Article Text

Abstract
Introduction Type 2 diabetes (T2D) is a common condition that, if left untreated or poorly managed, can lead to adverse microvascular and macrovascular complications. We estimated the prevalence and incidence of microvascular and macrovascular complications among patients newly diagnosed with T2D within a US integrated healthcare system.
Research design and methods We conducted a retrospective cohort study among patients newly diagnosed with T2D between 2003 and 2014. We evaluated 13 complications, including chronic kidney disease (CKD), cardiovascular disease (CVD), and all-cause mortality through 2018. Multivariable Cox proportional hazards models were used to study factors associated with complications.
Results We identified 135 199 patients with incident T2D. The mean age was 58 years, and 48% were women. The prevalence of CKD was the highest of the complications at the time of T2D diagnosis (prevalence=12.3%, 95% CI 12.2% to 12.5%), while the prevalence of CVD was among the lowest at 3.3% (95% CI 3.2% to 3.3%). The median time to incidence of a T2D complication ranged from 3.0 to 5.2 years. High incidence rates (95% CI) of T2D complications included peripheral neuropathy (26.9, 95% CI 26.5 to 27.3 per 1000 person-years (PY)), CKD (21.2, 95% CI 20.9 to 21.6 per 1000 PY), and CVD (11.9, 95% CI 11.7 to 12.2 per 1000 PY). The trend of 5-year incidence rates of T2D complications by diagnosis year decreased over time (p value<0.001). Older age, non-Hispanic white race/ethnicity, sex, higher A1C, smoking, and hypertension were associated with increased CKD and CVD incidence.
Conclusion Though incidence rates of T2D complications were lower in more recent years (2010–2014), a significant proportion of patients had complications at T2D diagnosis. Earlier preventive therapies as well as managing modifiable factors may help delay the development and progression of T2D complications.
- diabetes mellitus
- type 2
- diabetes complications
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Type 2 diabetes (T2D) is a very common condition that, if left untreated or with no proper care, can contribute to the development of microvascular and macrovascular complications. Previous studies suggest that some T2D complications are prevalent even at the time of diabetes diagnosis, such as chronic kidney disease (CKD).
While there has been a decreasing trend of T2D complications, including large reductions in cardiovascular disease (CVD), the development of microvascular and macrovascular complications remains a significant clinical concern for patients with T2D. Peripheral arterial disease, heart failure, and stable angina are suggested as early cardiovascular manifestations in patients with T2D.
What are the new findings?
Our findings show that a substantial proportion of patients had existing complications including CKD, stable angina, and peripheral neuropathy at the time of T2D diagnosis. Results also show that among those newly diagnosed with T2D, the highest incidence rates of complications included peripheral neuropathy, CKD, and CVD (myocardial infarction, unstable angina, and stroke).
Time to incidence of microvascular and macrovascular complications was only a few years; peripheral vascular disease, stable angina, CKD, and peripheral neuropathy developed earlier in the disease course.
Significance of this study
How might these results change the focus of research or clinical practice?
Understanding when complications develop following diagnosis and the prevalence of common diabetes complications and risk factors at the time of diagnosis may further guide screening and treatment decisions.
Findings also support the changes to the American Diabetes Association and the European Society Cardiology treatment guidelines, which emphasize the importance of ongoing risk assessment and comprehensive medical evaluations of comorbidities and complications to best decide on the appropriate treatment plan.
Introduction
Type 2 diabetes (T2D) is a common condition affecting approximately 463 million adults globally in 2019.1 Treatment and management of T2D is critical since the condition is associated with many adverse microvascular and macrovascular complications.2 Recent changes in diabetes treatment guidelines highlight the importance of assessing common comorbidities that affect people with diabetes and how these may impact their diabetes treatment choices.3 4 With newer treatment options, patients with T2D may be able to slow the development and progression of microvascular or macrovascular complications, such as chronic kidney disease (CKD) and cardiovascular disease (CVD).5
Despite the importance of comorbidities of T2D, there is a lack of evidence describing the natural progression of T2D, the prevalence and the long-term development of diabetes complications over time in a large contemporary cohort of T2D. A few US studies showed a decreasing trend of T2D complications over the last few decades with large reductions in myocardial infarction (MI) and stroke in older adults.6–8 Recent studies from Europe reported a similar trend,9 and heart failure and peripheral arterial disease were suggested as the most common early cardiovascular manifestations.10 11
In addition to the development of new diabetes complications, recent studies suggest that a substantial proportion of patients with T2D already have diabetes complications at the time of diabetes diagnosis. Gatwood et al reported that more than 30% of veterans had CKD prior to being diagnosed with diabetes.12 While previous studies from various countries investigated the prevalence of T2D complications,13 many studies investigated the prevalence of complications cross-sectionally and reported only a limited number of complications, or the timing of prevalence was not specifically at or from the time of T2D diagnosis.
An understanding of when complications develop following diagnosis during a long-term follow-up and the prevalence of common diabetes complications and risk factors at the time of diagnosis in a large contemporary T2D cohort may further guide screening and treatment decisions.
Accordingly, in this study, we aimed to (1) estimate the prevalence of microvascular and macrovascular complications among patients with incident T2D at the time of diabetes diagnosis, (2) estimate the incidence of microvascular and macrovascular complications over 15 years stratified by age, sex, race/ethnicity, and diabetes diagnosis year, and (3) investigate modifiable risk factors associated with microvascular and macrovascular complications.
Methods
Study setting
We conducted an observational retrospective cohort study using data obtained from administrative and electronic health records (EHRs) of Kaiser Permanente Southern California (KPSC), a large US-integrated healthcare delivery system. KPSC currently serves approximately 4.6 million members. KPSC provides medical services to its members through its own facilities, which include 15 hospitals, more than 200 outpatient facilities and a centralized laboratory. All clinical care and interactions with the healthcare delivery system are captured in comprehensive EHRs.
Study population and study period
We identified KPSC members aged ≥20 years with incident T2D between January 1, 2003 and December 31, 2014, using a validated algorithm14 that incorporated inpatient, emergency, ambulatory care, laboratory and pharmacy data in EHRs. We defined the first date the algorithm criteria were met as the date of diagnosis (index date). We required patients to have a minimum of 2 years of continuous KPSC membership and a prescription drug benefit prior to the index date to minimize the likelihood that patients with pre-existing diabetes entered the cohort. We excluded patients who had a prior history of any form of diabetes, had a missing date of birth, or who were in hospice or a skilled nursing facility in the 1 year prior to the index date.
We used the baseline period of 2 years before and 6 months after the index date (a total of 2.5 years) to collect baseline patient demographic and clinical characteristics. We included 6 months after the index date in the baseline period to allow for screening of diabetes complications. Patients were followed from 6 months after the index date until the outcome of interest, study end date (June 30, 2018), end of membership, or death, whichever occurred first. The incidence of each microvascular or macrovascular complication was evaluated among patients at risk.
Demographics and clinical characteristics
Age, sex, race/ethnicity, insurance type, body mass index (BMI), and smoking history were extracted from the EHR. Baseline laboratory measures (A1C, fasting plasma glucose (FPG), and lipid levels), medication use (antihyperglycemic agents, antihypertensive agents, other cardiovascular medications, and other concomitant medications), comorbidities (hypertension, hyperlipidemia, and the Charlson Comorbidity score), and healthcare use (inpatient stays and outpatient and emergency department visits) were obtained from EHRs.
Microvascular and macrovascular complications
We evaluated 13 microvascular and macrovascular complications commonly associated with T2D: MI, unstable angina, stroke, composite CVD (including MI, unstable angina, and stroke), heart failure, stable angina, peripheral vascular disease, lower extremity amputation, CKD, end-stage kidney disease (ESKD), proliferative diabetic retinopathy, peripheral neuropathy, and all-cause mortality. All outcomes were identified from a combination of primary inpatient, outpatient, and emergency department diagnosis codes using the International Classification of Diseases 9th Revision and 10th Revision codes or procedure codes (Current Procedural Technology, Fourth Edition) except for CKD, ESKD and all-cause mortality.
CKD was defined as two or more estimated glomerular filtration rate (eGFR) levels<60 mL/min/1.73 m2 at least 90 days apart by applying the Chronic Kidney Disease Epidemiology Collaboration equation to serum creatinine values. ESKD was defined as initiation of chronic dialysis or kidney transplant identified from the KPSC ESKD registry. Mortality was identified from KPSC hospital or administrative records, or state or federal mortality files.15 A definition of each microvascular and macrovascular complication is listed in online supplemental table S1.
Supplemental material
Statistical analysis
Descriptive statistics were used to summarize baseline patient demographics and clinical characteristics for the overall population and to estimate the prevalence of microvascular and macrovascular complications. The T2D complications identified during the 2.5-year baseline period were defined as prevalent cases.
All complications identified during the follow-up period were defined as incident cases. All analyses investigating incidence of complications were conducted among patients at risk. The cumulative incidence of microvascular and macrovascular complications was estimated using Kaplan-Meier survival analysis. The incidence rates per 1000 person-years were estimated using generalized linear regression with Poisson errors. Further stratified analyses of cumulative incidence were conducted by age, sex, and race/ethnicity. The yearly trend of incidence rates of 2 and 5 years were investigated by T2D diagnosis year. Multivariable Cox proportional hazards models were used to investigate baseline factors associated with CKD and CVD outcomes, the major outcomes of T2D clinical trials.5
Results
We identified 135 199 patients with incident T2D. Mean (SD) age was 57.8 (13.2) years old; 48% were women; 36% were non-Hispanic white; 35% were Hispanic; 13% were non-Hispanic Asians; and 12% non-Hispanic black. About 20% of patients were considered extremely obese (BMI≥35 kg/m2), and 21% were obese (BMI 30.0–34.9 kg/m2) (table 1).
Baseline characteristics of incident type 2 diabetes over time
Diabetes detection, treatment, and comorbidities over time
A higher percentage of patients had documented FPG testing at baseline in earlier years (2003–2005), whereas a higher percentage of patients had A1C testing in later years (2012–2014) (table 1). Within 6 months of diagnosis (index date), 44.3% initiated monotherapy and 3.3% initiated dual therapy, while 52.3% did not initiate any antihyperglycemic agents. Use of other cardiovascular medication, such as statins, increased over time from 28.3% in 2003–2005 to 36.1% in 2012–2014. A higher percentage of patients had comorbidities other than T2D in earlier years than in later years (≥2 Charlson Comorbidity score: 67.0% in 2003–2005 vs 51.1% in 2012–2014). A higher percentage of patients had one or more inpatient and emergency department visits in 2003–2005 than in 2012–2014.
Prevalence of microvascular and macrovascular complications at diagnosis
The prevalence of CKD was the most common complication at the time of T2D diagnosis (prevalence=12.3%, 95% CI 12.2% to 12.5%) followed by stable angina (4.6%, 95% CI 4.4% to 4.7%), peripheral neuropathy (3.8%, 95% CI 3.7% to 3.9%), and heart failure (3.5% 95% CI 3.4% to 3.6%) (table 2). At T2D diagnosis, the prevalence of CVD was 3.3% (94% CI 3.2% to 3.3%), while the prevalence of lower extremity amputation, proliferative diabetic retinopathy, and ESKD was less than 1%.
Prevalence and incidence of microvascular and macrovascular complications (N=135 199)
Incidence of microvascular and macrovascular complications
Complications with the highest incidence rates included peripheral neuropathy (26.9, 95% CI 26.5 to 27.3 per 1000 person-years), CKD (21.2, 95% CI 20.9 to 21.6 per 1000 person-years), CVD (11.9, 95% CI 11.7 to 12.2 per 1000 person-years), stable angina (7.1, 95% CI 7.0 to 7.3 per 1000 person-years), and heart failure (7.1, 95% CI 6.9 to 7.3 per 1000 person-years) (table 2). The median time to incidence of a diabetes complication ranged from 3.0 to 5.2 years. The median time to incidence was shorter for peripheral vascular disease (3.0 years), stable angina (3.0 years), CKD (3.2 years), and peripheral neuropathy (3.3 years) compared with lower extremity amputation (5.2 years) and ESKD (5.0 years).
Incidence of microvascular and macrovascular complications stratified by age, sex, and race/ethnicity
When stratified by age, a higher cumulative incidence of CKD was observed in older patients (60.6% for age 80+ years, 45.8% for age 65–79 years at 13 years) versus younger patients (19.6% for age 45–64 years, 5.2% for age 20–44 years at 13 years). The findings were consistent for CVD (45.6% for age 80+ years, 25.0% for age 65–79 years, 11.3% for age 45–64 years, 5.3% for age 20–44 years at 13 years) and all-cause mortality (86.9% for age 80+ years, 41.3% for age 65–79 years, 11.8% for 45–64 years, 3.7% for age 20–44 years at 13 years) (figure 1). The cumulative incidence of CKD rapidly increased in the years immediately following diagnosis especially among older patients. Men had a higher cumulative incidence of CVD than women, whereas women had a higher cumulative incidence of CKD compared with men. Non-Hispanic white patients had the highest cumulative incidence of CVD and CKD, and the highest all-cause mortality followed by non-Hispanic black patients.
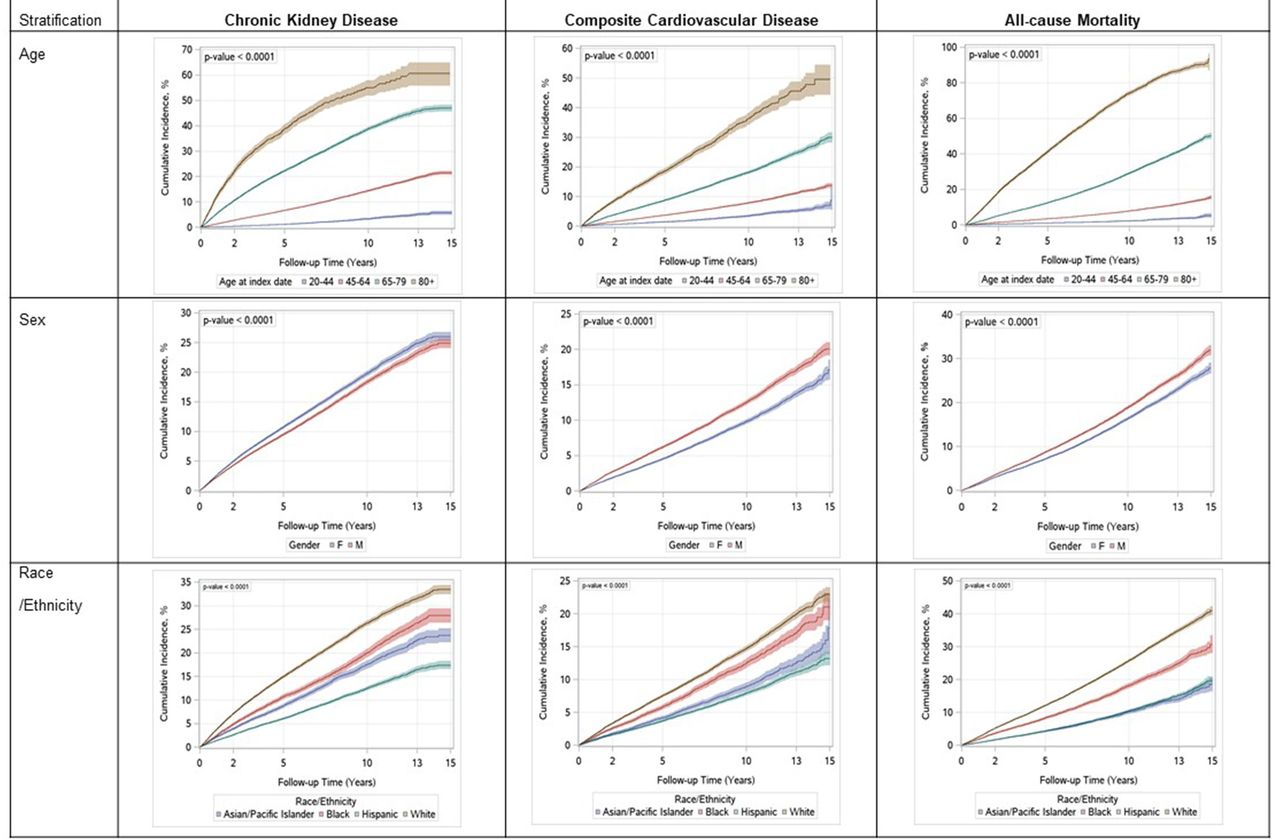
Cumulative incidence of type 2 diabetes complications stratified by age, sex, and race/ethnicity.
The cumulative incidence of other complications aside from CKD, CVD, and all-cause mortality is shown in online supplemental table S2. The cumulative incidence of the other complications was higher in older patients versus younger patients; however, the differences between age groups were smaller for lower extremity amputation, ESKD, and peripheral neuropathy. The cumulative incidence of proliferative diabetic retinopathy was higher in younger patients compared with older patients. Men had higher cumulative incidence of most of the complications, including stroke and ESKD than women, but the differences were less than 0.5% for these two complications. The cumulative incidence of ESKD was highest among non-Hispanic black patients followed by non-Hispanic Asian patients. The cumulative incidence of proliferative diabetic retinopathy was the highest among Hispanic patients followed by non-Hispanic black patients.
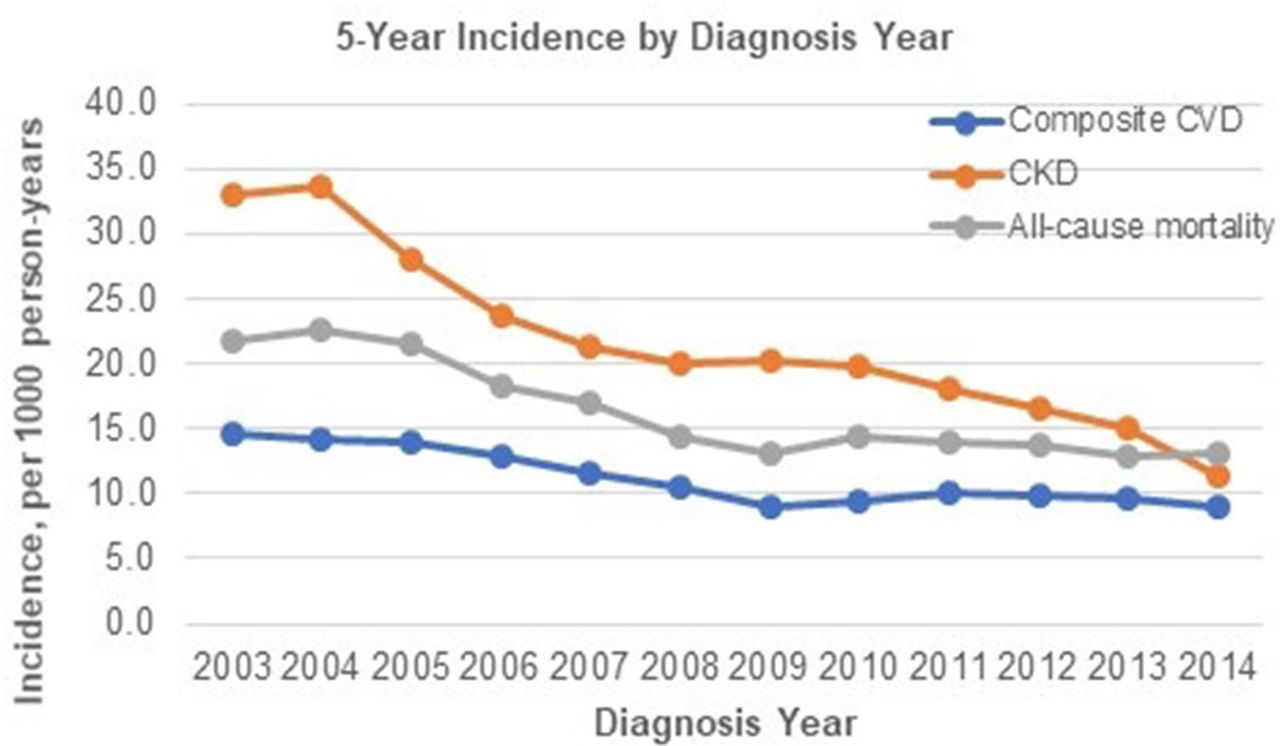
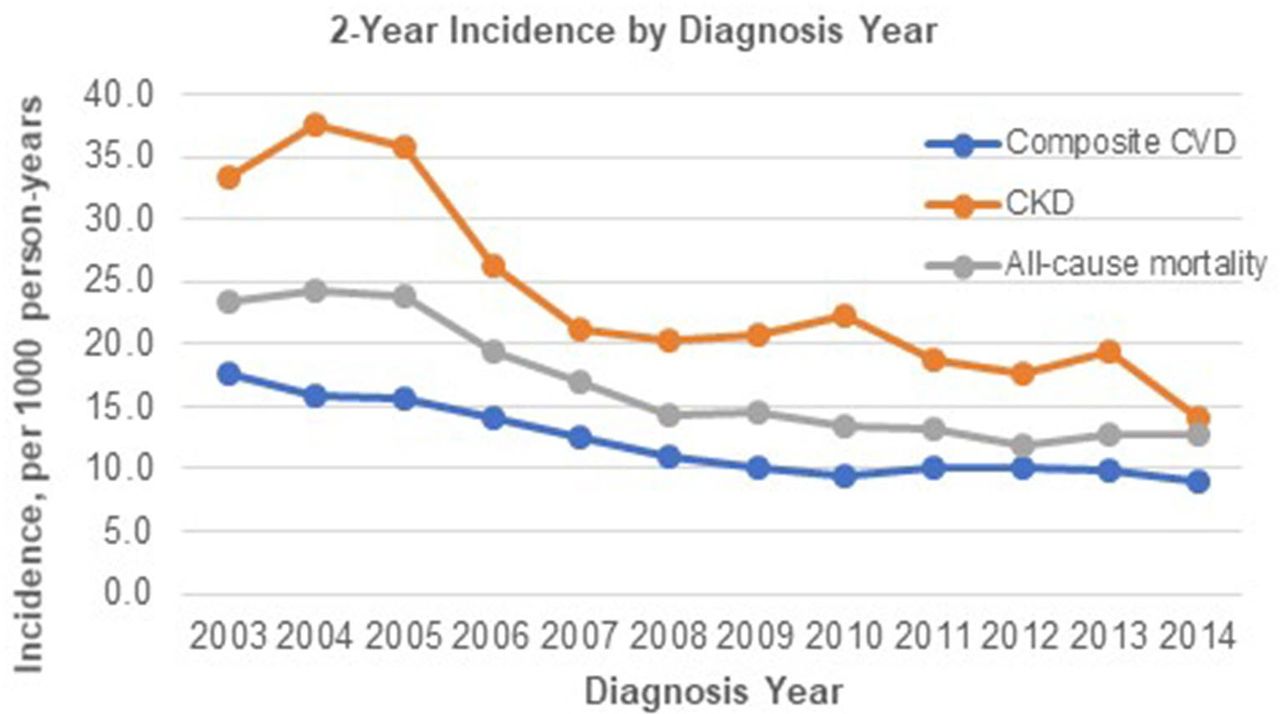
Trends of incidence rates of microvascular and macrovascular complications by diagnosis year
The incidence rates of complications of 2 and 5 years were investigated by diabetes diagnosis year. Lower incidence rates of CKD and CVD were observed among patients diagnosed with diabetes in later years (2013–2014) compared with earlier years (2003–2004), and the mortality rates were lower in later years as well (figures 2 and 3). These lower trends of event rates in later diagnosis years were observed for all complications (online supplemental table S3).

2 Year incidence rates by type 2 diabetes diagnosis year. CKD, chronic kidney disease; CVD, cardiovascular disease.
{kind=link}
{kind=link}
{kind=link}
5-Year incidence rates by type 2 diabetes diagnosis year. CKD, chronic kidney disease; CVD, cardiovascular
Modifiable factors associated with microvascular and macrovascular complications
Several modifiable factors were associated with CKD and/or CVD (online supplemental table S4). Smoking status (HR of current smoker vs never smoked=1.17, 95% CI 1.10 to 1.24), a higher number of comorbidities (HR of 4 or more comorbidities vs diabetes alone=1.55, 95% CI 1.47 to 1.64), hypertension (HR of hypertension vs no hypertension=1.60, 95% CI 1.53 to 1.67), and a higher baseline A1C (HR of A1C≥8% vs <8%=1.46, 95% CI 1.40 to 1.53) were associated with a higher risk of CKD. These factors were also associated with CVD outcomes: smoking status (HR of current smoker vs never smoked=1.60, 95% CI 1.50 to 1.72), a higher number of comorbidities (HR of 4 or more comorbidities vs diabetes alone=2.30, 95% CI 2.16 to 2.46), hypertension (HR of hypertension vs no hypertension=1.33, 95% CI 1.26 to 1.41), and high baseline A1C (HR of A1C≥8% vs <8%=1.19, 95% CI 1.13 to 1.26).
Discussion
Using data from a large US integrated healthcare system, this study estimated the prevalence and incidence of microvascular and macrovascular complications over 15 years among patients with newly diagnosed T2D. This study demonstrated that a substantial proportion of patients had existing complications, especially CKD, at the time of T2D diagnosis. Although the incidence of microvascular and macrovascular complications significantly decreased among patients diagnosed with T2D more recently, the time to incidence of these complications was still only a few years, suggesting the need for earlier preventive therapies.3
The current study showed that about 12% of patients had CKD at the time of T2D diagnosis. In addition, 40% had mild reduction in eGFR (60–89 mL/min/1.73 m2). The prevalence of stable angina, peripheral neuropathy, heart failure, and CVD was high, with 3%–4% for each compared with other conditions. This high prevalence of microvascular and macrovascular complications can be a result of hyperglycemia progression even before the clinical diagnosis of diabetes, but organ damage caused by the presence of other comorbidities may also play a role. To help delay the progression of diabetes complications further, the study findings suggest some patients may benefit from earlier introduction of therapies that have been shown to reduce complication risk. For example, newer treatment options for T2D such as sodium–glucose transport protein 2 inhibitors and glucagon-like peptide 1 receptor agonists have been shown to reduce CVD risk and to slow the progression of kidney disease.5 These agents may be appropriate first-line therapies among those with prevalent diabetes complications or in older populations (>65 years) due to the relatively rapid increase in incidence of these complications in that population.
The current study showed that patients diagnosed with T2D in more recent years (2012–2014) were at lower risk of microvascular and macrovascular complications compared with patients diagnosed with diabetes in earlier years (2003–2005). These findings are encouraging and consistent with previous US and European studies showing a decreasing trend of diabetes complications in patients with T2D.6–9 Improvements in risk factor control, including better blood pressure control with more ACE inhibitor use, better lipid control with more statin use, and more stringent glycemic control, may be responsible.16
The study results provide further insights into the timing of microvascular and macrovascular complications among patients with incident T2D. Among patients at risk, the median time to incidence of diabetes complications was only 3–5 years. These findings are consistent with recent multinational and UK studies investigating a large cohort of patients with T2D. Some of the earlier complications included peripheral vascular disease, stable angina, CKD, and peripheral neuropathy. These findings suggest the need for at least annual screening for these complications beginning at T2D diagnosis. These are in line with guideline recommendations from the American Diabetes Association and the European Society Cardiology, which emphasize the importance of ongoing risk assessment and comprehensive medical evaluations of comorbidities and complications to achieve patient health goals.3 4 In addition, earlier initiation of preventive therapies with individualized treatment options based on the risk of diabetes complications may help further delay the progression of microvascular and macrovascular complications for high-risk patients, such as those aged >65 years or with comorbidities. For lower-risk groups such as those aged <65 years or without comorbidities at diagnosis, it may be appropriate to save newer treatment options for later use in the disease course as our data show that these complications develop gradually over time.
The current study results confirm that the cumulative incidence of diabetes complications differed by age, sex, and race/ethnicity. Consistent with other literature,17 18 the incidence of CVD and CKD was significantly higher in older adults than young adults. However, younger patients with T2D had similar cumulative incidence of lower extremity amputation, ESKD, and peripheral neuropathy, and had a higher cumulative incidence of proliferative diabetic retinopathy compared with older patients. This may be due to higher baseline A1C levels, poor glycemic control over time, and poor adherence to regular eye exams in younger patients.12–14 Treating younger patients earlier and more intensively may be important to reduce lifetime risk for these complications. Moreover, this study showed that women with T2D are at higher risk of CKD than men, whereas men are at higher risk of CVD than women. These findings are generally in line with other study findings from various countries.19–21 The role of sex in the development of CKD is complex,22 and limited evidence currently exists for sex differences in CKD among patients with T2D. Future studies of the comparative impact of risk factors on CKD among men and women are needed.
We found racial/ethnic disparities of diabetes complications. Consistent with previous studies, we found racial/ethnic minorities are disproportionately affected by microvascular complications associated with T2D. The cumulative incidence of ESKD was the highest among non-Hispanic black patients followed by non-Hispanic Asian patients.23 Also, the cumulative incidence of proliferative diabetic retinopathy was the highest among Hispanic patients followed by non-Hispanic blacks patients, again similar to a previous study.24 For macrovascular complications, non-Hispanic whites patients are at a higher risk of CVD than other race/ethnicities, consistent with other study findings.23 While the consistency of these study findings relative to other published data is reassuring, some of our study findings are not necessarily the same as those of previous studies, such as a higher mortality among non-Hispanic white patients compared with other race/ethnicities.25 It is important to note that our study shows cumulative incidence of diabetes complications by race/ethnicity not adjusting for other demographic, biological, behavior, and socioeconomic factors; therefore, the results should be interpreted with caution.
Aside from older age, race/ethnicity, and sex, several modifiable factors were associated with both CKD and CVD outcomes, including smoking status and hypertension. Our study findings also showed the increased risk of diabetes complications associated with higher A1C levels at the time of T2D, which are consistent with recent findings.26 Our results underscore the importance of earlier identification of T2D and aggressive A1C control earlier in the disease course. Somewhat alarmingly, less than 50% of the study population initiated antihyperglycemic agents within 6 months of their T2D diagnosis. Previous studies have demonstrated that delays in therapy initiation are associated with poorer glycemic control, reduced therapy durability, and greater complication risk independent of baseline A1C.27 28 Future studies identifying barriers of early treatment initiation may help to better address these gaps.
This study has several strengths and limitations. The current study used a large and ethnically diverse contemporary population of patients with T2D with long-term follow-up up to 15 years. We investigated a comprehensive list of diabetes complications using EHRs. However, we investigated each complication in a separate at-risk population to estimate the incidence of diabetes complications. Patients may have multiple complications or may have developed multiple complications over time, but we did not investigate the natural progression of multiple diabetes complications or how they may relate to one another. Although the treatment of T2D may have affected the incidence rates of diabetes complications, we did not account for diabetes therapy in our analyses. As in other observational studies, there may be potential measurement bias to estimate the incidence rates of diabetes complications. Although this study used previously validated algorithms to identify incident T2D and to define a comprehensive list of diabetes complications, validation studies for some complications such as stable angina were not available. Lastly, this study was conducted in a single healthcare system among insured population, therefore, the incidence rates of diabetes complications in other populations may be different.
Conclusion
Patients with T2D diagnosed in recent years are at lower risk of diabetes complications; however, a significant proportion of patients already have microvascular and macrovascular complications at the time of diagnosis. The time to incidence of these complications was only a few years, suggesting the need for earlier and strategic initiation of T2D therapy. Modifiable factors associated with T2D complications, such as higher A1C, smoking, and hypertension, should be a focus of care management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Some study results were presented as a poster at the American Diabetes Association’s 79th Scientific Sessions; June 7–11, 2019; San Francisco, California, and at the American Diabetes Association 80th Scientific Sessions–Virtual; June 12–16, 2020.
Contributors JA contributed to the study design and interpretation of study findings, and drafted the manuscript for publication. GAN, LQ, TNH, and MAM contributed to the conception, study design, and interpretation of study findings, and significantly revised the manuscript. ZL and RW performed all data extraction and analyses and participated in data analysis planning, interpretation of study findings, and revising the manuscript. TW and SR contributed to the conception and interpretation of data, and revised the manuscript. KR contributed to the conception and oversaw the study design, interpretation of data, and revision of the manuscript. All authors read and approved the final manuscript. JA is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding Funding for this research was provided by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey, USA.
Competing interests JA and KR are employees of Kaiser Permanente Southern California, and GAN is an employee of Kaiser Permanente Northwest, who received funding through their institutions from Merck & Co., Inc., for the conduct of this study. TW and SR are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey, USA.
Patient consent for publication Not required.
Ethics approval The study was approved by the Kaiser Permanente Southern California institutional review committee (#11616) and informed consent was waived.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Due to sensitive nature of data, anonymized data that support the findings of this study are made available from the corresponding author after the legal and ethical reviews on reasonable request from qualified researchers with documented evidence of training for human subjects protections.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.