Article Text

Abstract
Introduction We investigated whether the presence of depressive symptoms among adults with diagnosed diabetes is associated with adverse quality of diabetes care.
Research design and methods The study population was drawn from the German national health survey ‘German Health Update’ 2014/2015-European Health Interview Survey and included 1712 participants aged ≥18 years with self-reported diabetes during the past 12 months. Depressive symptoms in the past 2 weeks were assessed by the eight-item depression module of the Patient Health Questionnaire (PHQ-8), with PHQ-8 sum score values ≥10 indicating current depressive symptoms. We selected 12 care indicators in diabetes based on self-reported information on care processes and outcomes. Associations of depressive symptoms with those indicators were examined in multivariable logistic regression models with stepwise adjustments.
Results Overall, 15.6% of adults with diagnosed diabetes reported depressive symptoms, which were higher in women than in men (18.7% vs 12.9%). Adjusted for age, sex, education, social support, health-related behaviors, and diabetes duration, adults with depressive symptoms were more likely to report acute hypoglycemia (OR 1.81, 95% CI 1.13 to 2.88) or hyperglycemia (OR 2.10, 95% CI 1.30 to 3.37) in the past 12 months, long-term diabetes complications (OR 2.30, 95% CI 1.55 to 3.39) as well as currently having a diet plan (OR 2.14, 95% CI 1.39 to 3.29) than adults without depressive symptoms. Significant associations between depressive symptoms and other care indicators were not observed.
Conclusions The present population-based study of adults with diagnosed diabetes indicates an association between depressive symptoms and adverse diabetes-specific care with respect to outcome but largely not to process indicators. Our findings underline the need for intensified care for persons with diabetes and depressive symptoms. Future research needs to identify underlying mechanisms with a focus on the inter-relationship between diabetes, depression and diabetes-related distress.
- diabetes complications
- depression
- quality of health care
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Clinical studies indicate that comorbid depression among persons with diabetes mellitus may adversely be associated with the course of the disease.
It is unclear whether this association is mediated by lower diabetes-related self-care and medical care utilization, especially in population-based studies.
What are the new findings?
Current depressive symptoms were associated with events of acute hypoglycemia or hyperglycemia in the past 12 months and diabetes-specific long-term complications, independent of potential confounders and based on a nationwide population-based survey.
Largely no associations were found with respect to self-care or medical care indicators, except for a higher chance of currently having a diet plan in persons with depressive symptoms.
A link between depressive symptoms and diabetes-related short-term or long-term outcomes via adverse care processes could not be supported.
How might these results change the focus of research or clinical practice?
The present population-based study confirms findings from clinical studies regarding adverse relations between depressive symptoms and care outcomes.
Our findings underline the need for intensified care for persons with diabetes and depressive symptoms.
For improved care, future research needs to disentangle the mechanisms underlying the link between depressive symptoms and diabetes complications, which may partly reflect the interaction with diabetes-related distress due to lower social and psychological resources.
Introduction
Diabetes is one of the leading causes of morbidity and mortality worldwide.1 2 Over the past three decades, global prevalence in adults has nearly doubled from 4.7% to 8.5%, mostly due to demographic changes and an increase in lifestyle-associated risk factors (eg, physical inactivity, obesity, smoking).3 Besides the burden of the disease in individuals, diabetes imposes a huge financial burden to healthcare systems; the estimated annual global health expenditures attributable to diabetes are estimated at over US$ 760 billion.4
Poorly controlled diabetes increases the likelihood of developing severe diabetes-specific complications such as kidney failure, vision loss or foot amputation,5 as well as comorbidities, in particular cardiovascular diseases,6 which may result in premature death.7 Therefore, early prevention and effective disease management are key factors in reducing the health and financial burden of diabetes.
Current clinical guidelines in Germany8 and in other countries9 recommend systematic screening for signs of depression among patients with diabetes, based on evidence that depression is more common in individuals with diabetes than without diabetes10–12 and is likely to adversely affect the course of the disease.13–15 Several previous studies have found that comorbid depression in diabetes is associated with specific indicators of lower self-care and treatment adherence,16–20 poor glycemic control,18 20–23 higher complication rates,13 24 and increased mortality.14 15 However, other studies could not show significant associations of depression with poor glycemic control25 26 and long-term complications.26 27 These conflicting findings may be due to differences in study design and population, as well as in assessments of depression and care indicators, which make comparisons of findings difficult. Most of these studies investigated only one single aspect of care (eg, self-care/medical care, treatment, glycemic control, complications) but not multiple aspects of care (ie, care processes and care outcomes) simultaneously in one study population. A recent clinical-based study indicated a link between depression and elevated hemoglobin A1c (HbA1c) values via self-care.20 With regard to epidemiological studies, it remains unclear whether the presence of depressive symptoms is associated with adverse outcomes among persons with diabetes, and whether this association may be, at least in part, mediated by care processes, particularly self-care processes. Therefore, based on a large nationwide population-based sample of adults with diabetes in Germany, the present study examined whether adults with and without depressive symptoms significantly differ with regard to diabetes-specific self-care or medical care processes, as well as to acute or long-term diabetes care outcomes, independent of potential confounders.
Research design and methods
Study design and data collection
The analysis was based on data from the nationwide cross-sectional health survey ‘German Health Update’ 2014/2015 (GEDA 2014/2015), which included the European Health Interview Survey (EHIS) core modules. This GEDA 2014/2015-EHIS survey was conducted by the Robert Koch Institute between November 2014 and July 2015 among a representative sample of persons aged 15 years and older with permanent residence in Germany.28 A two-stage stratified cluster sampling design was applied for the selection of survey participants (response rate 27.6%). In the first stage of sampling, primary sampling units (PSU) (ie, study locations) stratified for district and region size were selected from the list of municipalities in Germany to account for population size as well as regional population and employment density. In the second stage, age-stratified random samples proportional to the sex and age structure of the population in Germany were collected from local population registries within PSUs.
Data collection was based on a self-administered web questionnaire or a self-administered paper questionnaire. The GEDA 2014/2015-EHIS survey included the ‘European Health Interview Survey wave 2’ modules on health status, healthcare use, health determinants, and sociodemographic and psychosocial factors, as well as additional national questions. Data processing was conducted according to the quality and validation rules specified by Eurostat.
All participants were informed about the study’s aims and content, as well as about data protection, and provided their informed consent online (when using web questionnaire) or written (when using paper questionnaire) before study enrollment.
More details of the study design, sampling procedure, response rates and data collection have been published previously.28 29
Study population
In total, 24 824 participants completed the questionnaire, among them 24 016 adults (aged ≥18 years). In the ‘diseases’ module of the questionnaire, all participants were asked ‘During the past 12 months, have you had any of the following diseases or conditions?’ followed by a list of diseases which also included the item ‘diabetes (not including gestational diabetes)’; 23 345 participants had this information available.
Among those, 1712 participants (7.7%) answered ‘yes’, that is, reported the presence of diabetes mellitus (not including gestational diabetes) during the past 12 months, and thus comprised the study population for the present analyses.
Assessment of depressive symptoms
Depressive symptoms were assessed by a German version of the eight-item depression module of the Patient Health Questionnaire (PHQ-8), a self-rating scale measuring eight symptoms of depressive disorders (little interest or pleasure, depressed mood, sleep disturbances, tiredness or little energy, poor appetite or overeating, feelings of worthlessness or guilt, trouble concentrating, psychomotor retardation or agitation) from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition.30 Each of these eight symptoms was rated regarding its presence and frequency during the past 2 weeks on a scale between 0 (not at all), 1 (several days), 2 (more than half of the days) and 3 (nearly every day), leading to a sum score value between 0 and 24.
A sum score value between 10 and 24 was considered to indicate current depressive symptoms.30 For sensitivity analyses, we divided persons with depressive symptoms into two groups of moderate (sum score value 10–14) and severe (sum score value 15–24) depressive symptoms.
Furthermore, participants were asked whether they had consulted a psychologist, psychotherapist or psychiatrist in the past 12 months (coded as ‘yes’ and ‘no’). This information was used as proxy for mental healthcare utilization in a sensitivity analysis.
Assessment of care indicators
Overall, quality of care is a complex and multidimensional construct and can be classified into the dimensions ‘structure‘ (ie, material, human or organizational resources needed for care), ‘process‘ (ie, patient’s and practitioner’s activities in doing care) and ‘outcome‘ (ie, health status affected by care).31 For the present study, 12 care indicators were selected which were based on national guidelines and recommendations8 32 and covered (1) care processes (self-management, self-monitoring, medical care) and (2) care outcomes (acute and long-term complications). Details of the assessment and coding of these care indicators are described in online supplemental table S1.
Supplemental material
Care processes
Four indicators were chosen to evaluate self-management behavior of the participant with regard to ever taking part in a diabetes education program, currently having a diet plan due to diabetes, currently keeping a diabetes diary and ever holding a personal diabetes passport.
Indicators of self-monitoring consisted of performing blood glucose self-control generally and self-examination of the feet regarding pressure points or open wounds at least once a month. For sensitivity analyses, blood glucose self-control and foot self-examination were coded as ‘daily’ or ‘not daily’.
Three indicators concerned utilization of medical care by the participant regarding measurement of HbA1c level or examinations of the eyes including ocular fundus by an ophthalmologist (with dilating drops of the pupil) and of the feet by a physician or medical professional at least once in the past 12 months. For sensitivity analyses, ‘at least four times’, instead of ‘at least once’, was used for HbA1c measurement.
Care outcomes
To assess short-term complications, participants were asked about the presence of acute hypoglycemia and hyperglycemia in the past 12 months. Additionally, participants were asked whether the reported acute condition led to treatment by a physician, for example, hospital stay, emergency healthcare or use of medical service. For sensitivity analyses, this further information was used for a more stringent definition of hypoglycemia or hyperglycemia, requiring that participants who answered the initial question regarding hypoglycemia or hyperglycemia affirmatively also confirmed that they had received medical treatment.
To assess long-term complications, participants were asked whether they have or have ever had diabetes-specific complications, namely diabetic nephropathy (diabetes-specific kidney disease, dialysis due to diabetes-specific kidney disease or kidney transplant due to diabetes), diabetic retinopathy (diabetes-specific eye disease or blindness), diabetic neuropathy or diabetic foot/amputation. Participants who reported at least one complication were coded as ‘yes’ and otherwise as ‘no’.
Assessment of confounders
Several factors were chosen as potential confounders of the association between depressive symptoms and care indicators based on previous findings indicating associations of these factors with depression33 34 and care indicators.35–37
Educational level was assessed according to the Comparative Analysis of Social Mobility in Industrial Nations, encompassing general as well as vocational training, and classified into low, medium or high.38 Social support was assessed using the Oslo-3 Scale39 and categorized as low, moderate and high social support.
Smoking was defined as smoking daily or occasionally in contrast to non-smoking (ie, never and former smoking).40 Alcohol consumption (g/day) was obtained by an EHIS instrument based on the Alcohol Use Disorder Identification Test-Consumption Questions41 and classified into not risky (<20 g/day in men, <10 g/day in women) and risky (≥20 g/day in men, ≥10 g/day in women) alcohol consumption.42 Physical activity was assessed by the EHIS-Physical Activity Questionnaire43 and defined as meeting the WHO recommendations on recreational endurance exercise of >2.5 hours/week,44 in contrast to physical inactivity (≤2.5 hours/week). Body mass index (BMI) was calculated as the ratio of self-reported body weight (kg) and height squared (m2)42 and obesity was defined as BMI ≥30 kg/m2.
Diabetes duration was defined as duration between self-reported year of diabetes diagnosis and year of survey participation using the categories <5, 5–15 and ≥15 years.
Statistical analysis
An unweighted proportion of 28.0% of participants (n=480) had missing values in at least one variable used in the present analyses; missingness was 3.3% for depressive symptoms and ranged for the other variables between 0.23% for educational level and 8.8% for physical activity. Thus, we performed a multiple imputation of the missing values using the fully conditional specification approach, assuming that missing information was missing at random.45 By this approach, a set of data sets with full information on all variables was specified by estimating missing information in an iterative way by regression or discriminant functions. We chose a number of 30 imputation data sets which were then analyzed combined to obtain single estimates (proportion, mean, OR, 95% CI, p value), taking the within-variation and between-variation of the set of imputation data sets into account.
To account for the complex survey design and deviations of the study population from the population in Germany (as of December 31, 2014) with regard to gender, age, community type and educational level, all analyses were carried out with a weighting factor and appropriate survey procedures.29
For unadjusted analyses, associations between categorical variables and depressive symptoms were assessed by the Rao-Scott χ2 test; differences in mean age by depressive symptoms were tested by t-test.
Adjusted analyses were performed by logistic regression models to estimate ORs including 95% CIs separately for each care indicator for depressive symptoms versus no depressive symptoms (reference category). As basic model, model 1 was adjusted for age (continuous) and sex. Further adjustments were made additionally for sociodemographic factors (educational level and social support; model 2), additionally for lifestyle behaviors (smoking, alcohol consumption, physical activity and obesity; model 3), and finally for diabetes duration (model 4).
To assess the stability of the findings, we performed four sensitivity analyses using (1) moderate and severe depressive symptoms separately; (2) more stringent definitions for hypoglycemia/hyperglycemia (namely receiving medical treatment after the acute event); (3) more frequent blood sugar self-control and foot self-examinations (daily), as well as more frequent medical HbA1c measurements (at least four times in the past 12 months); and (4) an additional adjustment for consultation with a psychologist, psychotherapist or psychiatrist in the past 12 months.
Statistical analyses were performed with the SAS V.9.4 statistical software package. A p value <0.05 was considered to indicate statistical significance. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies.
Results
Description of the study population
The study population consisted of 1712 participants (968 men, 744 women) aged 19–99 years with a mean age (±SE) of 66.1 years (±0.4). Depressive symptoms were observed in 15.6% of the study population, with a higher prevalence in women than in men (18.7% vs 12.9%, p=0.008). Participants with depressive symptoms were significantly more likely to have lower levels of education and social support, as well as to be obese, smokers and less physically active, than participants with no depressive symptoms (table 1).
Distribution of characteristics of participants by no depressive symptoms and with depressive symptoms in the past 2 weeks
Depressive symptoms and care processes
In unadjusted analyses, participants with and without depressive symptoms did not generally differ with regard to indicators of self-management, self-monitoring and medical care (table 2). As one exception, currently having a diet plan due to diabetes was significantly and unexpectedly more often reported by participants with depressive symptoms compared with participants with no depressive symptoms (24.5% vs 12.1%, p<0.001).
Distribution of care indicators of participants by no depressive symptoms and with depressive symptoms in the past 2 weeks
This association persisted throughout adjustments for sociodemographic factors, lifestyle behaviors and diabetes duration with an OR of 1.95 (95% CI 1.25 to 3.03, p=0.003) in model 4 (figure 1, online supplemental table S2). Furthermore, participants with depressive symptoms were less likely to have had a dilated eye examination within the past 12 months than participants with no depressive symptoms in unadjusted analyses (table 2). However, this association was no longer significant after adjusting for sociodemographic factors, and was further attenuated after additional adjustments for lifestyle behaviors and diabetes duration (figure 1, online supplemental table S2).

Association of depressive symptoms in the past 2 weeks with indicators of care processes, estimated by logistic regression models (OR with 95% CI). Model 1: adjusted for age and sex; model 2: adjusted additionally for educational level and social support; model 3: adjusted additionally for smoking, alcohol consumption, physical activity and obesity; and model 4: adjusted additionally for diabetes duration. HbA1c, hemoglobin A1c.
Except for the indicator currently having a diet plan, the ORs for the other indicators in fully-adjusted analyses (model 4) were rather low (0.72–1.43; ie, change in odds <45%), with p>0.074 (figure 1, online supplemental table S2).
Depressive symptoms and care outcomes
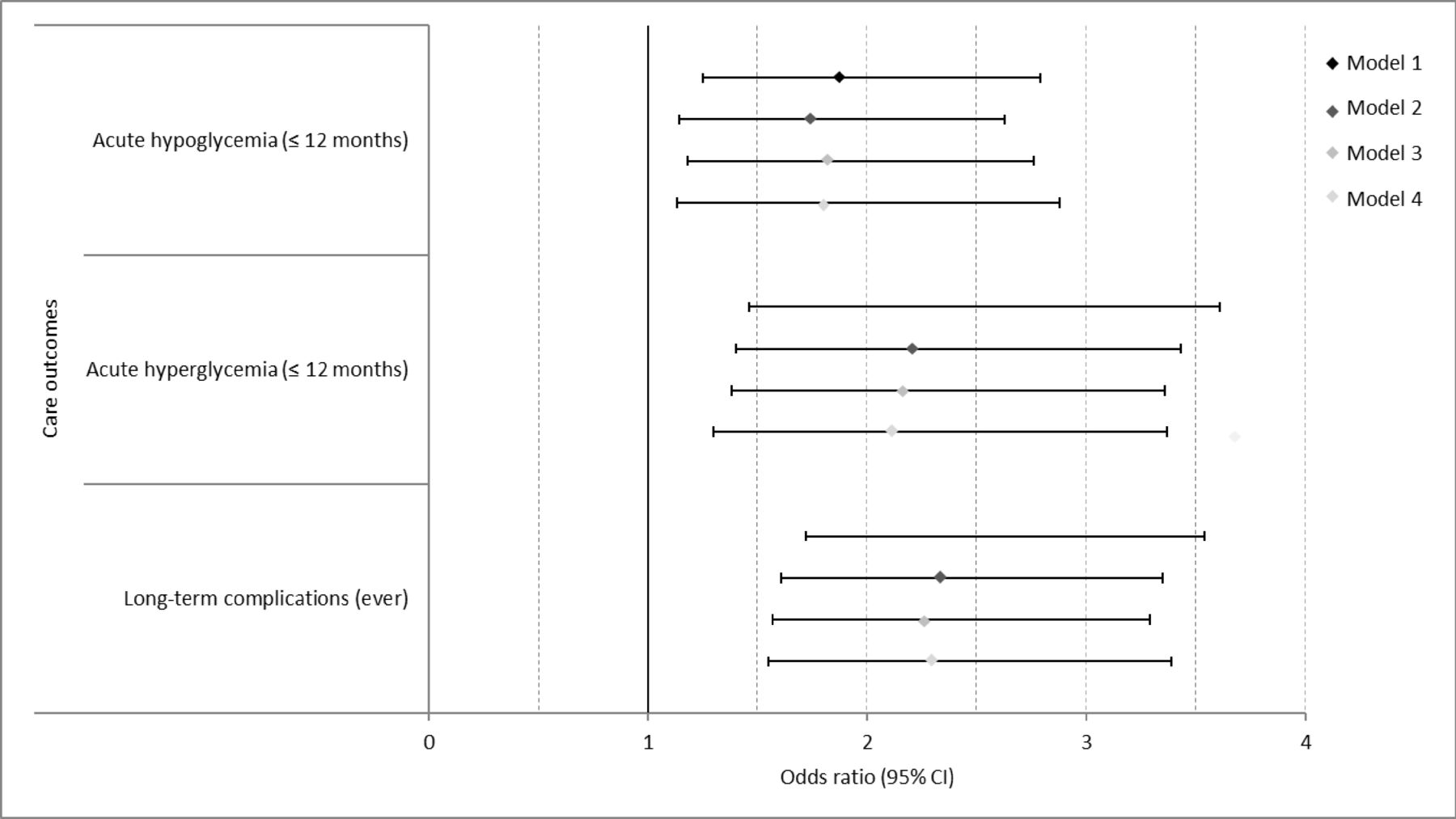
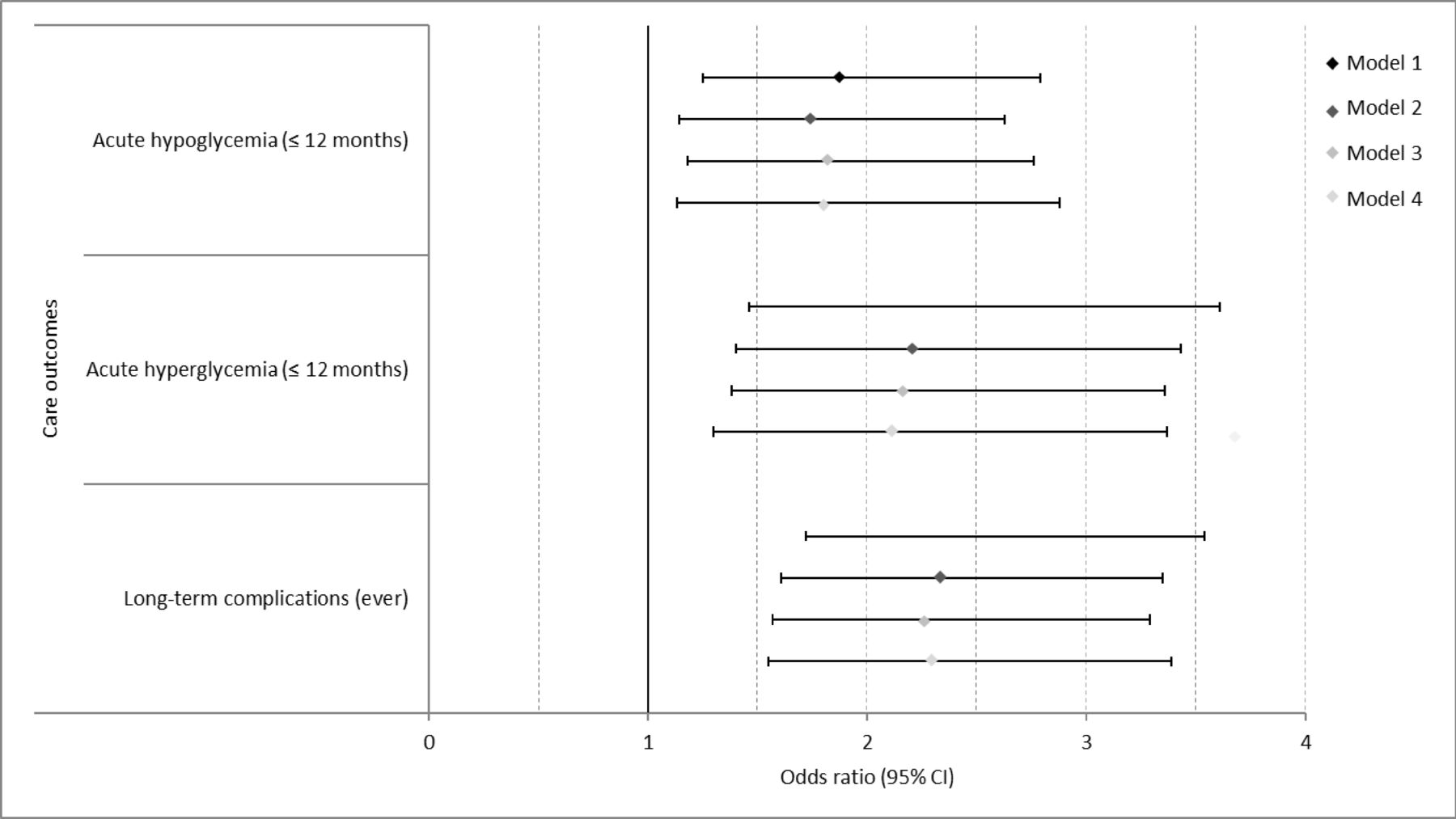
Adverse diabetes-specific care outcomes were consistently more frequently reported by participants with depressive symptoms compared with participants with no depressive symptoms, as shown in table 2, for acute hypoglycemia (23.6% vs 14.1%, p=0.002) or hyperglycemia (21.9% vs 11.0%, p<0.001) within the past 12 months, and the presence of at least one of six common long-term complications (34.0% vs 18.4%, p<0.001).
These associations were attenuated but remained significant when differences in age, sex, educational level and social support as well as lifestyle behaviors and diabetes duration were taken into account in multivariable logistic regression analyses (figure 2, online supplemental table S2). Adjusting for all selected confounders (model 4), participants with depressive symptoms were about two times more likely than participants with no depressive symptoms to report occurrence of acute hypoglycemia (OR 1.81, 95% CI 1.13 to 2.88, p=0.013) or acute hyperglycemia (OR 2.10, 95% CI 1.30 to 3.37, p=0.002) within the past 12 months and any diabetes-specific long-term complication (OR 2.30, 95% CI 1.55 to 3.39, p<0.001). Analyzing the relationship between depressive symptoms and specific types of long-term complications also revealed significant associations; the ORs in model 4 were 2.33 (95% CI 1.34 to 4.05) for nephropathy, 2.80 (95% CI 1.72 to 4.56) for retinopathy, 2.31 (95% CI 1.39 to 3.84) for neuropathy and 2.29 (95% CI 1.41 to 3.71) for diabetic foot/amputation (online supplemental table S3).
{kind=link}
{kind=link}
Association of depressive symptoms in the past 2 weeks with indicators of care outcomes, estimated by logistic regression models (OR with 95% CI). Model 1: adjusted for age and sex; model 2: adjusted additionally for educational level and social support; model 3: adjusted additionally for smoking, alcohol consumption, physical activity and obesity; and model 4: adjusted additionally for diabetes duration.
Sensitivity analyses
To assess the stability of the main findings described above, we performed four sensitivity analyses which are displayed with their estimates in the logistic regression analyses, adjusted as in models 4.
First, applying a more stringent definition of acute hypoglycemia/hyperglycemia, that is, only if participants also confirmed that they had needed medical treatment, confirmed the associations of depressive symptoms with hypoglycemia (model 4: OR 2.29, 95% CI 1.07 to 4.94, p=0.034) and hyperglycemia (model 4: OR 2.84, 95% CI 1.39 to 5.77, p=0.004); the ORs tended to be even higher (online supplemental table S4). Of note, the prevalence of self-reported events requiring medical attention was small even among participants with depressive symptoms (hypoglycemia: 5.2%; hyperglycemia: 8.3%). Thus, these findings should be taken with caution due to a small number of observations.
Second, using more stringent criteria to define blood sugar self-control and foot self-examination by using ‘daily’ versus ‘not daily’ as categories largely confirmed the results observed in the main analyses. As shown in online supplemental table S4, multivariable logistic regression analyses (model 4) revealed similar estimates for blood sugar self-control (OR 1.53, 95% CI 0.997 to 2.38, p=0.057) and stronger estimates for foot self-examination (OR 1.39, 95% CI 0.96 to 2.00, p=0.081) compared with the main analyses (figure 1, online supplemental table S2). A stricter definition for HbA1c measurement with reporting at least four measurements in the past 12 months as threshold revealed no substantial differences compared with the main analyses (data not shown).
Third, we used moderate (sum score 10–14) and severe (sum score ≥15) depressive symptoms as two separate groups in the logistic regression analyses with no depressive symptoms as reference group. These analyses confirmed the findings of the main analyses for most indicators, with largely comparable estimates in the two groups. However, for the indicator performing foot self-examination, a significant association was found for participants with severe depressive symptoms (OR 2.26, 95% CI 1.12 to 4.57, p=0.024), but not for participants with moderate depressive symptoms (OR 0.89, 95% CI 0.58 to 1.35, p=0.573), compared with participants with no depressive symptoms. Furthermore, the ORs for currently having a diet plan, acute hyperglycemia and long-term complications increased from moderate to severe depressive symptoms; however, the increase in OR was not significant (online supplemental table S5). These findings should be taken with caution due to the low prevalence of severe depressive symptoms in the study population (5.4%).
Fourth, adding consultation with a psychologist, psychotherapist or psychiatrist in the past 12 months confirmed the results from the main analyses (model 4), including the results for currently having a diet plan (OR 2.26, 95% CI 1.45 to 3.53, p<0.001), acute hypoglycemia (OR 1.66, 95% CI 1.03 to 2.67, p=0.036), acute hypoglycemia (OR 2.01, 95% CI 1.25 to 3.25, p=0.004), and having at least one diabetes-specific long-term complication (OR 2.23, 95% CI 1.50 to 3.34, p<0.001) (data not shown).
Discussion
Overall findings
The present study investigated the association between depressive symptoms and 12 selected indicators of quality of care in diabetes in a sample of people with diabetes identified from a cross-sectional, nationwide and population-based survey in Germany. After adjusting for potential confounders, we found that individuals with depressive symptoms were more likely to report acute hypoglycemia or hyperglycemia in the past 12 months, as well as at least one of six common diabetic-specific long-term complications in their lifetime, compared with individuals without depressive symptoms. No consistent pattern of associations between depressive symptoms and indicators of care processes (self-management, self-monitoring and medical care) could be revealed, except for a higher chance of currently having a diet plan due to diabetes in individuals with depressive symptoms.
Depressive symptoms and care processes
Based on findings from two meta-analyses,16 17 we hypothesized that persons with diabetes would be less likely to engage in the complex and time-intensive processes of diabetes care (self-management, self-monitoring, medical care) in the presence of depressive symptoms. This lack of treatment adherence has been linked to typical characteristics of depression such as feelings of hopelessness and lethargy and to associated aspects such as reduced cognitive functioning and social isolation.16
In the present epidemiological study, participants with depressive symptoms did not generally report lower levels of care process indicators than participants without depressive symptoms after adjusting for educational level and social support in the main analyses. They were even more likely to report currently having a diet plan due to diabetes. Previous studies indicating an association of depressive symptoms with lower self-care or medical care and treatment adherence16–20 were conducted mostly in clinical or care settings. Thus, they are based on patients with diabetes who were more likely to be involved currently or at least recently in care processes. This is in contrast to the present study population, which was randomly drawn from the general population.
Due to the high prevalence of depressive symptoms among individuals with diabetes and its negative impact on disease outcomes, there has been a growing alertness among healthcare professionals,46 leading to the development of guidelines8 9 47 which recommend special attention to care of persons with diabetes and comorbid depressive symptoms. This could also serve as one possible explanation for the lack of an association between depressive symptoms and diabetes care utilization in our study among adults with diabetes.
In contrast to the other self-care indicators, currently having a diet plan due to diabetes was significantly more frequent in persons with diabetes with depressive symptoms than without depressive symptoms, even after adjusting for potential confounders such as obesity. Besides the overall low prevalence of persons fulfilling this care indicator (~14%), presumably due to under-representation in German diabetic guidelines,8 physicians might regard diet plans as a helpful tool to structure daily routines and thus as especially useful for patients with comorbid depressive symptoms to control dietary habits. This may also hold for the significant associations of depressive symptoms and daily foot self-examination as well as of severe depressive symptoms and foot self-examination (daily or ≤4 weeks), as shown in the sensitivity analysis.
Depressive symptoms and care outcomes
Several previous studies based on clinical, registry or care system data reported significant associations between depressive symptoms and acute hypoglycemia,22 23 poor glycemic control18 20 21 and long-term complications,13 24 which could be confirmed by our study drawn from the general population.13 18 20 22 23 It was suggested that the depression–outcome relationship may be driven by poor health behaviors such as low self-care and treatment adherence, as well as by psychobiological changes such as dysregulation of the autonomic nervous system and increased inflammatory processes due to depressive symptoms, which may lead to glycemic variations22 23 and diabetes-related microvascular complications.13 48 A recent cross-sectional study based on a sample drawn from an inpatient diabetes center indicated a link between depression and elevated HbA1c values via self-care; the direct association between depression and elevated HbA1c was repealed by low self-care.20 The patients of this clinical study sample may be in a more advanced diabetes stage as diabetes-related long-term complications were present in 62% of patients with type 2 diabetes and 31% of patients with type 1 diabetes, which were substantially higher than in the present population-based study of persons with self-reported diabetes during the past 12 months (21%); this difference may have contributed to the missing link in the depressive symptoms–hyperglycemia association via self-care in our study.
The mentioned studies were cross-sectional20 23 considering depression as exposure as in our study, or longitudinal13 18 22 with depression at baseline and the respective outcome at follow-up. However, the depression–outcome relation in persons with diabetes may be regarded not only as an effect of depressive symptoms on an outcome but also vice versa, as an effect of an outcome on depressive symptoms. A bidirectionality has been suggested for the relationship of depression and diabetes10 due to sharing common inter-related biological pathways.49 These underlying mechanisms may also contribute to a bidirectional depression–outcome relation in people with diabetes. A prospective study among 3742 adults with type 1 diabetes based on diabetes registry data showed that depression and severe hypoglycemia/hyperglycemia events were associated bidirectionally.50 Thus, it may be possible that in our study depressive symptoms could be the consequence rather than the cause of severe diabetes-related outcomes as largely no significant associations were found between depressive symptoms and care process indicators. A prospective case–control study of 40 subjects with insulin-treated diabetes drawn from a diabetes outpatient unit showed an increased risk for depression for those with a recent spontaneous episode of severe hypoglycemia at baseline compared with those without such an episode.51 The experience of an acute glycemic event or of diabetes-related complications may lead to persistent fear and uneasiness regarding the course of diabetes and finally to increased levels of depressive symptoms.
Depressive symptoms and diabetes distress
We used PHQ-8 as an established epidemiological screening instrument measuring current depressive symptoms in contrast to (self-reported) medical history of clinical depression. By using this approach we ensured solely including currently affected persons, since it has been proposed earlier that adequate antidepressant treatment outweighs the negative effects of depressive symptoms on diabetes care.52
It remains unclear to what degree ‘diabetes distress’, a term which is often used for describing psychosocial burden and mental health problems associated with diabetes,53 is represented by the entity of ‘depressive symptoms’ (eg, measured by PHQ-8), or whether it should rather be regarded as a separate entity.54 55 Previous studies based on patients with diabetes drawn from clinical settings indicated a mediating role of diabetes distress in the association of depression and hyperglycemia; especially the coincidence of the two conditions was prone to impair glycemic control.56–58 In these studies, depression and diabetes distress were rather moderately correlated and therefore cannot be considered as more or less convertible. Depressive symptoms may reflect, at least in part, diabetes-related distress due to lower personal, social and psychological resources.
To overcome depressive symptoms and diabetes-related distress in persons with diabetes, psychological interventions based on cognitive and emotional components in order to strengthen self-efficacy, resilience and coping strategies might be an important option to reduce deficits in diabetes care, but also in lifestyle-associated risk factors.52 An intervention study applying an intensive case management according to rigorous treat-to-target guidelines for depression, diabetes and cardiovascular disease found positive intervention effects on outcomes such as depression or HbA1c levels after a mean follow-up of 11 months.59
Strengths and limitations
A major strength of the present study is that it was based on a sample of adults with diabetes drawn from a large population-based sample representative of the adult population in Germany with standardized and quality-controlled data ascertainment. Furthermore, as far as we know, it is the first epidemiological study investigating the association of depressive symptoms with indicators of care processes and outcomes simultaneously in the same data set.
However, the present study has several limitations. First, the findings discussed were based on a cross-sectional study design; hence it was not possible to determine the direction of association, that is, whether depressive symptoms may be the underlying cause of the presence of adverse diabetes outcomes or vice versa, adverse diabetes outcomes may be the cause of the presence of depressive symptoms. Causal conclusions would require longitudinal modeling as in cohort studies or in an experimental setting. Second, in the present epidemiological study all variables used for the analyses were based on self-reports and not on medical interviews, which may have led to misclassifications and underestimations due to recall or reporting bias and selective non-response of less healthy participants. This may have contributed to the largely non-significant associations between depressive symptoms and care process indicators, even though sensitivity analyses found largely no substantial differences regarding moderate or severe depressive symptoms. Third, a distinction in our analyses between type 1 and type 2 diabetes was not possible. However, as type 2 diabetes accounts for about 90% of all diabetes cases, the present findings were related mainly to type 2 diabetes. Fourth, information on antidiabetic drug treatment or medication treatment in order to assess disease severity was not available with sufficient extent. Furthermore, we had no information about potential antidepressive medications. However, in a sensitivity analysis, an item regarding consultation with a psychologist, psychotherapist or psychiatrist within the past 12 months was used as proxy for mental healthcare utilization and did not substantially change the results (ORs) when added to the logistic regression models. Fourth, an under-representation of persons with advanced diabetes and further serious illnesses as well as persons living in institutions such as nursing homes cannot be excluded.
Implications for diabetes care and future research
The results of the present study emphasize the need for including the assessment of depressive symptoms into coordinated diabetes care, for example, in the German disease management programs for type 1 and type 2 diabetes. In order to adjust care processes to the needs of patients with diabetes, future research needs to unravel the complex inter-relationship between depression, diabetes-related distress and diabetes outcomes. Depression has been shown to adversely affect mental as well as metabolic health among persons with diabetes.49 In a vicious circle this may be aggravated by diabetes distress resulting from poor care outcomes and low satisfaction with care processes. As shown in the present study and in previous research,25 60 depression among persons with diabetes has been linked to lower social status, lack of social support, and the presence of diabetes complications. Consequently, care processes should be tailored to the different needs of specific subgroups of patients with diabetes. Thus, innovative research on depression and diabetes should be integrated in routine care and be based on electronic patient record data as well as patient-reported outcomes.61
Conclusions
The present cross-sectional, population-based and nationwide survey of adults with diabetes showed significant and consistent associations between the presence of depressive symptoms in the past 2 weeks and adverse diabetes-specific outcomes, including events of acute hypoglycemia or hyperglycemia in the past year and one or more diabetes-specific long-term complications. However, we could not confirm a pathway from depressive symptoms to diabetes-related outcomes via adverse care processes.
In conclusion, our findings underline the need for intensified care for persons with diabetes and depressive symptoms. Future research needs to be integrated in routine care based on electronic patient records and patient-reported outcomes in order to develop care concepts tailored to the needs of different subgroups of patients with diabetes.
Acknowledgments
We thank all participants of the GEDA-2014/2015-EHIS study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Presented at DDG-Kongress, Berlin, 31.05.19 (Diabetes Congress of the German Diabetes Association) Baumert J, Jung A, Du Y, Nübel J, Heidemann C, Scheidt-Nave C. Depressive Symptomatik und Versorgungsqualitat in der Diabetesbehandlung – Ergebnisse der bundesweiten GEDA 2014/15-EHIS-Studie.
Contributors AJ performed statistical analyses and drafted the manuscript. JB performed statistical analyses and made substantial contribution to the interpretation of data. YD, CH, JN and MAB made substantial contribution to the interpretation of data. CS-N had the idea for the study and made substantial contribution to the interpretation of data. All authors critically revised the manuscript for important intellectual content and read and approved the final version of the manuscript.
Funding This work was supported by research grant from the German Center for Diabetes Research (DZD), funded by the Federal Ministry of Education and Research, Germany (FKZ: HMGU2018Z3), and a grant from the Federal Ministry of Health, Germany, to develop a diabetes surveillance system in Germany (grant number: GE 2015 03 23). The GEDA 2014/2015-EHIS study was funded by the Robert Koch Institute and the Federal Ministry of Health, Germany. The Robert Koch Institute is a Federal Institute within the portfolio of the Federal Ministry of Health, Germany.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The GEDA 2014/2015-EHIS survey was approved by the ‘Federal Commissioner for Data Protection and Freedom of Information in Germany’ (III-401/008#0015).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The minimal data set underlying the findings presented in this manuscript is archived at the Health Monitoring Research Data Centre at the Robert Koch Institute (RKI) and can be accessed by all interested researchers. On-site access to the data set is possible at the Secure Data Center of the RKI’s Health Monitoring Research Data Centre. Requests should be submitted to fdz@rki.de.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.