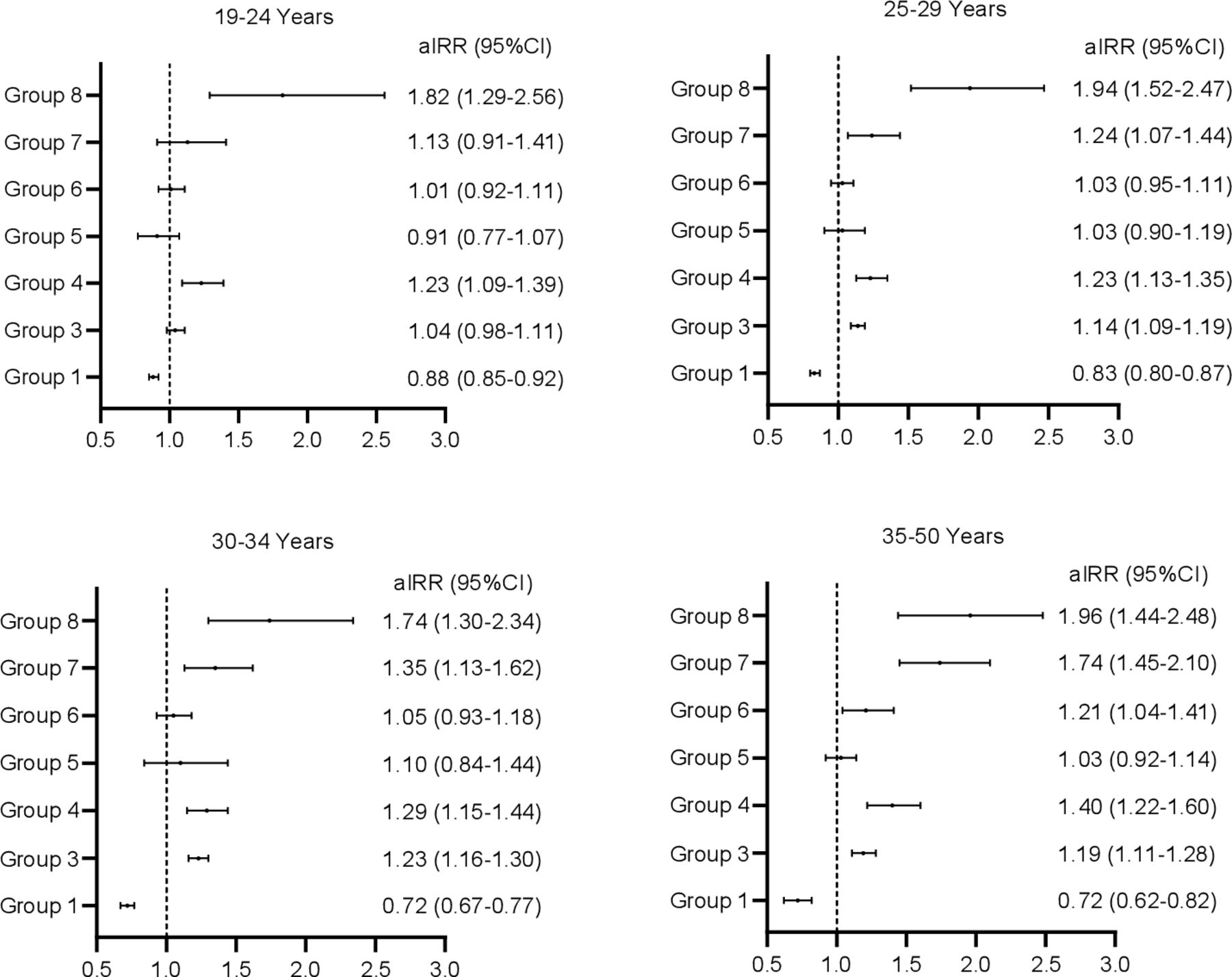
Association of IFG and BMI with risk of LGA by maternal age group. Pre-pregnancy status of FSG and BMI are defined as follows: group 1, underweight (BMI <18.5) plus normoglycemia (FSG <6.1 mmol/L); group 2, normal weight (18.5–24.0) plus normoglycemia; group 3, overweight (27.9≥BMI≥24) plus normoglycemia; group 4, obesity (BMI ≥28) plus normoglycemia; group 5, underweight plus IFG (7.0 mmol/L>FSG≥6.1 mmol/L); group 6, normal weight plus IFG; group 7, overweight plus IFG; group 8, obesity plus IFG. aIRR, adjusted incidence risk ratio; BMI, body mass index; FSG, fasting serum glucose; IFG, impaired fasting glucose; LGA, large for gestational age.
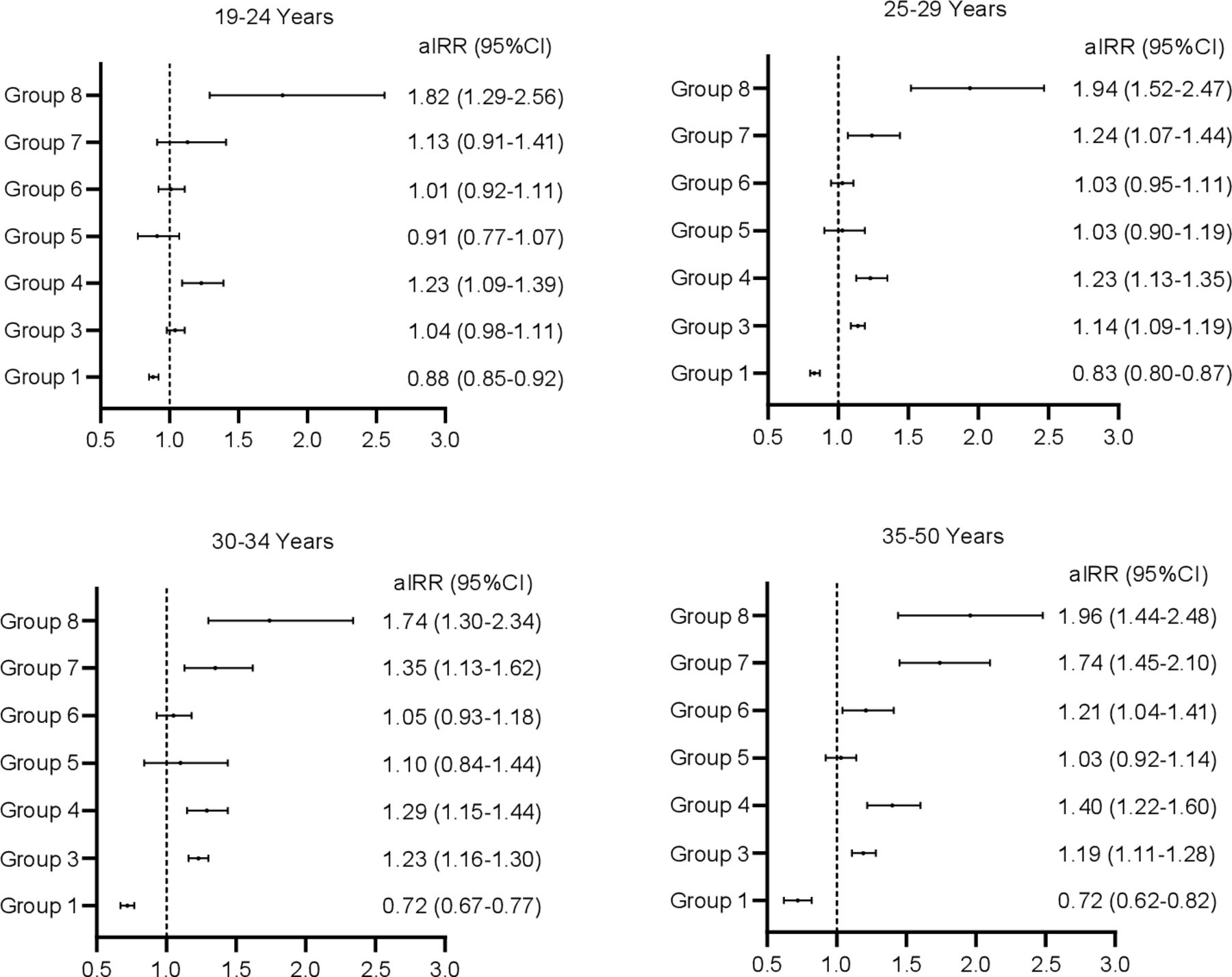
The associations of pre-pregnancy FSG and BMI with PTB differed by maternal age (figure 2). Stratified analysis showed that underweight with normoglycemia was associated with increased risk of PTB among mothers younger than 30 years, and underweight with IFG was associated with increased risk of PTB among mothers aged 19–24 years (1.24; 1.05 to 1.45). Obesity with normoglycemia was associated with increased risk of PTB among mothers aged 25–29 years (1.14; 1.01 to 1.28), and obesity with IFG was associated with increased risk of PTB among mothers younger than 30 years. Overweight with normoglycemia was only associated with increased risk of PTB among mothers aged older than 35 years (1.14; 1.03 to 1.26).

{kind=link}
{kind=link}
Association of IFG and BMI with risk of PTB by maternal age group. Pre-pregnancy status of FSG and BMI are defined as follows: group 1, underweight (BMI <18.5) plus normoglycemia (FSG <6.1 mmol/L); group 2, normal weight (18.5–24.0) plus normoglycemia; group 3, overweight (27.9≥BMI≥24) plus normoglycemia; group 4, obesity (BMI ≥28) plus normoglycemia; group 5, underweight plus IFG (7.0 mmol/L>FSG≥6.1 mmol/L); group 6, normal weight plus IFG; group 7, overweight plus IFG; group 8, obesity plus IFG. aIRR, adjusted incidence risk ratio; BMI, body mass index; FSG, fasting serum glucose; IFG, impaired fasting glucose; PTB, preterm birth.
Sensitivity analyses
In the sensitivity analyses, the association of pre-pregnancy FSG and BMI with the four outcomes did not substantially change with additional adjustment for the length of time from pre-pregnancy examination to last menstrual period or inclusion of the year participated NFPHEP (online supplemental table 4).
Supplemental material
Discussion
To our knowledge, this is the first study to investigate the associations for pre-pregnancy IFG, stratified by maternal BMI, with the risks of LGA and PTB. In this large cohort study conducted in China, with effect estimates for 5 years, we provide evidence of markedly increased risks for LGA and severe LGA after exposure to overweight or obesity with normoglycemia, and the risks were much higher for mothers who were overweight and obese with IFG; however, underweight with normoglycemia was inversely associated with the risks of LGA and severe LGA. The associations of IFG and BMI with LGA were similar among women of all age groups. In addition, risk of PTB was increased for underweight mothers regardless of IFG, and obese mothers with IFG had the highest risk of PTB. However, the associations of IFG and BMI with PTB differed according to maternal age.
In the context of pregnancy, insulin resistance is a critical normal pathophysiologic mechanism to ensure adequate energy supply for the growing fetus.22 However, among women with obesity, metabolic syndrome, and women with hyperglycemia or diabetes, the increasing insulin resistance demands of normal pregnancy place further burden on the maternal β cell to step up secretion. Unmet to this demand leads to excess glucose, lipid and amino acid exposure to the fetal-placental unit.23 This often leads to hyperinsulinemia that enhances fetal growth and an overabundance of maternal substrate for excess fetal fat accretion.24 In this study, we found the risk of LGA and severe LGA were much higher for overweight/obese mothers with pre-pregnancy IFG than overweight/obese mothers without IFG, probably because both obesity/overweight and pre-pregnancy IFG are associated with hyperglycemia and insulin resistance,25 26 leading to increased placental energy transfer and secretion of insulin in combination with an excess of triglyceride, leptin and adiponectin.27 It is noted that although IFG and BMI are interrelated, their associations with LGA or severe LGA are partially independent, and obesity/overweight alone accounts for more risk of LGA and severe LGA than pregnancies complicated by pre-pregnancy IFG alone.26 27 The associations of pre-pregnancy IFG and BMI with LGA were similar among all age groups, suggesting that the underlying mechanisms causing LGA are similar by age, and implied that weight loss or glucose control before pregnancy might be a preventive measure against LGA among obese/overweight or/and IFG women.
Findings from our study suggested markedly higher risk of PTB among underweight women regardless of IFG and among obese women with IFG, but no significant higher risk of PTB among obese women with normoglycemia, which were consistent with some studies conducted in low-income and middle-income countries,28 but inconsistent with studies conducted in developed countries.29 30 The discrepancy might be related to the different characteristics of the study population, for example, obese women in developed countries are prone to be hyperglycemia.28–30 In addition, although previous studies demonstrated that pre-pregnancy IFG had a higher risk of PTB,11 31 we did not find significant associations between normal weight/overweight with IFG and PTB, which may imply that risk of PTB among IFG mothers mainly derived from underweight and obesity.
Our findings showed that the associations of pre-pregnancy IFG and BMI with PTB differed by maternal age, which is similar to a previous study.29 In women aged 20 years or older, maternal overweight/obesity and IFG could increase the risk of gestational diabetes and pre-eclampsia, which might subsequently increase the risk of PTB.32 However, in China, women older than 30 years are more likely to be multipara (online supplemental table 5), who might have knowledge, experiences and skills against PTB.20 The risk of PTB differed by maternal age highlights that specific tailored recommendations for pregnancy according to maternal age are urgently needed to accurately stratify the risk of PTB, although more work is needed.29
Supplemental material
Strengths and limitations
The major strength of this study is the sample size. For this cohort, we recruited more than 634,000 women and followed up pregnancy outcomes with strict quality controls. The number of each exposure category and events per baseline variables were enough that the multivariable regression models were not over-fitted. The large sample size also allowed us to assess the effect of maternal age on the associations of pre-pregnancy IFG and BMI with LGA and PTB. The measurement of the exposures is the other major strength of the study that minimizes exposure misclassification—BMI was measured by calibrated instruments and IFG was measured by a fasting blood glucose test. Ascertaining these exposures prior to pregnancy is also a strength as compared with many studies that obtained pre-pregnancy weight from self-reports during pregnancy.33
The study has some limitations. First, we cannot identify whether the associations of pre-pregnancy IFG and BMI with LGA and PTB were modified by pregnancy complications (pre-eclampsia and gestational diabetes) because most of the participants (99.1%) did not test for gestational diabetes and pre-eclampsia. Women with pregnancy complications may lead to overestimate the effect of BMI and pre-pregnancy IFG on LGA and PTB, while women who have controlled the glucose level through lifestyle change may lead to underestimate the effect of pre-pregnancy IFG and BMI on the outcomes. Second, the NFPHEP did not collect data on the reason for each case of PTB, which precludes us from doing analyses for each subtype of PTB. Third, maternal BMI is only measured before pregnancy, thus we cannot adjust for weight gain in the analysis, although previous study suggested that weight gain did not substantially affect the association of pregnancy BMI with PTB.15 Third, we excluded women with pre-existing chronic diseases, including anemia, hypertension, diabetes, heart disease, hepatitis B, epilepsy, thyroid disease, chronic nephritis and cancer from our analysis, and thus our findings cannot be generalized to these populations, although these chronic diseases have a known impact on adverse pregnancy outcomes. Fourth, the study population have a higher rate of underweight and lower rate of obesity than that in western countries, which may limit the generalizability of our findings. Finally, although we have adjusted for many potential confounders, we cannot rule out the possibility of residual confounding by unknown factors.
Conclusion
In conclusion, in this large retrospective cohort study, pre-pregnancy overweight/obesity was associated with increased risk of LGA regardless of the pre-pregnancy IFG, and the associations were similar observed among mothers of all age groups. Pre-pregnancy underweight regardless of IFG was associated with increased risk of PTB, and the risk of PTB was highest among mothers who were obese with IFG. However, the associations of IFG and BMI with PTB differed by maternal age. These findings may have implications for future risk assessment and counseling to prevent adverse birth outcomes, although these findings need to be validated in a different population. These findings may also suggest that keeping normal BMI and normoglycemia before pregnancy may reduce the risk of LGA and PTB.
Acknowledgments
We thank Dr. Weiju Zhou, Faculty of Education, Health and Wellbeing, University of Wolverhampton, for his assistance in making figures. We also express our gratitude to all the community staff who participated in data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JT and QZ had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All the authors contributed to the conception, analysis and writing of the manuscript.
Funding This study was supported by the National Natural Science Foundation of China (81773457 and 81302445).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study proposal was approved by Guangzhou Medical University and Guangdong Institute of Family Planning Science and Technology, in which the review boards determined that this study was exempt for ethical approval owing to the use of de-identified data.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. None of the participant (de-identified) data collected in the study can be shared.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.