Article Text

Abstract
Introduction Experimentally, gamma-aminobutyric acid (GABA) has been found to exert immune-modulatory effects and induce beta-cell regeneration, which make it a highly interesting substance candidate for the treatment of type 1 diabetes (T1D). In many countries, including those in the European Union, GABA is considered a pharmaceutical drug. We have therefore conducted a safety and dose escalation trial with the first controlled-release formulation of GABA, Remygen (Diamyd Medical).
Research design and methods Six adult male subjects with long-standing T1D (age 24.8±1.5 years, disease duration 14.7±2.2 years) were enrolled in an 11-day dose escalation trial with a controlled-release formulation of GABA, Remygen. Pharmacokinetics, glucose control and hormonal counter-regulatory response during hypoglycemic clamps were evaluated at every dose increase (200 mg, 600 mg and 1200 mg).
Results During the trial there were no serious and only a few, transient, adverse events reported. Without treatment, the counter-regulatory hormone response to hypoglycemia was severely blunted. Intake of 600 mg GABA more than doubled the glucagon, epinephrine, growth hormone and cortisol responses to hypoglycemia.
Conclusions We find that the GABA treatment was well tolerated and established a counter-regulatory response to hypoglycemia in long-standing T1D. Further studies regarding not only the clinical potential of Remygen for beta-cell regeneration but also its potential use as hypoglycemic prophylaxis are warranted.
Trail registration number NCT03635437 and EudraCT2018-001115-73.
- diabetes mellitus
- type 1
- hypoglycemia
- receptors
- GABA-A
Data availability statement
Data are available upon reasonable request. The data sets generated during the current study can be made available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Gamma-aminobutyric acid (GABA) has, in experimental studies, been found to exert immune-modulatory effects and induce beta-cell regeneration, which make it a highly interesting substance candidate for the treatment of type 1 diabetes (T1D).
Activation of the GABA-A receptor by benzodiazepines has been found to blunt the counter-regulatory response to hypoglycemia.
In many countries, including those in the European Union, GABA is considered a pharmaceutical drug.
What are the new findings?
GABA treatment is well tolerated in subjects with T1D.
GABA can paradoxically establish a counter-regulatory response to hypoglycemia in long-standing T1D.
How might these results change the focus of research or clinical practice?
GABA has a potential use as hypoglycemic prophylaxis in clinical practice in addition to its potential beta-cell regenerative effects.
Introduction
Gamma-aminobutyric acid (GABA) is a mediator in the central nervous system (CNS) and in peripheral tissues with effects exerted through ionotropic GABA-A and GABA-C, as well as metabotropic GABA-B receptors.1 GABA is synthesized from glutamate by glutamic acid decarboxylase, a well-known autoantigen in type 1 diabetes (T1D).2 In the adult brain, GABA is the main inhibitory neurotransmitter, while its peripheral effects vary depending on the tissue. Outside the CNS, GABA is found at the highest concentrations in beta-cells and immune cells.3 4 Most immune cells express GABA receptor subunits and the metabolic machinery required for GABA metabolism. GABA exerts a predominantly inhibitory effect on immune cells by inhibiting the production of inflammatory cytokines.5 6 GABA receptor activation also enhances regulatory T cells, contributing to its immunosuppressive functions.7 In addition to beta-cells, GABA-A receptors are also expressed in a number of peripheral tissues, including the pituitary, chromaffin cells in the adrenal medulla and hepatocytes.8–10 In experimental studies with rodent and human beta-cells, GABA has been shown to reverse diabetes by stimulating beta-cell regeneration, both through beta-cell proliferation and, although more controversial, transdifferentiation.11–13 The combined immune-modulatory and beta-cell effects make GABA a highly interesting candidate for the treatment of T1D. However, in many countries, including those in the European Union, GABA is considered a pharmaceutical drug. In this initial safety and dose escalation study, we have evaluated short-term GABA treatment in subjects with T1D as a first step toward testing the potential of GABA as a beta-cell regenerative treatment.
Methods
Ethics and study design
GABA is considered a pharmaceutical drug within the European Union. All participants were provided oral and written information and signed a written consent prior to inclusion in the study.
The study was an open-label, investigator-driven phase I clinical trial, primarily assessing the safety of a controlled-release formulation of GABA, Remygen (Diamyd Medical, Stockholm, Sweden), in adult male subjects with long-standing T1D. GABA was dosed in three steps: low (200 mg), medium (600 mg) and high (1200 mg) dose, with subsequent pharmacokinetic evaluation. Remygen was administered orally as a single daily dose to be taken under fasting conditions in the morning and each dose was administered for three consecutive days. The study period consisted of visits at the hospital for 11 consecutive days. Sample size was decided after dialogue with the Swedish Medical Products Agency. The study included two mixed meal tolerance tests (MMTT), four hypoglycemic clamps and three pharmacokinetic evaluations. All study visits were conducted at Uppsala University Hospital. A detailed study design and all inclusion/exclusion criteria can be found at ClinicalTrials.gov.
Safety monitoring
All subjects underwent general and neurological examinations, as well as blood sampling for laboratory testing, at multiple time points during the safety trial. The study was monitored by Uppsala Clinical Research Center. An external Data Safety Monitoring Board reviewed the data.
Laboratory testing
Laboratory tests included metabolic parameters (glucose, hemoglobin A1c (HbA1c) and C peptide), hematology status, renal function and markers of liver injury (aspartate transaminase (AST), alanine aminotransferase (ALT), alkaline phosphate, bilirubin). During the hypoglycemic clamp, the counter-regulatory hormones glucagon, growth hormone (GH), cortisol, epinephrine and norepinephrine were analyzed. Routine blood samples were analyzed at the central laboratory of Uppsala University Hospital. Epinephrine and norepinephrine concentrations were analyzed at Karolinska University Hospital laboratory. C peptide concentrations were also analyzed with an ultrasensitive C peptide ELISA (Mercodia, Uppsala, Sweden). Glycemic control was monitored by flash glucose monitoring (FGM) (FreeStyle Libre, Abbott Laboratories, Chicago, Illinois, USA).
Pharmacokinetics of GABA
GABA concentrations in plasma were determined the first day of every dose increase at 0, 30, 60, 120, 180, 300 min and 24 hours (nadir value) after GABA administration. GABA levels were analyzed by mass spectrometry at the Mass Spectrometry Based Metabolomics Facility at Uppsala University with a method approved by the US Food and Drug Administration.
Mixed meal tolerance test
An MMTT was performed after overnight fasting at baseline and at day 11, that is, last day of treatment with 1200 mg GABA. C peptide and glucose levels were measured at 0, 15, 30, 60, 90 and 120 min after ingestion of 6 mL/kg (maximum 360 mL) Resource Protein (Nestlé Health Science, Switzerland).
Hypoglycemic clamp
A hypoglycemic clamp was performed after overnight fasting at baseline and at each GABA dosage step. An individualized insulin infusion dose was calculated based on body weight (2 mIE/kg/min) and a separate glucose infusion was titrated to achieve and maintain euglycemia (5.5 mmol/L) for 30 min, followed by hypoglycemia (2.5 mmol/L) for 30 min. Blood samples were collected at the end of each plateau. GABA was administrated 30 min before start.
Endpoints
The primary outcomes of the trial were (1) number of serious and adverse events (SAE/AE) and (2) changes in laboratory parameters, physical examinations and vital signs. The secondary outcomes were (1) C peptide response during MMTT determined as area under the curve (AUC), mean and peak values; and (2) hormonal counter-regulatory response. Additional variables such as fasting plasma C peptide, HbA1c, autoantibodies and number of self-reported hypoglycemic events were included in the general assessment.
Statistical analysis
Safety laboratory tests were compared with baseline with repeated measurements one-way analysis of variance (ANOVA) with Dunnett’s post-hoc test. For FGM data a non-parametric one-way ANOVA with Dunn’s multiple comparisons test was applied. Hormonal counter-regulatory response under normoglycemic and hypoglycemic conditions was computed by multiple t-tests and corrected for multiple testing with the Holm-Sidak method. Data are presented as mean±SEM. P values <0.05 were considered statistically significant.
Results
Characteristics of the subjects
Ten male subjects with T1D were screened, of whom four were excluded from participation in the study (C peptide >0.12 nmol/L (n=2), elevated AST/ALT (n=1) and difficult venous access (n=1)). Six subjects were included and all completed the 11-day trial. All subjects had long-standing T1D (age 24.8±1.5 years, disease duration 14.7±2.2 years). Full descriptive data are presented in table 1.
Descriptive data including autoantibodies of study participants at baseline
Safety evaluation
None of the patients had SAE and there were no AEs reported during treatment with the low dose, while four patients reported mild and transient AEs (mostly neurological sensations) at the medium and high dose of GABA (online supplemental table 1). Hemoglobin levels decreased when compared with baseline during the medium-dose and high-dose treatment, which was deemed to be related to the extensive blood sampling during the study (baseline 142.8±3.1 g/L, low-dose 137.5±2.6 g/L, medium-dose 131.3±2.3 and high-dose 124.8±2.5, p<0.001). Blood platelet and leukocyte counts were unaffected by GABA treatment. Also, ALT, AST, bilirubin and creatinine levels were unaffected, whereas alkaline phosphate levels slightly decreased during the high-dose treatment (data not shown). As expected, the GABA pharmacokinetics displayed increasing AUC levels at higher doses (online supplemental table 2).
Supplemental material
Supplemental material
Metabolic parameters
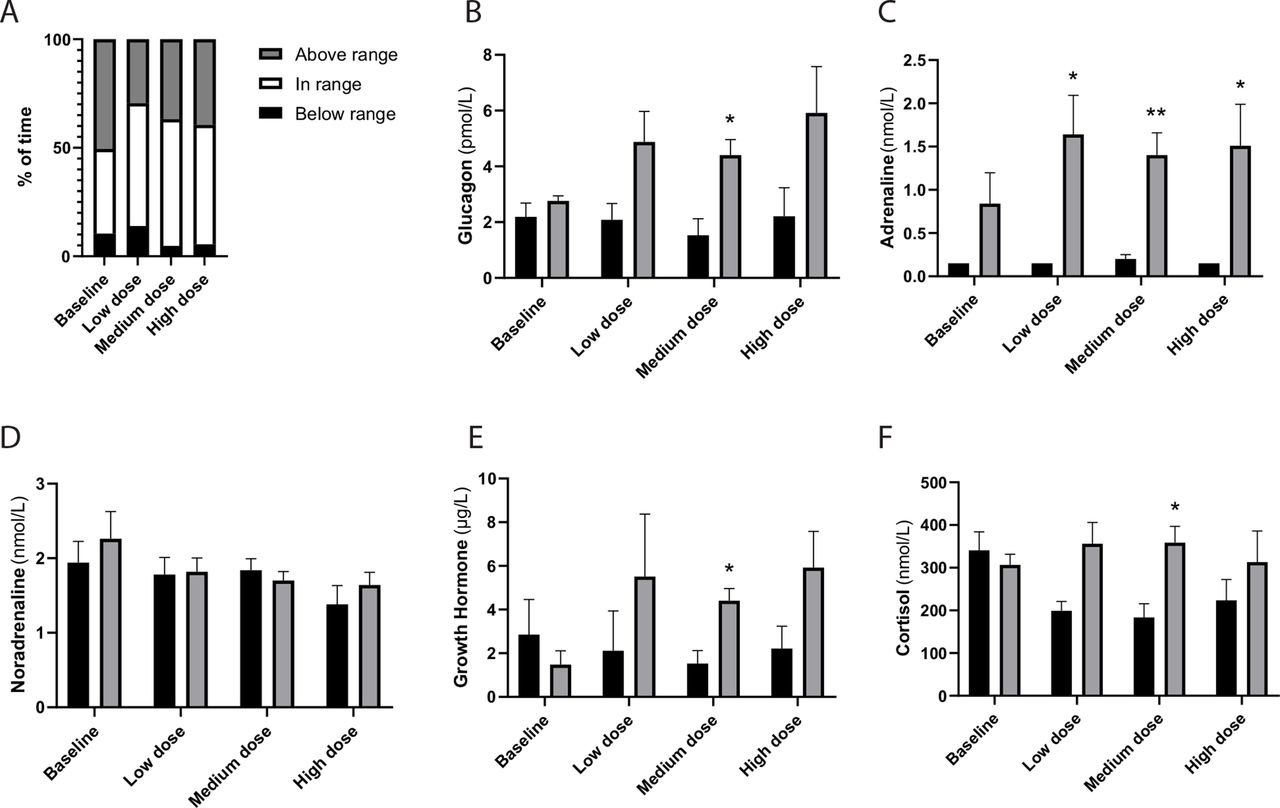
Five of the patients had undetectable C peptide levels when analyzed with the standard clinical assay (ie, <0.01 nmol/L), and both the fasting and stimulated levels were unaffected by short-term GABA treatment. When assessed by the ultrasensitive C peptide ELISA, three patients were found to have detectable C peptide under fasting conditions and one additional patient during stimulated conditions. The levels were, however, unaffected by the short-term GABA treatment (data not shown). Given the small sample size and limited study period, we could not detect any significant differences with regard to time in range, or time below range, when analyzing the FGM data (figure 1A).

{kind=link}
GABA treatment improves the counter-regulatory hormone response to hypoglycemia in type 1 diabetes. (A) Flash glucose monitoring for all subjects (n=6) at baseline and during short-term oral treatment with GABA in increasing doses. (B–F) Hormonal counter-regulatory response during hyperinsulinemic hypoglycemic clamps. Glucose levels were regulated by an intravenous continuous rate of insulin and a variable rate of glucose in order to reach first a 30 min plateau with glucose levels of 5.5 mmol/L, followed by a 30 min plateau at 2.5 mmol/L. Blood samples were collected at the end of each plateau. The analysis contains data from the five subjects without detectable C peptide (<0.01 nmol/L) in which the counter-regulatory response was blunted at baseline. Black bars represent normoglycemia (5.5 mmol/L) and gray bars hypoglycemic conditions (2.5 mmol/L). Data are presented as mean±SEM. *P<0.05 and **P<0.01 compared with the normoglycemic levels at the respective occasion. GABA, gamma-aminobutyric acid.
Response to hypoglycemia
The patient with remaining C peptide displayed a normal hormonal counter-regulatory response to hypoglycemia at baseline, which was maintained under the GABA treatment (data not shown). In contrast, the five patients without detectable C peptide (<0.01 nmol/L) displayed absence of counter-regulatory response at baseline (figure 1B–F). During GABA treatment (600 mg) a counter-regulatory response of glucagon, epinephrine, GH, as well as cortisol occurred in response to hypoglycemia (figure 1B–F).
Discussion
Short-term oral GABA treatment was not associated with any SAEs. AEs were registered in four subjects, but they were all mild and transient, mainly neurological sensations. In previous studies, fatigue and mild weakness have also been reported.14 In another study, 3 g of GABA caused mild transaminase increases in 2% of study subjects.15 Glucose control was maintained during the study period and the frequency of hypoglycemia did not increase.
In contrast to previous studies in which activation of the GABA-A receptor by benzodiazepines has been found to blunt the counter-regulatory response,16 we paradoxically found that the hormonal counter-regulatory response to hypoglycemia was enhanced by GABA treatment. A tentative explanation for this difference in results is that GABA per se has limited capacity to cross the blood–brain barrier, while benzodiazepines easily cross to exert their effects in the CNS. The mechanism for the counter-regulatory failure induced by benzodiazepines has previously been shown to be lactate release in the ventromedial hypothalamus.17 Also, the metabolism of GABA and benzodiazepines differs, which could in turn impact the counter-regulatory response. The present study shows that if the peripheral effects of GABA are isolated, the hormonal counter-regulatory response instead become enhanced by yet unknown mechanisms. A possible explanation could be the activation of GABA-A receptors in other peripheral organs/tissues of importance for the hormonal counter-regulatory response. For instance, GABA-A receptor activation in chromaffin cells within the adrenal glands induces the secretion of catecholamines.9 The study period and sample size (number of subjects included) were, however, in this study too small to assess potential clinical benefits in hypoglycemia severity and frequency.
We conclude that the controlled-release formulation of GABA (Remygen) can be considered a safe treatment in T1D and that a larger, long-term clinical trial is warranted in order to further study the clinical potential of GABA as a drug for beta-cell regeneration and, in view of the findings in this study, hypoglycemia protection.
Data availability statement
Data are available upon reasonable request. The data sets generated during the current study can be made available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by both the Uppsala County Ethics Board (Dnr 2018/200/1) and the Swedish Medical Products Agency. The reported investigations were carried out in accordance with the principles of the Declaration of Helsinki as revised in 2013.
Acknowledgments
We are grateful for the great efforts and expert assistance by Karin Kjellström and Rebecka Hilmius (research nurses at Uppsala University Hospital). Diamyd Medical is gratefully acknowledged for providing Remygen. We are grateful for the expert assistance with GABA analysis by Professor Jonas Bergquist and Dr Kumari Ubhayasekera at the Mass Spectrometry Based Metabolomics Facility (Uppsala University, Sweden) and to Mercodia (Uppsala, Sweden) for their expert assistance with ultrasensitive C peptide analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DE and HL are joint first authors.
Contributors P-OC, DE and BB designed the study. HL, DE, HH, AE, JC-C (until February 28, 2019) and P-OC performed the clinical assessments in the study. DE, HH and P-OC researched the data, and DE, HL and P-OC wrote the manuscript. All authors critically reviewed the manuscript. P-OC is the guarantor of this work.
Funding We are grateful for the financial support from Barndiabetesfonden, Vetenskapsrådet, Diabetesfonden, Exodiab and the Swedish Society for Medical Research.
Disclaimer Funders were not involved in the study design, acquisition, analysis and interpretation of data or writing of this article.
Competing interests DE and POC are listed as coinventors for a patent application submitted by Diamyd Medical, but do not have any financial interests in Diamyd Medical. None of the other authors have any conflicts of interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.