Article Text

Abstract
Introduction People with type 1 diabetes are recommended to exercise regularly. However, limited evidence exists on how frequency and duration of exercise affect the risk of hypoglycemia. The study aimed to compare the percentage of time spent in hypoglycemia between two 5-day periods with different frequency and duration of physical activity.
Research design and methods In this outpatient randomized crossover study, 26 participants aged 18–65 years with type 1 diabetes for ≥2 years and insulin pump use for ≥1 year were included. After a 7-day observation period, participants completed two 5-day intervention periods separated by a washout period of at least 14 days. One period included five exercise sessions on 5 consecutive days (5S), each consisting of 4 min of resistance training and 30 min of aerobic exercise. Another period included two exercise sessions on 2 days with at least 2 days in between (2S), each consisting of 10 min of resistance training and 75 min of aerobic exercise. During each period, participants performed in total 150 min of aerobic exercise and 20 min of resistance training and wore continuous glucose monitors (Dexcom G6) and accelerometers (ActiGraph wGT3X-BT).
Results Twenty insulin pump-treated adults (10 women) with type 1 diabetes completed the study. The baseline median (range) age was 48 (24–64) years, glycated hemoglobin 55 (44–66) mmol/mol, diabetes duration 24 (8–57) years, and body mass index 28.4 (22.3–35.8) kg/m2. No differences were observed between 5S and 2S in the percentage (mean±SD) of time spent below 3.9 mmol/L (3.5%±2.8% vs 4.5%±4.2%, p=0.28), time spent in 3.9–10.0 mmol/L (65.3%±15.0% vs 68.5%±13.6%, p=0.31), time spent above 10.0 mmol/L (31.2%±16.4% vs 27.3%±14.5%, p=0.15), mean glucose (8.7±1.3 mmol/L vs 8.5±1.2 mmol/L, p=0.33) and glycemic variability (35.8%±5.3% vs 35.8%±6.6%, p=0.97).
Conclusions Time spent in hypoglycemia was comparable between the two 5-day periods with different duration and frequency of physical activity.
Trial registration number NCT04089462.
- diabetes mellitus
- type 1
- exercise
- hypoglycemia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
People with type 1 diabetes are recommended to perform aerobic exercise for at least 150 min per week and resistance training two to three times per week.
The impact of the distribution of the 150 min of exercise per week is unknown.
What are the new findings?
A combination of resistance training and aerobic exercise for 5 consecutive days does not significantly change the percentage of time spent in hypoglycemia compared with a similar amount of exercise performed on two separate days in a 5-day period.
We found similar distribution of percentage of time in ranges (<3.9 mmol/L, 3.9–10.0 mmol/L, and >10 mmol/L) in two intervention periods with combined resistance training and aerobic exercise, either 34 min on 5 consecutive days or 85 min on 2 separate days.
In the study there were similar sleep scores and activity energy expenditure (kcal/day) when participants performed the same amount of resistance and aerobic training 5 or 2 days weekly.
If confirmed in larger studies, adults with type 1 diabetes can choose to exercise the same total amount of exercise on 5 consecutive days or on two separate sessions without their choice affecting glucose control.
How might these results change the focus of research or clinical practice?
The results of this study suggest that people with type 1 diabetes can achieve similar glucose control whether they choose to perform the recommended weekly physical activity during five short sessions or two long sessions.
Introduction
Regular exercise is associated with reduced risk of major adverse cardiovascular events, improved quality of life and physical well-being.1–3 According to different guidelines such as the American Diabetes Association’s standards of medical care, people with diabetes should aim for 30 min of moderate-to-vigorous-intensity aerobic exercise at least 5 days a week or a total of 150 min per week.4 In addition, they should practice resistance training at least two to three times per week. However, less than 40% of people with type 1 diabetes achieve the recommended exercise levels.5 6
In addition to the beneficial effects, regular exercise is associated with increased risk of hypoglycemia—both during and in the hours after the exercise session.7 8 Due to fear of hypoglycemia, people with type 1 diabetes may prioritize a sedentary lifestyle despite the increased risk of macrovascular complications.3
The glucose response to exercise is highly dependent on the type of exercise. During aerobic exercise blood glucose mostly decreases. During resistance training blood glucose is often stable or can even increase.9 Compared with aerobic exercise only, prior resistance training attenuates the decrease in blood glucose during aerobic exercise.10 However, both resistance training and aerobic exercise cause delayed-onset hypoglycemia in the hours following the session.7
To minimize exercise-related hypoglycemia, different strategies for insulin dosing and carbohydrate intake can be applied.9 11–13 These strategies require planning and initiation before the upcoming exercise session to avoid iatrogenic hyperinsulinism and thereby the risk of hypoglycemia.14 Since different exercise types affect blood glucose concentrations differently, a universal prevention strategy for exercise-induced hypoglycemia may not be applicable.9 The existing guidelines do not explicitly recommend a daily workout routine but rather outline recommendations for weekly fitness goals.4 Furthermore, several observational studies indicate that frequency and duration of an exercise session affect the risk of hypoglycemia.15–18 Another study indicates that aerobic exercise sessions may alter the following night’s sleep quality.7 However, no solid intervention studies have investigated the impact of exercise duration and frequency on the risk of hypoglycemia and sleep quality.
We hypothesized that hypoglycemia would be lower if the same amount of exercise was split into shorter sessions on consecutive days compared with longer sessions with days in between. Our aim was to evaluate the impact of 150 min of aerobic exercise and 20 min of resistance training split into either five sessions on consecutive days (5S) or two sessions with at least 2 days in between (2S) during a 5-day period on the percentage of time spent in hypoglycemia, on other glycemic parameters and on sleep from 06:00 on the first day of exercise until 06:00 on the sixth day.
Research design and methods
Design
We undertook an open-label, randomized crossover study involving a screening visit, an observation period and two intervention periods separated by a washout period. The study was registered at ClinicalTrials.gov. The randomization list was created using sealedenvelope.com and uploaded to the web application Research Electronic Data Capture (REDCap, Vanderbilt, Tennessee, USA).
Screening
After providing informed consent, screening was performed to collect the following baseline data: sex, age, exercise habits, diabetes duration, duration of insulin pump use, total daily insulin dose (average of previous 7 days), continuous glucose monitor (CGM) usage, medication, height, weight, blood pressure, heart rate and 12-lead electrocardiography, and biochemistry from blood and urine samples.
Observation period
After screening, the participants wore a real-time CGM and a wrist-worn activity monitor for 7 days. Furthermore, they were asked to maintain their normal physical activity level and behave as usual during the 7-day observation period.
Intervention periods
The 5S intervention period consisted of five exercise sessions on 5 consecutive days; each session included 4 min of resistance training and 30 min of aerobic exercise. The 2S intervention period consisted of two exercise sessions on 2 days separated by at least 1 day; each session included 10 min of resistance training and 75 min of aerobic exercise. The participants were asked to perform the same type and intensity of aerobic exercise during the two intervention periods and were instructed to start each session with the resistance training (table 1). There were no restrictions in terms of time of the day for performing the exercise. Participants were instructed not to drink alcohol during the intervention periods.
Type and duration of exercise in the two intervention periods
Washout period
Between the two intervention periods was a washout of at least 14 days. The participants were encouraged to keep their prestudy physical activity level, but they were not monitored during this period.
Glucose management during exercise
Participants were advised orally and in writing on how to manage insulin dosing and carbohydrate intake for the different exercise intensities, exercise durations and for meals taken within 1 hour before the exercise sessions, as recommended in the exercise consensus report by Riddell et al.9 These instructions were used as guidelines only and participants were free to make any desired adjustments.
Exercise diary
A diary was provided to the participants, in which they were encouraged to register adjustments of insulin delivery and carbohydrate intake before and during each exercise session. Further, CGM values before the sessions, hypoglycemic events, and symptoms of hypoglycemia during the sessions were recorded in the diary. We defined a hypoglycemic event during exercise as an event with subjective symptoms of hypoglycemia and/or a sensor glucose value below 3.9 mmol/L.
Glucose and activity monitoring
During the intervention and observation periods, participants wore a real-time CGM (Dexcom G6, Dexcom, California, USA) and a blinded wrist-worn triaxial accelerometer (ActiGraph wGT3X-BT, ActiGraph, Florida, USA) on the non-dominant wrist. For all participants, the CGM high sensor glucose alarm was set at 10.0 mmol/L and the low alarm at 4.0 mmol/L. After each period, the CGM and insulin pump were uploaded to Diasend (Glooko, California, USA) and/or Carelink (Medtronic, California, USA)) and the activity monitor was uploaded to ActiLife (ActiGraph). Physical activity level and sleep quality measures were estimated by and analyzed using the ActiLife software with Freedson and Cole-Kripke algorithms, respectively.19–21
Participants
Participants were recruited from the outpatient clinic at Steno Diabetes Center Copenhagen, Denmark. The inclusion criteria were age 18–64 years, type 1 diabetes ≥2 years, insulin pump treatment ≥1 year, use of carbohydrate counting, and the insulin pump bolus calculator for all meals and snacks. The exclusion criteria included use of drugs other than insulin affecting glucose metabolism, alcohol or drug abuse, pregnancy, breast feeding, chronic use of acetaminophen, hypoglycemia unawareness quantified by Høi-Hansen et al,22 severe hypoglycemia within the last year, vigorous-intensity exercise for more than 60 min for 3 days per week or more, and other concomitant medical or psychological condition that according to the investigator’s assessment made the participant unsuitable for study participation. Participants’ prestudy activity levels were assessed using the International Physical Activity Questionnaire Short Form. Participants using an insulin pump with low glucose suspend, predictive low glucose management or hybrid closed-loop functions were asked to deactivate these functions in the intervention and observation periods. If women experienced need for change in insulin delivery through their menstrual cycle, we scheduled the two intervention periods in the same part of their menstrual cycle.
Statistical methods
To detect a difference of 2% points in the percentage of time spent in hypoglycemia between the study arms with 80% power, a 5% significance level, and a 3% within-group and between-group SD, 20 participants should be included. To account for a 20% dropout rate, we aimed at including 25 participants.
The primary outcome was the percentage of time spent in hypoglycemia. Secondary outcomes included time in range (3.9–10.0 mmol/L), time above range, mean sensor glucose, glycemic variability (SD), coefficient of variance (CV), low blood glucose index (LBGI), high blood glucose index (HBGI), continuous overall net glycemic action (CONGA), physical activity measures (metabolic expenditure rate and percentages of time spent in sedentary and in each physical activity intensity; ie, light, moderate and vigorous physical activity), and sleep measures (total sleep time, sleep efficiency, time of wake after sleep onset). Paired t-tests were used to compare the outcomes between the intervention periods. CGM data were included in the statistical analysis if data for at least three consecutive days were available and exercise was performed for at least 75 min per period. The primary registration period was from 06:00 on study day 1 to 06:00 on study day 6, that is, 5 full days. To investigate any effects on glucose values lasting beyond the primary registration, we also undertook a secondary a priori defined analysis of an extended observation period starting 08:00 on study day 1 and lasting 7 full days. We used Microsoft Excel (Microsoft Office 365, California, USA) for statistical analyses and considered p<0.05 as statistically significant. If not otherwise stated, calculated data are presented as mean (±SD) and baseline characteristics as median (range).
For per-protocol treatment we allowed minor protocol violations: for both arms, exercise duration of least 75 min per period was accepted; for 2S, one session >75 min was accepted (instead of two); for 5S, four full consecutive sessions were accepted (instead of five).
Results
Participants
Twenty-one of twenty-six included insulin pump-treated adults with type 1 diabetes completed the study. One participant did not comply with the study protocol and was excluded. Two participants did not complete the study due to COVID-19-related lockdown in Denmark in March 2020. Two participants withdrew consent for personal reasons, and one withdrew due to CGM alarm fatigue. Assessment of prestudy activity level using the International Physical Activity Questionnaire Short Form showed high physical activity for 2 participants, moderate physical activity for 14 participants and low physical activity for 4 participants. The baseline characteristics of the 20 participants (10 women) who completed the study are presented in table 2. The washout period was on average (range) 22 (14–40) days.
Baseline characteristics of the 20 participants with type 1 diabetes completing the study
CGM measurements
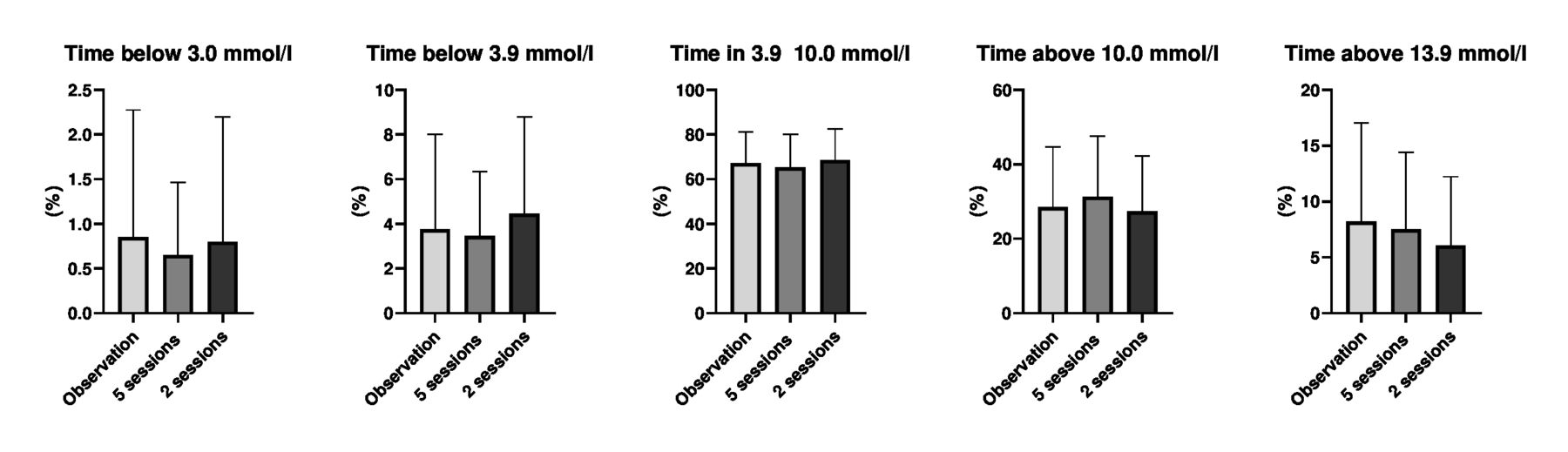
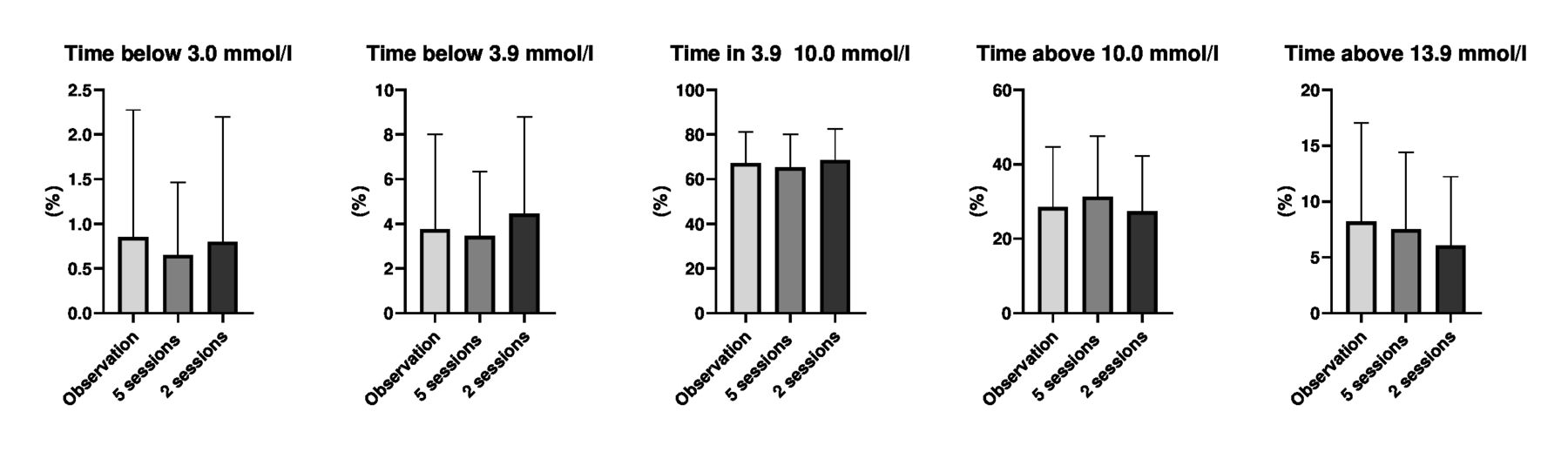
For the 20 participants who completed the study we had 5% missing CGM data points in the two intervention periods. No statistically significant difference was observed between 5S and 2S in the percentage (mean±SD) of time spent below 3.9 mmol/L (3.5%±2.8% vs 4.5%±4.2%, p=0.32), time in range (3.9–10.0 mmol/L) (65.3%±15.0% vs 68.5%±13.6%, p=0.32), time above range >10.0 mmol/L (31.3%±16.0% vs 27.3%±14.5%, p=0.25), mean glucose (8.7±1.3 mmol/L vs 8.5±1.2 mmol/L, p=0.33) and CV (35.8%±5.3% vs 35.8%±6.6%, p=0.97) (figure 1). No statistical differences were observed between interventions for other glycemic variability measures (SD, LBGI, HBGI, and CONGA). Similarly, no differences were found in the abovementioned CGM measurements for the extended observation period.
{kind=link}
Continuous glucose monitoring data on the 20 participants who completed the study. Data are presented as mean±SD of the percentage of time below 3.0 mmol/L, time below 3.9 mmol/L, time in range 3.9–10 mmol/L, time above 10.0 mmol/L and time above 13.9 mmol/L.
Activity monitor
There were no statistically significant differences between the two intervention periods in daily activity level and activity energy expenditure (table 3). There were no statistically significant differences between the observation period and the two intervention periods in the daily activity level and activity energy expenditure (table 3). Furthermore, no difference was observed in sleep measures between the intervention periods (table 4).
Data from the ActiGraph activity monitor
Sleep scores obtained by the activity monitor during the two intervention periods
Exercise diary
The percentual basal insulin reduction 1–2 hours before an exercise was not significantly different per session in 2S compared with 5S (40%±28% vs 33%±33%, p=0.53), and the participants consumed similar amounts of carbohydrates without insulin before each exercise session in 2S compared with 5S (25±37 g vs 22±20 g, p=0.47). The number of hypoglycemic events per intervention period was similar in 5S compared with 2S (1.05 events/person/week and 0.8 events/person/week, p=0.40).
Types of exercise during intervention and participant preference
The types of aerobic exercise the participant chose for the intervention periods were cycling (n=8), fast walking (n=4), running (n=2), and a combination of cycling, running and cross-training (n=6).
Discussion
In contrast to our hypothesis, we found that among people with type 1 diabetes, time spent in hypoglycemia was comparable irrespective of whether exercise was performed on 5 consecutive days or on any 2 days within a 5-day period. Furthermore, no significant differences were found in time in range, time above range, glycemic variability, carbohydrate intake and insulin dosing, as well as on activity and sleep parameters.
To the best of our knowledge, this is the first study examining the relation between exercise frequency and duration and the risk of hypoglycemia in people with type 1 diabetes. In people without diabetes, some studies have compared health-related effects based on exercise performed as frequent smaller sessions or less frequent longer sessions.23 24 Murphy and colleagues23 reviewed 16 studies and reported similar health benefits in blood pressure, weight loss, and lipid profiles of dividing the same amount of exercise into frequent shorter or fewer longer sessions. Furthermore, Shambrook and colleagues24 performed a systematic review of 16 studies in sedentary healthy persons and concluded that the glycemic response to accumulated exercise or single-bout exercise was the same.
Numerous studies have demonstrated delayed hypoglycemia after exercise, typically occurring from 8 to 12 hours in recovery from prolonged activity.7 10 25 There are two main mechanisms for this increased risk. First, liver and muscle glycogen stores must be restored after the exercise sessions and therefore the body’s glucose consumption is increased compared with resting. Second, increased insulin sensitivity can persist for hours and even days after the exercise session.7 We found similar time in hypoglycemia during daytime for 5S and 2S (4.8% vs 3.6%) and night-time for 2S and 5S (2.5% vs 3.1%).
In a study by Reddy et al7 it was found that individuals with type 1 diabetes lost 70 min of their sleep on the night after an aerobic exercise session compared with 27 min after resistance exercise session. In our study, the combination of aerobic and resistance training seemed not to alter the sleep duration or efficiency from the observation period to the two intervention periods. Unfortunately, data on when sleep started during the observation period were obtained less accurate than in the intervention periods. However, no differences in sleep parameters were seen between the two intervention periods, both including a mixture of aerobic and resistance exercise. Thus, our data indicate that sleep is not affected by the distribution of the exercise amount, but cannot explain how sleep is affected by the different types of exercise.
Strengths and limitations
The strengths of the present study include the robust study design and the use of CGM and activity monitoring to investigate the relationship of physical activity, risk of hypoglycemia and quality of sleep. We have valid CGM measurements data with only 5% missing data points in the two intervention periods used in the primary endpoint. Moreover, the participants did undertake the study in home settings, only wearing non-invasive wearables with minimal burden on participants’ everyday life activities. In addition, our sample contains participants with a body mass index (BMI) ranging from 22 kg/m2 to 35 kg/m2. However, larger study samples are needed to demonstrate whether glucose profile during each intervention is similar across the BMI spectrum.
The study has limitations. First, the participants were not restricted to perform exercise at a specific time during the day, which means that circadian factors could have affected glucose response to exercise.26 Second, the study may have been underpowered in order to detect the actual difference of 1% in time below range. We based our power calculation on an expected difference of 2% in time below 3.9 mmol/L. Third, the number of missing data on insulin dosing, carbohydrate intake, activity and sleep measurement, as well as the small sample size, limits the possibility of adjusting for these factors in the statistical analysis. Fourth, most of our included participants had a moderately active physical activity level and therefore the study results are limited to the particular group and may not be applicable for persons with a different activity level. We suggest similar studies in people habitually doing more intense exercise and studies comparing other distributions and frequencies of the exercise sessions. Fifth, we used the wrist-worn accelerometer to assess the physical activity level. A study by Chomistek et al27 showed that moderate to vigorous activity less than 10 min may not be recorded with accelerometers. Furthermore, dips may not be recorded as the wrist is not involved in these movements. Moreover, the ActiGraph is not validated for our specific training program with jumps, dips, and push-ups, which is why vigorous activity in general may be under-reported in our study. Lastly, most of our included participants were already moderately active and therefore the study results are limited to this particular group and may not be applicable for persons with different habitual activity levels.
Conclusion
Our findings suggest that performing exercise for 5 consecutive days does not reduce the percentage of time in hypoglycemia compared with similar amounts of exercise performed on 2 days over a 5-day period. If our results are confirmed in larger studies, people can be recommended to choose freely how to distribute their weekly exercise sessions.
Acknowledgments
The authors thank the study participants for giving their time to this study. Furthermore, the authors thank Christian Laugesen, PhD student, Steno Diabetes Center Copenhagen, for help with recruitment of participants.
References
Footnotes
Contributors IIKS, AGR, SS and KN conceived the idea and designed the study. IIKS performed the studies, analyzed the data and wrote and edited the manuscript. AGR analyzed the data and reviewed and edited the manuscript. SS and KN reviewed, edited and approved the final manuscript. IIKS, AGR and KN take full responsibility for the content of this article and are responsible for the integrity of the work as a whole.
Funding This study was funded by the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The Danish Diabetes Academy holds no rights to the study results.
Competing interests IIKS has received speaker grants from Roche Diabetes Care and Rubin Medical. SS has served on the continuous glucose monitoring advisory board of Roche Diabetes Care. KN serves as adviser for Medtronic, Abbott and Novo Nordisk A/S, owns shares in Novo Nordisk A/S, has received research grants from Novo Nordisk A/S, Zealand Pharma, Medtronic and Roche Diabetes Care, and has received fees for speaking from Medtronic, Roche Diabetes Care, Rubin Medical, Sanofi, Novo Nordisk A/S, Zealand Pharma and Dexcom. AGR declares no duality of interest associated with his contribution to this manuscript.
Patient consent for publication Not required.
Ethics approval The study was approved by the Regional Committee on Health Research Ethics (H-19035830) and the Danish Data Protection Agency (P-2019-373).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article. The protocol can be available from the corresponding author by email.