Article Text

Abstract
Introduction Insulin pump access in type 1 diabetes may be inequitable. We studied the association between government funding programs for insulin pumps and rates of insulin pump use and disparities between pump users and non-users.
Research design and methods Adults with type 1 diabetes were identified in the National Diabetes Repository, a primary care electronic medical record database of individuals with diabetes from five Canadian provinces. Proportions of individuals using insulin pumps were compared between provinces with and without pump funding programs. Multivariable logistic regression models were used to estimate the odds of insulin pump use adjusting for confounders. Univariate logistic regression models were used to estimate the odds of insulin pump use according to each predictor, according to pump funding program status.
Results Of 1559 adults with type 1 diabetes, proportions using insulin pumps were 47.8% (95% CI 45.1% to 50.5%) and 37.7% (95% CI 31.5% to 44.1%) in provinces with and without pump funding programs (p=0.0038). Adjusting for age, sex, HbA1c, income quintile, and rural/urban location, the OR for insulin pump use was 1.45 (1.08–1.94) for provinces with pump funding programs compared with provinces without. Higher income was associated with a greater odds of insulin pump use in provinces with pump funding programs, and rural/urban location was not associated with insulin pump use.
Conclusions Insulin pump use is more common in regions with government funding programs. Further research is required to best understand and comprehensively address persistent income disparities between pump users and non-users despite the availability of reimbursement programs.
- insulin pump
- clinical epidemiology
- health services research
- diabetes mellitus
- type 1
Data availability statement
Data may be obtained from a third party and are not publicly available. Data is de-identified electronic medical record data maintained by Diabetes Action Canada in the National Diabetes Repository (https://repository.diabetesaction.ca/). Data is available only upon request to approved investigators and after review by a Research Governing Committee.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Insulin pump therapy, though costly, has a number of benefits for people living with type 1 diabetes.
There are significant disparities in insulin pump use related to social determinants of health such as income and ethnicity.
It is unknown how universal funding programs for insulin pump therapy address inequities in insulin pump use.
What are the new findings?
Insulin pump use was more common in Canadian provinces with government-funded insulin pump programs (48% vs 38%).
Residing in provinces with government-funded insulin pump programs was independently associated with greater odds of insulin pump use compared with residing in provinces without pump funding programs.
Even in provinces with pump funding programs, lower income is associated with lower odds of insulin pump use.
How might these results change the focus of research or clinical practice?
Given the benefits of insulin pump therapy including emerging closed-loop systems, further efforts are required to improve equitable access to insulin pump therapy.
Introduction
In type 1 diabetes, intensive insulin therapy targeting a hemoglobin A1c (HbA1c) ≤7.0% is the standard of care and can be delivered by two methods: multiple daily injections of insulin (MDI), or continuous subcutaneous insulin infusion, also referred to as insulin pump therapy.1 Potential advantages of insulin pump therapy compared with MDI include improved glycemic control, reduced rate of severe hypoglycemia, greater flexibility, and higher quality of life.2–6 Although insulin pump therapy is more expensive than MDI (annual expenses of $C6247.18 for insulin pump therapy vs $C4949.49 for MDI),7 it has been found to be cost-effective.7 8
Despite the benefits and cost-effectiveness of insulin pump therapy, inequitable access to insulin pump therapy remains a concern. Indeed, among adults with type 1 diabetes, individuals who are older, male, ethnic minorities, or of lower income are significantly less likely to use insulin pumps.9–13 These differences have been observed in both countries with insulin pump funding programs (New Zealand, Denmark, France)9–11 and those without (USA, Brazil).12 13 The costs for insulin pump therapy may be paid out of pocket through private insurance coverage (which is only available for some individuals) or through government funding programs. Whether government-funded insulin pump programs result in more equitable insulin pump use is currently unknown.
In Canada, healthcare is delivered provincially with funding models for insulin pump therapy differing by province (online supplemental table 1). Thus, Canada is an ideal model for conducting a ‘natural experiment’ assessing the impact of government funding for insulin pump therapy on rates and equity of insulin pump use, which would be broadly applicable to other regions. We recently derived and validated algorithms identifying type 1 diabetes in a Canadian primary care electronic medical record (EMR) database, permitting for the first time the ability to compare pump users to non-users in Canadian EMR databases.14 We used the Diabetes Action Canada (DAC) National Diabetes Repository,15 which consists of primary care EMR data for patients with diabetes from five provinces throughout Canada. Of these, the Ontario and Alberta provincial governments provide funding for insulin pumps and a portion of supplies for individuals with type 1 diabetes of all ages.16 17 In contrast, the provincial governments in Manitoba and Quebec offer reimbursement only for children younger than 18 years old.18 19 In Newfoundland, government funding for insulin pump therapy has been provided for children and adults under the age of 25 since 2010, though it was recently announced that the program will expand to adults of all ages.20
Supplemental material
In this study, our primary objective was to determine whether the rate of insulin pump use in adults with type 1 diabetes is higher in provinces with government-funded insulin pump programs compared with provinces without. Our secondary objective was to determine whether characteristics of pump users and non-users differ between provinces with and without government-funded insulin pump programs. We hypothesized that insulin pump use would be more common in provinces with government-funded insulin pump programs, and there would be greater disparities between pump users and non-users in provinces without government-funded insulin pump programs.
Research design and methods
Study design and setting
This was a cross-sectional analysis using primary care EMR data from five provinces (Alberta, Manitoba, Ontario, Quebec, and Newfoundland), which in total account for approximately 78% of the Canadian population.21Although Canada employs a universal healthcare system, the delivery of health services, such as insulin pump therapy for type 1 diabetes, is overseen by individual provinces and territories. This study was designed and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and the Reporting of Studies Conducted Using Observational Routinely Collected Health Data statement.22 23
Data sources
This study used the DAC National Diabetes Repository, which consists of deidentified clinical data for individuals with diabetes obtained from the EMR of participating primary care providers (family physicians and nurse practitioners).15 The data are processed and stored in a single, secure virtual environment in Ontario, Canada.15 Available data include patient demographic characteristics, comorbidities, risk factors, physical and laboratory examinations, and medication prescriptions. Currently, there are approximately 100 000 individuals included in the DAC National Diabetes Repository.
Participants
Eligible subjects for this study were individuals with type 1 diabetes aged >18 years with an EMR encounter between 1 January 2015 and 30 June 2019. Type 1 diabetes was identified by a previously validated algorithm defined by prescription of insulin without any other antihyperglycemic medications and age younger than 55 years old (sensitivity 72.8%, specificity 99.5%, positive predictive value 86%, negative predictive value 99%). Thus, only individuals with type 1 diabetes between the ages of 18 and 55 were identified.14 The absence of robust free text data within the National Diabetes Repository precluded the use of other EMR algorithms for identifying type 1 diabetes.
Exposures, covariates and outcomes
All variables were assessed using encounter data for the 2 years prior to the most recent visit date. The primary exposure was the presence or absence of a government-funded insulin pump program for the province in which an individual resided, which was present for Ontario, Alberta, and Newfoundland (if age ≤25 in Newfoundland), and absent for Manitoba, Quebec, and Newfoundland (if age >25 in Newfoundland).
The primary outcome was the proportion of individuals with type 1 diabetes using insulin pumps. Insulin pump use was identified based on the prescription of only bolus insulin without basal, mixed, or regular insulin. One prescription per year for basal insulin was permitted to account for pump users receiving a ‘back up’ insulin prescription for emergency use.
Covariates included age, sex, neighborhood-level income quintile, location of residence (rural or urban), comorbidities (depression, hypertension, cardiovascular disease, which have been previously validated in the DAC National Diabetes Repository), medications, and laboratory values. Each individual was assigned a neighborhood-level income quintile based on postal code and before tax income for the corresponding census metropolitan area using standard Statistics Canada methodology, with 1 being the lowest income quintile and 5 being the highest.
Statistical methods
Sample size calculations were based on a conservative estimate of the current prevalence of type 1 diabetes among adults in Canada. We estimated that 5% of all patients between the ages of 18 and 55 with diabetes in the DAC National Diabetes Repository had type 1 diabetes, resulting in an estimated 939 patients in provinces with government-funded insulin pump programs and 207 in provinces without government-funded insulin pump programs. We hypothesized that 33% of patients would use insulin pumps in provinces with government-funded insulin pump programs and 20% would use insulin pumps in provinces without government-funded insulin pump programs. Given our estimated sample size, this provided >90% power to detect a difference of at least this magnitude.
Descriptive statistics were used to compare characteristics (demographics, socioeconomic status factors, comorbidities, medications and laboratory values) between individuals living in provinces with and without government-funded insulin pump programs. Continuous variables were compared by Student’s t-tests or Wilcoxon rank-sum depending on normality of distribution, and categorical variables were compared by χ2. The proportion of individuals with type 1 diabetes using insulin pumps with corresponding 95% CIs was determined separately for provinces with government-funded insulin pump programs and provinces without.
The OR for insulin pump use according to presence or absence of a government-funded insulin pump program was determined using logistic regression. This analysis was performed as: (1) unadjusted; (2) adjusted for age, sex, HbA1c (also assessing for an interaction between sex and status of government-funded insulin pump program); and (3) adjusted for previous covariates and income quintile and rural or urban location of residence. Univariate logistic regression models were used to determine associations between characteristics (demographics, socioeconomic status factors, comorbidities, medications and laboratory values) and the odds of insulin pump use, according to the presence or absence of government-funded insulin pump programs.
Missing data were assumed to be missing at random and multiple imputation was used for missing data in multivariable models.
Sensitivity analyses
Sensitivity analyses were performed using generalized estimating equation (GEE) models as an alternative to logistic regression models in order to account for clustering by primary care clinic site. The most influential variable for clustering would likely be diabetes specialist or diabetes clinic site, but these variables were not available in this primary care database, thus the analyses accounting for clustering by primary care clinic were chosen as sensitivity analyses. Sensitivity analyses using complete case analyses for missing data instead of multiple imputation were also performed.
Statistical analyses were performed using SAS (V.9.4) software (SAS Institute). P values <0.05 were considered statistically significant.
Patient and public involvement
Patient partners with lived experience with type 1 diabetes were consulted in the planning of this study and interpretation of results.
Results
Participant characteristics
Of the 95 699 individuals with an EMR encounter between 1 January 2015 and 30 June 2019 in the DAC National Diabetes Repository, 1559 were identified as adults with type 1 diabetes and meeting all of the inclusion criteria (online supplemental figure 1). Of these, 1320 lived in provinces with government-funded insulin pump programs and 239 lived in provinces without government-funded insulin pump programs.
Baseline characteristics of study participants by the main exposure (residing in a province with an insulin pump program vs no pump program) are presented in table 1. Characteristics according to province type and pump use or non-use are also shown in online supplemental table 2. Individuals living in provinces with and without insulin pump funding programs were of similar age (40 years (IQR 31–49) vs 41 years (IQR 33–39), p=0.33) and sex distribution (47% vs 49% female, p=0.53). Individuals in provinces with insulin pump funding programs had older primary care providers (51 years (IQR 41–59) vs 47 years (IQR 37–55), p<0.0001) and a greater proportion of female primary care providers (43% vs 33%, p=0.0003). Individuals in provinces with insulin pump funding programs had a lower HbA1c compared with provinces without insulin pump funding programs (8.44%±1.99% vs 8.86%±2.04%, p=0.0013). There were no differences in income quintile distribution between individuals living in provinces with insulin pump funding programs compared with those without.
Characteristics of participants in provinces with and without government-funded insulin pump programs
Proportion of adults with type 1 diabetes using insulin pumps
Six hundred and thirty-one individuals used insulin pumps in provinces with pump funding programs and 90 used insulin pumps in provinces without pump funding programs. The proportion using insulin pumps was higher in provinces with insulin pump funding programs compared with provinces without (47.8% (95% CI 45.1% to 50.5%) vs 37.7% (95% CI 31.5% to 44.1%), p=0.0038, figure 1).
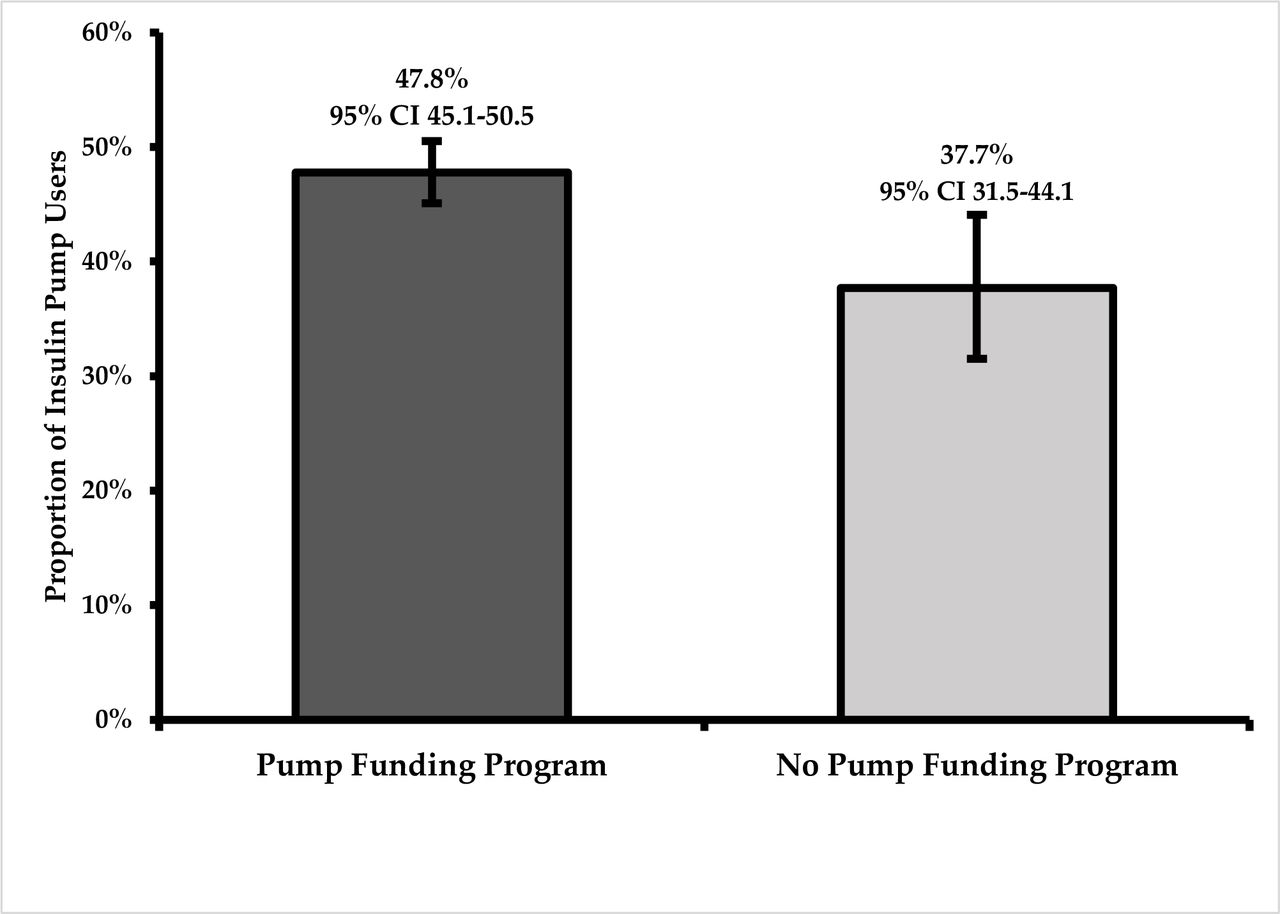
Proportion of individuals using insulin pumps in provinces with and without government-funded insulin pump programs.
Association between pump funding program and insulin pump use
Logistic regression models were used to assess the association between insulin pump funding program status (yes/no) on the odds of insulin pump use (table 2). In an unadjusted model, the presence of an insulin pump funding program was associated with greater odds of insulin pump use (OR 1.52, 95% CI 1.14 to 2.01). This effect persisted after sequentially adjusting for potential confounders. The OR was 1.46 (95% CI 1.10 to 1.945) after adjustment for age, sex, and HbA1c, and 1.43 (95% CI 1.05 to 1.94) after adjustment for age, sex, HbA1c, income quintile and urban versus rural residence. There was no interaction between sex and pump funding program status (p=0.15) and thus an interaction term was not included in any model. Older age, male sex and higher HbA1c were associated with lower odds of using an insulin pump. Higher income quintile was independently associated with greater odds of insulin pump use (OR 1.56, 95% CI 1.00 to 2.43 for highest vs lowest income quintile).
Odds of insulin pump use adjusting for pump funding program status and other characteristics
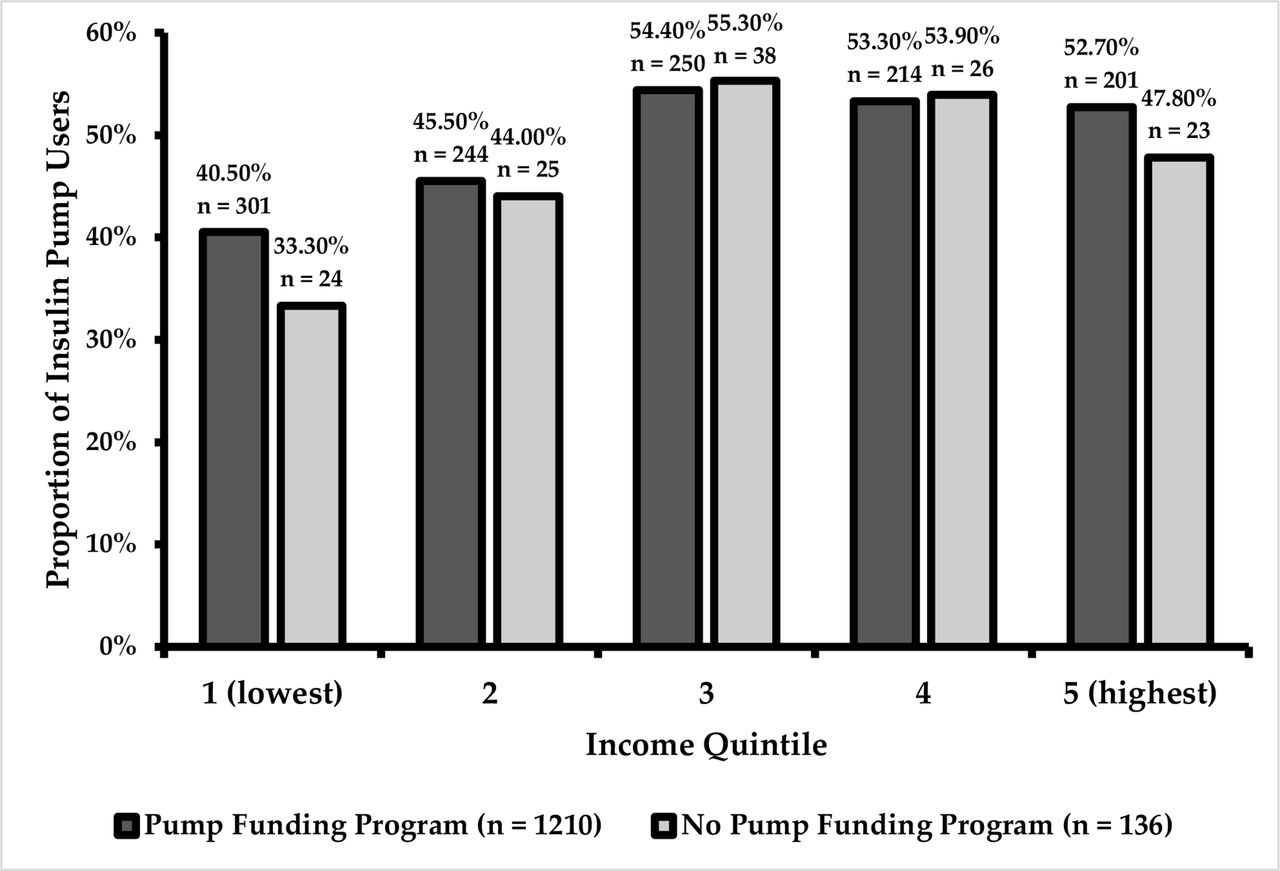
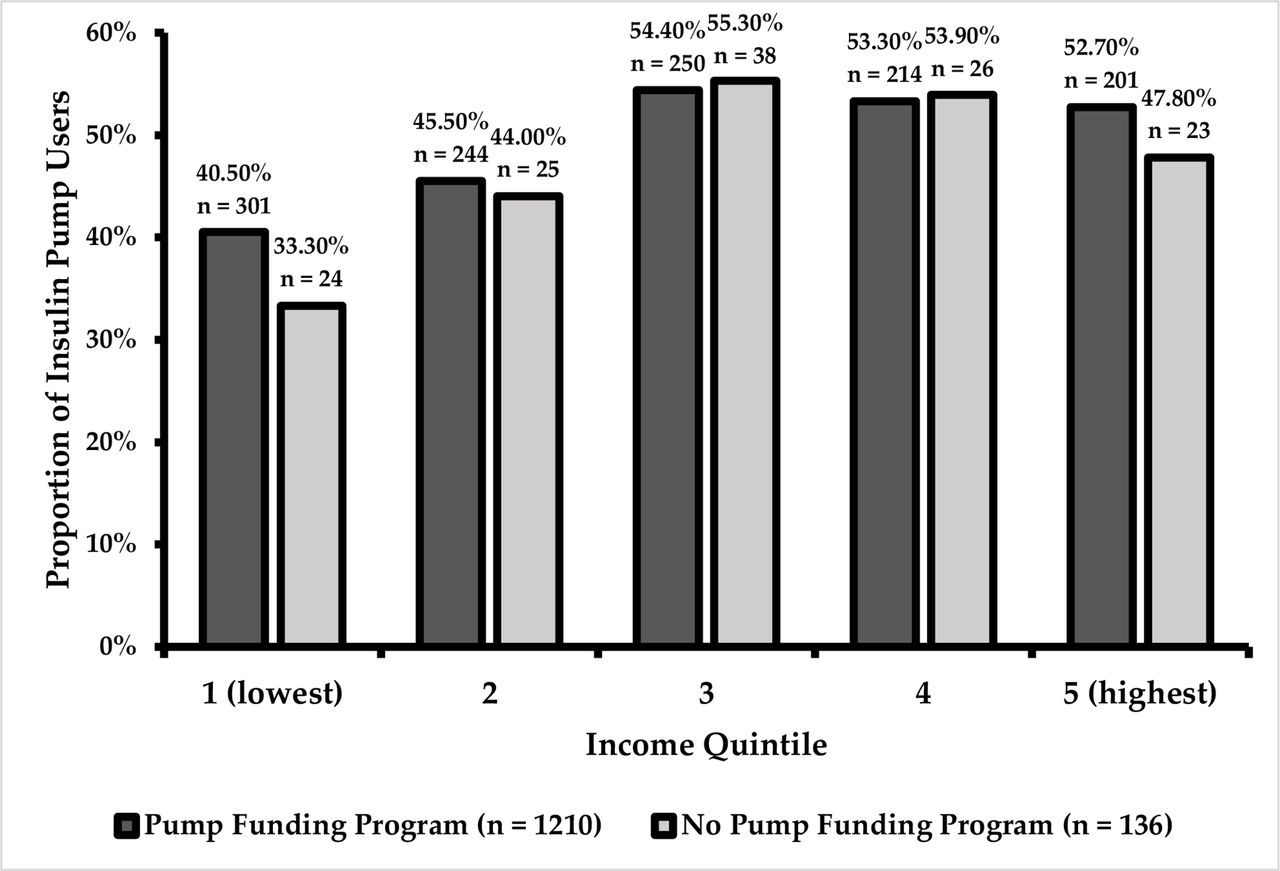
The association between each predictor and insulin pump use was also determined using unadjusted logistic regression models according to the presence or absence of an insulin pump funding program (table 3). Males and individuals with depression were less likely to use insulin pumps in provinces with pump funding programs but not provinces without (0.77 (95% CI 0.62 to 0.96) vs 0.94 (95% CI 0.55 to 1.58) for male sex; 0.69 (95% CI 0.55 to 0.87) vs 1.00 (95% CI 0.55 to 1.83) for depression). Individuals in higher income quintiles were more likely to use insulin pumps in provinces with insulin pump funding programs (figure 2). In provinces without insulin pump funding programs, a similar trend for the association with income quintile was observed although not statistically significant; however, the sample sizes were smaller and the CIs were wide.
Association between individual characteristics and odds of insulin pump use according to pump funding program status
{kind=link}
{kind=link}
Proportion of individuals using insulin pumps by income quintile in provinces with and without government-funded insulin pump programs. P values from lowest to highest income quintile: 0.52, 1.00, 1.00, 1.00, 0.67. P values were calculated with χ2 using Fisher’s exact test.
Sensitivity analyses
All multivariable models were repeated using complete case analysis rather than multiple imputation and results were consistent with the primary analysis (data not shown). In addition, all multivariable models were repeated using GEEs that accounted for clustering by primary care clinic and results are presented in online supplemental tables 3 and 4. As expected with GEE models, CIs were wider for all estimated ORs. The OR for the association between pump program and odds of insulin pump use was consistent with the primary analysis. The findings for the associations between age, sex and HbA1c and the odds of insulin pump use were unchanged (online supplemental table 2).
Conclusions
In this cross-sectional study comparing insulin pump use in Canadian provinces with and without government-funded insulin pump programs for adults with type 1 diabetes, insulin pump use was more common in provinces with pump funding programs compared with provinces without. After adjustment for potential confounders, individuals living in provinces with government-funded insulin pump programs were approximately 50% more likely to use insulin pumps compared with provinces without funding programs. This is important because insulin pump therapy may improve glycemic control, reduces the rate of severe hypoglycemia, and is associated with greater quality of life.2–6 While we hypothesized that government-funded insulin pump programs may remove financial barriers to insulin pump use, we found a substantial residual association of higher income with insulin pump use even in provinces with pump funding programs. Therefore, these findings suggest that while government funding may improve access to insulin pumps, they may inadvertently favor those of higher socioeconomic status.
The total proportion of individuals using insulin pumps in this study was 46%, which may be an overestimate due to our definition of pump use based on insulin prescriptions. Furthermore, our algorithm restricted identification of type 1 diabetes to individuals between the ages of 18 and 55 and, since insulin pump use is more common in younger ages, this might have also inflated the proportion of pump users in both provinces with and without insulin pump funding programs.24 There is limited knowledge of the true proportion of insulin pump use among individuals with type 1 diabetes in Canada currently, and our study provides the only estimates to date among adults in population-based samples for many provinces. Insulin pump use in the current study is similar to 44% reported in the Canadian Study of Longevity in Diabetes, although that study represented a selected cohort of older individuals with type 1 diabetes and was susceptible to volunteer bias.25 In a population-based study using Ontario primary care EMR data, the proportion of adults with type 1 diabetes using insulin pumps was 32%.14 Among the pediatric population (<18 years old) in Ontario, the proportion using insulin pumps in 2012 was reported as 38%, though this has likely increased since.26 Internationally, the reported proportions of individuals with type 1 diabetes using insulin pumps in countries with government-funded insulin pump programs are also lower than observed in the current study (eg, 11% for all ages in New Zealand,9 20% for all ages in Sweden,27 21% for adults in Denmark,11 and 37% for adults in Germany and Austria24). Australia, a country with no funding program for insulin pumps, has reported insulin pump use among only 10% of individuals of all ages with type 1 diabetes.28 Even though we may have overestimated the number of individuals using insulin pumps, this would have been a non-differential bias, affecting individuals in provinces with and without pump funding programs similarly. Thus, the 10% difference in pump use between provinces with and without pump funding programs is valid, even if the absolute numbers of pump users within each type of province may be overestimated.
Socioeconomic disparities between pump users and non-users have been well described. The cost of insulin pumps and supplies are the most commonly reported barrier by patients against initiation of insulin pump therapy,29 and insulin pump use is consistently less common among lower income individuals compared with higher income individuals, even in countries with government-funded insulin pump programs.12 13 This is consistent with the pediatric population in Ontario, as patients from lower income backgrounds are less likely to use insulin pumps and more likely to discontinue pump therapy.30 In Brazil, where insulin pumps are paid out of pocket, pump users have higher levels of education than non-users.12 This may be explained by the tendency for practitioners to prescribe insulin pump therapy to individuals who they believe are ‘more educationally able’ to operate an insulin pump.31 In addition, education and income are correlated.32 Ethnic minorities are also consistently less likely to use insulin pumps.9 12 13 For example, in the USA, insulin pump use is significantly lower among individuals from Black and Hispanic backgrounds,13 while in New Zealand, this disparity is noted for individuals from Maori, Asian, and Pacific backgrounds.9 Although numerous explanations for this ethnic disparity may exist, having a non-English primary language may be an additional barrier to insulin pump use.33 Finally, area of residence may also influence insulin pump accessibility, with wide geographic variation in the rate of insulin pump use evident within many countries.9 11 34 Individuals living in rural areas are less likely to be prescribed insulin pump therapy compared with urban areas,35 which may be explained by differences in access to medical centers with greater resources for managing patients using insulin pumps.36
Our study showed higher rates of insulin pump use in provinces with pump funding programs, which may be due to minimizing financial barriers. However, we observed persistent disparities in income quintile even in provinces with pump funding programs, and the disparities by income quintile were not greater in provinces without pump funding programs as would have been expected. Differences in insulin pump use within each income quintile by pump funding program status were greatest in the lowest income quintile (insulin pump use was 7% higher in provinces with pump funding programs) and the highest income quintile (pump use was 5% higher in provinces with pump funding programs), whereas the rates of insulin pump use were more similar in the middle-income quintiles. Although it is unclear why this disparity would be higher in the highest income quintile, these results must be interpreted with caution since sample sizes by income quintile were small for provinces without pump funding programs, and differences within income quintiles were not statistically significant. Additionally, this may have been due to insensitive measures for socioeconomic variables since education, ethnicity, occupation and primary language were not available in the database, and income quintile was based on neighborhood averages. Furthermore, removing financial barriers to insulin pumps may not be sufficient for overcoming barriers to insulin pump use. Residual barriers might include insufficient resources for supporting insulin pump therapy, such as availability of healthcare providers and appropriate education and training.37 For example, despite having universal access to insulin pump therapy since 2012, New Zealand continues to report significant disparities in insulin pump use between different geographical regions.9 Enrollment in government-funded insulin pump programs may also require fulfilling certain criteria and managing and completing paperwork regularly, which could be an additional barrier disproportionately affecting individuals with a non-English primary language or lower education level. Thus, while government funding for insulin pumps may reduce disparities in access, more comprehensive approaches are likely needed to address additional and related barriers to insulin pump use, such as language, education, and access to expert health teams. Whether government funding for insulin pumps affects all individuals similarly or whether this differs based on characteristics such as age, sex, ethnicity, glycemic control or other factors remains unknown.
Our study has a number of strengths. First, this is one of the only estimates to our knowledge of the proportion of individuals with type 1 diabetes using insulin pumps in Canada. Second, our study is unique in that differing provincial policies for insulin pump funding permitted a ‘natural experiment’ within the same country. To our knowledge, there are no previous studies that have examined the effects of insulin pump funding programs on accessibility and use of insulin pumps. Third, our sample is less susceptible to selection bias than those obtained from diabetes specialist clinics which would be more likely to overestimate insulin pump use. Finally, we demonstrated the utility of the new DAC National Diabetes Repository for conducting health services research across multiple provinces in Canada. However, our study also has some limitations. First, there may have been misclassification of type 1 diabetes and insulin pump use. As noted previously, we expect this would have affected provinces with pump funding programs and provinces without pump funding programs similarly, resulting in a non-differential bias. Individuals who recently switched from MDI to insulin pump therapy or those using basal insulin in combination with an insulin pump may have been misclassified as not using insulin pump therapy, though we expect this would be uncommon. It is difficult to validate our estimated proportion of people with diabetes having type 1 diabetes and proportion of people with type 1 diabetes using insulin pumps given the limited reporting of such data in Canada. Second, the DAC National Diabetes Repository did not contain information pertaining to ethnicity, education, primary language, self-reported income, duration of diabetes, age at initiation of insulin pump therapy, or diabetes complications. It also did not include information regarding use of other diabetes technologies such as continuous glucose-monitoring devices. Third, our study population may be affected by bias due to a number of reasons including the algorithm being 73% sensitive and thus misclassifying some individuals with type 1 as having type 2 diabetes, the possibility that some individuals with type 1 diabetes do not regularly see a primary care provider (since specialists typically manage type 1 diabetes in Canada), and being limited to including individuals between the ages of 18 and 55. The sample size was particularly small for provinces without insulin pump funding programs which limits comparison between groups. Finally, as for all observational studies, we cannot conclude there is a causal relationship between pump funding programs and the observed association with insulin pump use.
Using a natural experiment to examine the effects of differing policies for insulin pump reimbursement on rates of insulin pump use, we demonstrated that insulin pump use is more common in regions with reimbursement programs. However, current government funding for insulin pumps does not appear to be sufficient to address disparities—such as higher income—between pump users and non-users. Given the benefits of insulin pump therapy and the emerging promise of closed-loop systems (which require both insulin pumps and continuous glucose-monitoring devices), comprehensive strategies for improving equitable use of insulin pumps are urgently required.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data is de-identified electronic medical record data maintained by Diabetes Action Canada in the National Diabetes Repository (https://repository.diabetesaction.ca/). Data is available only upon request to approved investigators and after review by a Research Governing Committee.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the research ethics board at Mount Sinai Hospital (MSH REB number: 19-0215-C). Participant consent for inclusion in the National Diabetes Repository is not required.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AW conceived and designed the study with input from GLB and BAP. AW analyzed the data. CS conducted the literature search and wrote the first draft of the manuscript. All authors interpreted the data, provided critical revisions, and approved the final version.
Funding Funding for this study was provided by Diabetes Action Canada and CIHR’s Ontario SPOR Support Unit.
Disclaimer The study sponsor/funder was involved in data collection only and not involved in the design of the study; analysis and interpretation of data; writing the report; and did not impose any restrictions regarding the publication of the report.
Competing interests BAP has received speaker honoraria from Medtronic, Novo Nordisk, Abbott, AstraZeneca and Sanofi; has received research grant support from Boehringer Ingelheim and the Bank of Montreal; and serves as a consultant for Boehringer Ingelheim, Abbott and Insulet. BAP is supported by the Sam and Judy Pencer Family Chair in Diabetes Research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.