Article Text

Abstract
Introduction Lockdown measures have a profound effect on many aspects of daily life relevant for diabetes self-management. We assessed whether lockdown measures, in the context of the COVID-19 pandemic, differentially affect perceived stress, body weight, exercise and related this to glycemic control in people with type 1 and type 2 diabetes.
Research design and methods We performed a short-term observational cohort study at the Leiden University Medical Center. People with type 1 and type 2 diabetes ≥18 years were eligible to participate. Participants filled out online questionnaires, sent in blood for hemoglobin A1c (HbA1c) analysis and shared data of their flash or continuous glucose sensors. HbA1c during the lockdown was compared with the last known HbA1c before the lockdown.
Results In total, 435 people were included (type 1 diabetes n=280, type 2 diabetes n=155). An increase in perceived stress and anxiety, weight gain and less exercise was observed in both groups. There was improvement in glycemic control in the group with the highest HbA1c tertile (type 1 diabetes: −0.39% (−4.3 mmol/mol) (p<0.0001 and type 2 diabetes: −0.62% (−6.8 mmol/mol) (p=0.0036). Perceived stress was associated with difficulty with glycemic control (p<0.0001).
Conclusions An increase in perceived stress and anxiety, weight gain and less exercise but no deterioration of glycemic control occurs in both people with relatively well-controlled type 1 and type 2 diabetes during short-term lockdown measures. As perceived stress showed to be associated with glycemic control, this provides opportunities for healthcare professionals to put more emphasis on psychological aspects during diabetes care consultations.
- diabetes mellitus
- type 1
- type 2
- COVID-19
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Lockdown measures affect many aspects of daily life that are relevant for diabetes self-management, while access to diabetes care is changed.
What are the new findings?
In people with type 1 and type 2 diabetes lockdown measures during the COVID-19 pandemic resulted in increased stress and anxiety, weight gain and less exercise.
Despite these changes, no deterioration in glycemic control was present.
Increased stress was associated with difficulty in glycemic control.
How might these results change the focus of research or clinical practice?
Diabetes care professionals should take the psychological impact of lockdown measures into account when discussing diabetes self-management and well-being during consultations.
Introduction
The COVID-19 pandemic is a major healthcare crisis and has a major impact on daily life worldwide. With currently no vaccine or treatment available, this viral pandemic results in a rapid increase in morbidity and mortality rates. So far over 63 million cases have been confirmed, resulting in almost 1.5 million deaths worldwide.1
Mortality rates from COVID-19 are highest in elderly people.2
Also people with diabetes mellitus have been identified to be at increased mortality risk.2 Often no distinction is made between type 1 diabetes and type 2 diabetes. But as other risk factors for adverse outcomes of COVID-19 such as elderly age, obesity, hypertension and cardiovascular disease are very prevalent in type 2 diabetes, people with this diabetes subtype are considered to be at even higher risk.3
In an attempt to control the outbreak, many countries implemented lockdown measures.4 Lockdown strategies diverged from lockdown of cities, regions or countries to voluntary home curfews, travel restrictions and prohibition of public and social events.5 These measures resulted in major changes in daily life and social behavior. Such sudden and major disruptions in everyday life are known to influence both physical and mental health.6
The alterations in behavioral patterns, daily life and exercise as well as increased feelings of stress and anxiety are all known to influence diabetes self-management and glycemic control.7–14 Also a change in diabetes care by health professionals further increased the importance of adequate self-management behavior of people with diabetes mellitus. Thus, several factors coincided that challenged maintenance of glycemic control during the lockdown measures. It is unclear how the lockdown has a differential impact on people with type 1 and type 2 diabetes and whether the presence of additional risk factors for severe outcomes of COVID-19 in these people plays a role.
Methods
People with type 1 and type 2 diabetes that were treated at the diabetes outpatient clinic of the Leiden University Medical Center were invited to participate. Other inclusion criteria were age ≥18 years, sufficient comprehension of the Dutch language and ability to perform fingerpricks and complete an online supplemental questionnaire. People that were pregnant, recently (≤6 months) diagnosed with a malignancy, receiving immunotherapy or chemotherapy or admitted to a hospital or rehabilitation centre were excluded from participation.
Supplemental material
Lockdown period and measures taken
Lockdown measures were implemented in the Netherlands on 15 March 2020 by the government. These measures included stay-at-home orders for people working in non-vital areas of society, social distancing and closures of schools, restaurants, bars and public spaces. A sudden reduction in mobility around the workplace (40%) and in the context of retail and recreation (40%) and an increase in mobility around residential grounds (20%) occurred immediately after March 15 as shown by mobility data of the Dutch population validating the effect of the lockdown measures.15 Because of the measures taken and the results of the mobility data, March 15 was considered the start of the lockdown period. Data were collected 8–11 weeks after the start of the lockdown period. During the entire data collection period, the lockdown measures were maintained.
Assessment of the impact of the lockdown period
After informed consent was provided, participants received a link to the online supplemental questionnaire via email. The online supplemental questionnaire consisted of multiple items to assess the impact of the lockdown on glycemic control and medication use, daily routines, physical activity and psychological stress, including the ‘Perceived Stress Scale’.16
A hemoglobin A1c (HbA1c) fingerprick set was sent to the participant’s home in order to prevent visits to the hospital. This set consists of a small tube, a lancet and a return medical envelope. Via a fingerprick a small amount of capillary blood was collected in a tube by patients at home, which was then sent to the hospital laboratory by mail.17 This is a validated and well-established measuring method for HbA1c analysis, providing identical results compared with HbA1c measurements in venous blood samples.18
HbA1c 8–11 weeks (interval median (IQR) 65 (61–71) days) after the start of the lockdown period was compared with the last known HbA1c before 15 March 2020 (interval median (IQR) 178 (137–218) days before the start of the lockdown).
For people with type 1 diabetes using a continuous glucose monitor (CGM) or flash glucose monitor (FGM) data were analysed during 2 weeks before the lockdown period (24 February until 8 March) and 6 weeks after the start of the lockdown period (24 April until 7 May). Online data sharing platforms were used to gain access to those data. If participants were on holiday during one or both of these weeks prior to the lockdown period, they provided the data of two adjacent regular weeks prior to the lockdown period. As a recent start of FGM or CGM can improve glycemic control, people who had started CGM or FGM within 2 months of the start of the lockdown period were excluded from glucose sensor data and HbA1c analysis. CGM or FGM data were used to calculate time below range (% of time glucose <4.0 mmol/L), time in range (% of time glucose 4.0–10.0 mmol/L), time above range (% of time glucose ≥10.0 mmol/L), the coefficient of variation (% CV), the time of active use (% of time) and the average number of scans per day (n).
Statistical analysis
Differences in questionnaire outcomes between people with type 1 and type 2 diabetes were analysed using χ2 tests. The change in glycemic control was analysed by paired t-tests. Differences in change in HbA1c between people with type 1 diabetes and type 2 diabetes were analysed using unpaired t-tests. Regression analyses were used to assess associations between glycemic parameters, body mass index (BMI) and outcomes on lifestyle, insulin use, glucose regulation and stress. CIs of the regression coefficients are reported. People were divided into tertiles based on their HbA1c prior to the lockdown period and associations with questionnaire outcomes were analysed using ordinal logistical regression analysis. We performed complete case analyses. STATA V.14.2 was used to perform the analyses.
Results
A total of 435 participants (42% female) were included (type 1 diabetes n=280, type 2 diabetes n=155) (table 1). A basal-bolus regimen was used by 76.8% and basal insulin only by 8.3% of people. People with type 2 diabetes were on average 12.3 years older and had a higher BMI (table 1). The prevalence of cardiovascular complications, elevated systolic blood pressure and use of blood pressure-lowering agents was higher in people with type 2 diabetes (table 1).
Baseline characteristics
Stress, weight change and exercise
In total, 399 participants completed the questionnaire on daily routines, physical activity, psychological stress and participant’s glycemic control and medication use (online supplemental table 1).
Supplemental material
During self-lockdown 34.1% of all participants reported elevated stress (figure 1), without any difference between people with type 1 and type 2 diabetes (33.6% vs 35.1%, Perceived Stress Score: 13.7 (±6.2) vs 12.8 (±6.7), respectively). A change in perceived stress was associated with a change in HbA1c (95% CI 0.015 to 0.38, p=0.034). People who reported more difficult glycemic control experienced higher stress during the lockdown period (95% CI 0.41 to 0.83, p<0.0001) and needed more insulin than before the lockdown period (95% CI 1.35 to 2.08, p<0.0001). Furthermore, 27.3% of all participants reported elevated levels of anxiety (figure 1), without any difference between people with type 1 and type 2 diabetes (27.5% vs 26.9%). Anxiety for COVID-19 infection was not associated with the change in HbA1c.
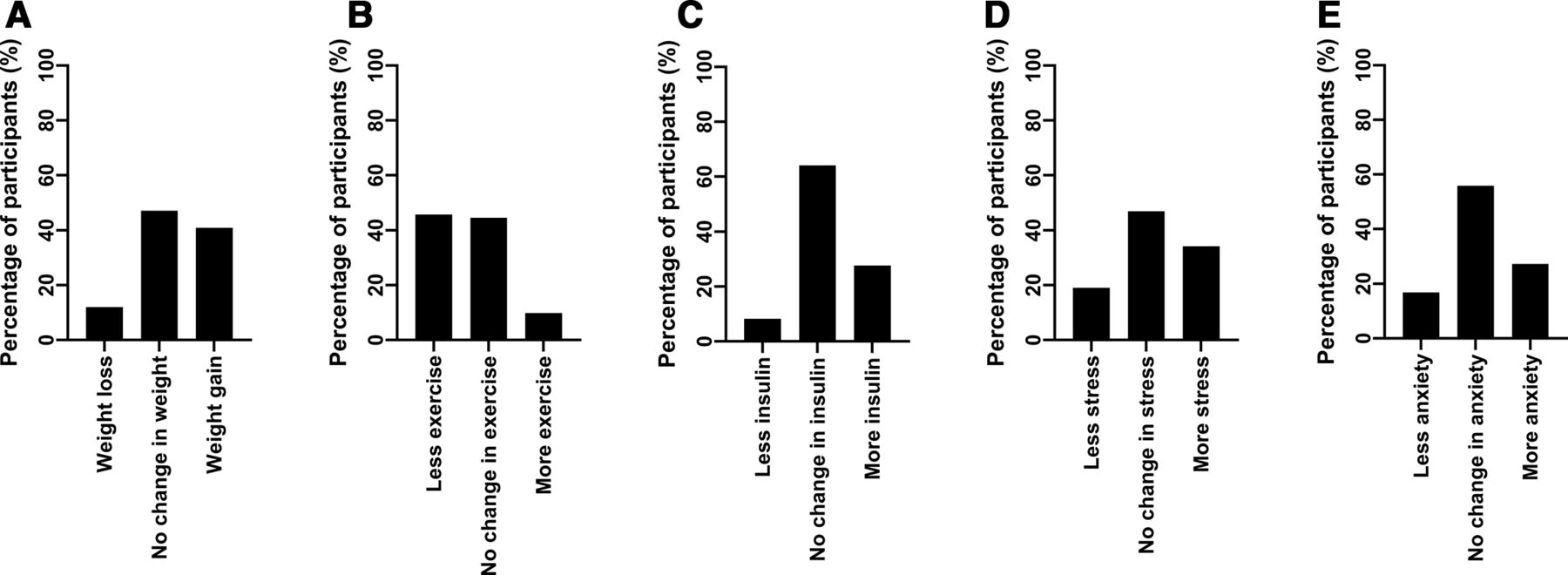
Change in self-reported weight (A), exercise (B), insulin use (C), perceived stress (D) and anxiety (E) during the lockdown period. (A) Weight loss: sum of percentage of participants in different categories of weight loss (online supplemental table 1). Weight gain: sum of percentage of participants in different categories of weight gain (online supplemental table 1). (C) Less insulin: sum of percentage of participants in different categories of less insulin use. More insulin: sum of percentage of participants in different categories of more insulin use. (D) Less stress: sum of percentage of participants in categories of less stress. More stress: sum of percentage of participants in different categories of more stress. (E) Less anxiety: sum of percentage of participants in different categories of less anxiety. More anxiety: sum of percentage of participants in different categories of more anxiety.
Furthermore, 40.9% of the participants reported weight gain and 45.7% reported less exercise than before (figure 1). Only 12% of the participants reported a loss of weight and 10% of the participants reported more exercise. Less exercise was associated with weight gain during the period of self-lockdown (p<0.0001). The change in exercise or weight gain was not associated with the change in HbA1c (95% CI −0.20 to 0.05, p=0.25 and 95% CI −0.002 to 0.39, p=0.053, respectively).
Impact of lockdown measures on glycemic control
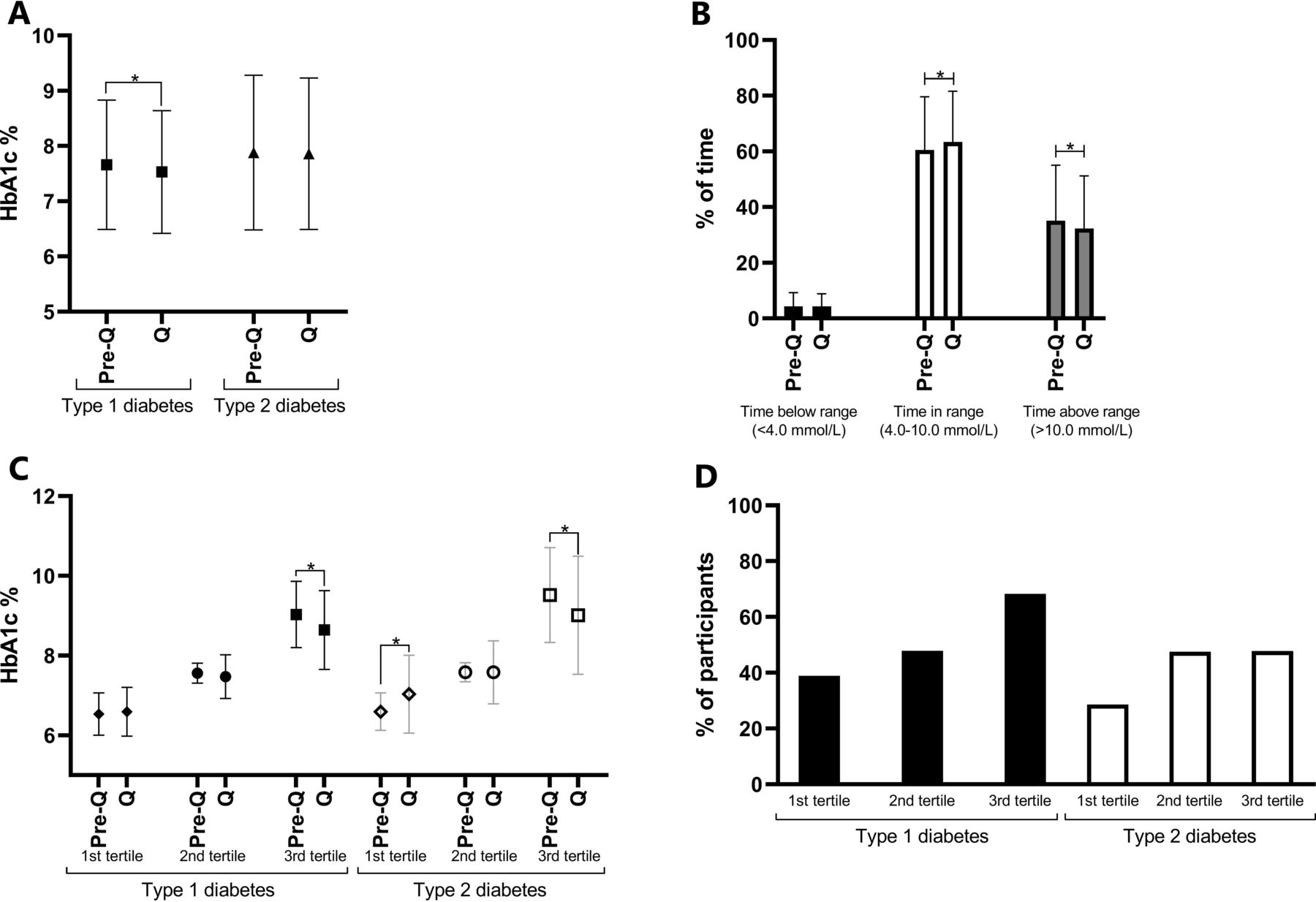
HbA1c was slightly lower in people with type 1 diabetes in the lockdown period (pre-lockdown 7.68%±1.2 (60.4±12.7 mmol/mol) vs lockdown 7.52%±1.1 (58.7±12.2 mmol/mol), p<0.0001) but not in people with type 2 diabetes (figure 2A). Glucose monitoring data reflected this improvement in HbA1c in people with type 1 diabetes. Time in range was higher (pre-lockdown 60.5% vs lockdown 63.4%, p=0.0009) and time above range was lower (pre-lockdown 34.6% vs lockdown 32.1%, p<0.003) (figure 2B). Glucose variability did not change. There was more frequent active glucose monitoring with an increase in the number of FGM scans per day (pre-lockdown 9.6 (±6.5) vs lockdown 11.8 (±8.1) scans/day, 95% CI −3.81 to −0.58, p<0.01) in people with type 1 diabetes indicating more focus on self-management.
{kind=link}
{kind=link}
(A) Hemoglobin A1c (HbA1c) before the lockdown period (pre-Q) and during the lockdown period (Q) in people with type 1 diabetes and type 2 diabetes. (B) Ambulatory glucose profiles before and during the lockdown period in people with type 1 diabetes (n=90). (C) HbA1c per tertile before (pre-Q) and during (Q) the lockdown period in people with type 1 diabetes and type 2 diabetes. First tertile: type 1 diabetes mellitus (T1DM): HbA1c 4.92%–7.22%, type 2 diabetes mellitus (T2DM): 5.43%–7.20%; second tertile: T1DM: 7.23%–8.09%, T2DM: 7.23%–8.02%; third tertile: T1DM: HbA1c 8.13%–12.18%, T2DM: HbA1c 8.16%–12.72%. (D) Percentage of people with type 1 and type 2 diabetes with improvement of HbA1c per tertile. HbA1c was available for 339 participants.
Both people with type 1 and type 2 diabetes that were in the highest pre-lockdown tertile of HbA1c (type 1 diabetes: HbA1c 8.13%–12.18%, type 2 diabetes: HbA1c 8.16%–12.72%) showed improvement in HbA1c (type 1 diabetes: −0.39%, 95% CI 0.22 to 0.55 %, p<0.0001, type 2 diabetes: −0.62%, 95% CI 0.22 to 1.03%, p=0.0036) (figure 2C). Proportionally more people with type 1 diabetes in the highest HbA1c tertile group showed improvement in HbA1c compared with people with type 2 diabetes in that tertile (figure 2D).
Risk factors for a more severe outcome of COVID-19
BMI, presence of cardiovascular disease, systolic blood pressure or use of blood pressure-lowering agents was not associated with a change in stress or HbA1c during the lockdown period.
Discussion
People with diabetes mellitus are considered a high-risk population prone to a complicated course of COVID-19 and associated mortality.19 Here, we show that in people with relatively well controlled type 1 and type 2 diabetes the COVID-19 pandemic and lockdown measures increased stress and resulted in weight gain and less physical exercise during this short observational period. However, despite these factors no deterioration in glycemic control was observed.
Previous research has shown a lockdown to be associated with increased levels of emotional distress and anxiety,5 6 which is in line with our findings. Distress, as well as changes in daily structures and behavior, which were inevitable due to the lockdown period, are known to influence diabetes self-management and glycemic control.7–10 Adding to this challenge of maintaining glycemic control was the increased emphasis on diabetes self-management due to a shift to COVID-19 care and social distancing rules in hospitals, which led to cancellations of face-to-face consultations, and the use of telemedicine. The small overall improvement in HbA1c in people with type 1 diabetes (−0.16%) may be statistically significant but clinically not relevant. Together with an increase in scans of glucose sensors, these results indicate an increased focus on self-management. However, it should be noted that seasonal variation in glycemic control has been shown and higher temperatures are associated with lower HbA1c.20 21 Thus, the small improvement in glycemic control could be due to a seasonal variation in our and other studies. Our results also indicate that the presence of more risk factors for a severe outcome of COVID-19, such as a higher BMI, cardiovascular comorbidities and hypertension, was not associated with stress, anxiety or change in HbA1c.
One of the main strengths of our study is the large study population, consisting of both people with type 1 and type 2 diabetes. We were able to assess changes in psychological stress, body weight and exercise providing important insight in participant’s daily life during the lockdown period and knowledge about potential opportunities for improvement of diabetes care. The large study population allowed us to investigate these factors both in people with good and poor glycemic control, and we used both HbA1c and glucose monitoring data. For people with type 1 diabetes, our findings are in line with flash glucose monitoring data in a small group of 55 people, in which a small improvement in time in range and time above range was observed.22
A limitation of the study is the reliance on self-reported data due to restricted access to health facilities during the lockdown period. Self-reported data about weight change are often an underestimation of the actual change in weight.23 So the proportion of participants that increased in weight may be even larger. Furthermore, while HbA1c reflects glycemic control during the previous 3 months, the lockdown period had only been going on for 8–11 weeks at the time that the HbA1c measurement was performed and may underestimate the impact of lockdown on glycemic control. It should also be noted that most of the people with diabetes who participated in the study were relatively well controlled. In addition, most participants with type 2 diabetes used insulin. Therefore, the results are not representative for all people with diabetes, especially for people with type 2 diabetes as the majority of them do not need insulin treatment and are treated in primary care.
Poor glycemic control is considered a risk factor for adverse outcomes of infections.24–26 Although no data are available, the message that poor glycemic control poses a higher risk is often conveyed to people in the context of COVID-19.27 We found a decrease of HbA1c in the group with the poorest glycemic control. People who experienced most difficulty with glycemic control also experienced more stress. Potentially, people with the poorest glycemic control may have put more emphasis on glycemic control in order to cope with the increased stress levels, ultimately improving their HbA1c values during the lockdown period. However, also for this subanalysis seasonal effects in HbA1c cannot be completely excluded.
In conclusion, our short-term observational study shows that lockdown measures resulted in increased levels of perceived stress, weight gain and less exercise in both people with relatively well-controlled type 1 and type 2 diabetes, however this did not negatively impact glycemic control. Additional risk factors for adverse outcomes of COVID-19, including poor glycemic control, do not appear to influence this effect. Since a third of the participants reported elevated levels of stress, associated with difficulties in glycemic control, diabetes care professionals should take these aspects into account when discussing diabetes self-management and well-being during consultations.
Acknowledgments
The authors would like to thank the people from the outpatient hospital clinic of the LUMC for participating in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MMR, HR, SDH and EJPdK designed the study and developed the methodology. MMR, HR and CPL coordinated the field work. MMR analyzed the data, wrote the manuscript and interpreted the results. HR, SDH and EJPdK reviewed the analysis, interpretations and manuscript and did the final review. CPL, MS, IJ, MFN, HP, BEPBB and OD reviewed the analysis and manuscript. MMR is the guarantor of this work and, as such, had access to all data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Medical Ethics Committee of Leiden, Den-Haag, Delft under the Medical Research Involving Human Subjects Act (WMO) prior to the start of the study (NL73778.058.20).
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request. The data used in this article can be requested at the Leiden University Medical Center.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.