Article Text

Abstract
Introduction Here we report the glycemic efficacy and safety of ertugliflozin in patients in the VERTIS CV cardiovascular outcome trial with chronic kidney disease (CKD) stage 3.
Research design and methods Prespecified and post-hoc analyses were performed in patients with an estimated glomerular filtration rate (eGFR) 30–<60 mL/min/1.73 m2 at screening. The primary endpoint was glycemic efficacy at week 18. Longer term glycemic efficacy and changes in body weight, systolic blood pressure (SBP), and eGFR were also evaluated.
Results Among 8246 patients in VERTIS CV, 1776 patients had CKD stage 3; 1319 patients had CKD stage 3A (eGFR 45–<60 mL/min/1.73 m2); 457 patients had CKD stage 3B (eGFR 30–<45 mL/min/1.73 m2). Week 18 least squares (LS)-mean (95% CI) placebo-adjusted changes from baseline in glycated hemoglobin (HbA1c) for 5 mg and 15 mg ertugliflozin were −0.27% (−0.37% to –0.17%) and −0.28% (−0.38% to –0.17%), respectively, for CKD stage 3 overall and −0.27% (−0.38% to –0.15%) and −0.31% (−0.43% to –0.19%), respectively, for CKD stage 3A (all p<0.001). For CKD stage 3B, the reduction in HbA1c for 5 mg ertugliflozin was −0.28% (−0.47% to –0.08%) (p=0.006) and for 15 mg ertugliflozin was −0.19% (−0.39% to 0.01%) (p=0.064). LS-mean placebo-adjusted reductions in body weight (range: −1.32 to −1.95 kg) and SBP (range: −2.42 to −3.41 mm Hg) were observed across CKD stage 3 categories with ertugliflozin. After an initial dip, eGFR remained above or near baseline with ertugliflozin treatment. The incidence of overall adverse events (AEs), symptomatic hypoglycemia, hypovolemia, and kidney-related AEs did not differ between ertugliflozin and placebo across CKD stage 3 subgroups.
Conclusions In VERTIS CV patients with CKD stage 3A, ertugliflozin resulted in reductions in HbA1c, body weight and SBP, maintenance of eGFR, and was generally well tolerated. Results in the CKD stage 3B subgroup were generally similar except for an attenuated HbA1c response with the 15 mg dose.
Trial registration number NCT01986881.
- diabetes mellitus
- type 2
- kidney failure
- chronic
- glycated hemoglobin A
- drug therapy
Data availability statement
Data are available upon reasonable request. Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA’s data sharing policy, including restrictions, is available at http://engagezone.msd.com/ds_documentation.php. Requests for access to the clinical study data can be submitted through the EngageZone site or via email to dataaccess@merck.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Patients with type 2 diabetes mellitus (T2DM) and chronic kidney disease (CKD) are at increased risk of further progression of CKD.
The glycemic efficacy of sodium–glucose cotransporter 2 (SGLT2) inhibitors is dependent on glomerular filtration and is attenuated in patients with CKD stage 3 (estimated glomerular filtration rate (eGFR) 30–<60 mL/min/1.73 m2); however, independent of glycemic efficacy, members of the SGLT2 inhibitor class have been shown to slow the deterioration of kidney function in this patient population.
What are the new findings?
This secondary analysis of the ertugliflozin cardiovascular outcome study, VERTIS CV, explored the glycemic efficacy and safety of ertugliflozin, compared with placebo, in patients with CKD stage 3.
Treatment with ertugliflozin 5 and 15 mg doses, compared with placebo, resulted in modest reductions in glycated hemoglobin from baseline, which were maintained long term; reductions in body weight and systolic blood pressure were similar to those observed in previous analyses of patients with preserved kidney function.
The safety profile of ertugliflozin in VERTIS CV patients with CKD stage 3 was consistent with previous assessments of ertugliflozin safety; ertugliflozin, compared with placebo, slowed the decrease of eGFR over time.
How might these results change the focus of research or clinical practice?
The present analyses add to the growing body of evidence on the positive benefit/risk profile of the SGLT2 inhibitor class in patients with T2DM and CKD stage 3.
Introduction
Diabetes mellitus is a common cause of chronic kidney disease (CKD).1 A recent analysis of National Health and Nutrition Examination Survey (NHANES) data showed that among US adults with diabetes, 28.1% had concomitant CKD (defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 or a urinary albumin–creatinine ratio (UACR) ≥30 mg/g).2 NHANES data have also shown a ~5-fold increase in the incidence of CKD in patients with diabetes versus patients without diabetes.3 Furthermore, people with CKD are at high risk of further deterioration of kidney function over time and at risk of cardiovascular (CV) events including myocardial infarction, stroke, and heart failure. According to the US Renal Data System 2020 Annual Data Report, heart failure and acute myocardial infarction were about four times as common and stroke/transient ischemic attack was more than twice as common in patients with CKD versus those without CKD.4 Treatment of these inter-related conditions has become a prominent focus of the treatment of people with type 2 diabetes mellitus (T2DM) and CKD.5
The glycemic efficacy of sodium–glucose cotransporter 2 (SGLT2) inhibitors is dependent on glomerular filtration, and glycemic efficacy is attenuated in patients with CKD stage 3 (eGFR 30–<60 mL/min/1.73 m2). However, SGLT2 inhibitors have beneficial CV and kidney protective effects in patients with T2DM that are related to glycemic control and that are independent of glycemic control.6–8 Based on the results from multiple outcome trials that have demonstrated the beneficial effects of SGLT2 inhibitors on CV and kidney endpoints, including in patients with CKD stage 3, society guidelines recommend the addition of an SGLT2 inhibitor for patients with T2DM and established CKD (eGFR 30–≤60 mL/min/1.73 m2 or UACR >30 mg/g) to reduce the risk of CKD progression and future CV events, including hospitalization for heart failure (HHF).9–11
Ertugliflozin is an SGLT2 inhibitor approved for use in adults with T2DM as an adjunct to diet and exercise to improve glycemic control.12 13 VERTIS CV was the CV outcome trial for ertugliflozin, conducted in patients with T2DM and atherosclerotic cardiovascular disease (ASCVD), which assessed the CV safety of ertugliflozin.14 15 Enrollment criteria in VERTIS CV allowed for the entry of patients with an eGFR as low as 30 mL/min/1.73 m2 at screening, providing an opportunity for a characterization of glycemic efficacy, CV outcomes, and safety across a spectrum of kidney function. The present analyses assessed the glycemic efficacy and safety of ertugliflozin in the subgroup of VERTIS CV patients with CKD stage 3 at trial entry.
Materials and methods
Study design
Glycemic efficacy and safety were assessed in the subset of patients with baseline CKD stage 3 who participated in VERTIS CV. VERTIS CV was a prospective, randomized, double-blind, placebo-controlled, parallel-group, multicenter trial conducted in patients with T2DM and established ASCVD comparing ertugliflozin versus placebo.14 15 Eligible patients were randomly assigned (1:1:1) to once-daily ertugliflozin 5 mg or 15 mg or placebo in addition to background standard-of-care treatment. During the initial 18 weeks after randomization, patients’ background antihyperglycemic regimen was to remain stable unless glycemic rescue was required, or the patient experienced clinically significant hypoglycemia. This design facilitated the assessment of glycemic efficacy and other metabolic parameters in those patients with CKD stage 3, compared with placebo, without the confounding influence of changes in background antihyperglycemic therapy during the first 18 weeks.
Patient population
Detailed inclusion and exclusion criteria for the trial have been published previously.14 15 Adult patients (≥40 years of age) with T2DM (glycated hemoglobin (HbA1c) 7.0%–10.5%, inclusive) and stable, established ASCVD of the coronary, cerebrovascular, and/or peripheral arterial systems were included. Key exclusion criteria were type 1 diabetes, history of ketoacidosis, and eGFR <30 mL/min/1.73 m2, calculated using the four-variable Modification of Diet in Renal Disease study equation.16 For the present subgroup analyses, patients with CKD stage 3 were classified based on an eGFR of 30–<60 mL/min/1.73 m2 at baseline; patients with CKD stage 3A based on an eGFR of 45–<60 mL/min/1.73 m2 at baseline; and patients with CKD stage 3B based on an eGFR of 30–<45 mL/min/1.73 m2 at baseline.
Efficacy outcomes and analysis
Subgroup analyses of glycemic efficacy outcomes in patients with CKD stage 3A were prespecified in the VERTIS CV statistical analysis plan. The prespecified glycemic efficacy outcomes were change from baseline to week 18 in HbA1c and fasting plasma glucose (FPG), and the proportion of patients with HbA1c <7.0% at week 18. Post-hoc analyses of change from baseline to week 18 in body weight and systolic blood pressure (SBP) were also conducted. Analyses of change over time in HbA1c at weeks 18, 52, 104, 156, and 208 in patients with CKD stage 3 were prespecified. The subgroup analyses of the same efficacy outcomes in patients with CKD stage 3 and CKD stage 3B were post-hoc analyses, conducted using the same statistical methodology as the prespecified analyses. Analyses included those patients in the respective subgroup who were randomized, received at least one dose of study medication (ertugliflozin or placebo), and had at least one assessment at or after baseline. Efficacy data reported for week 18 endpoints were censored after initiation of any glycemic rescue therapy if the rescue occurred prior to week 18. Long-term assessments of efficacy included data regardless of changes in background antihyperglycemic medications.
Least squares (LS)-mean change from baseline to week 18 in efficacy outcomes with 95% CIs was calculated using a constrained longitudinal data analysis (cLDA) model with fixed effects for treatment, time (categorical), baseline eGFR, and the interaction of time-by-treatment. Change over time in HbA1c at weeks 18, 52, 104, 156, and 208 was calculated using an analysis of covariance model adjusted for baseline HbA1c, treatment, time, subgroup, treatment-by-subgroup interaction, and treatment-by-subgroup-by-time interaction. Adjusted ORs for patients with HbA1c <7.0% at week 18 with 95% CIs were calculated using a logistic regression model fitted with fixed effects for treatment and covariates for baseline HbA1c and baseline eGFR. Missing data for HbA1c in the logistic regression model were multiply imputed using predicted values from the cLDA model of the primary analysis. In the overall subgroup of patients with CKD stage 3, week 18 HbA1c values were missing in 120 of 617 (19.4%), 102 of 559 (18.2%), and 130 of 597 (21.8%) patients in the full analysis set for the ertugliflozin 5 mg, 15 mg, and placebo treatment groups, respectively. Nominal p values (unadjusted for multiplicity) were calculated.
Safety outcomes and analysis
The safety analysis population included all patients with CKD stage 3 who had undergone randomization and received at least one dose of study medication (ertugliflozin or placebo). Safety analyses included data collected over the entire duration of the VERTIS CV trial (not limited to the week 18 efficacy endpoint). Safety analyses included adverse events (AEs) collected from randomization to 14 days after the final dose of study medication and 2 days after the final dose of study medication for laboratory endpoints. Safety was analyzed separately for patients with CKD stage 3, CKD stage 3A, and CKD stage 3B; the analyses were designed to compare treatment groups within each subgroup. Assessments included AEs, serious AEs (SAEs), discontinuations due to AEs, deaths, vital signs, and laboratory evaluations. The Medical Dictionary for Regulatory Activities (MedDRA; V.22.1) was used to classify AEs with respect to system organ class and preferred term. Kidney-related AEs were identified using the Standardised MedDRA Query of ‘Acute renal failure’. Adjudication of potential kidney events was performed by an independent, blinded committee to assess causality relative to study medication as ‘Very likely’, ‘Probable’, ‘Possible’, ‘Doubtful’, and ‘Not related’. Potential kidney events were identified by systematically searching AEs, SAEs, and predefined limits of change (doubling of serum creatinine from baseline or ≥50% decrease from baseline eGFR). Prespecified AEs of special clinical interest included AEs related to urinary tract infection (UTI), genital mycotic infection (GMI), symptomatic hypoglycemia, and hypovolemia.
Results
Patient disposition and baseline characteristics
In VERTIS CV, a total of 8246 patients with T2DM and ASCVD underwent randomization; 8238 patients received at least one dose of ertugliflozin or placebo.14 15 Of the 8246 patients randomized, 1776 patients with CKD stage 3 at baseline were identified based on an eGFR of 30–<60 mL/min/1.73 m2, comprising 1319 patients with CKD stage 3A (eGFR 45–<60 mL/min/1.73 m2) and 457 patients with CKD stage 3B (eGFR 30–<45 mL/min/1.73 m2).
Baseline demographic and clinical characteristics were well balanced across treatment groups in the subgroup of patients with CKD stage 3 (table 1). In the overall population of patients with CKD stage 3, the majority of patients were white (86.1%) and male (64.3%); mean baseline age (±SD) was 68.1±7.6 years; mean duration of T2DM was 15.7±8.9 years; mean HbA1c was 8.2%±0.9%; and mean eGFR was 49.3±7.5 mL/min/1.73 m2.
Baseline demographics and clinical characteristics of VERTIS CV patients with CKD stage 3*
Baseline characteristics were also similar across treatment groups in the CKD stage 3A and CKD stage 3B subgroups of patients (online supplemental table 1). Patients with CKD stage 3B had a slightly longer mean duration of T2DM (16.7±9.3 years) and less frequent use of metformin (45.1%) but more frequent use of insulin (68.5%) compared with patients with CKD stage 3A (mean duration of T2DM: 15.3±8.8 years; metformin use: 68.9%; insulin use: 54.7%). In line with a more advanced stage of kidney function impairment, patients with CKD stage 3B also had a lower mean eGFR (38.8±4.0 mL/min/1.73 m2) and a higher prevalence of macro-albuminuria (21.9%) at baseline compared with patients with CKD stage 3A (mean eGFR: 53.0±4.3 mL/min/1.73 m2; macro-albuminuria: 13.5%).
Supplemental material
HbA1c efficacy outcomes
In the subgroup of VERTIS CV patients with CKD stage 3, significant reductions in HbA1c over 18 weeks were observed with ertugliflozin 5 mg and 15 mg versus placebo (figure 1A). The placebo-adjusted LS-mean changes from baseline (95% CI) to week 18 were −0.27% (−0.37% to –0.17%) with ertugliflozin 5 mg and −0.28% (−0.38% to –0.17%) with ertugliflozin 15 mg (both p<0.001). Long-term change in HbA1c over time in the CKD stage 3 subgroup of patients is shown in figure 1B. Greater reductions in HbA1c with ertugliflozin, compared with placebo, were observed over 4 years.

(A) HbA1c efficacy at week 18 in VERTIS CV patients with CKD stage 3, CKD stage 3A, and CKD stage 3B. Calculated using a cLDA model with fixed effects for treatment, time (categorical), baseline (BL) eGFR (continuous), and the interaction of time-by-treatment. P values are nominal; n is the number of patients in the cLDA FAS (ie, randomized patients who took at least one dose of study medication and had at least one assessment at or after BL) with non-missing assessments at BL. (B) HbA1c efficacy over time in VERTIS CV patients with CKD stage 3. Calculated using an ANCOVA model adjusted for baseline HbA1c, treatment, time, subgroup, treatment-by-subgroup interaction, and treatment-by-subgroup-by-time interaction; n is the number of patients in the ANCOVA FAS (ie, randomized patients who took at least one dose of study medication and had a BL and at least one post-BL assessment) with non-missing assessments at the specific time point. CKD stage was based on eGFR calculated using the MDRD equation. ANCOVA, analysis of covariance; CKD, chronic kidney disease; CKD stage 3, eGFR 30–<60 mL/min/1.73 m2; CKD stage 3A, eGFR 45–<60 mL/min/1.73 m2; CKD stage 3B, eGFR 30–<45 mL/min/1.73 m2; cLDA, constrained longitudinal data analysis; eGFR, estimated glomerular filtration rate; ERTU, ertugliflozin; FAS, full analysis set; HbA1c, glycated hemoglobin; LS, least squares; MDRD, Modification of Diet in Renal Disease; PBO, placebo.
Significant reductions in HbA1c were observed with both ertugliflozin doses versus placebo in the subgroup of patients with CKD stage 3A (figure 1A). The adjusted mean changes from baseline to week 18 were −0.27% (−0.38% to –0.15%) with ertugliflozin 5 mg and −0.31% (−0.43% to –0.19%) with ertugliflozin 15 mg (both p<0.001). In the subgroup of patients with CKD stage 3B, a significant placebo-adjusted reduction in HbA1c from baseline to week 18 was observed with the 5 mg dose of ertugliflozin (−0.28% (−0.47% to –0.08%); p=0.006) (figure 1A) but the observed reduction in HbA1c was not statistically significant for the 15 mg dose (−0.19% (−0.39% to 0.01%); p=0.064) (figure 1A).
In the subgroup of patients with CKD stage 3, the proportion of patients who had HbA1c <7.0% at week 18 was greater in the ertugliflozin 5 mg and 15 mg groups compared with placebo (table 2).
Other efficacy outcomes at week 18 in VERTIS CV patients with CKD stage 3*
Other efficacy outcomes
In patients with CKD stage 3, both the 5 and 15 mg doses of ertugliflozin, compared with placebo, were associated with significant reductions in FPG, body weight, and SBP over 18 weeks (table 2). Significant reductions in FPG from baseline to week 18 were observed with ertugliflozin versus placebo in patients with CKD stage 3A; however, in the subgroup of patients with CKD stage 3B, reductions in FPG were not statistically significant (online supplemental table 2). Both the 5 and 15 mg doses of ertugliflozin significantly reduced body weight in the CKD stage 3A and stage 3B subgroups of patients (online supplemental table 2). Compared with placebo, ertugliflozin significantly reduced SBP over 18 weeks in the subgroup of patients with CKD stage 3A; however, in the subgroup of patients with CKD stage 3B, reductions in SBP were not statistically significant (online supplemental table 2).
Safety outcomes
In the subgroup of patients with CKD stage 3, the incidence of AEs, SAEs, AEs leading to study drug discontinuation, and deaths did not differ across the ertugliflozin and placebo treatment groups (table 3). An analysis of prespecified AEs of interest revealed a similar incidence of UTIs with ertugliflozin and placebo in patients with CKD stage 3 (table 3). An increased incidence of GMIs was observed with ertugliflozin treatment compared with placebo in both women and men (table 3). The proportion of patients experiencing events of symptomatic hypoglycemia or hypovolemia was well balanced across placebo and ertugliflozin treatment groups in patients with CKD stage 3 (table 3).
Adverse events in VERTIS CV patients with CKD stage 3*
The incidence of kidney-related AEs, including the incidence of acute kidney injury, was similar with placebo and ertugliflozin treatment in patients with CKD stage 3 (table 3). The occurrence of kidney-related AEs meeting prespecified criteria for adjudication was also similar across treatment groups in patients with CKD stage 3. The majority of adjudicated kidney events were assessed as having ‘Doubtful’ or ‘Not related’ causality to the study medication (table 3). No events were assessed as ‘Very Likely’ or ‘Probable’ and few events were adjudicated as ‘Possible’ with no evidence of increased frequency associated with ertugliflozin treatment.
The general pattern of AEs observed between treatment groups in the subgroups of patients with CKD stage 3A and stage 3B (online supplemental table 3) was consistent with that seen in the overall group of patients with CKD stage 3 (table 3), including the incidence of AEs, SAEs, AEs leading to study drug discontinuation, deaths, prespecified AEs of interest, and kidney-related AEs. Although the incidence of kidney-related AEs was balanced across placebo and ertugliflozin treatment groups in patients with CKD stage 3A and CKD stage 3B, kidney-related AEs were more frequently reported in patients with CKD stage 3B across all treatment groups (online supplemental table 3), consistent with having a more advanced impairment in kidney function.
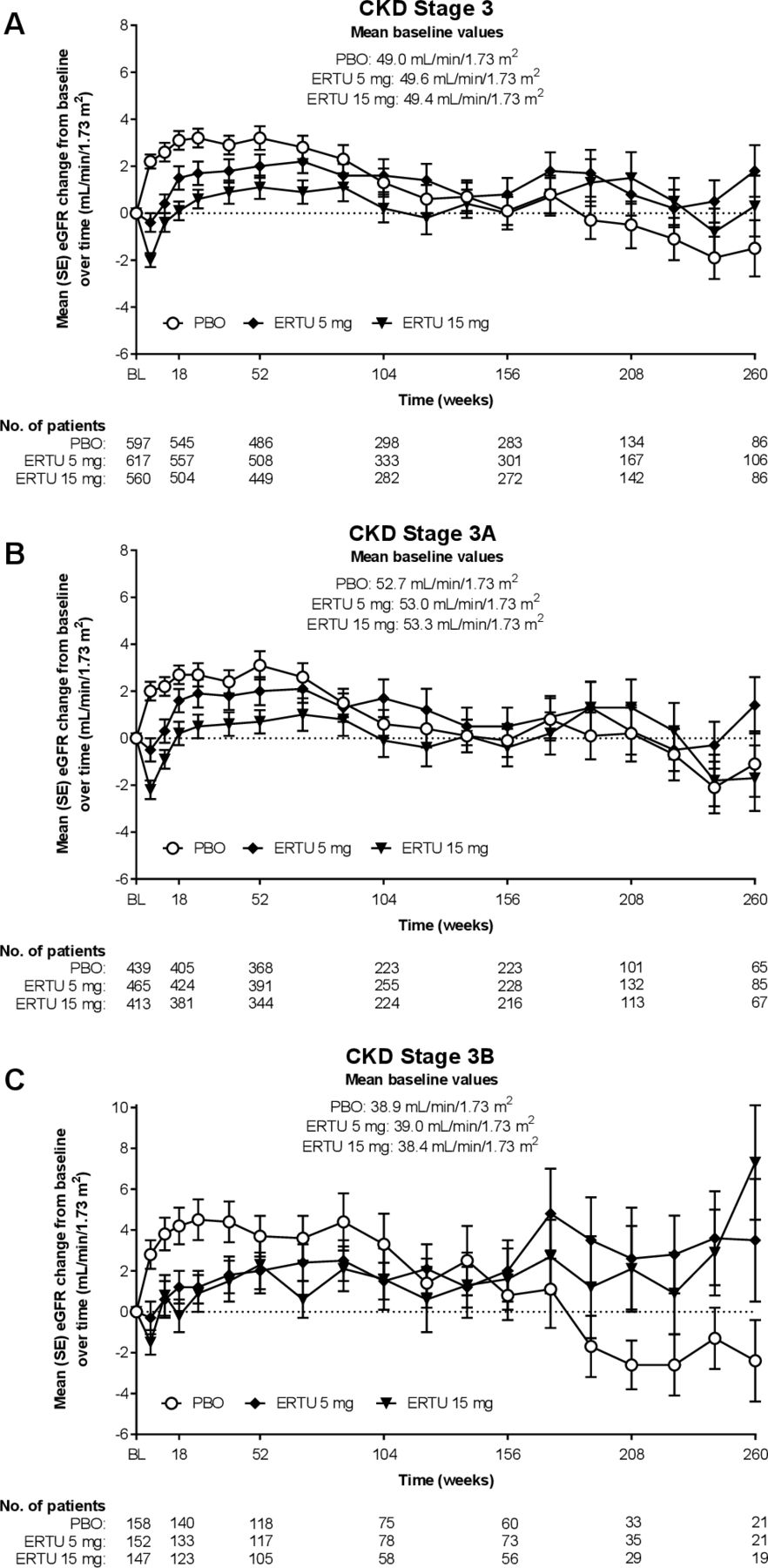
Compared with placebo, initiation of ertugliflozin treatment was associated with an early dip in eGFR that was transient and followed by eGFR levels that were maintained above or near baseline (figure 2A). The pattern of change from baseline in eGFR over time observed in the subgroups of patients with CKD stage 3A (figure 2B) and CKD stage 3B (figure 2C) was also generally similar to that seen in the overall group of patients with CKD stage 3 (figure 2A).

{kind=link}
{kind=link}
Mean (±SE) change from baseline (BL) in eGFR over time in VERTIS CV patients with (A) CKD stage 3, (B) CKD stage 3A, and (C) CKD stage 3B. CKD stage was based on eGFR calculated using the MDRD equation. n is the number of patients with non-missing assessments at both BL and the specific time point. CKD, chronic kidney disease; CKD stage 3, eGFR 30–<60 mL/min/1.73 m2; CKD stage 3A, eGFR 45–<60 mL/min/1.73 m2; CKD stage 3B, eGFR 30–<45 mL/min/1.73 m2; eGFR, estimated glomerular filtration rate; ERTU, ertugliflozin; MDRD, Modification of Diet in Renal Disease; PBO, placebo.
Discussion
The inclusion criteria for the VERTIS CV study allowed the entry of patients with an eGFR ≥30 mL/min/1.73 m2, which resulted in the randomization of 21.5% (1776 of 8246) of patients with CKD stage 3 in the trial. Among those with CKD stage 3, ~74% had CKD stage 3A and ~26% had CKD stage 3B. The inclusion of these patients in the VERTIS CV trial allowed a comprehensive assessment of ertugliflozin glycemic efficacy and safety in patients with T2DM, ASCVD, and CKD stage 3.
The use of data from the initial 18 weeks of VERTIS CV was designed to allow a comparison with placebo as doses of background antihyperglycemic medications were held stable during this period; after week 18, investigators were encouraged to optimize glycemic therapy to achieve individualized treatment goals. The present analyses demonstrated that both doses of ertugliflozin (5 mg and 15 mg) resulted in statistically significant placebo-adjusted reductions in HbA1c from baseline at week 18 in the overall CKD stage 3 subgroup and in the CKD stage 3A subgroup. In the CKD stage 3B subgroup, the ertugliflozin 15 mg dose did not achieve statistical significance, compared with placebo, and may be due to the relatively small patient numbers in this subgroup. Another contributing factor to the apparent absence of dose–response in the CKD stage 3B subgroup could be the greater degree of diminished kidney function in this subgroup in the context of the dose–response curve of ertugliflozin (model-predicted HbA1c and 24-hour urinary glucose excretion responses for ertugliflozin 5 mg and 15 mg doses are >80% and >90%, respectively, of the maximum model-predicted response).17
The observed reductions from baseline at week 18 in FPG roughly paralleled those observed for HbA1c. The reduction in HbA1c in the CKD stage 3B group, despite the lack of a significant decrease in FPG levels, likely resulted from suppression of postprandial plasma glucose, a stronger contributor to HbA1c than FPG. Although the longer term assessment of HbA1c efficacy for CKD stage 3 overall is confounded by changes in background medication that were encouraged to meet individualized glycemic goals after 18 weeks, the data indicate that ertugliflozin treatment, compared with placebo, was associated with consistently better glycemic control over 4 years. In the VERTIS CV trial protocol,14 participating clinics were encouraged to optimize glycemic control after 18 weeks, using agents from all antihyperglycemic classes except SGLT2 inhibitors. Thus, the continued separation of the HbA1c curves between the placebo group and the ertugliflozin groups most likely reflects practice patterns by the study investigators.15 However, the durable efficacy observed in the ertugliflozin-treated groups could also be due to the weight loss (which improves glycemic control) and/or preservation of kidney function (which supports the mechanism of action of SGLT2 inhibitors) that was observed in these patients.
Although glycemic parameters following ertugliflozin treatment in the CKD stage 3 and stage 3A categories were statistically significantly different from placebo, as anticipated by the SGLT2 inhibitor mechanism of action within the kidney, the reductions in HbA1c in the CKD stage 3 categories were attenuated compared with the HbA1c reductions with ertugliflozin 5 mg and 15 mg observed in a pooled analysis of placebo-controlled VERTIS phase 3 glycemic efficacy studies that did not include VERTIS CV.18 In those studies, in which exclusion criteria required randomized patients to have an eGFR ≥55 mL/min/1.73 m2 (average eGFR was ~89 mL/min/1.73 m2), the changes from baseline in HbA1c at week 26 were −0.8% and −0.9% for ertugliflozin 5 mg and 15 mg, respectively.18
The magnitude of the HbA1c reductions observed in this analysis of VERTIS CV CKD stage 3, 3A, and 3B subgroups is consistent with that observed for other SGLT2 inhibitors in this patient population. In a subgroup analysis of the EMPA-REG OUTCOME trial,19 the placebo-adjusted change from baseline at week 12 in HbA1c in patients with CKD stage 3 treated with empagliflozin 10 mg and 25 mg was −0.36% for each dose group. The placebo-adjusted changes from baseline at week 12 in HbA1c in patients with CKD stage 3A and stage 3B (pooled 10 mg and 25 mg doses) were −0.43% and −0.21%, respectively.19 Similarly, in a subgroup analysis of CANVAS trial data,20 the placebo-adjusted change from baseline at week 18 in HbA1c in patients with CKD stage 3 treated with canagliflozin (pooled 100 mg and 300 mg doses) was −0.42%, and in the subgroups of patients with CKD stage 3A and stage 3B was −0.45% and −0.35%, respectively. In the DERIVE study, the placebo-adjusted change from baseline at week 24 in HbA1c in patients with CKD stage 3A treated with dapagliflozin 10 mg was −0.34%.21 The HbA1c reductions observed in the present analysis are also consistent with the previous ertugliflozin study in patients with moderately impaired kidney function (VERTIS RENAL).22 In contrast to the attenuated glycemic efficacy of SGLT2 inhibitors observed in patients with CKD stage 3, previous studies have reported a more potent HbA1c-lowering effect of SGLT2 inhibitors in patients with preserved kidney function, with placebo-subtracted HbA1c reductions from baseline of −0.6% to −0.8% in monotherapy studies.23 24
Although HbA1c efficacy was attenuated in this patient population, reductions in body weight and SBP with ertugliflozin in patients with CKD stage 3 were similar to those observed in patients with preserved kidney function in a pooled analysis of placebo-controlled VERTIS phase 3 studies.18 The similar body weight and SBP reductions in patients with varying degrees of kidney function suggest that the effects of ertugliflozin on body weight and SBP are independent from glucosuria.
In the present analyses of VERTIS CV patients with CKD stage 3, the safety of ertugliflozin was consistent with that observed in the overall population followed over the duration of the VERTIS CV study and consistent with the known safety profile of ertugliflozin from the VERTIS phase 3 development program.15 25 Incidences of summary AE measures, kidney-related AEs, and adjudicated kidney events were similar in the ertugliflozin and placebo groups within the CKD stage 3, stage 3A, and stage 3B subgroups of patients. Symptomatic hypoglycemia was also similar across treatment groups within each of the CKD categories. The incidence of GMIs was higher in both men and women in the ertugliflozin groups within each CKD category compared with placebo.
The observation that after the initial dip in eGFR with ertugliflozin treatment, eGFR returned to baseline and remained near or above baseline to the end of the study in patients with CKD stage 3, as opposed to remaining below baseline as was observed in the overall VERTIS CV population,15 is consistent with the results from CV outcomes trials of other SGLT2 inhibitors.20 26 27 As is the case for the long-term pattern of changes in eGFR observed in the overall VERTIS CV population, the present results also suggest an effect of ertugliflozin on the preservation of kidney function in patients with baseline eGFR levels between 30 and 60 mL/min/1.73 m2.
The goal of the VERTIS CV trial was to attempt to achieve glycemic equipoise between the placebo and ertugliflozin groups. Although it is unlikely the modest reductions in HbA1c observed in the CKD stage 3 subgroup contributed significantly to cardiorenal outcomes in these patients, the Diabetes Control and Complications Trial and other landmark studies have demonstrated a linear relationship between HbA1c reduction and decreased risk of microvascular complications (reviewed in reference 28). From that perspective, reductions in HbA1c of the magnitude observed in this analysis would be clinically meaningful. Moreover, the attenuated glycemic efficacy observed with SGLT2 inhibitors in patients with CKD stage 3 should be viewed within the broader context of other effects of SGLT2 inhibitors in this patient population who are at high risk of further deterioration of kidney function over time and of HHF. Preservation of kidney function and reduction in the risk of HHF in patients with CKD stage 3 have been demonstrated by other members of the SGLT2 inhibitor class.27 29–31 In VERTIS CV, prespecified secondary analyses have demonstrated that treatment with ertugliflozin, compared with placebo, slowed the deterioration of kidney-filtering capacity (eGFR), reduced albuminuria (UACR), and reduced progression and increased regression of albuminuria across a range of baseline kidney function subgroups defined by baseline eGFR (including CKD stage 3), albuminuria, and Kidney Disease: Improving Global Outcomes risk categories.32 In VERTIS CV, the assessment of HHF risk was a prespecified secondary objective. The assessment showed that ertugliflozin treatment, compared with placebo, was associated with a 30% reduction in the risk of HHF.15 33 In addition, the effect of ertugliflozin on reducing the risk of HHF was greater (higher relative risk reductions and absolute risk reductions) in the subgroup of VERTIS CV patients with CKD stage 3.33
There are several potential limitations to the present analysis. The analysis was a subgroup analysis rather than a dedicated study in patients with CKD stage 3. The duration of the placebo-controlled period was limited to 18 weeks. However, maximal HbA1c efficacy is typically observed after initiation of SGLT2 inhibitor therapy by week 12, and the observed response should be useful to assist clinicians in setting expectations for glycemic control for these patients. This substudy was conducted exclusively in patients with T2DM and ASCVD; nonetheless, the findings are likely to be broadly applicable to patients with T2DM without prevalent ASCVD. Finally, the study population was predominantly white (~86%), which limits the generalizability of our findings to individuals from under-represented populations.
In conclusion, the present analyses of VERTIS CV patients with CKD stage 3 demonstrated reductions in glycemic parameters (HbA1c and FPG), body weight, and SBP similar to those observed for other members of the SGLT2 inhibitor class. These results, and results from the main VERTIS CV study, suggest that ertugliflozin preserves kidney function and reduces the risk of HHF, in addition to providing a modest degree of glycemic control in patients with CKD stage 3. The totality of these effects indicates a positive benefit/risk profile of ertugliflozin in patients with T2DM, ASCVD, and CKD stage 3. The present findings add to the body of evidence on the effects of SGLT2 inhibitors in patients with T2DM and CKD stage 3, and provide further support for recent society guidelines for the use of this drug class in this patient population.9–11
Data availability statement
Data are available upon reasonable request. Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA’s data sharing policy, including restrictions, is available at http://engagezone.msd.com/ds_documentation.php. Requests for access to the clinical study data can be submitted through the EngageZone site or via email to dataaccess@merck.com.
Ethics statements
Patient consent for publication
Ethics approval
The VERTIS CV trial was conducted in compliance with the ethical principles of the Declaration of Helsinki and in compliance with all International Conference on Harmonisation Good Clinical Practice Guidelines. Written informed consent was obtained from all participants, and the final protocol and informed consent documentation were reviewed and approved by the institutional review board or independent ethics committee for each of the 567 investigational centers located across 34 countries.
Acknowledgments
The authors would like to thank the investigators, staff, and participants of the VERTIS CV study (Protocol B1521021), and Christopher P Cannon, Bernard Charbonnel, Philip Jones, Ingrid Adamsons, and Mario Maldonado for their critical review of this work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SD-J, REP, DZIC, DKM, JL, RF, JPM, AR, and IG substantially contributed to the conception, design and/or planning of the study. JL, RF, JPM, AR, and IG substantially contributed to the acquisition of data for the study. All authors substantially contributed to the analysis and/or interpretation of the data. SD-J, REP, DZIC, DKM, JL, and IG substantially contributed to the drafting of the manuscript. All authors substantially contributed to the critical review and revision of the manuscript. All authors approved the final version of the manuscript for publication.
Funding This study was sponsored by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey, USA, and Pfizer Inc., New York, New York, USA. Editorial support was provided by Shirley Smith of Engage Scientific Solutions (Horsham, UK) and was funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey, USA, and Pfizer Inc., New York, New York, USA.
Competing interests SD-J has led clinical trials for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk; has received consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Janssen, Merck & Co, and Sanofi; has equity interests in Jana Care and Aerami Therapeutics; and serves on the editorial boards of The American Journal of the Medical Sciences, BMJ Open Diabetes Research & Care, Experimental Biology & Medicine, and Frontiers in Endocrinology. REP has received grants (directed to his institution) from Hanmi Pharmaceutical Co, Janssen, Metavention, Novo Nordisk, Poxel SA, and Sanofi; has received consulting fees (directed to his institution) from AstraZeneca, Corcept Therapeutics Incorporated, Glytec, Hanmi Pharmaceutical Co, Janssen, Merck & Co, Mundipharma, Novo Nordisk, Pfizer, Sanofi, Scohia Pharma, and Sun Pharmaceutical Industries; and has received support for attending meetings/travel (directed to his institution or to the travel provider) from AstraZeneca, Glytec, Merck & Co, Mundipharma, Novo Nordisk, and Pfizer. DZIC has received consulting fees and/or speaking honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Janssen, Merck & Co, Mitsubishi-Tanabe, Novo Nordisk, Prometic, and Sanofi; and has received operating funds from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck & Co, Novo Nordisk, and Sanofi. DKM has received consulting fees from Afimmune, Applied Therapeutics, AstraZeneca, Boehringer Ingelheim, Esperion, Lexicon, Lilly USA, Merck Sharp & Dohme, Metavant, Novo Nordisk, Pfizer, and Sanofi US; has received honoraria from Boehringer Ingelheim; has received payment for expert testimony from Kirkland & Ellis on behalf of Boehringer Ingelheim; and has participated on data safety monitoring boards/advisory boards for CSL Behring, AbbVie, Eidos, Otsuka, Arena, and Akebia. FC has received research grants from the Swedish Research Council, Swedish Heart & Lung Foundation, and King Gustav V and Queen Victoria Foundation; and has received consulting fees from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Merck Sharp & Dohme, Mundipharma, Novo Nordisk, and Pfizer. JL, AR, and IG are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, New Jersey, USA, and may own stock in Merck & Co., Inc., Kenilworth, New Jersey, USA. RF and JPM are employees of, and may own shares/stock options in, Pfizer Inc., New York, New York, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.