Article Text

Abstract
Introduction Patients with type 2 diabetes (T2D) have an increased risk of worsening kidney function (WKF) over time compared with patients without diabetes. Data evaluating the inter-relation between WKF, cardiovascular risk, and clinical events are scarce. We aim to study the association of WKF with subsequent cardiovascular events and the probabilities of transition from WKF to hospitalization or death according to patients’ risk. We have used a large population of patients with T2D and a high cardiovascular risk enrolled in the Action to Control Cardiovascular Risk in Diabetes Study.
Research design and methods Time-updated, joint, and multistate modeling were used. WKF was defined as an estimated glomerular filtration rate (eGFR) decline greater than 40% from baseline. A total of 10 251 patients were included, of whom 1213 (11.8%) presented WKF over a median (percentile25–75) follow-up time of 5.0 (4.1–5.7) years.
Results Patients who experienced WKF were slightly older, more frequently women, and had longer diabetes duration. Patients experiencing WKF, regardless of baseline kidney function, had a higher risk of subsequent cardiovascular events, including the composite of cardiovascular death or hospitalization for heart failure (HHF), with ≈2-fold higher risk. Joint modeling showed that renal function deterioration frequently occurs even among patients who did not experience a cardiovascular event. In multistate models, patients with a medium-high cardiovascular risk (compared with those with a low cardiovascular risk) are at higher risk of HHF or cardiovascular death first (HR=4.76, 95% CI 3.63 to 6.23) than of WKF first (HR=1.37, 95% CI 1.21 to 1.56); remarkably, the risk of cardiovascular death or HHF is highest after a WKF event (HR=6.20, 95% CI 2.71 to 14.8).
Conclusions In patients with T2D and a high cardiovascular risk, WKF occurs in more than 10% of patients and is independently associated with risk of subsequent cardiovascular events, irrespective of baseline eGFR. Preventing serious WKF and the transition from WKF to HHF or cardiovascular death is an important objective of future trials.
Trial registration number NCT00000620.
- diabetes complications
- kidney diseases
- cardiovascular system
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Patients with type 2 diabetes (T2D) have an increased risk of worsening kidney function (WKF) over time compared with patients without diabetes.
Data evaluating the inter-relation between WKF, cardiovascular risk, and clinical events are scarce.
What are the new findings?
WKF was independently associated with subsequent cardiovascular events regardless of baseline kidney function, and the risk of cardiovascular death or heart failure hospitalization was sixfold higher after a WKF event.
How might these results change the focus of research or clinical practice?
These results suggest that prevention of WKF should be a treatment target for patients with T2D.
Introduction
Patients with type 2 diabetes (T2D) have an increased risk of kidney function deterioration over time compared with patients without diabetes.1 Until recently, the only treatments capable of delaying the deterioration of kidney function were ACE inhibitors (ACEi) and angiotensin receptor blockers (ARBs). By improving both cardiovascular (heart failure hospitalizations in particular) and kidney outcomes, the advent of sodium glucose cotransporter 1/2 inhibitors (SGLT1/2i) and the mineralocorticoid receptor antagonist finerenone has changed the therapeutic landscape of patients with T2D, particularly those with a high risk of cardiovascular events and chronic kidney disease (CKD).2–6
Although clinically important, until recently worsening kidney function (WKF) events were not considered in the primary outcome of large outcome trials of patients with T2D, which usually considered acute kidney injury as a safety endpoint.7 Beyond the methodological issues that may arise from merging events of different clinical relevance in the same time-to-first event analysis (eg, WKF and death), it is uncertain how WKF relates to subsequent cardiovascular events, particularly hospitalization for heart failure (HHF) and cardiovascular death (which seem closely related to WKF), and which WKF thresholds should be considered as an endpoint in patients with T2D.8 9 Recent trials have used a deterioration in the estimated glomerular filtration rate (eGFR) superior to 40%–50% as endpoint, although further study is required to ascertain the clinical importance of such thresholds.10 11
Using a large population of patients with T2D and a high cardiovascular risk enrolled in the Action to Control Cardiovascular Risk in Diabetes Study (ACCORD), we aim to study the association of WKF with subsequent HHF and cardiovascular death and the probabilities of transition from WKF to HHF or cardiovascular death according to baseline patient risk.
Methods
ACCORD glycemia intervention study design
The rationale and design of the ACCORD trial and a description of the glycemia intervention have been previously described.12 13 ACCORD was a multicenter clinical study, sponsored by the National Heart, Lung, and Blood Institute, and conducted in 77 clinical centers in the USA and Canada. ACCORD enrolled patients with T2D and a glycated hemoglobin level of 7.5% or greater and who had evidence of cardiovascular disease or significant atherosclerosis, albuminuria, left ventricular hypertrophy, or at least two additional risk factors for cardiovascular disease (dyslipidemia, hypertension, current status as a smoker, or obesity).
A total of 10 251 patients were randomly assigned to receive either intensive antihyperglycemic therapy targeting a glycated hemoglobin level of less than 6.0% or to receive standard therapy targeting a glycated hemoglobin level of 7.0%–7.9%. All patients provided written informed consent to participate in the study. Patients in the intensive therapy group attended monthly visits for the first 4 months and then every 2 months thereafter. Additional visits could be scheduled as needed to achieve glycemic goals. Patients in the standard therapy group had glycemic management visits every 4 months.
Outcomes were adjudicated by a central committee whose members were unaware of study group assignments on the basis of predefined criteria. In the present study we used the composite outcome of time-to-first of cardiovascular death or HHF and cardiovascular death alone as the main outcomes of interest.
WKF definition
WKF was created by assessing the % of change in eGFR at each study visit relative to the baseline visit. Increases or no changes in eGFR were set as ‘reference’ and eGFR decreases were assessed as a continuous (log and spline transformed variable) and categorical eGFR drop of >30%, >40%, and >50% relative to baseline. Missing eGFR values were carried forward from the last available visit. In ACCORD, eGFR was determined by the Modification of Diet in Renal Disease (MDRD) formula.14
Our main analysis focuses on the first occurrence of WKF because we aim to study the relationship between the occurrence of WKF and subsequent death from cardiovascular causes and HHF; if we considered to separate time-points for confirmation of ‘sustained’ WKF (eg, 3 months apart), then cardiovascular death could occur before the second eGFR measurement and would not be captured. Moreover, by design, in ACCORD, intensive and standard therapy groups had different visit schedules, whereby patients in the intensive group had more visits and eGFR measurements, with more ‘opportunities’ to capture ‘sustained’ WKF. Notwithstanding, as exploratory analysis, we have also studied the association between a sustained WKF defined by a ‘sustained’ eGFR drop in at least two consecutive visits separated by a minimum of 3 months.
Statistical analysis
Patients’ characteristics between patients experiencing WKF and not were compared with means and proportions for continuous and categorical variables, respectively. To identify the variables with stronger association with cardiovascular outcomes (cardiovascular death or HHF and cardiovascular death alone), we have built a model incorporating variables known to have strong prognostic value and to be readily available in routine clinical practice. We started by including age, sex, history of cardiovascular disease, race, diabetes duration, dyslipidemia, hypertension, smoking, waist circumference, systolic blood pressure, glycated hemoglobin, eGFR, urinary albumin to creatinine ratio (UACR), and the randomized treatment (intensive vs standard glucose-lowering treatment) in the model, and then applied a stepwise (‘forward’) selection with a p value <0.05 to enter and stay in the model with the randomized treatment ‘forced’ into the model. The final model included age (≤65 years vs >65 years), sex (female vs male), history of cardiovascular disease including HHF (yes vs no), UACR (≤30 mg/g vs >30 mg/g), waist circumference (≤88 cm for women and ≤102 cm for men vs >88 cm for women and >102 cm for men), and glycated hemoglobin (≤8% vs >8%). We then assigned integer points based on the β-coefficients of the associations to build a simple and easy-to-implement clinical risk score that allowed classification of patients by level of risk (low, medium, and high). These variables included in the risk model were used for adjustment in all the multivariate analyses and to compare patients with medium/high risk versus low risk in multistate models. We generated eGFR % drop from baseline by comparing the % of eGFR decrease relative to the baseline eGFR as described above. We used time-updated Cox models to study the crude and adjusted associations between WKF (continuous ‘spline transformed’ and categorical) and subsequent cardiovascular outcomes. Time-updated models consider the last observed WKF episode (before event or censor). Additionally, joint modeling was used to study the evolution of eGFR changes throughout the follow-up in patients with and without an event with log-transformed continuous eGFR to fit the models’ assumptions. We examined potential unmeasured confounding by calculating E-values.15 Multistate ‘Markov’ models were used to compute the transition probabilities by baseline patient risk. Here, the occurrence of WKF was considered a ‘transition state’ from where the patient can either have no event or experience a subsequent HHF or cardiovascular death, that is, ‘absorbing state’. We have used a Weibull parametric approach to fit our models, which was the functional form with the lowest akaike information criterion (AIC)/Bayesian information criterion (BIC).16 Stata V.16 was used for the analyses, which included the ‘Merlin’ package.17
Results
Baseline characteristics by occurrence of WKF
A total of 10 251 patients were enrolled in the trial, of whom 1213 (11.8%) presented WKF (ie, >40% eGFR drop) over a median (percentile25–75) follow-up time of 5.0 (4.1–5.7) years. Patients who experienced WKF were slightly older (63.1 years vs 62.7 years), more frequently women (43% vs 38%), with longer diabetes duration, higher level of glycated hemoglobin, more frequent history of hypertension, and abdominal obesity/elevated waist circumference (p<0.05 for all). Patients experiencing WKF presented higher baseline eGFR (104 vs 89 mL/min/1.73 m2) and were more frequently treated with loop diuretics (14% vs 9%), ACEi/ARB (72% vs 69%), calcium channel blockers (22% vs 19%), biguanides (67% vs 64%), sulfonylureas (57% vs 53%), and insulin (38% vs 35%) (table 1). The differences in patients’ characteristics by >30% and >50% eGFR drop were similar to the described above.
Patients’ characteristics by worsening kidney function
Baseline patient risk and risk score
Risk factors independently associated with the occurrence of cardiovascular death or HHF (model C-index=0.73) and cardiovascular death alone (model C-index=0.72) were a history of cardiovascular disease (including heart failure) (β=1.05), an UACR >30 mg/g (β=0.86), older than 65 years (β=0.50), an eGFR <90 mL/min/1.73 m2 (β=0.32), a glycated hemoglobin >8% (β=0.31), an elevated waist circumference (β=0.29), and men (β=0.17). Based on this risk model, we built a simple integer risk score ranging from 0 to 11 points to classify patients in risk categories (ie, tertiles of risk): 0–3 points=low risk (n=3453); 4–6 points=medium risk (n=4217); and 7–11 points=high risk (n=2581) (online supplemental table 1).
Supplemental material
Time-updated models for risk of cardiovascular events after WKF and plausibility of causation
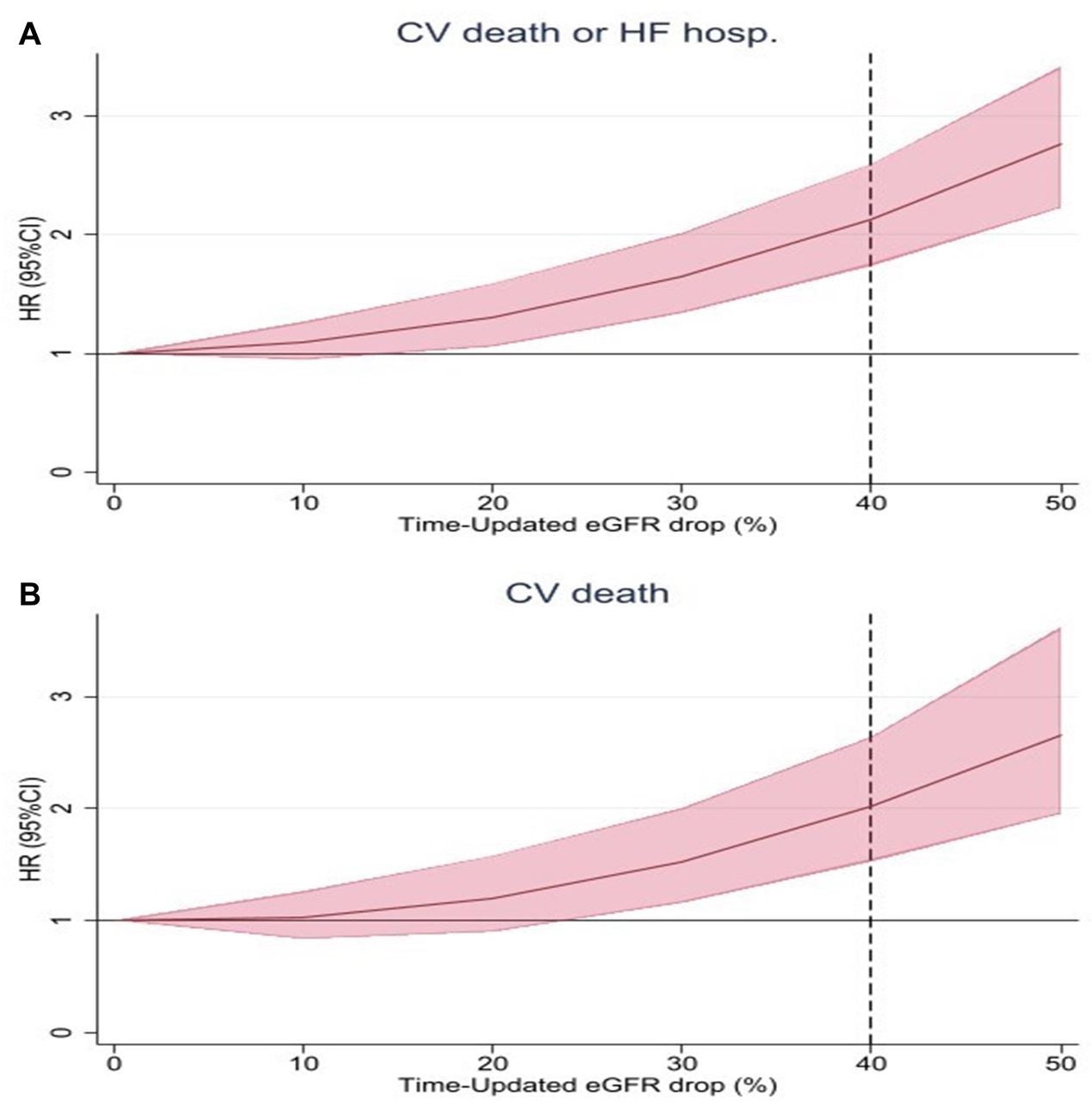
Patients experiencing WKF had a higher risk of subsequent cardiovascular events, including the composite of cardiovascular death or HHF and cardiovascular death, with ≈2.5-fold higher risk with an eGFR drop >40% from baseline (figure 1). The (adjusted) HR (95% CI) representing the association of WKF with a subsequent event of cardiovascular death or HHF was 1.97 (1.66 to 2.34) for >30% eGFR drop, 2.51 (2.06 to 3.07) for >40% eGFR drop, and 3.03 (2.33 to 3.92) for >50% eGFR drop. The (adjusted) HR (95% CI) representing the association of WKF with a subsequent cardiovascular death event was 1.89 (1.47 to 2.45) for >30% eGFR drop, 2.41 (1.77 to 3.29) for >40% eGFR drop, and 3.29 (2.19 to 4.92) for >50% eGFR drop. No interaction of WKF by baseline eGFR was observed in these models (interaction p>0.1 for all). The (adjusted) HR (95% CI) representing the association of HHF with subsequent cardiovascular death was 5.17 (3.91 to 6.83) (figure 2, table 2 and online supplemental figure 1).

Association of continuous (spline) eGFR drop from baseline and CV events: (A) CV death or hospitalization for heart failure and (B) CV death. Model adjusted for age (≤65 years vs >65 years), sex (female vs male), history of CV disease including hospitalization for heart failure (yes vs no), urinary albumin to creatinine ratio (≤30 mg/g vs >30 mg/g), waist circumference (≤88 cm for women and ≤102 cm for men vs >88 cm for women and >102 cm for men), glycated hemoglobin (≤8% vs >8%), and randomized treatment (intensive vs standard glucose-lowering treatment). CV, cardiovascular; eGFR, estimated glomerular filtration rate; HF, heart failure.

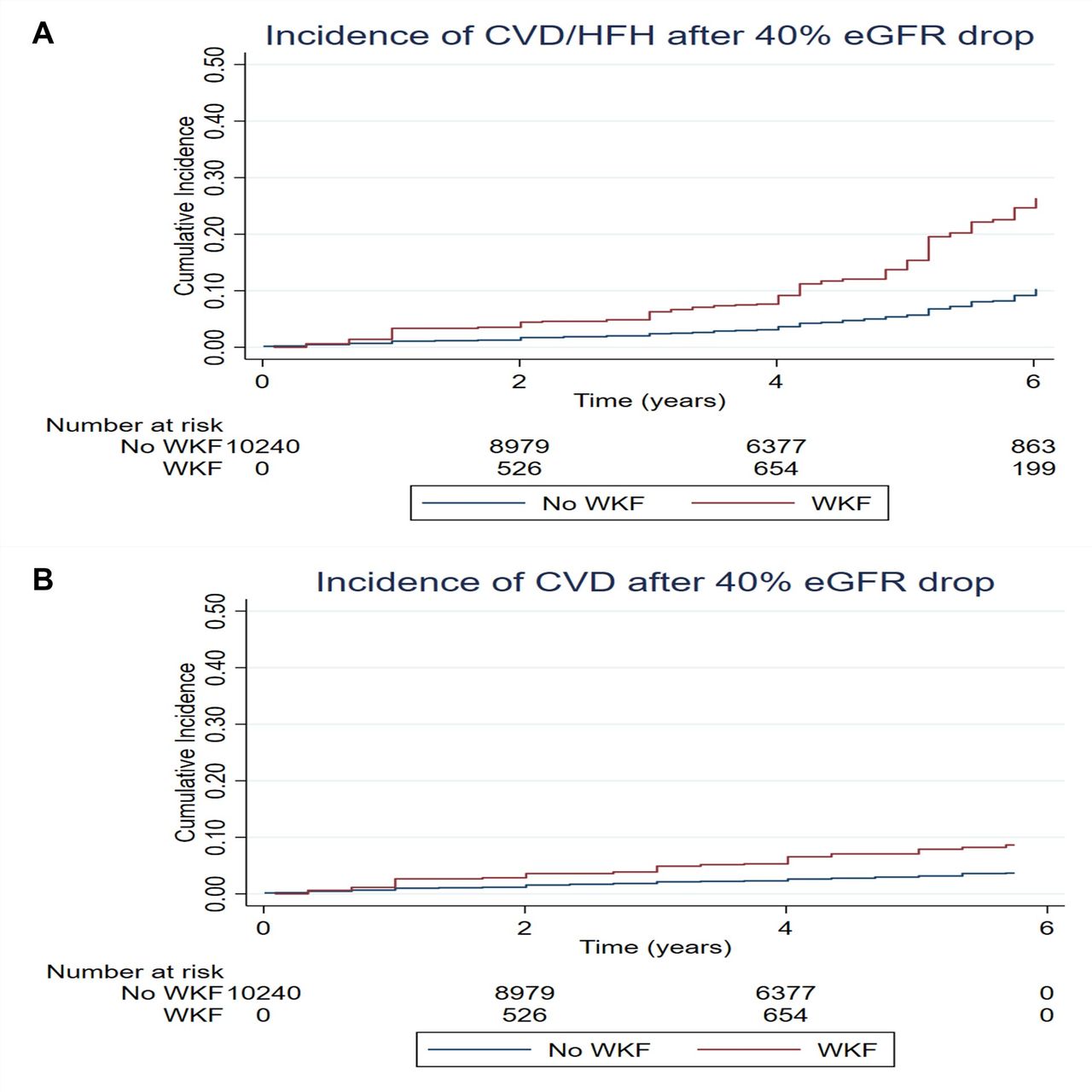
Time-updated WKF and subsequent cardiovascular events: (A) CVD or hospitalization for heart failure and (B) CVD. Adjusted HR (95% CI) for the composite of CVD or heart failure hospitalization after >40% eGFR drop=2.51 (2.06 to 3.07) (p<0.001). Adjusted HR (95% CI) for CVD after >40% eGFR drop=2.41 (1.77 to 3.29) (p<0.001) (see also table 2). Model adjusted for age (≤65 years vs >65 years), sex (female vs male), history of CVD including hospitalization for heart failure (yes vs no), urinary albumin to creatinine ratio (≤30 mg/g vs >30 mg/g), waist circumference (≤88 cm for women and ≤102 cm for men vs >88 cm for women and >102 cm for men), glycated hemoglobin (≤8% vs >8%), and randomized treatment (intensive vs standard glucose-lowering treatment). No interaction of WKF by baseline eGFR was observed: interaction p=0.42 for CVD/HFH; interaction p=0.47 for CVD. CVD, cardiovascular death; eGFR, estimated glomerular filtration rate; HFH, heart failure hospitalization; WKF, worsening kidney function.
Time-updated models for risk of cardiovascular events after worsening kidney function and hospitalization for heart failure
Despite more frequent, the associations of >30% eGFR drop with subsequent cardiovascular death were weaker, with an E-value of 2.48, which is very close to the HR observed for UACR (HR=2.36) and history of cardiovascular disease (HR=2.85), meaning that other covariate(s) with similar association with outcome could offset the association of an eGFR >30% back to null (ie, HR≈1). The E-values for eGFR >40% and >50% were greater than 3 (far from the strongest associations seen in the study), suggesting that it would be unlikely for a covariate to offset these associations back to the null (online supplemental figure 2).
The joint model approach shows that most patients with T2D (even those without a cardiovascular event) experienced a deterioration of their kidney function over time. Notwithstanding, eGFR deterioration was strongly associated with subsequent cardiovascular death or HHF: coefficient for log-transformed eGFR over time=0.46 (95% CI 0.39 to 0.52) (p<0.001) (online supplemental figure 3).
The association between a ‘sustained’ WKF >30%, 40%, and 50% from baseline is presented in online supplemental table 2, showing similar associations to those described for the first WKF occurrence, confirming the 40% threshold as the optimal ‘balance’ between events captured and the strength of the association with cardiovascular mortality: adjusted HR for sustained 30% WKF=1.46 (95% CI 0.94 to 2.25) (p=0.085), sustained 40% WKF=1.96 (95% CI 1.18 to 3.24) (p=0.009), and sustained 50% WKF=2.67 (95% CI 1.42 to 5.02) (p=0.002).
Multistate models representing the transition from baseline to WKF (‘transition state’) and to cardiovascular death or heart failure hospitalization (‘absorbing state’) according to patients’ risk
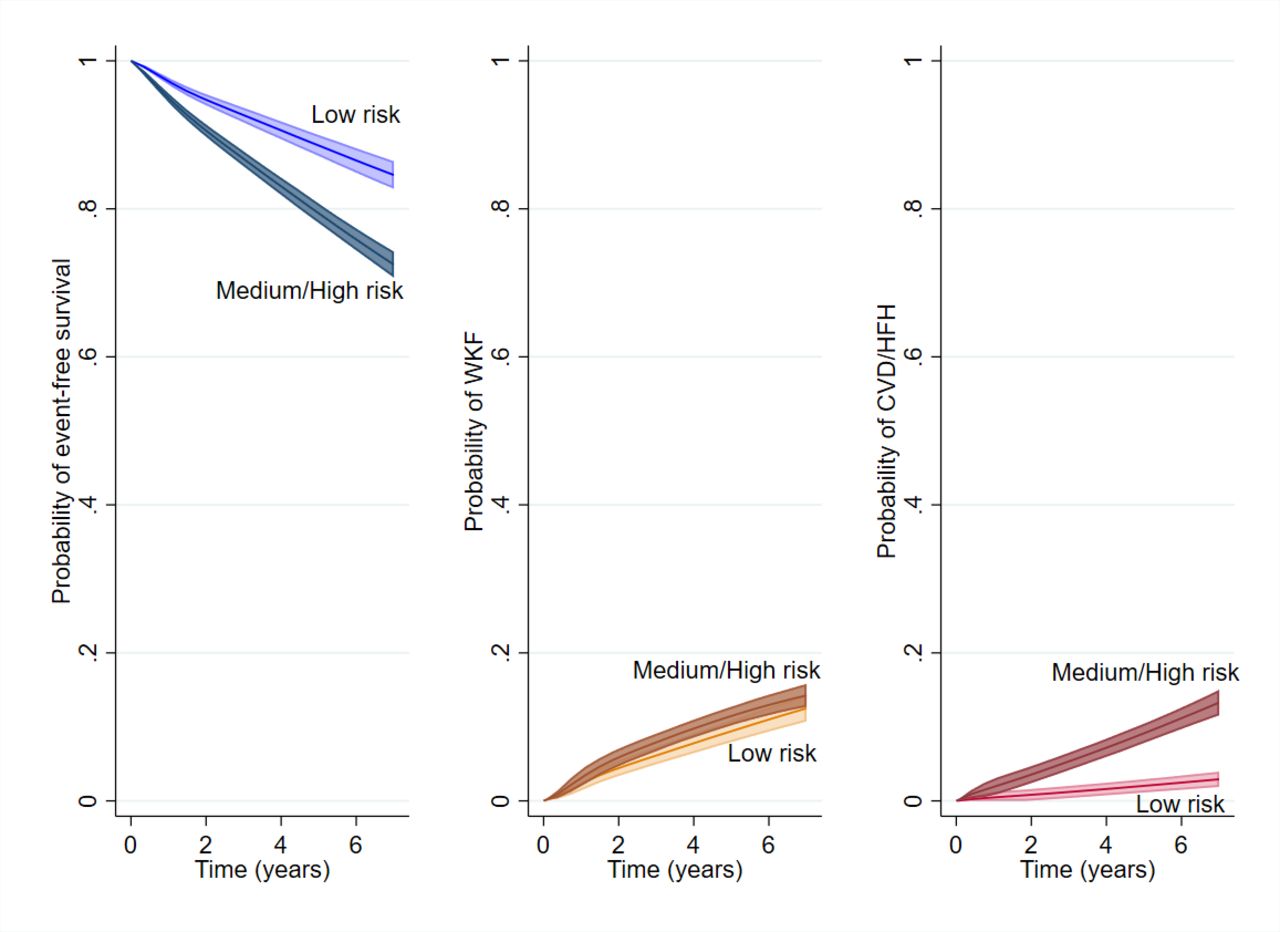
Compared with patients with low baseline risk, those with medium/high baseline risk (see online supplemental table 1) had a higher probability of experiencing WKF (ie, >40% eGFR drop), cardiovascular death or heart failure hospitalization, and cardiovascular death or heart failure hospitalization after WKF. In medium-risk/high-risk patients, the risk of transitioning directly to WKF was relatively mild (HR=1.37, 95% CI 1.21 to 1.56), whereas the risk of transitioning directly to a cardiovascular death or heart failure hospitalization event was high (HR=4.76, 95% CI 3.63 to 6.23); still, the risk of cardiovascular death or heart failure hospitalization after WKF was even higher (HR=6.20, 95% CI 2.71 to 14.8) (table 3). This can be visualized in figure 3, where low-risk patients had higher probability of survival, slightly lower probability of WKF, and much lower probability of cardiovascular death or heart failure hospitalization.
Multistate model transition matrix according to patients’ risk
{kind=link}
{kind=link}
{kind=link}
Multistate models representing the probability of event-free survival, WKF, and CVD or hospitalization for heart failure by patients’ baseline risk. Probabilities are displayed as a comparison of a medium-risk/high-risk patient with a low-risk patient. A low-risk patient is a patient with up to 3 risk points. A patient with more than 3 risk points is a medium-risk/high-risk patient (see also online supplemental table 1). CVD, cardiovascular death; HFH, heart failure hospitalization; WKF, worsening kidney function.
Discussion
Several points with important clinical and trial design implications should be highlighted from the present study. (1) The occurrence of WKF is relatively frequent in patients with T2D and a high cardiovascular risk. (2) Patients experiencing WKF were older, had more comorbid conditions, and longer diabetes duration; however, they had higher baseline eGFR, suggesting that patients starting with higher eGFR levels might be more susceptible to drop. Notwithstanding, the associations of WKF with subsequent cardiovascular events were not modified by baseline eGFR, supporting the use of clinically meaningful WKF definitions irrespective of baseline eGFR. (3) A WKF defined by >30% eGFR drop was frequent (>15% of observations), but the associations with cardiovascular events were prone to confounding; the associations of eGFR drop >40% and 50% were less prone to confounding, but an eGFR drop >50% was relatively rare (<3%), which supports the use of an eGFR drop >40% as the ‘sweet spot’ for use as kidney outcome in cardio-kidney trials and as threshold for clinical awareness in patients with T2D. (4) The strong and independent association of >40% eGFR drop with subsequent cardiovascular events (HHF or cardiovascular death) supports the integration of this WKF outcome as a clinically meaningful endpoint that can be integrated in the primary outcome of cardio-kidney composite outcomes in T2D trials. (5) The risk of cardiovascular death or heart failure hospitalization can be accurately predicted from patients’ risk and increases by more than sixfold after a patient develops WKF. (6) The deterioration in renal function over time observed in patients with T2D supports the use of means that capture more subtle eGFR changes (eg, eGFR ‘slope’ analysis). Together, these findings highlight the need to target WKF as an outcome of primary clinical importance for patients with T2D.
A composite outcome should capture clinically meaningful events that are sensible to the treatment being studied.10 Incorporating WKF in a composite outcome could be considered only when a certain threshold is achieved because random and hemodynamic variations in renal function without clinical implication often occur in patients with frequent therapeutic alterations, such as in patients with T2D. In this regard, we have found that an eGFR drop >40% from baseline fulfills the criteria for clinical meaningfulness as it is strongly and independently associated with subsequent cardiovascular events (including cardiovascular death) while occurring in a relatively frequent proportion of patients over time. Identification of baseline cardiovascular risk can be accomplished using simplified tools that use routinely available clinical variables. In patients with medium/high cardiovascular risk, the probability of transition from a WKF ‘state’ toward a heart failure hospitalization or cardiovascular death ‘state’ was much higher (6.2-fold) than a direct transition from baseline toward a heart failure hospitalization or cardiovascular death (4.8-fold), supporting the clinical relevance of avoiding WKF. However, one might argue that despite the strong association with outcomes, WKF has relatively lower clinical importance than a hospitalization or fatal event. A WKF >40% eGFR drop was associated with a 2.4-fold increase in risk of subsequent cardiovascular death, whereas a heart failure hospitalization was associated with a 5.2-fold higher risk of subsequent cardiovascular death. A potential way to overcome the limitations of a time-to-first composite analysis is to perform a hierarchical analysis using the ‘win ratio’, where cardiovascular death would be the most important (and final) event, followed by heart failure hospitalization and then WKF.8 18 Another important aspect to consider is the evolution of renal function over time that can be much more subtle and harder to detect than a rapid eGFR drop. Our study also shows that patients with T2D have a tendency to see their renal function deteriorate continuously with time, even in patients who did not experience a heart failure or cardiovascular death event during the follow-up, which does not mean that they could not experience such event(s) or progress toward CKD if the trial had continued for a longer period. For this reason, on top of WKF, it is also important to assess the impact of treatments on the continuous deterioration of renal function over time (eg, using eGFR ‘slope’ analysis).19
Diabetes mellitus is the main cause of CKD worldwide, affecting up to 40% of people with T2D.20 The development of CKD increases the risk of heart failure and death by several-fold compared with patients with T2D but without CKD.21 As newer treatments, such as SGLT1/2i and finerenone, showed to improve both cardiac and kidney outcomes in patients with T2D, it is expected that in the future more trials expand their primary outcomes to include WKF, as this would increase the study power while preserving the clinical meaning of the findings. This work provides a robust framework advocating for such WKF outcome inclusion.
Limitations
Some important limitations should be acknowledged in our study. This is a post-hoc analysis of an open-label, randomized controlled trial with a factorial design, whereby from the 10 251 patients included in the present analysis 4733 were included in the blood pressure arm by being randomly assigned to receive either intensive or standard (less intensive) antihypertensive therapy. In addition, 5518 patients were included in the lipid-lowering arm by being randomly assigned to receive either fenofibrate or placebo while maintaining low-density lipoprotein cholesterol control with simvastatin. Given this trial design, our findings may not apply to other populations of T2D with more stable and updated treatment regimens. WKF was not a prespecified endpoint in the ACCORD trial. Furthermore, patients in the intensive therapy arm had more frequent study visits, which might have led to more opportunities to capture WKF episodes. Despite using several statistical techniques with consistent findings, causality cannot be established from these results.
Conclusion
In patients with T2D and a high cardiovascular risk, a drop in eGFR superior to 40% from baseline occurs in more than 10% of patients and is independently associated with a substantial increase in risk of subsequent cardiovascular events, irrespective of baseline eGFR. Preventing serious WKF and the transition from WKF to HHF or cardiovascular death is an important objective of future trials.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Ethics approval
The study protocol was approved by the institutional review board or ethics committee at each center, as well as by a review panel at the National Heart, Lung, and Blood Institute (NHLBI). Access to the ACCORD database was provided by the NHLBI/BioLINCC with ethical approval from the Faculty of Medicine of the University of Porto (process number #500/2020).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JPF performed the statistical analysis and drafted manuscript and its revisions; all other authors provided critical input. JPF is the guarantor of this work and as such had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JPF is a consultant for Boehringer Ingelheim and receives research support from AstraZeneca and Novartis. PR reports personal fees from Ablative Solutions, AstraZeneca, Bayer, Boehringer Ingelheim, Corvidia, CVRx, Fresenius, G3P (stocks), Grunenthal, Idorsia, KBP, Novartis, NovoNordisk, Relypsa, Sanofi, Sequana Medical, Servier, Stealth Peptides, Vifor, and Vifor Fresenius Medical Care Renal Pharma; and cofounder: CardioRenal, a company developing sensors for home monitoring of potassium and creatinine. FZ reports personal fees from Boehringer Ingelheim, during the conduct of the study; personal fees from Janssen, Novartis, Boston Scientific, Amgen, CVRx, AstraZeneca, Vifor Fresenius, Cardior, Cereno Pharmaceutical, Applied Therapeutics, Merck, Bayer, and CellProthera, outside the submitted work; and other support from CVCT and CardioRenal, outside the submitted work. AS reports receiving support from the Fonds de Recherche Santé Quebec (FRSQ) Junior 1 Clinician Scholars Program, Canada Institute for Health Research (CIHR grant #175095), European Society of Cardiology Young Investigator Grant, Roche Diagnostics, Boehringer Ingelheim, Novartis, AstraZeneca, and Takeda. All other authors have no potential conflicts of interest to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.