Article Text

Statistics from Altmetric.com
Provocative rodent studies taken together with cross-sectional human epidemiological data have shown that there may be a cross-talk between circulating leptin levels and whole-body iron metabolism.1 2 In this study, we aim to discover the effects of recombinant leptin administration on iron parameters in patients with partial lipodystrophy.
We studied serum samples from 19 patients with partial lipodystrophy (median age: 42 years, IQR: 34–57, male/female: 3/16) gathered from an open-label study previously performed at the University of Michigan (ClinicalTrials.gov identifier: NCT01679197; article in press). All patients included in this analysis had familial partial lipodystrophy. We measured iron (assay range: 5–1000 µg/dL), soluble transferrin receptor (sTfR; assay range: 3.0–80.0 nmol/L), hepcidin (assay range: 2.5–1000 ng/mL), and high-sensitive C reactive protein (hs-CRP; assay range 0.1–80 mg/L) levels using commercially available assays. We integrated the results into an existing database of metabolic parameters. Repeated-measures analysis of variance was used to compare multiple time points. Paired t-test was used to compare month 6 values to baseline (a prespecified endpoint). Otherwise, multiplicity correction was performed. Normality was assessed by the Kolmogorov-Smirnov test and the Shapiro-Wilk’s W test and also by plotting a histogram of the variable of interest. Log transformation was used for skewed data. Data are presented as median, IQR.
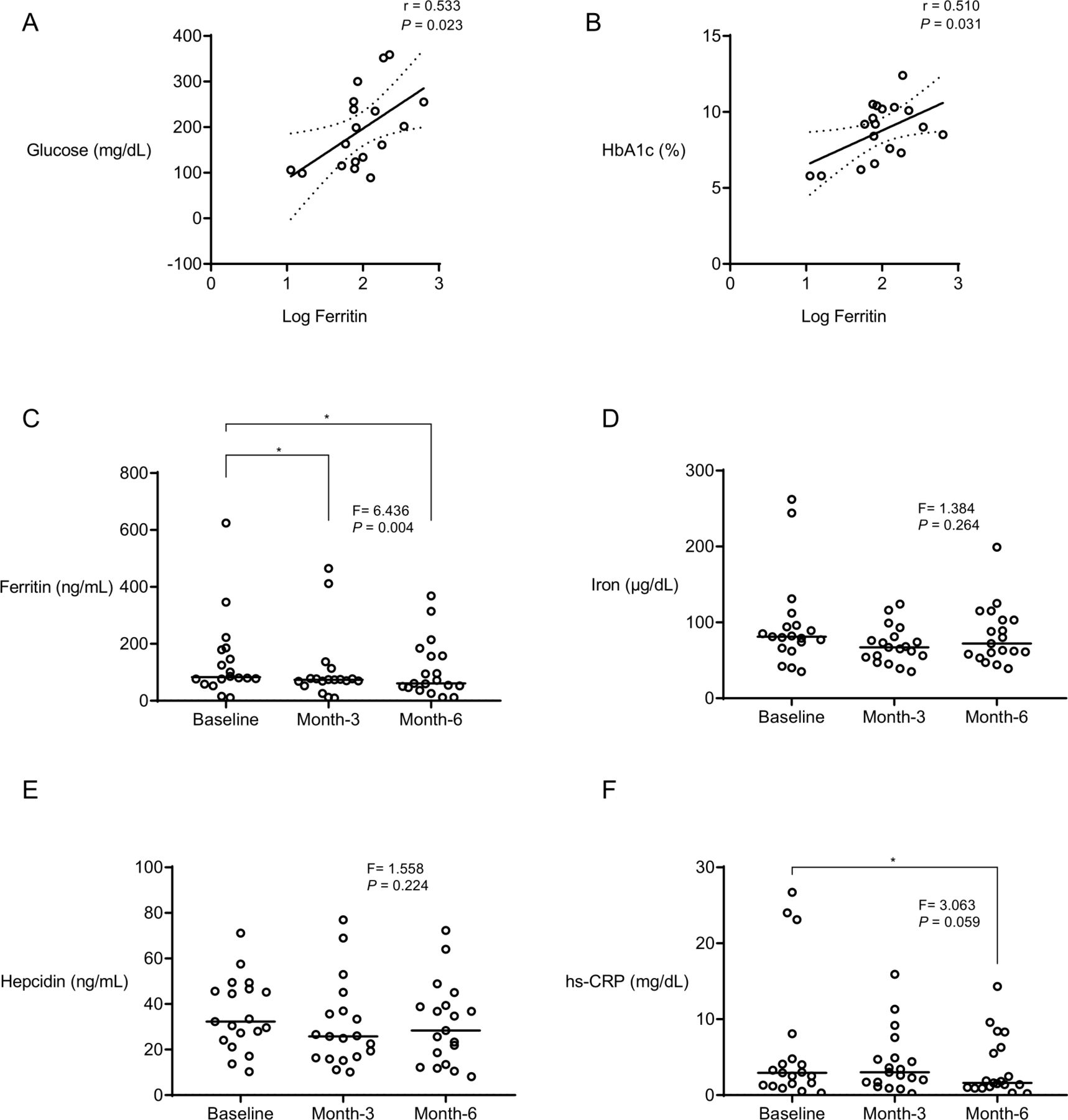
At baseline, ferritin levels were positively correlated with fasting glucose (r=0.533; p=0.023; figure 1A) and HbA1c (r=0.510; p=0.031; figure 1B). We also calculated Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) in 14 participants who underwent a mix-meal test in the parent protocol for whom fasting insulin measurements were available. In these participants, HOMA-IR was correlated with serum iron levels (r=0.592; p=0.030). After 6 months of therapy, hepatic fat content measured by MRI Dixon method decreased (12.7%, 9.8–20.6 vs 8.9%, 7.0–11.0; p=0.031). Triglyceride levels tended to decrease at 6 months (346 mg/dL, 240–1771 vs 295 mg/dL, 207–495; p=0.091). HbA1c levels did not change significantly (9.2%, 7.3–10.3 vs 8.5%, 6.8–9.5; p=0.264).
{kind=link}
Correlation of ferritin with fasting glucose (A) and HbA1c (B). The effect of exogenous leptin on ferritin (C), iron (D), hepcidin (E) and hs-CRP (F). Data are presented as median, IQR. We report the F-statistic and p value from a repeated-measures ANOVA. * indicates p<0.05 versus baseline, paired sample t-test. These p values are marked if they are significant after multiplicity correction. Paired t-test was used to compare month 6 values with baseline (without multiplicity correction) as the change at 6 months versus baseline was a prespecified endpoint. P values were calculated by using log-transformed ferritin, iron, hepcidin and hs-CRP levels. ANOVA, analysis of variance; hs-CRP, high-sensitive C reactive protein.
We observed significant reductions in serum ferritin after treatment (F=6.436, p=0.004; 83 ng/mL, 76–179 vs month 3: 74 ng/mL, 68–79; p=0.007; and month 6: 61 ng/mL, 46–158; p=0.004; figure 1C). Although slight reductions were observed in circulating levels of iron (figure 1D) and hepcidin (figure 1E), these changes did not reach statistical significance. Changes in sTfR were not statistically significant either. However, there were notable reductions in hs-CRP levels at 6 months (2.9 mg/L, 1.3–4.8 vs 1.6 mg/L, 1.0–6.3; p=0.012; figure 1F). Additionally, we observed modest correlations between changes in serum iron and triglycerides (r=0.491, p=0.033) and hepatic fat (r=0.412, p=0.079).
In the NHANES Study, higher serum ferritin levels were associated with newly diagnosed diabetes.3 Elevated levels of ferritin have been previously linked to altered fat distribution.4 Likewise, decreased iron stores as a result of phlebotomy have been associated with improved insulin sensitivity.5 In keeping with previous evidence from type 2 diabetes and metabolic syndrome, we found a significant relationship between ferritin and glycemic status in patients with partial lipodystrophy.
In an intriguing translational study, Gao et al1 reported that serum ferritin was one of the best predictors of serum leptin under physiological conditions. The study also reported that adipocyte-specific loss of the iron exporter ferroportin resulted in iron loading and decreased leptin. Although hepcidin and iron levels tended to decrease after leptin in our study population, these changes were not statistically significant in our relatively small sample size. However, leptin therapy was associated with reductions in triglycerides and hepatic fat along with significant decreases in ferritin and hs-CRP levels.
In conclusion, our data add to the growing body of evidence that iron metabolism may be more directly linked to the pathophysiology of insulin resistance than previously thought and support the notion that increasing leptin signal via exogenous administration may lower ferritin levels in a rare human metabolic disease associated with insulin resistance and diabetes. However, whether the decrease in ferritin directly indicates a decrease in iron stores or is mediated by an effect on inflammation remains not clear at this time.
Ethics statements
Ethics approval
The study was approved by the University of Michigan Institutional Review Board (IRBMED: HUM00058708). All participants gave informed consent before taking part.
Acknowledgments
We are indebted to the participants for volunteering in the original partial lipodystrophy study.
Footnotes
Contributors EYA and SB performed data analyses and created the figure. EYA wrote the first draft of the manuscript. BJR and JFH performed measurements of the iron parameters. EAO designed the study, and provided oversight in the execution of the study, data analyses, and manuscript writing. She also followed the participants clinically and performed all regulatory reporting and correspondence. All other authors (PS, BA, AHN, and RH) contributed to data collection and analysis. All authors read and approved the final version of the letter. EAO is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The partial lipodystrophy study is supported by the National Institutes of Health (NIH) grant R01 DK088114. BJR was supported by NIH grant T32-DK-007245 and F32-DK-117522.
Competing interests EAO reports the following conflicts: grant support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Ionis Pharmaceuticals, Akcea Therapeutics, Gemphire Therapeutics, GI Dynamics (current), AstraZeneca (past 2 years); consultant or advisor: AstraZeneca, Thera Therapeutics, and BMS (past), Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Regeneron Pharmaceuticals (current); drug support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Akcea Therapeutics, Rhythm Pharmaceuticals (all current); other support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Regeneron Pharmaceuticals (current). BA has attended Scientific Advisory Board Meetings organized by Aegerion Pharmaceuticals (now Amryt Pharmaceuticals) and Regeneron Pharmaceuticals and has received honoraria as a speaker from AstraZeneca, Lilly, MSD, Novartis, Novo Nordisk, Boehringer-Ingelheim, Servier, and Sanofi-Aventis. Other authors report no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.